
Inter- and Intra-Observer Variability and the Effect of Experience in Cine-MRI for Adhesion Detection
 ,
,  , , , , and
, , , , and
Abstract
1. Introduction
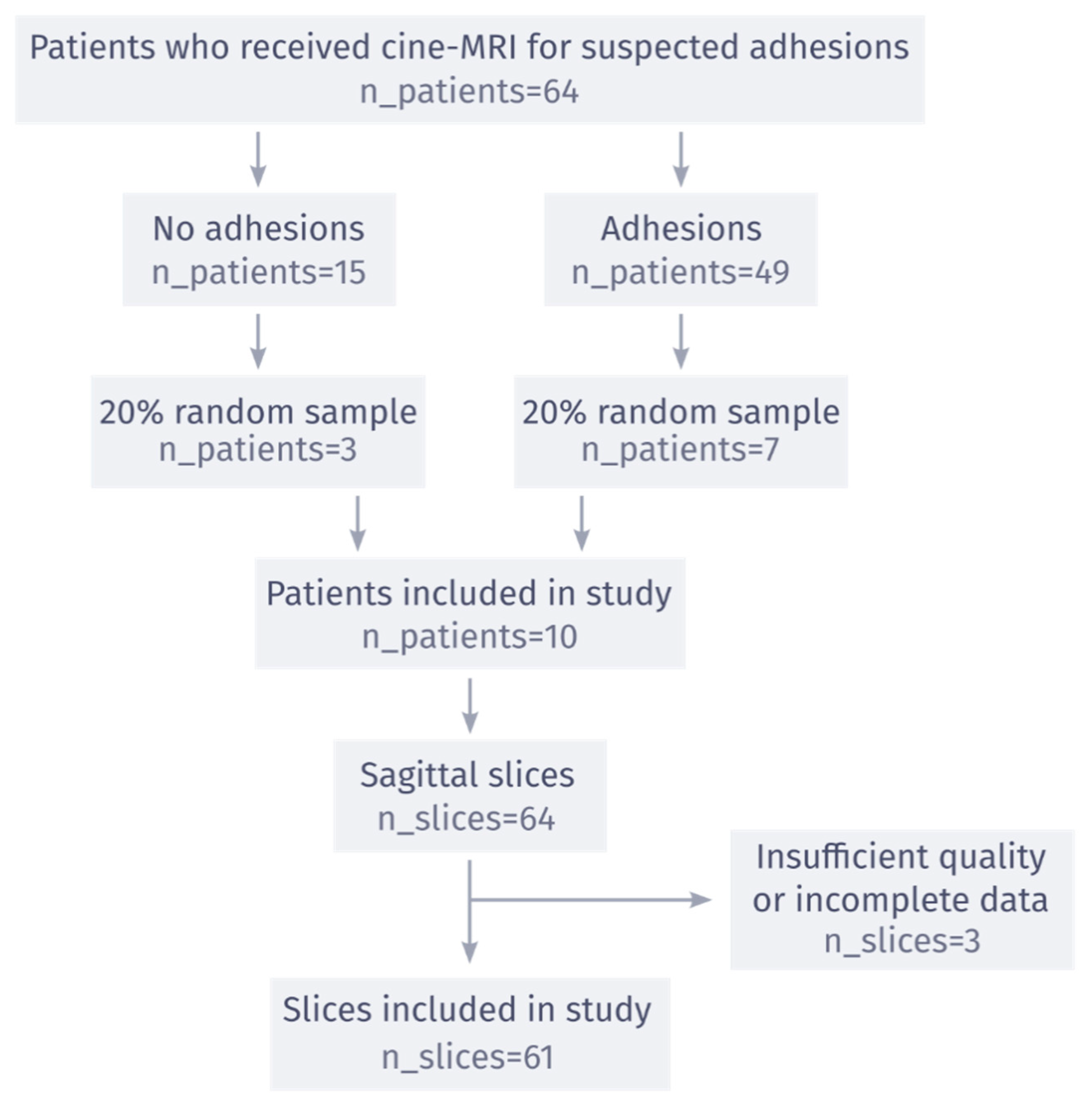
2. Materials and Methods
3. Results
4. Discussion
4.1. Comparison with the Literature
4.2. Limitations
4.3. Future Perspective
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bruce, J.; Krukowski, Z.H. Quality of Life and Chronic Pain Four Years After Gastrointestinal Surgery. Dis. Colon Rectum 2006, 49, 1362–1370. [Google Scholar] [CrossRef]
- Sperber, A.D.; Morris, C.B.; Greemberg, L.; Bangdiwala, S.I.; Goldstein, D.; Sheiner, E.; Rusabrov, Y.; Hu, Y.; Katz, M.; Freud, T.; et al. Development of Abdominal Pain and IBS Following Gynecological Surgery: A Prospective, Controlled Study. Gastroenterology 2008, 134, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Broek, R.P.G.T.; Issa, Y.; Van Santbrink, E.J.P.; Bouvy, N.D.; Kruitwagen, R.F.; Jeekel, J.; Bakkum, E.A.; Rovers, M.; Van Goor, H. Burden of adhesions in abdominal and pelvic surgery: Systematic review and met-analysis. BMJ 2013, 347, f5588. [Google Scholar] [CrossRef] [PubMed]
- Bojahr, B.; Römer, T.; Lober, R. The value of laparoscopy in diagnosis and therapy in patients with chronic pelvic pain. Zentralbl. Gynakol. 1995, 117, 304–309. [Google Scholar] [PubMed]
- Cheong, Y.C.; Reading, I.; Bailey, S.; Sadek, K.; Ledger, W.; Li, T.C. Should women with chronic pelvic pain have adhesiolysis? BMC Women’s Health 2014, 14, 36. [Google Scholar] [CrossRef] [PubMed]
- Swank, D.; Swank-Bordewijk, S.; Hop, W.; van Erp, W.; Janssen, I.; Bonjer, H.; Jeekel, J. Laparoscopic adhesiolysis in patients with chronic abdominal pain: A blinded randomised controlled multi-centre trial. Lancet 2003, 361, 1247–1251. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.A.; Buhmann, S.; Hopman, A.; Steitz, H.-O.; Lienemann, A.; Reiser, M.F.; Jauch, K.-W.; Hüttl, T.P. Cine-MRI detection of intraabdominal adhesions: Correlation with intraoperative findings in 89 consecutive cases. Surg. Endosc. 2008, 22, 2455–2461. [Google Scholar] [CrossRef] [PubMed]
- Langbach, O.; Holmedal, S.H.; Grandal, O.J.; Røkke, O. Adhesions to Mesh after Ventral Hernia Mesh Repair Are Detected by MRI but Are Not a Cause of Long Term Chronic Abdominal Pain. Gastroenterol. Res. Pract. 2015, 2016, e2631598. [Google Scholar] [CrossRef] [PubMed]
- Beukel, B.A.W.V.D.; Stommel, M.; van Leuven, S.; Strik, C.; Ijsseldijk, M.; Joosten, F.; van Goor, H.; Broek, R.T. A Shared Decision Approach to Chronic Abdominal Pain Based on Cine-MRI: A Prospective Cohort Study. Am. J. Gastroenterol. 2018, 113, 1229–1237. [Google Scholar] [CrossRef] [PubMed]
- Gerner-Rasmussen, J.; Donatsky, A.M.; Bjerrum, F. The role of non-invasive imaging techniques in detecting intra-abdominal adhesions: A systematic review. Langenbeck’s Arch. Surg. 2018, 404, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Kirchhoff, S.; Ladurner, R.; Mussack, T.; Reiser, M.F.; Lienemann, A. Detection of recurrent hernia and intraabdominal adhesions following incisional hernia repair: A functional cine MRI-study. Abdom. Imaging 2009, 35, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Kirchhoff, S.; Nicolaus, M.; Schirra, J.; Reiser, M.F.; Göke, B.; Lienemann, A. Assessment of colon motility using simultaneous manometric and functional cine-MRI analysis: Preliminary results. Abdom. Imaging 2010, 36, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Lienemann, A.; Sprenger, D.; Steitz, H.O.; Korell, M.; Reiser, M. Detection and Mapping of Intraabdominal Adhesions by Using Functional Cine MR Imaging: Preliminary Results. Radiology 2000, 217, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Gallas, B.D.; Bandos, A.; Samuelson, F.W.; Wagner, R.F. A Framework for Random-Effects ROC Analysis: Biases with the Bootstrap and Other Variance Estimators. Commun. Stat.—Theory Methods 2009, 38, 2586–2603. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Zinther, N.B.; Zeuten, A.; Marinovskij, E.; Haislund, M.; Friis-Andersen, H. Detection of abdominal wall adhesions using visceral slide. Surg. Endosc. 2010, 24, 3161–3166. [Google Scholar] [CrossRef] [PubMed]
- Randall, D.; Joosten, F.; Broek, R.P.T.; Gillott, R.; Bardhan, K.D.; Strik, C.; Prins, W.; Van Goor, H.; Fenner, J.W. A novel diagnostic aid for intra-abdominal adhesion detection in cine-MRI: Pilot study and initial diagnostic impressions. Br. J. Radiol. 2017, 90, 20170158. [Google Scholar] [CrossRef] [PubMed]
- De Wilde, B.; ten Broek, R.P.; Huisman, H. Cine-MRI detection of abdominal adhesions with spatio-temporal deep learning. arXiv 2021, arXiv:210608094. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Observer | Years Experience | Cine Cases Reviewed | Adhesion Cases Reviewed | Clinical Significance Threshold |
|---|---|---|---|---|
| Observer 1 * | 4 | 30 | 30 | 40% |
| Observer 2 * | 30 | 100 | 100 | 80% |
| Observer 3 * | 0 | 0 | 0 | 60% |
| Observer 4 | 6 | 30 | 30 | 40% |
| Observer 5 | 15 | 100 | 0 | 20% |
| Observer 6 | 5 | 150 | 0 | 40% |
| Observer 7 | 7 | 50 | 50 | 80% |
| Observer 8 | 6 | 30 | 30 | 40% |
| Observer 9 | 17 | 0 | 0 | 0% |
| Observer 10 | 2 | 15 | 15 | 40% |
| Observer 11 | 2 | 0 | 0 | 0% |
| Observer 12 | 2 | 0 | 0 | 60% |
| Observer 13 | 3 | 0 | 0 | 60% |
| Observer 14 | 3 | 50 | 0 | 40% |
| Observer 15 | 4 | 20 | 20 | 60% |
| Group | Fleiss’ κ | % Agreement | AUC |
|---|---|---|---|
| consensus | 0.28 [0.10, 0.44] | 79.23 [74.32, 84.15] | - |
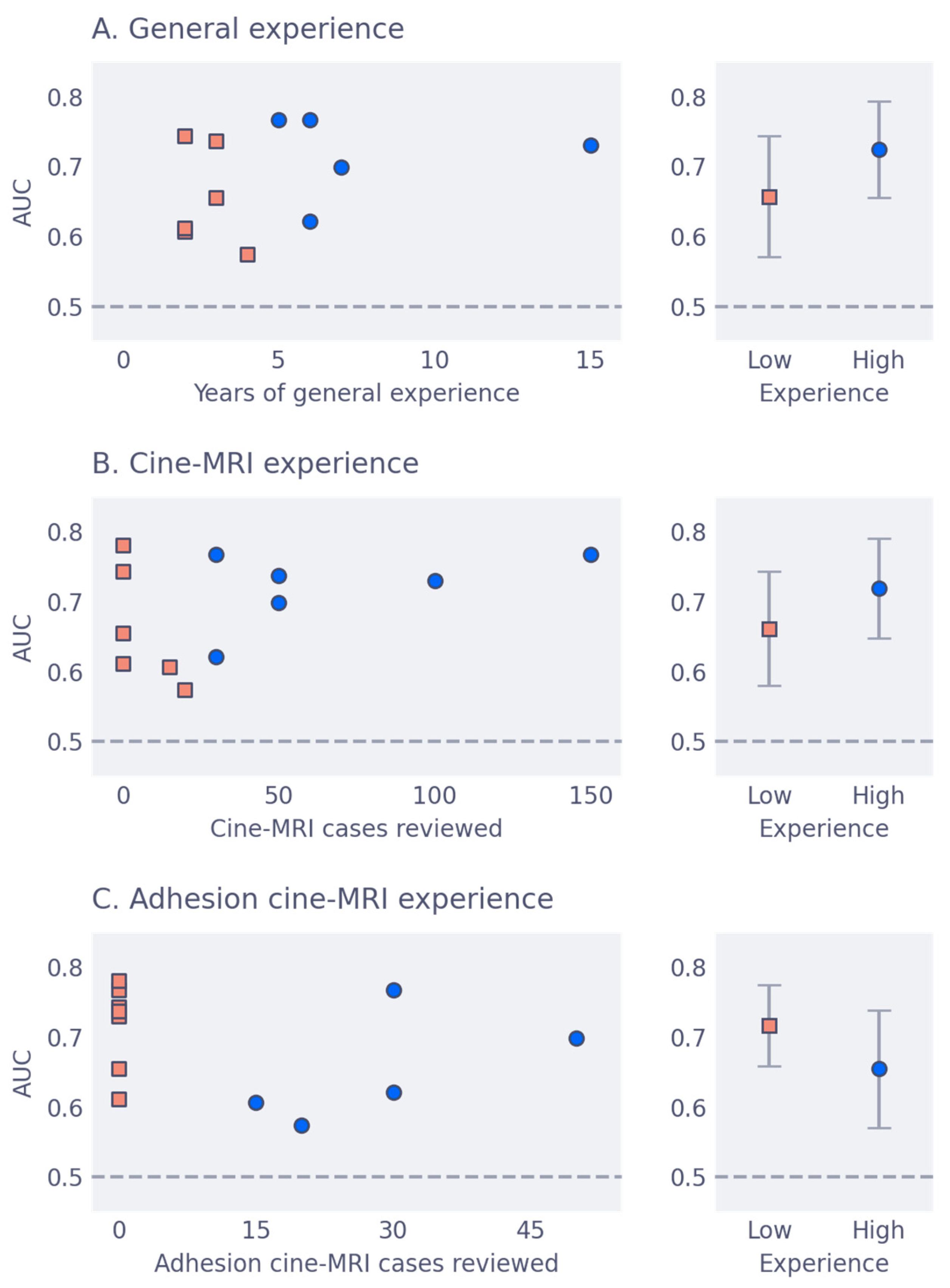
| low-year | 0.06 [−0.01, 0.13] | 56.28 [53.77, 58.91] | 0.66 [0.57, 0.74] |
| high-year | 0.34 [0.24, 0.42] | 67.10 [64.59, 69.62] | 0.72 [0.65, 0.79] |
| low-cine | 0.04 [−0.03, 0.11] | 56.28 [53.77, 58.91] | 0.66 [0.58, 0.74] |
| high-cine | 0.34 [0.24, 0.43] | 67.54 [65.03, 69.95] | 0.72 [0.65, 0.79] |
| low-adhesion | 0.15 [0.09, 0.21] | 57.53 [55.35, 59.72] | 0.72 [0.66, 0.78] |
| high-adhesion | 0.11 [0.02, 0.18] | 56.39 [53.11, 59.51] | 0.66 [0.57, 0.74] |
| Observer | Cohen’s κ | % Agreement |
|---|---|---|
| Observer 2 * | 0.44 [0.22, 0.64] | 78.69 [68.85, 86.89] |
| Observer 3 * | 0.37 [0.20, 0.55] | 75.41 [65.57, 83.61] |
| Observer 7 | 0.50 [0.29, 0.69] | 78.69 [70.49, 86.89] |
| Observer 4 | 0.53 [0.36, 0.68] | 75.41 [65.57, 83.61] |
| Observer 15 | −0.12 [−0.18, −0.06] | 75.41 [65.57, 83.61] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Wilde, B.; Joosten, F.; Venderink, W.; Davidse, M.E.J.; Geurts, J.; Kruijt, H.; Vermeulen, A.; Martens, B.; Schyns, M.V.P.; Huige, J.C.B.M.; et al. Inter- and Intra-Observer Variability and the Effect of Experience in Cine-MRI for Adhesion Detection. J. Imaging 2023, 9, 55. https://doi.org/10.3390/jimaging9030055
de Wilde B, Joosten F, Venderink W, Davidse MEJ, Geurts J, Kruijt H, Vermeulen A, Martens B, Schyns MVP, Huige JCBM, et al. Inter- and Intra-Observer Variability and the Effect of Experience in Cine-MRI for Adhesion Detection. Journal of Imaging. 2023; 9(3):55. https://doi.org/10.3390/jimaging9030055
Chicago/Turabian Stylede Wilde, Bram, Frank Joosten, Wulphert Venderink, Mirjam E. J. Davidse, Juliëtte Geurts, Hanneke Kruijt, Afke Vermeulen, Bibi Martens, Maxime V. P. Schyns, Josephine C. B. M. Huige, and et al. 2023. "Inter- and Intra-Observer Variability and the Effect of Experience in Cine-MRI for Adhesion Detection" Journal of Imaging 9, no. 3: 55. https://doi.org/10.3390/jimaging9030055
APA Stylede Wilde, B., Joosten, F., Venderink, W., Davidse, M. E. J., Geurts, J., Kruijt, H., Vermeulen, A., Martens, B., Schyns, M. V. P., Huige, J. C. B. M., de Boer, M. C., Tonino, B. A. R., Zandvoort, H. J. A., Lammert, K., Parviainen, H., Vuorinen, A.-M., Syväranta, S., Vogels, R. R. M., Prins, W., ... Huisman, H. (2023). Inter- and Intra-Observer Variability and the Effect of Experience in Cine-MRI for Adhesion Detection. Journal of Imaging, 9(3), 55. https://doi.org/10.3390/jimaging9030055