
Evaluating the Specificity of Community Injury Hospitalization Data over Time



Abstract
:1. Introduction
2. Methodology
3. Results and Discussion
3.1. Specificity of External Cause Codes
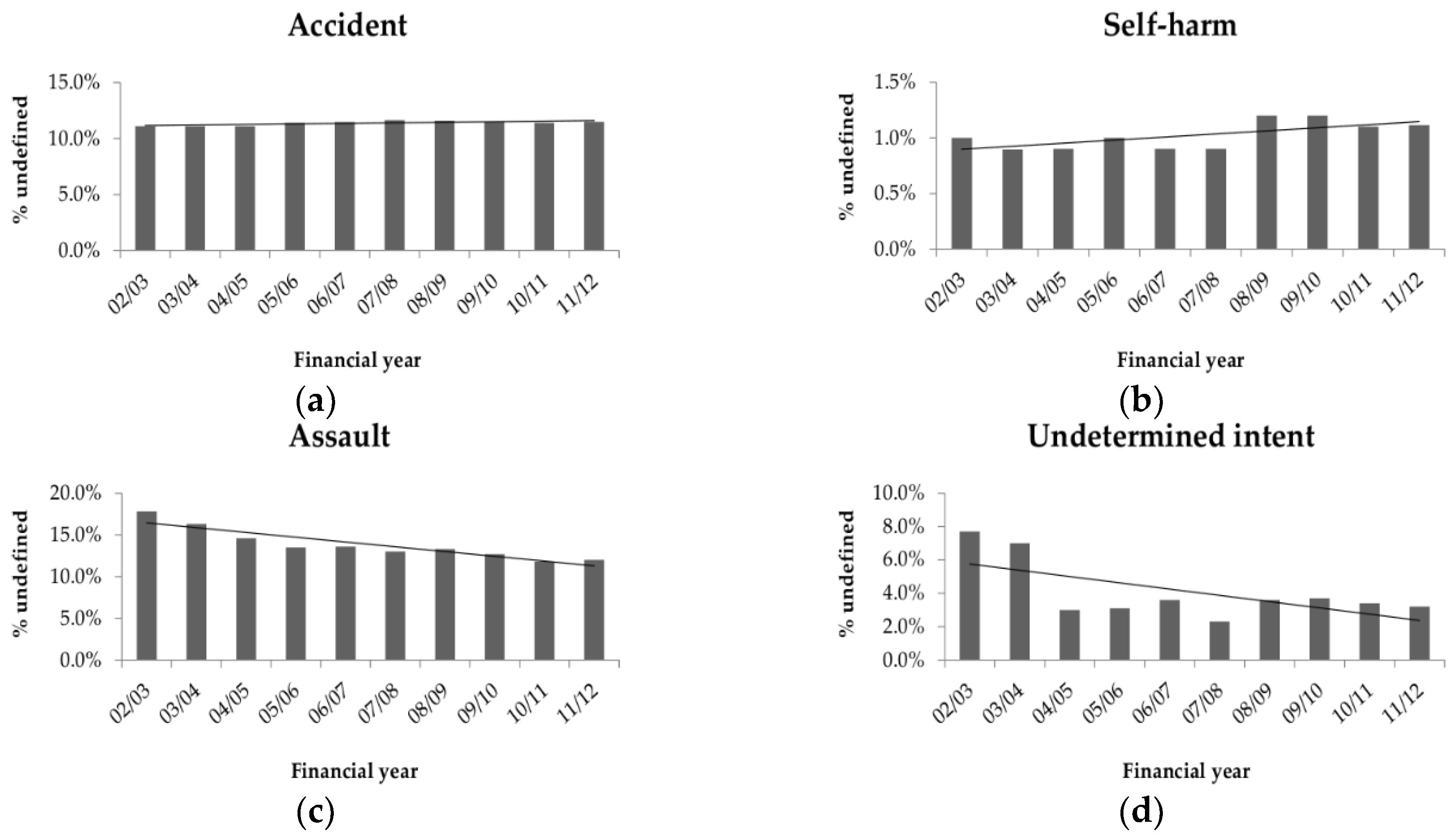
3.2. Changing Specificity of External Cause Codes
3.3. Specificity of Place Codes
3.4. Changing Specificity of Place Codes
3.5. Specificity of Activity Codes
3.6. Changing Specificity of Activity Codes
3.7. Changing Specificity by Hospital and Patient Characteristics
4. Discussion
5. Conclusions
Key Messages
- The specificity of injury data describing causes of injuries, where injuries occur and what activities people are undertaking at the time when injuries occur affects our ability to appropriately target injury prevention policy and practice.
- Previous Australian research quantified the level of specificity in injury hospitalization data with considerably poor specificity for some major intent categories (unintentional injuries and assaults), mechanisms (falls, burns, and poisonings), and for activity and place codes.
- As injury hospitalization data are a critical epidemiological tool for directing injury prevention policy and practice in Australia, it is important to understand the strengths and weaknesses of these data and identify any improvements or deteriorations in these data over time.
- This research identified the key areas where there was considerably poor specificity and/or where there was a highly significant reduction in the level of specificity of codes over time.
- Discrepancies in the specificity of data by subgroups was identified, including by jurisdiction, sector, location, age, sex, and intent, suggesting certain subgroups may require more attention to improve external cause data quality overall.
- Key focal areas where there was significant and worsening deficiencies in data specificity included the mechanisms of falls, firearms, sharp objects, drowning, forces of nature, and poisonings, and the subgroups of private hospitals, remote hospitals, and patients over 60 years of age.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Australian Burden of Disease Study: Fatal Burden of Disease 2010; Australian burden of disease study series No. 1. Cat. No. Bod 1.; AIHW: Canberra, Australia, 2015.
- World Health Organisation. Who Injury Surveillance Guidelines; World Health Organisation: Geneva, Switzerland, 2001. [Google Scholar]
- Annest, J.L.; Fingerhut, L.A.; Gallagher, S.S.; Grossman, D.C.; Hedegaard, H.; Johnson, R.; Kohn, M.; Pickett, D.; Thomas, K.E.; Trent, R.B. Strategies to improve external cause-of-injury coding in state-based hospital discharge and emergency department data systems: Recommendations of the cdc workgroup for improvement of external cause-of-injury coding. MMWR 2008, 57, 1–15. [Google Scholar] [PubMed]
- McKenzie, K.; Fingerhut, L.; Walker, S.; Harrison, A.; Harrison, J. Classifying external causes of injury: History, current approaches, and future directions. Epidemiol. Rev. 2012, 34, 4–16. [Google Scholar] [CrossRef] [PubMed]
- National Centre of Classification in Health (NCCH). The International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM), 9th ed.; University of Sydney: Sydney, Australia, 2015. [Google Scholar]
- Langley, J.; Stephenson, S.; Thorpe, C.; Davie, G. Accuracy of injury coding under icd-9 for new zealand public hospital discharges. Inj. Prev. 2006, 12, 58–61. [Google Scholar] [CrossRef] [PubMed]
- LeMier, M.; Cummings, P.; West, T.A. Accuracy of external cause of injury codes reported in washington state hospital discharge records. Inj. Prev. 2001, 7, 334–338. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, C.R.; Ackland, M.J.; Chandraraj, E.J. Accuracy of injury coding in victorian hospital morbidity data. Aust. N. Z. J. Public Health 1997, 27, 779–783. [Google Scholar]
- Langlois, J.A.; Buechner, J.S.; O’Connor, E.A.; Nacar, E.Q.; Smith, G.S. Improving the E coding of hospitalizations for injury: Do hospital records contain adequate documentation? Am. J. Public Health 1995, 85, 1261–1265. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M.; Colwell, L.S.; Sniezek, J.E. An evaluation of external cause-of-injury codes using hospital records from the indian health service, 1985. Am. J. Public Health 1990, 80, 279–281. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, K.; Enraght-Moony, E.; Walker, S.; McClure, R.; Harrison, J. Accuracy of external cause of injury coding in hospital records. Inj. Prev. 2009, 15, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Bergstrom, M.F.; Byberg, L.; Melhus, H.; Michaelsson, K.; Gedeborg, R. Extent and consequences of misclassified injury diagnoses in a national hospital discharge registry. Inj. Prev. 2011, 17, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Langley, J.; Davie, G.; Simpson, J. Quality of hospital discharge data for injury prevention. Inj. Prev. 2007, 13, 42–44. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, K.; Harding, L.F.; Walker, S.M.; Harrison, J.E.; Enraght-Moony, E.L.; Waller, G.S. The quality of national data on injuries requiring hospitalisation. Med. J. Aust. 2006, 185, 526. [Google Scholar] [PubMed]
- Soo, I.; Lam, M.; Rust, J.; Madden, R. Do we have enough information? How ICD-10-AM activity codes measure up. Health Inf. Manag. J. 2009, 38, 22–34. [Google Scholar]
- Finch, C.; Boufous, S. Do inadequacies in ICD-10-AM activity coded data lead to underestimates of the population frequency of sports/leisure injuries? Inj. Prev. 2008, 14, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Finch, C.F.; Boufous, S. Activity and place—Is it necessary both to identify sports and leisure injury cases in icd-coded data? Int. J. Inj. Control Saf. Promot. 2008, 15, 119–121. [Google Scholar] [CrossRef] [PubMed]
- National Casemix and Classification Centre. ICD-10-AM/ACHI/ACS Chronicle: Chronicle of Changes, 1st ed.–8th ed.; University of Wollongong: Wollongong, Australia, 2013. [Google Scholar]
- National Public Health Partnership (NPHP). The National Injury Prevention and Safety Promotion Plan: 2004–2014; NPHP: Canberra, Australia, 2004.
- McKenzie, K.; Enraght-Moony, E.; Harding, L.; Walker, S.; Waller, G.; Chen, L. Coding external causes of injuries: Problems and solutions. Accid. Anal. Prev. 2008, 40, 714–718. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| ICD-10-AM Code | ICD-10-AM Description | Number of Separations | Percent of Injuries | Undefined Codes | Undefined Codes N | Undefined Codes % | Percent Change 1 |
|---|---|---|---|---|---|---|---|
| Major intent blocks | |||||||
| V00–X59 | Accidents | 3,688,537 | 87.2% | X58, X59 | 420,227 | 11.4% | 0.4% * |
| X60–X84 | Intentional self-harm | 257,788 | 6.1% | X83, X84 | 2645 | 1.0% | 0.1% |
| X85–Y09 | Assault | 233,341 | 5.5% | Y08, Y09 | 32,132 | 11.4% | −5.8% * |
| Y10–Y34 | Event of undetermined intent | 48,727 | 1.2% | Y33, Y34 | 1813 | 3.7% | −4.5% * |
| Accident mechanism blocks | |||||||
| V00–V99 | Transport (all) | 574,567 | 13.6% | V98, V99 | 5187 | 0.9% | −0.9% * |
| V00–V09 | Transport: Pedestrians | 42,587 | 1.0% | V09 | 4447 | 10.4% | −6.8% ** |
| V10–V19 | Transport: Pedal cyclist | 96,213 | 2.3% | V19 | 22,509 | 23.4% | −11.6% ** |
| V20–V29 | Transport: Motorcycle rider | 142,984 | 3.4% | V29 | 28,993 | 20.3% | −6.1% * |
| V30–V39 | Transport: Three-wheeled occupant | 767 | 0.02% | V39 | 153 | 19.9% | −4.6% |
| V40–V49 | Transport: Car occupant | 196,830 | 4.6% | V49 | 14,813 | 7.5% | −4.2% * |
| V50–V59 | Transport: Pick up truck/van occupant | 5456 | 0.1% | V59 | 795 | 14.6% | −6.6% * |
| V60–V69 | Transport: Heavy transport occupant | 8329 | 0.2% | V69 | 1342 | 16.1% | −12.3% ** |
| V70–V79 | Transport: Bus occupant | 4978 | 0.1% | V79 | 988 | 19.8% | −12.4% ** |
| V80–V89 | Transport: Other land transport | 59,464 | 1.4% | V87.7–V87.9, V88.7–V88.9, V89 | 7261 | 12.2% | 4.1% * |
| V90–V94 | Transport: Water transport | 9940 | 0.2% | V94 | 2730 | 27.5% | 4.5% |
| V95–V97 | Transport: Air and space transport | 1832 | 0.04% | V95.8, V95.9, V96.80, V96.9, V97.0, V97.8 | 423 | 23.1% | 17.6% ** |
| W00–W19 | Falls | 1,590,974 | 37.6% | W17.8, W17.9, W18.8, W18.9, W19 | 665,123 | 41.8% | 1.5% * |
| W20–W49 | Inanimate mechanical forces | 617,361 | 14.6% | W49 | 35,868 | 5.8% | 4.2% * |
| W50–W64 | Animate mechanical forces | 150,088 | 3.6% | W64 | 2345 | 1.6% | −0.3% |
| W65–W74 | Drowning and submersion | 5236 | 0.1% | W73, W74 | 1445 | 27.6% | 20.1% ** |
| W75–W84 | Threats to breathing | 7859 | 0.2% | W83, W84 | 541 | 6.9% | 3.9% |
| W85–W99 | Electricity, radiation, temperature | 10,122 | 0.2% | W99 | 26 | 0.3% | 0.2% |
| X00–X09 | Smoke, fire, flames | 24,208 | 0.6% | X08, X09 | 6829 | 28.2% | −4.2% * |
| X10–X19 | Heat and hot substances | 39,765 | 0.9% | X19 | 3119 | 7.8% | 0.2% |
| X20–X29 | Venomous animals and plants | 34,668 | 0.8% | X27.8, X28, X29 | 610 | 1.8% | 1.3% * |
| X30–X39 | Forces of nature | 7188 | 0.2% | X39 | 451 | 6.3% | 11.4% ** |
| X40–X49 | Poisoning by noxious substances | 102,095 | 2.4% | X44, X47.8, X47.9, X49 | 42,802 | 41.9% | 5.0% * |
| X50–X57 | Overexertion, travel, privation | 104,179 | 2.5% | X57 | 67 | 0.1% | 0.0% |
| W00–X57 | Non-transport Accident (minor code blocks) | 2,693,743 | 63.7% | All of above | 759,226 | 28.2% | 3.6% * |
| Intentional self-harm blocks | |||||||
| X60–X69 | Poisoning by noxious substances | 212,481 | 5.0% | X64, X67.8, X67.9, X69 | 22,433 | 10.6% | −1.6% * |
| X71 | Drowning and submersion | 213 | 0.01% | X71.8, X71.9 | 42 | 19.7% | −12.6% |
| X72–X74 | Firearms | 473 | 0.01% | X74.9 | 121 | 25.6% | 12.0% |
| X78 | Sharp object | 32,596 | 0.8% | X78.8, X78.9 | 8551 | 26.2% | −5.9% * |
| X82 | Motor vehicle occupant | 700 | 0.02% | X82.2, X82.3, X82.8, X82.9 | 142 | 20.3% | 9.0% |
| X60–X82 | Intentional self-harm (minor code blocks) | 255,143 | 6.0% | All of above | 31,289 | 12.3% | −2.0% * |
| Assault blocks | |||||||
| X85–X90 | Poisoning by noxious substances | 781 | 0.02% | X89, X90 | 155 | 19.8% | 8.1% * |
| X92 | Drowning and submersion | 19 | 0.00% | X92.8, X92.9 | 1 | 5.3% | 0.0% |
| X93–X95 | Firearms | 1165 | 0.03% | X95.9 | 521 | 44.7% | 18.0% ** |
| X99 | Sharp object | 28,270 | 0.7% | X99.8, X99.9 | 7133 | 25.2% | 1.8% |
| Y03 | Motor vehicle occupant | 272 | 0.01% | Y03.2, Y03.3, Y03.8, Y03.9 | 237 | 87.1% | −9.1% |
| X85–Y07 | Assault (minor code blocks) | 201,209 | 4.76% | All of above | 8047 | 4.0% | 0.2% |
| Undetermined intent blocks | |||||||
| Y10–Y19 | Poisoning by noxious substances | 38,352 | 0.9% | Y14, Y17.8, Y17.9, Y19 | 7092 | 18.5% | 8.0% * |
| Y21 | Drowning and submersion | 80 | 0.00% | Y21.8, Y21.9 | 22 | 27.5% | 15.9% |
| Y22–Y24 | Firearms | 430 | 0.01% | Y24.9 | 221 | 51.4% | −2.2% |
| Y28 | Sharp object | 2837 | 0.07% | Y28.8, Y28.9 | 1041 | 36.7% | 13.8% ** |
| Y32 | Motor vehicle occupant | 17 | 0.00% | Y32.2, Y32.3, Y32.8, Y32.9 | 5 | 29.4% | 0.0% |
| Y10–Y32 | Undetermined intent (minor code blocks) | 46,914 | 1.1% | All of above | 8381 | 17.9% | 4.3% * |
| ICD-10-AM Code | ICD-10-AM Description | Number of Separations | Percent of Injuries | Undefined Codes | Undefined Codes N | Undefined Codes % | Percent Change 1 |
|---|---|---|---|---|---|---|---|
| Place | |||||||
| Y92 | Place (major code block) | 4,224,439 | – | Y92.88, Y92.9 | 1,800,725 | 42.6% | 2.0% * |
| Y92.0 | Home | 1,118,683 | 26.5% | Y92.09 | 890,062 | 79.6% | −46.7% ** |
| Y92.1 | Residential institution | 207,203 | 4.9% | Y92.18, Y92.19 | 9515 | 4.6% | −1.3% * |
| Y92.2 | School, other institution, and public admin area | 133,993 | 3.2% | Y92.29 | 12,912 | 9.6% | −1.4% * |
| Y92.3 | Sports and athletic area | 218,095 | 5.2% | Y92.38, Y92.39 | 24,685 | 11.3% | 2.1% * |
| Y92.4 | Street and highway | 422,691 | 10.0% | Y92.48, Y92.49 | 102,772 | 24.3% | 75.3% ** |
| Y92.5 | Trade and service area | 125,915 | 3.0% | Y92.58, Y92.59 | 24,392 | 19.4% | 4.5% * |
| Y92.6 | Industrial and construction area | 66,420 | 1.6% | Y92.68, Y92.69 | 17,719 | 26.7% | −6.7% * |
| Y92.0–Y92.7 | Place (minor code blocks) | 2,423,714 | – | All of the above | 1,082,057 | 44.6% | −9.7% * |
| Activity | |||||||
| U50–U73 | Activity(major code block) | 4,221,759 | – | U73.8, U73.9 | 3,043,973 | 72.1% | −2.1% * |
| U50–U72 | Sports or leisure | 529,921 | 12.5% | U70–U72 | 124,937 | 23.6% | 6.6% * |
| U73.0 | Working | 262,269 | 6.2% | U73.08,U73.09 | 146,699 | 55.9% | 7.1% * |
| U50–U73.2 | Activity (minor code blocks) | 1,177,786 | – | All of the above | 271,636 | 23.1% | 3.4% * |
| Characteristic | Number of Separations | Percent of Injuries | Undefined Codes N | Undefined Codes % | Change 1 |
|---|---|---|---|---|---|
| Hospital jurisdiction | |||||
| ACT | 60,673 | 1.4% | 16,933 | 27.9% | −5.1% * |
| NSW | 1,344,254 | 32.0% | 438,910 | 32.7% | 2.2% * |
| NT | 61,606 | 1.5% | 13,159 | 21.4% | 3.2% * |
| Qld | 882,381 | 21.0% | 277,685 | 31.5% | 2.0% * |
| SA | 317,182 | 7.5% | 105,281 | 33.2% | 1.6% * |
| Tas | 67,652 | 1.6% | 16,959 | 25.1% | 0.1% |
| Vic | 1,056,832 | 25.0% | 349,430 | 33.1% | 1.5% * |
| WA | 412,777 | 9.8% | 130,318 | 31.6% | 4.7% * |
| Hospital location | |||||
| Major cities | 2,366,884 | 65.7% | 630,770 | 26.6% | 2.1% * |
| Inner regional | 729,180 | 20.2% | 203,583 | 27.9% | 0.8% * |
| Outer regional | 399,939 | 11.1% | 112,788 | 28.2% | 0.1% |
| Remote | 58,197 | 1.6% | 17,056 | 29.3% | 1.2% |
| Very remote | 46,880 | 1.3% | 16,979 | 36.2% | 5.7% * |
| Hospital sector | |||||
| Public | 3,601,080 | 85.2% | 981,176 | 27.2% | 1.5% * |
| Private | 627,313 | 14.8% | 381,104 | 60.8% | 8.6% * |
| Patient age | |||||
| 0–14years | 637,512 | 15.1% | 166,397 | 26.1% | −2.0% * |
| 15–29 years | 1,004,699 | 23.8% | 264,222 | 26.3% | 0.5% |
| 30–44 years | 758,935 | 17.9% | 204,089 | 26.9% | 1.9% * |
| 45–60 years | 589,398 | 13.9% | 175,550 | 29.8% | 2.0% * |
| 60+ years | 1,237,821 | 29.3% | 552,015 | 44.6% | 1.1% * |
| Patient gender | |||||
| Female | 1,790,463 | 42.3% | 631,564 | 35.3% | 2.3% * |
| Male | 2,437,880 | 57.7% | 730,704 | 30.0% | 1.7% * |
| External cause | |||||
| Accidents | 3,688,537 | 87.2% | 1,277,973 | 34.6% | 2.5% * |
| Intentional self-harm | 257,788 | 6.1% | 33,934 | 13.2% | −2.0% * |
| Assault | 233,341 | 5.5% | 40,179 | 17.2% | −5.6% * |
| Event of undetermined intent | 48,727 | 1.2% | 10,194 | 20.9% | 0.3% |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vallmuur, K.; Watson, A. Evaluating the Specificity of Community Injury Hospitalization Data over Time. Safety 2016, 2, 6. https://doi.org/10.3390/safety2010006
Vallmuur K, Watson A. Evaluating the Specificity of Community Injury Hospitalization Data over Time. Safety. 2016; 2(1):6. https://doi.org/10.3390/safety2010006
Chicago/Turabian StyleVallmuur, Kirsten, and Angela Watson. 2016. "Evaluating the Specificity of Community Injury Hospitalization Data over Time" Safety 2, no. 1: 6. https://doi.org/10.3390/safety2010006
APA StyleVallmuur, K., & Watson, A. (2016). Evaluating the Specificity of Community Injury Hospitalization Data over Time. Safety, 2(1), 6. https://doi.org/10.3390/safety2010006