

SCOLIONET: An Automated Scoliosis Cobb Angle Quantification Using Enhanced X-ray Images and Deep Learning Models


Abstract
:
1. Introduction
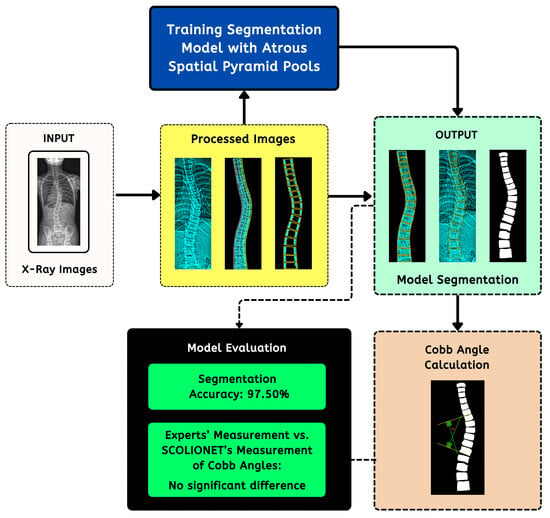
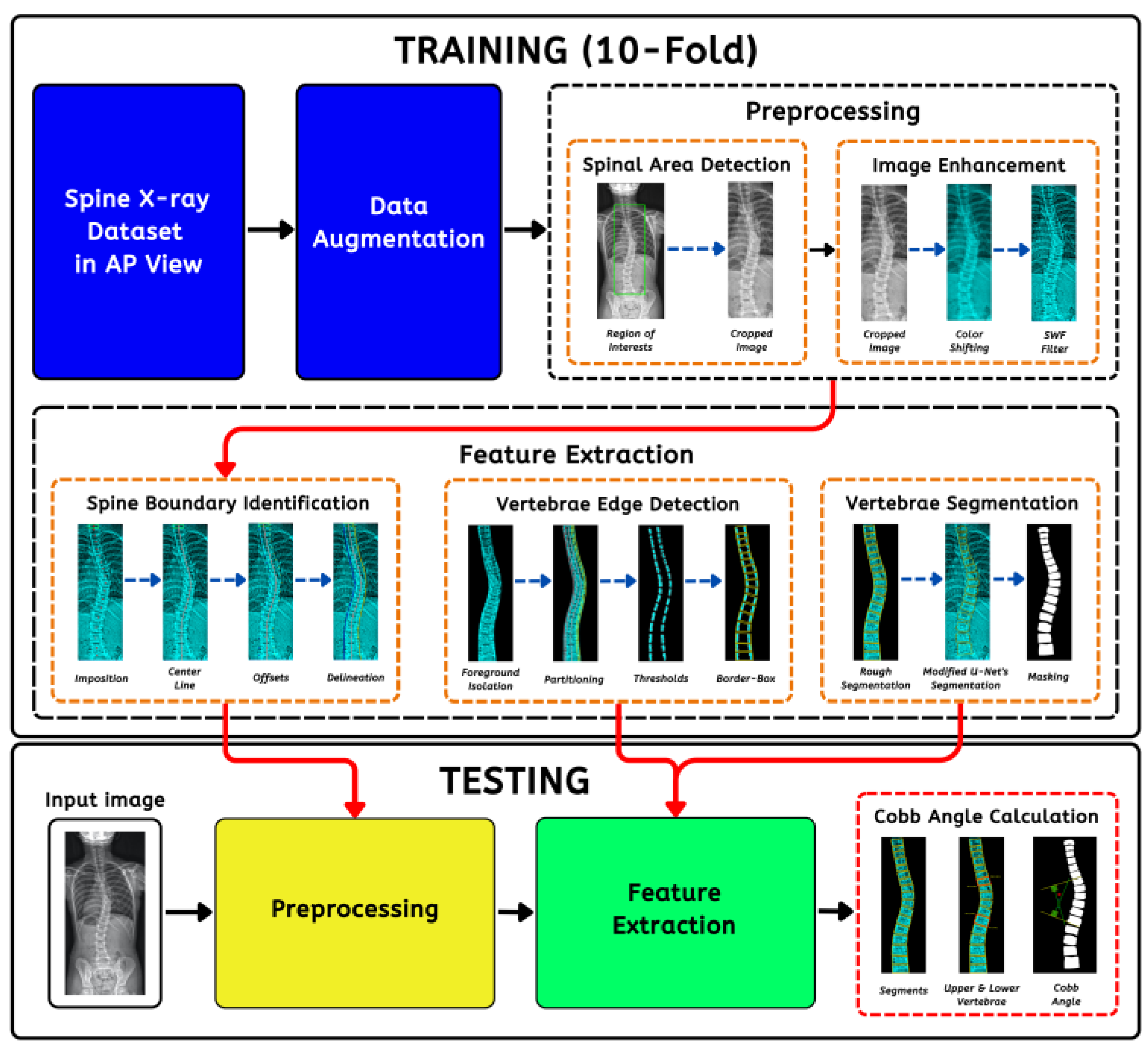
2. Methodology
2.1. Data Collection
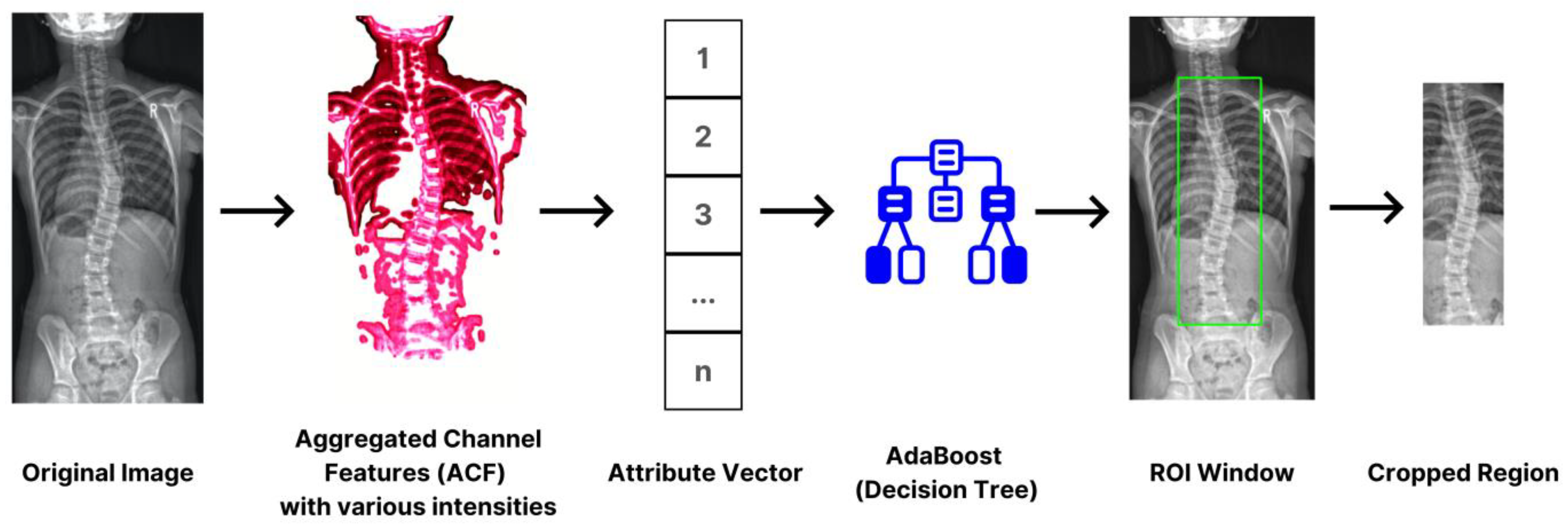
2.2. Spinal Region Isolation
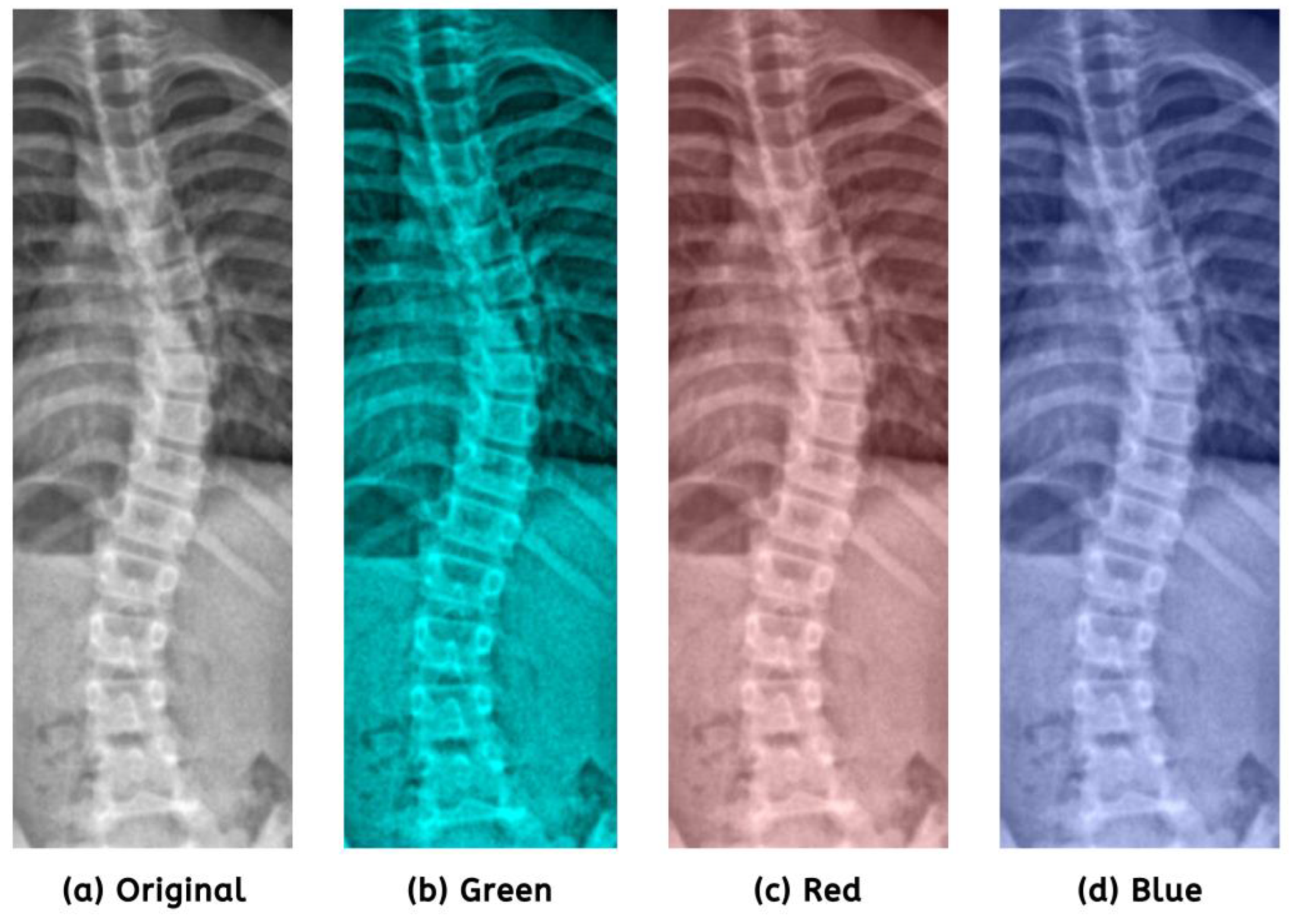
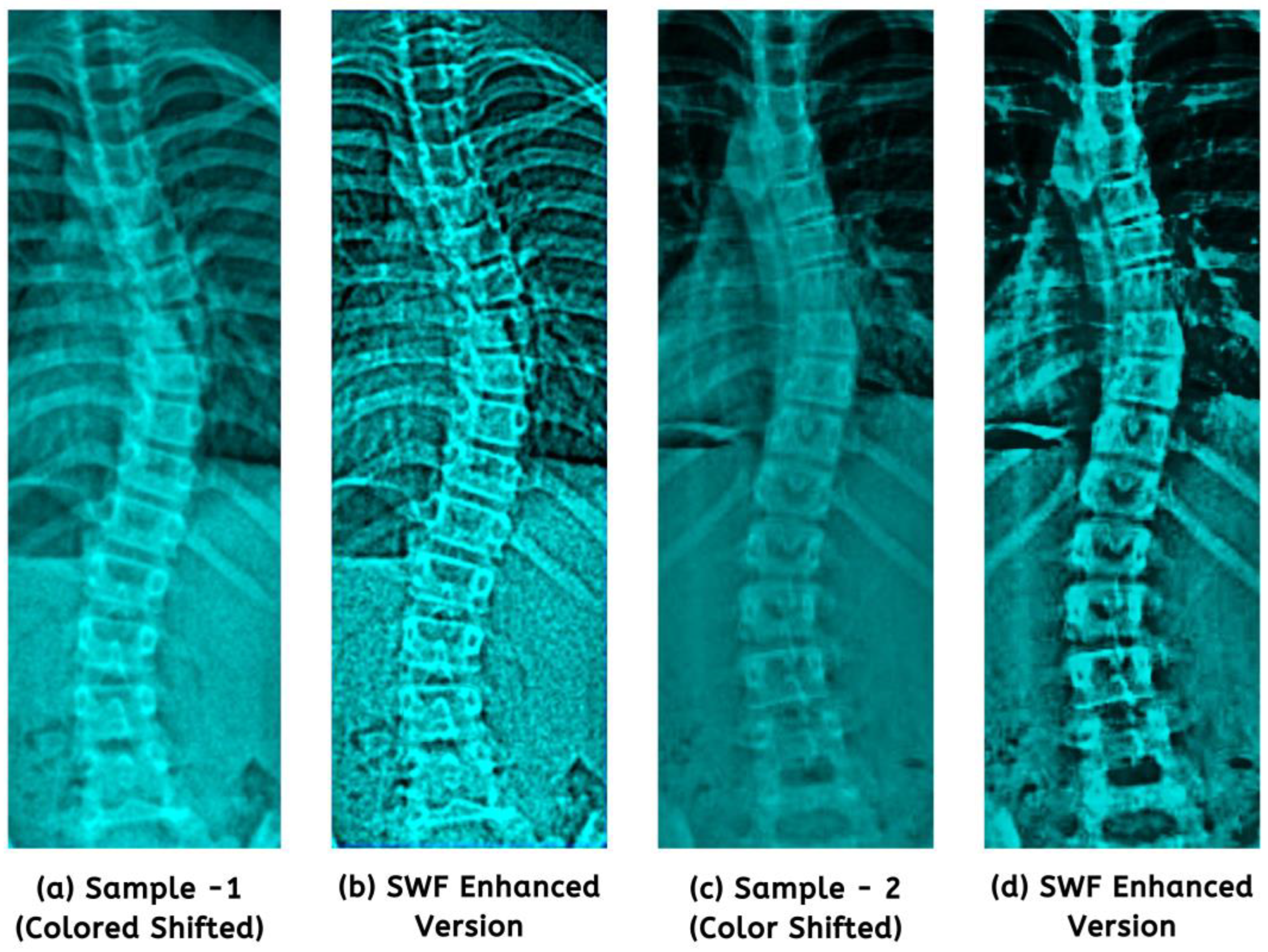
2.3. Color Standardization and Image Enhancement
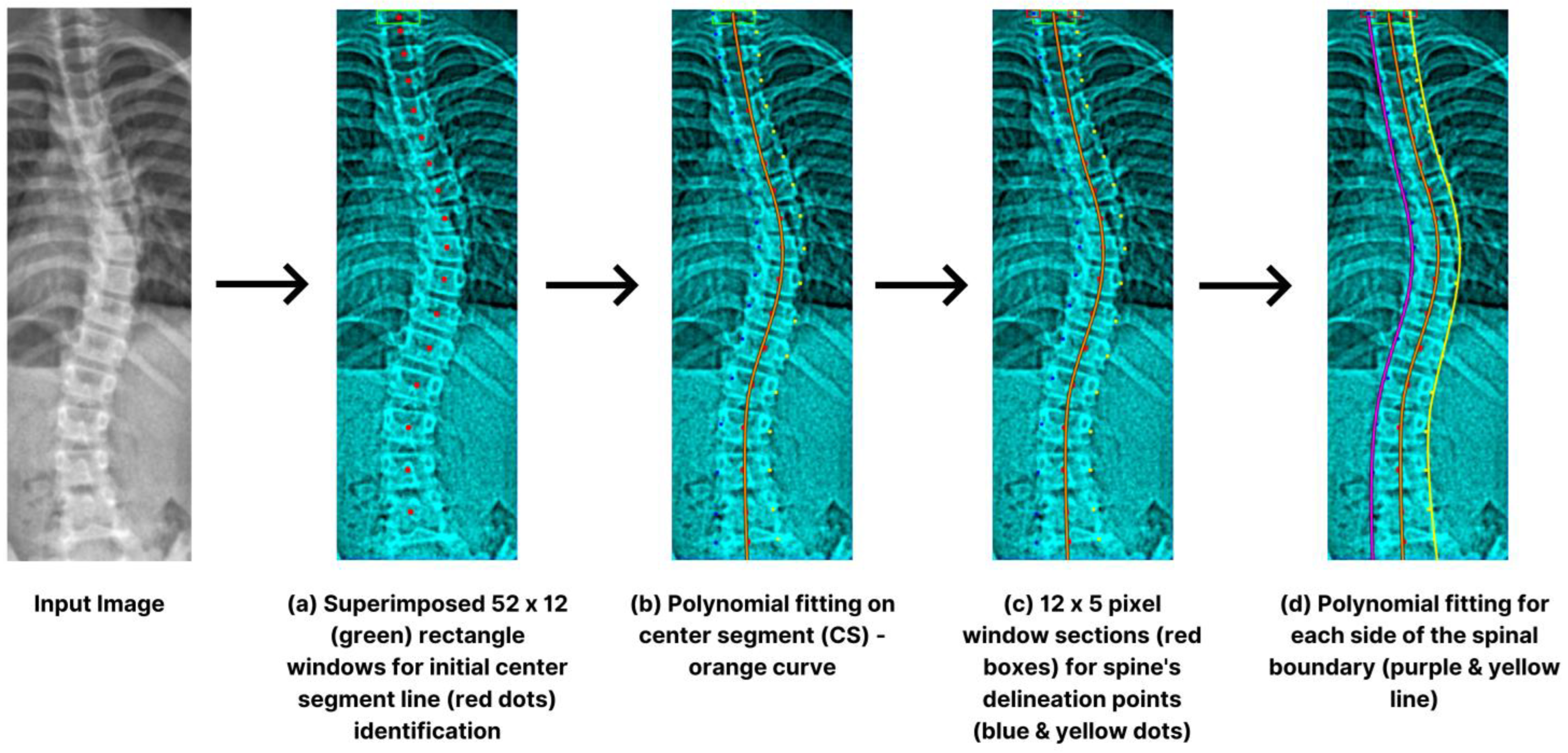
2.4. Spinal Boundary Detection
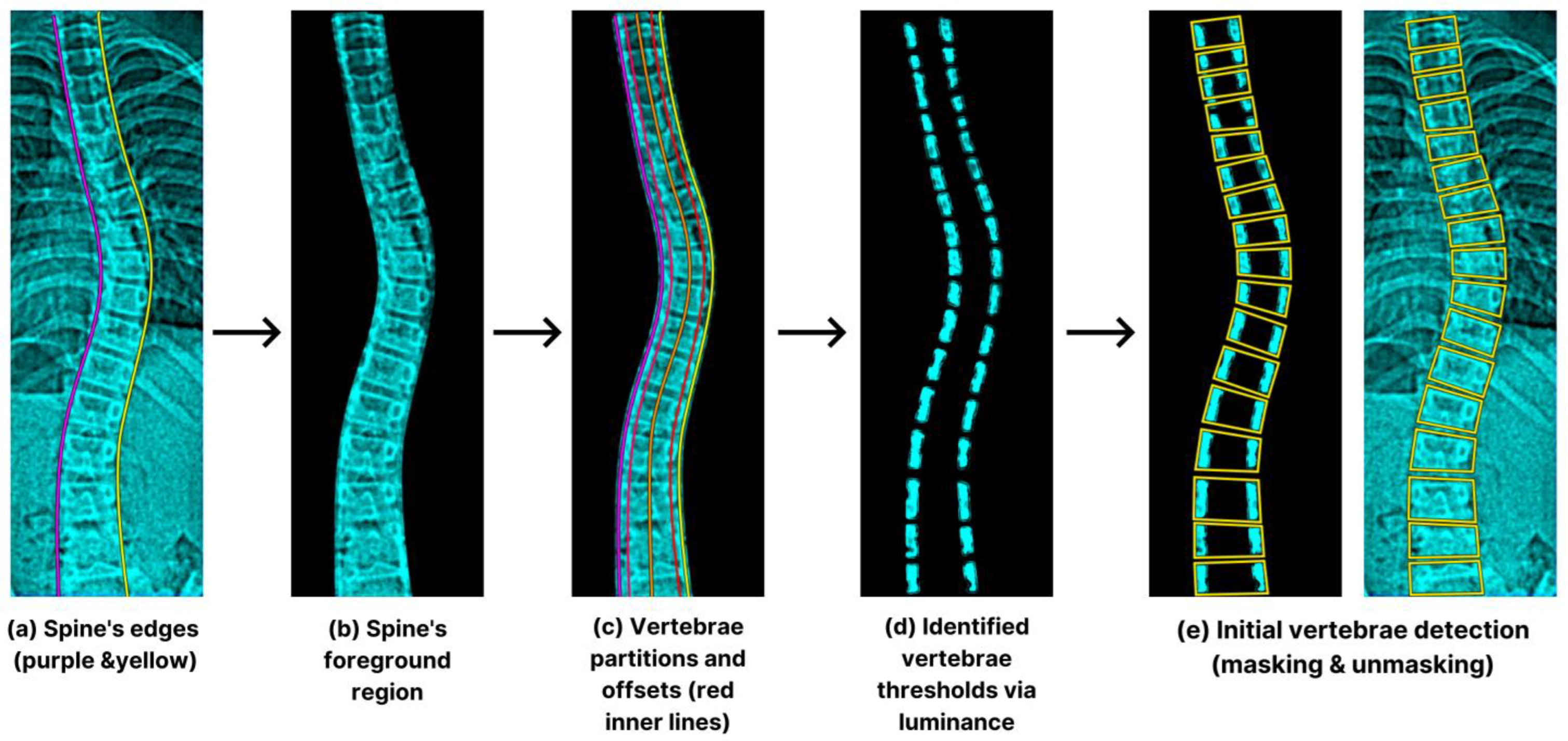
2.5. Initial Vertebra Identification
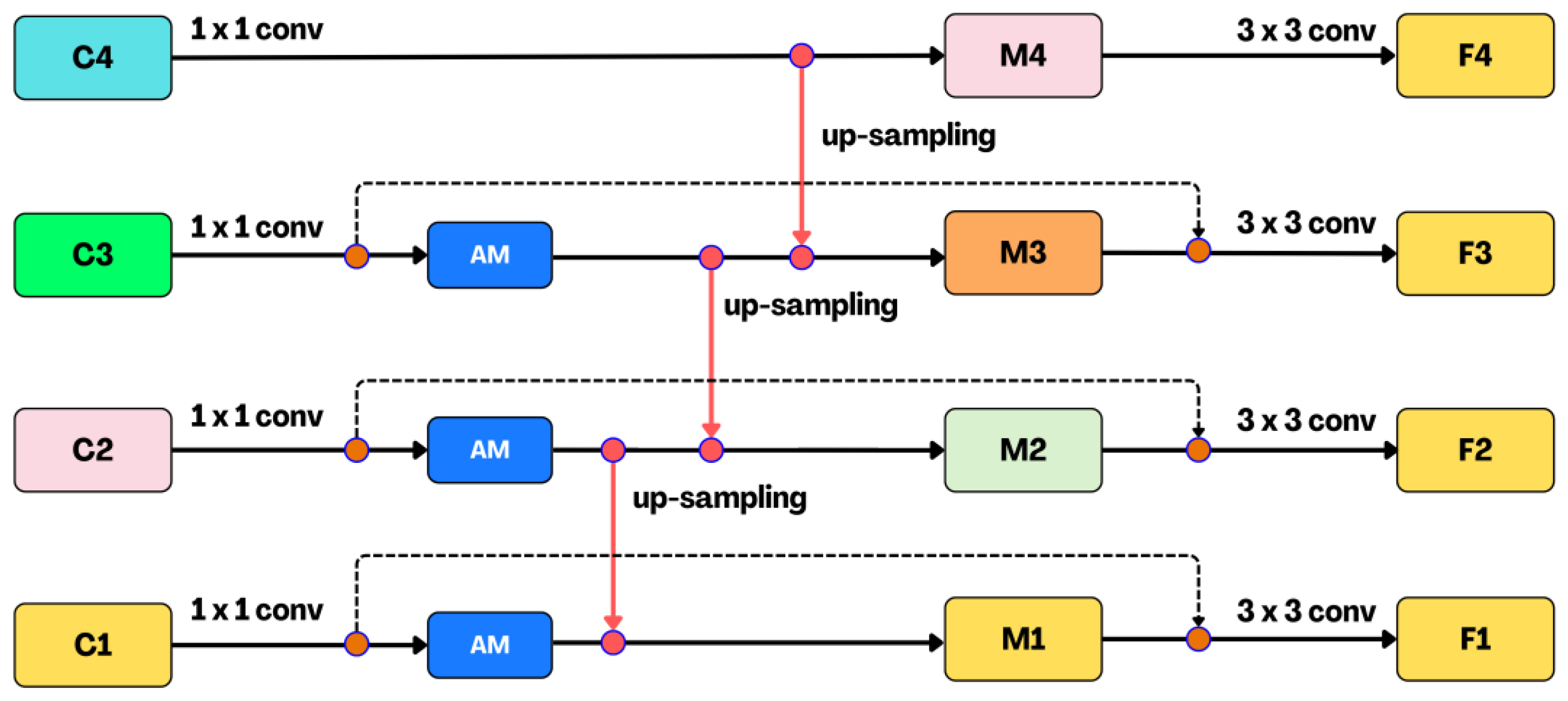
2.6. SCOLIONET’s Detailed Core Network Architecture
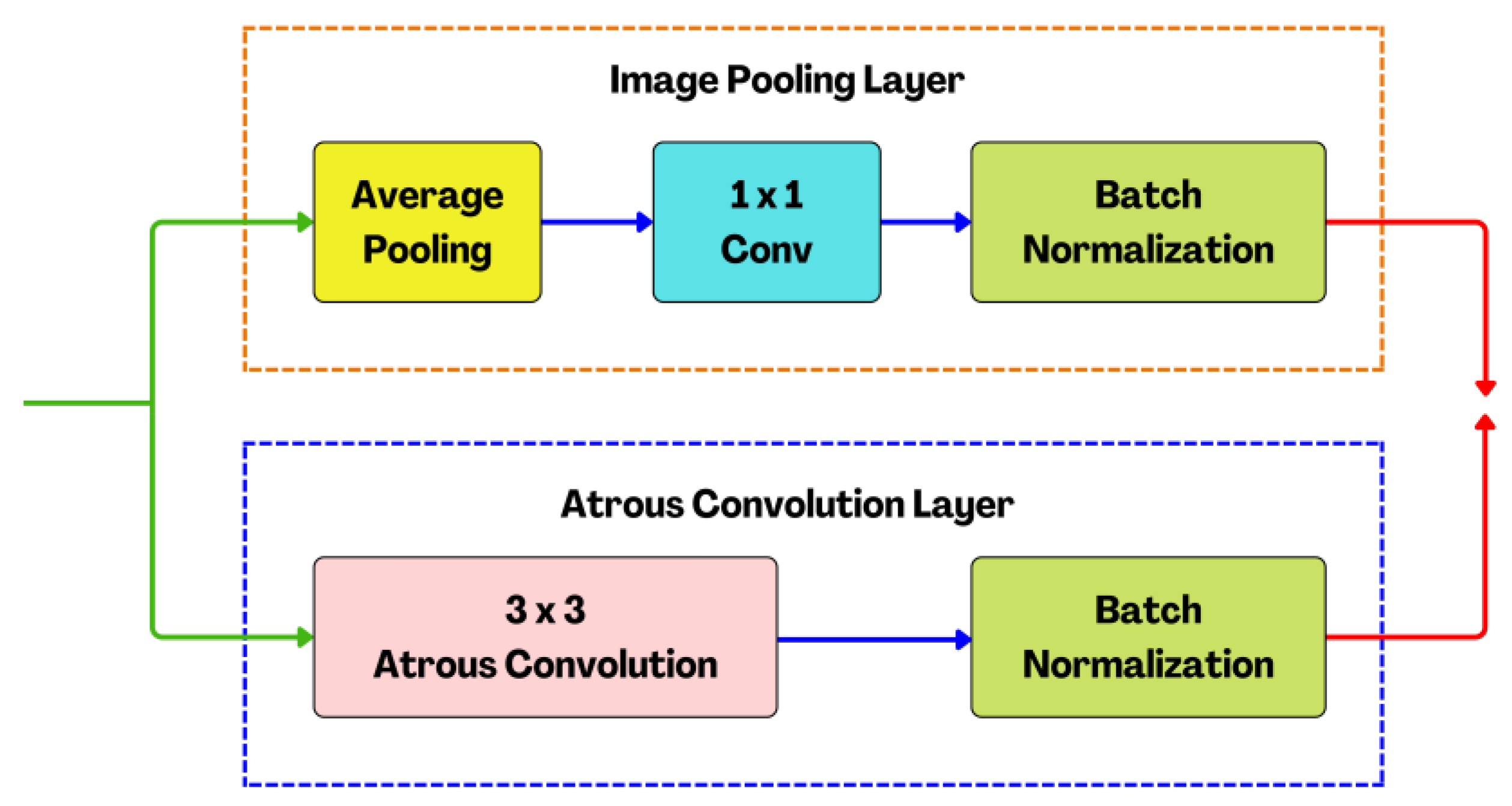
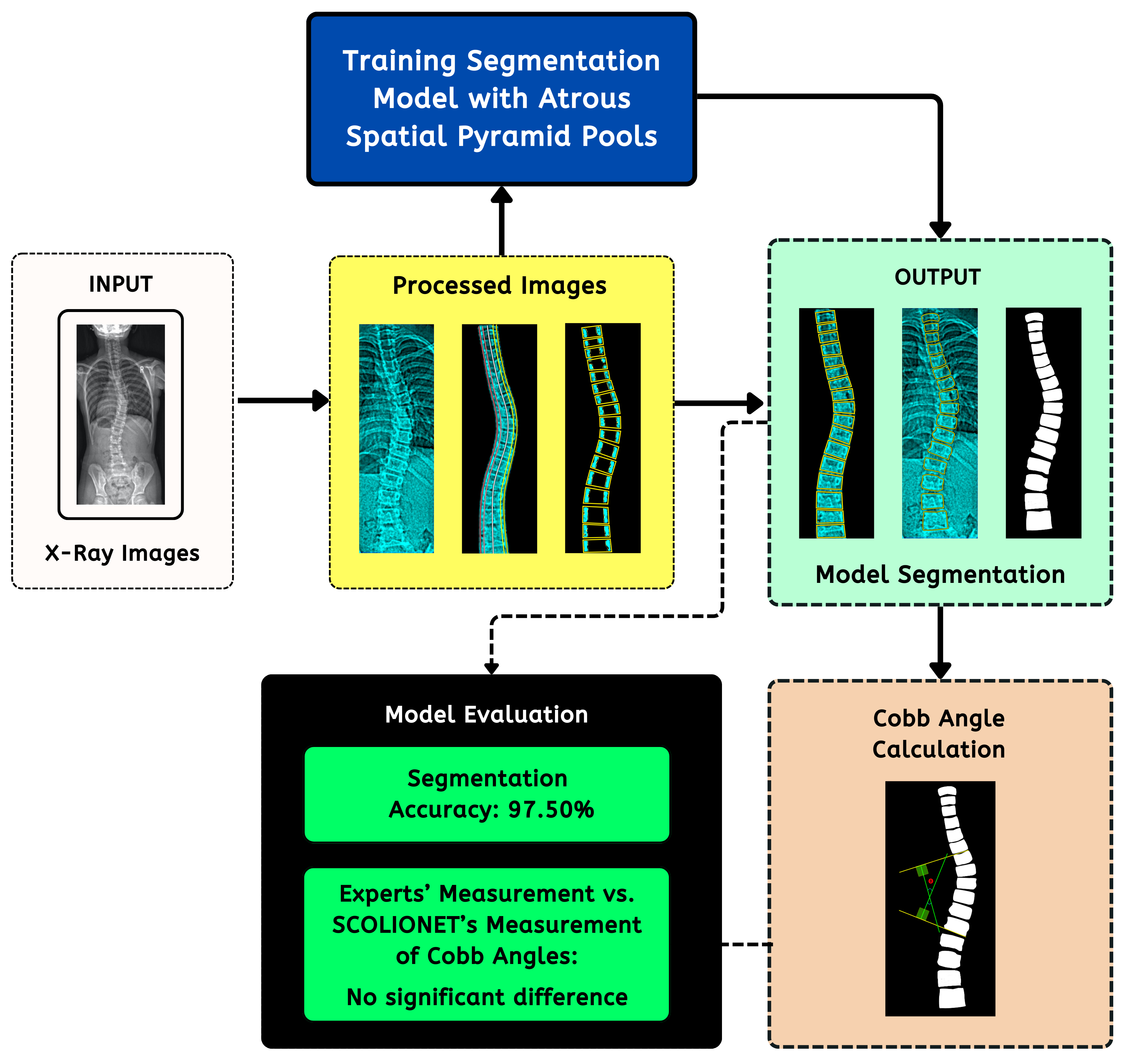
2.7. Atrous Spatial Pyramid Pooling (ASPP) Structure
2.8. Cobb Angle Reference and Calculation
2.9. Quantitative Image Enhancement Evaluation
2.10. Segmentation Assessment Measures
2.11. Degree of Difference Evaluation Metrics
2.12. Cobb Angle Measurement’s Reliability Test
3. Results
3.1. Image Enhancement Performance Evaluation
3.2. Computing Performance Assessment
3.3. Segmentation Performance and Visual Confirmation Evaluation
3.4. Cobb Angle Performance Evaluation
3.5. Benchmarked Performance versus Existing State-of-the-Art Approaches
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vertebrae Column. Available online: https://www.britannica.com/science/vertebra/ (accessed on 25 June 2023).
- Labrom, F.; Izatt, M.; Claus, A.; Little, J. Adolescent idiopathic scoliosis 3D vertebral morphology, progression and nomenclature: A current concepts and review. Eur. Spine J. 2023, 30, 1823–1834. [Google Scholar] [CrossRef] [PubMed]
- McAviney, J.; Roberts, C.; Sullivan, B.; Alevras, A.; Graham, P.; Brown, B. The prevalence of adult de novo scoliosis: A systematic review and meta-analysis. Eur. Spine J. 2020, 29, 2960–2969. [Google Scholar] [CrossRef] [PubMed]
- Scoliosis Degrees of Curvature Chart. Scoliosis Reduction Center. Available online: https://www.scoliosisreductioncenter.com/blog/scoliosis-degrees-of-curvature-chart/ (accessed on 5 July 2023).
- Victoria, M.; Lau, H.; Lee, T.; Alarcon, D.; Zheng, Y. Comparison of ultrasound scanning for scoliosis assessment: Robotic versus manual. Int. J. Med. Robot. Comput. Assist. Surg. 2022, 19, e2468. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Xing, Y.; Zhao, Z.; Meng, X.; Xu, G.; Hai, Y. Comparison of manual versus automated measurement of cobb angle in idiopathic scoliosis based on a deep learning keypoint detection technology. Eur. Spine J. 2021, 31, 1969–1978. [Google Scholar] [CrossRef]
- Maaliw, R.; Soni, M.; Delos Santos, M.; De Veluz, M.; Lagrazon, P.; Seño, M.; Salvatierra-Bello, D.; Danganan, R. AWFCNET: An attention-aware deep learning network with fusion classifier for breast cancer classification using enhanced mammograms. In Proceedings of the IEEE World Artificial Intelligence and Internet of Things Congress (AIIoT), Seattle, DC, USA, 7–10 June 2023. [Google Scholar]
- Pradhan, N.; Sagar, S.; Singh, A. Analysis of MRI image data for Alzheimer disease detection using deep learning techniques. Multimed. Tools Appl. 2023, 1–24. [Google Scholar] [CrossRef]
- Maaliw, R.; Mabunga, Z.; De Veluz, M.; Alon, A.; Lagman, A.; Garcia, M.; Lacatan, L.; Dellosa, R. An enhanced segmentation and deep learning architecture for early diabetic retinopathy detection. In Proceedings of the IEEE 13th Annual Computing and Communication Workshop and Conference (CCWC), Las Vegas, NV, USA, 8–11 March 2023. [Google Scholar]
- Tu, Y.; Wang, N.; Tong, F.; Chen, H. Automatic measurement algorithm of scoliosis Cobb angle based on deep learning. J. Phys. Conf. Ser. 2019, 1187, 042100. [Google Scholar] [CrossRef]
- Okashi, O.; Du, H.; Al-Assam, H. Automatic spine curvature estimation from X-ray images of a mouse model. Comput. Methods Programs Biomed. 2017, 140, 175–184. [Google Scholar] [CrossRef]
- Alharbi, R.; Alshaye, M.; Alhanhal, M.; Alharbi, N.; Alzahrani, M.; Alrehaili, O. Deep learning based algorithm for automatic scoliosis angle measurement. In Proceedings of the IEEE 3rd International Conference on Computer Applications & Information Security (ICCAIS), Riyadh, Saudi Arabia, 19–21 March 2020. [Google Scholar]
- Zhang, K.; Xu, N.; Yang, G.; Wu, J.; Fu, X. An automated Cobb angle estimation method using convolutional neural network with area limitation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention (MICCAI), Shenzhen, China, 13–17 October 2019. [Google Scholar]
- Huang, C.; Tang, H.; Fan, W.; Cheung, K.; To, M.; Qian, Z.; Terzopoulos, D. Fully-automated analysis of scoliosis from spinal X-ray images. In Proceedings of the IEEE 33rd International Symposium on Computer-Based Medical Systems (CBMS), Rochester, MN, USA, 28–30 July 2020. [Google Scholar]
- Pasha, S.; Flynn, J. Data-driven classification of the 3d spinal curve in adolescent idiopathic scoliosis with applications in surgical outcome prediction. Sci. Rep. 2018, 8, 16296. [Google Scholar] [CrossRef]
- Moura, C.; Correia, M.; Barbosa, J.; Reis, A.; Laranjeira, M.; Gomes, E. Automatic Vertebra Detection in X-ray Images. In Proceedings of the International Symposium CompImage, Coimbra, Portugal, 20–21 October 2016. [Google Scholar]
- Mukherjee, J.; Kundu, R.; Chakrabarti, A. Variability of Cobb angle measurement from digital X-ray image based on different de-noising techniques. Int. J. Biomed. Eng. Technol. 2014, 16, 113–134. [Google Scholar] [CrossRef]
- Lecron, F.; Benjelloun, M.; Mahmoudi, S. Fully automatic vertebra detection in X-ray images based on multi-class SVM. In Proceedings of the Medical Imaging, San Diego, CA, USA, 8–9 February 2012. [Google Scholar]
- Maaliw, R.; Alon, A.; Lagman, A.; Garcia, M.; Susa, J.; Reyes, R.; Fernando-Raguro, M.; Hernandez, A. A multistage transfer learning approach for acute lymphoblastic leukemia classification. In Proceedings of the IEEE 13th Annual Ubiquitous Computing, Electronics & Mobile Communication Conference, New York, NY, USA, 26–29 October 2022. [Google Scholar]
- Vijh, S.; Gaurav, P.; Pandey, H. Hybrid bio-inspired algorithm and convolutional neural network for automatic lung tumor detection. Comput. Math. Methods Med. 2020, 35, 23711–23724. [Google Scholar] [CrossRef]
- Peng, C.; Wu, M.; Liu, K. Multiple levels perceptual noise backed visual information fidelity for picture quality assessment. In Proceedings of the IEEE International Symposium on Intelligent Signal Processing and Communication Systems (ISPACS), Penang, Malaysia, 22–25 November 2022. [Google Scholar]
- Tsuneki, M. Deep Learning Models in Medical Image Analysis. J. Oral Biosci. 2022, 64, 312–320. [Google Scholar] [CrossRef]
- Chakraborty, S.; Mali, K. An Overview of Biomedical Image Analysis from the Deep Learning Perspective; IGI Global: Hershey, PA, USA, 2023; pp. 43–59. [Google Scholar]
- Abdou, M. Literature review: Efficient deep neural networks techniques for medical image analysis. Neural Comput. Appl. 2022, 34, 5791–5812. [Google Scholar] [CrossRef]
- Varoquaux, G.; Cheplygina, V. Machine learning for medical imaging: Methodological failures and recommendations for the future. NPJ Digit. Med. 2022, 5, 48. [Google Scholar] [CrossRef] [PubMed]
- Aljabri, M.; AlGhamdi, M. A review on the use of deep learning for medical images segmentation. Neurocomputing 2022, 506, 311–335. [Google Scholar] [CrossRef]
- Karpiel, I.; Ziębiński, A.; Kluszczyński, M.; Feige, D. A survey of methods and technologies used for diagnosis of scoliosis. Sensors 2021, 21, 8410. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Sun, L.; Fu, Y.; Lu, R.; Zhang, Y. U-Net-Based Medical Image Segmentation. J. Healthc. Eng. 2022, 2022, 4189781. [Google Scholar] [CrossRef]
- Arif, S.; Knapp, K.; Slabaugh, G. Shapeaware deep convolutional neural network for vertebrae segmentation. In Proceedings of the International Workshop on Computational Methods and Clinical Applications in Musculoskeletal Imaging (MICCAI), Quebec City, QC, Canada, 10 September 2017. [Google Scholar]
- Zhang, J.; Li, H.; Lu, L.; Zhang, Y. Computer-aided Cobb measurement based on automatic detection of vertebral slope using deep neural network. Int. J. Biomed. Imaging 2017, 2017, 9083916. [Google Scholar] [CrossRef]
- Staritsyn, M.; Pogodaev, N.; Chertovshih, R.; Pereira, F. Feedback maximum principle for ensemble control of local continuity equations: An application to supervised machine learning. IEEE Control Syst. Lett. 2021, 6, 1046–1051. [Google Scholar] [CrossRef]
- Fan, W.; Ge, Z.; Wang, Y. Adaptive Weiner filter based on fast lifting wavelet transform for image enhancement. In Proceedings of the 7th World Congress on Intelligent Control and Automation, Chongqing, China, 25–27 June 2008. [Google Scholar]
- Horng, M.; Kuok, C.; Fu, M.; Lin, C.; Sun, Y. Cobb angle measurement of spine from X-ray images using convolutional neural network. Comput. Math. Methods Med. 2019, 2019, 6357171. [Google Scholar] [CrossRef]
- Prodan, M.; Vlasceanu, G.; Boiangiu, C. Comprehensive evaluation of metrics for image resemblance. J. Inf. Syst. Oper. Manag. 2023, 17, 161–185. [Google Scholar]
- Ieremeiev, O.; Lukin, V.; Okarma, K.; Egiazarian, K. Full-Reference quality metric based on neural network to assess the visual quality of remote sensing images. Remote Sens. 2020, 12, 2349. [Google Scholar] [CrossRef]
- Aviles, J.; Medina, F.; Leon-Muñoz, V.; de Baranda, P.S.; Collazo-Diéguez, M.; Cabañero-Castillo, M.; Ponce-Garrido, A.B.; Fuentes-Santos, V.E.; Santonja-Renedo, F.; González-Ballester, M.; et al. Validity and absolute reliability of the Cobb angle in idiopathic scoliosis with TraumaMeter software. Int. J. Environ. Res. Public Health 2022, 19, 4655. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Angle in Degrees | Spine Class |
|---|---|---|
| 1 | 0–10 | Normal |
| 2 | 10–20 | Mild |
| 3 | 20–40 | Moderate |
| 4 | >40 | Severe |
| Method | Correlation Coefficient (CC) | Spearman Rank Order Correlation Coefficient (SROCC) |
|---|---|---|
| VIF | 0.973 | 0.968 |
| Deep Neural Network Model | Training Time in Minutes | |
|---|---|---|
| Four Active Processor Cores | Eight Active Processor Cores | |
| Standard U-Net | 21.16 | 18.35 |
| Residual U-Net | 23.81 | 20.15 |
| SCOLIONET | 24.48 | 19.38 |
| Deep Neural Network Model | Memory Consumption Based on Number of Batches | ||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 4 | 8 | 16 | 32 | 64 | |
| Standard U-Net | 0.67 | 0.63 | 0.67 | 0.67 | 0.67 | 0.66 | 0.68 |
| Residual U-Net | 0.72 | 0.66 | 0.72 | 0.72 | 0.71 | 0.73 | 0.78 |
| SCOLIONET | 0.72 | 0.65 | 0.71 | 0.70 | 0.70 | 0.72 | 0.77 |
| Fold | SDC | IoU | MSE | ||||||
|---|---|---|---|---|---|---|---|---|---|
| U-Network | SCOLIONET | RU-Network | U-Network | SCOLIONET | RU-Network | U-Network | SCOLIONET | RU-Network | |
| 1 | 0.939 ± 0.034 | 0.978 ± 0.027 | 0.952 ± 0.025 | 0.923 ± 0.042 | 0.967 ± 0.028 | 0.940 ± 0.045 | 0.031 ± 0.018 | 0.021 ± 0.014 | 0.028 ± 0.018 |
| 2 | 0.943 ± 0.035 | 0.973 ± 0.025 | 0.953 ± 0.024 | 0.921 ± 0.045 | 0.963 ± 0.027 | 0.942 ± 0.040 | 0.032 ± 0.015 | 0.025 ± 0.015 | 0.029 ± 0.016 |
| 3 | 0.941 ± 0.031 | 0.975 ± 0.026 | 0.951 ± 0.029 | 0.922 ± 0.044 | 0.960 ± 0.028 | 0.939 ± 0.039 | 0.033 ± 0.016 | 0.024 ± 0.016 | 0.030 ± 0.018 |
| 4 | 0.942 ± 0.034 | 0.976 ± 0.027 | 0.949 ± 0.026 | 0.923 ± 0.045 | 0.969 ± 0.031 | 0.941 ± 0.041 | 0.034 ± 0.017 | 0.025 ± 0.014 | 0.032 ± 0.017 |
| 5 | 0.942 ± 0.035 | 0.977 ± 0.028 | 0.951 ± 0.027 | 0.921 ± 0.041 | 0.961 ± 0.029 | 0.942 ± 0.043 | 0.032 ± 0.015 | 0.027 ± 0.015 | 0.033 ± 0.019 |
| 6 | 0.943 ± 0.033 | 0.975 ± 0.024 | 0.949 ± 0.028 | 0.929 ± 0.046 | 0.964 ± 0.030 | 0.940 ± 0.043 | 0.033 ± 0.019 | 0.029 ± 0.020 | 0.030 ± 0.016 |
| 7 | 0.941 ± 0.032 | 0.976 ± 0.027 | 0.950 ± 0.029 | 0.925 ± 0.043 | 0.962 ± 0.030 | 0.948 ± 0.040 | 0.032 ± 0.017 | 0.028 ± 0.016 | 0.032 ± 0.018 |
| 8 | 0.942 ± 0.032 | 0.977 ± 0.028 | 0.951 ± 0.030 | 0.931 ± 0.045 | 0.965 ± 0.032 | 0.946 ± 0.039 | 0.034 ± 0.015 | 0.027 ± 0.013 | 0.031 ± 0.016 |
| 9 | 0.941 ± 0.035 | 0.978 ± 0.026 | 0.950 ± 0.028 | 0.932 ± 0.048 | 0.968 ± 0.033 | 0.945 ± 0.040 | 0.033 ± 0.016 | 0.023 ± 0.012 | 0.031 ± 0.018 |
| 10 | 0.940 ± 0.037 | 0.974 ± 0.025 | 0.949 ± 0.029 | 0.933 ± 0.049 | 0.964 ± 0.031 | 0.943 ± 0.041 | 0.032 ± 0.018 | 0.024 ± 0.017 | 0.029 ± 0.016 |
| Mean ± Standard deviation | 0.941 ± 0.033 | 0.975 ± 0.026 | 0.950 ± 0.027 | 0.926 ± 0.044 | 0.963 ± 0.029 | 0.942 ± 0.041 | 0.032 ± 0.016 | 0.025 ± 0.015 | 0.030 ± 0.017 |
| Training duration, eight processing cores (in minutes): | SCOLIONET (19.38), RU-Network (20.15), and U-Network (18.35) | ||||||||
| Test duration, eight processing cores (in seconds): | SCOLIONET (0.04), RU-Network (0.03), and U-Network (0.02) | ||||||||
| X-ray ID | SCOLIONET’s Cobb Angle | Experts’s Cobb Angle (Observed) | Absolute Difference of Vertebral References (SCOLIONET vs. Expert) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Most Tilted Upper Vertebrae | Most Tilted Lower Vertebrae | Cobb Angle Degree | Most Tilted Upper Vertebrae | Most Tilted Lower Vertebrae | Cobb Angle Degree | Most Tilted Upper Vertebrae | Most Tilted Lower Vertebrae | Cobb Angle Degree | |
| 0021 | TH08 | LU03 | 23.80 | TH08 | LU03 | 23.50 | TH08—0 | LU03—0 | 0.30 |
| 0055 | TH12 | LU02 | 12.50 | TH12 | LU02 | 13.70 | TH12—0 | LU02—0 | 1.20 |
| 0071 | TH09 | LU04 | 13.60 | TH09 | LU03 | 15.20 | TH09—0 | LU04/LU03—1 | 1.60 |
| 0085 | TH05 | TH11 | 25.30 | TH05 | TH11 | 26.20 | TH05—0 | TH11—0 | 0.90 |
| 0103 | TH06 | TH12 | 24.60 | TH06 | TH12 | 24.50 | TH06—0 | TH12—0 | 0.10 |
| 0123 | TH10 | LU03 | 23.10 | TH10 | LU03 | 22.90 | TH10—0 | LU03—0 | 0.20 |
| 0203 | TH03 | TH09 | 41.20 | TH02 | LU01 | 43.70 | TH03/TH07—3 | TH09/LU01—3 | 3.50 |
| 0233 | TH05 | LU04 | 32.60 | TH05 | LU04 | 32.50 | TH05—0 | LU04—0 | 0.10 |
| 0253 | TH05 | LU02 | 40.60 | TH06 | LU04 | 42.50 | TH03/TH06—2 | LU02/LU04—2 | 3.00 |
| 0313 | TH06 | TH12 | 16.70 | TH06 | TH12 | 17.20 | TH06—0 | TH12—0 | 0.50 |
| Legend: | TH01–TH12 (thoracic), LU01–LU05 (lumbar) [1] | ||||||||
| T-test (SCOLIONET vs. Experts) | t = 0.1713, p-value = 0.8659 (Not significant at p < 0.05) | ||||||||
| MAPE (SCOLIONET vs. Experts) | 3.86% (Accuracy = 96.13) | ||||||||
| Mean absolute difference of measurements (SCOLIONET vs. Experts) | 2.86 degrees | ||||||||
| Architectures/Approaches/Models/Mechanisms | Accuracy |
|---|---|
| Standard U-Net (with different configurations) [22] | 88.01% |
| Patch-wise portioning + minimum bounding boxes [14] | 88.60% |
| K-Means clustering + regression [15] | 88.20% |
| Residual U-Net [23] | 88.30% |
| Lateral boundary detection [16] | 88.50% |
| 3-Stage process (Otsu algorithm, morphology, and polynomial fitting) [11] | 90.20% |
| Otsu thresholds + Hough transformations [17] | 90.30% |
| Corner tracking + support vector machines [18] | 90.40% |
| Dense U-Net [23] | 94.20% |
| Residual U-Net (polynomial fitting + minimum border box) [24] | 95.10% |
| SCOLIONET (spinal isolation via Adboost + color shifting + SWF + polynomial fitting + bounding box method + modified U-Net with atrous spatial pyramid pooling) | 97.50% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maaliw, R.R., III. SCOLIONET: An Automated Scoliosis Cobb Angle Quantification Using Enhanced X-ray Images and Deep Learning Models. J. Imaging 2023, 9, 265. https://doi.org/10.3390/jimaging9120265
Maaliw RR III. SCOLIONET: An Automated Scoliosis Cobb Angle Quantification Using Enhanced X-ray Images and Deep Learning Models. Journal of Imaging. 2023; 9(12):265. https://doi.org/10.3390/jimaging9120265
Chicago/Turabian StyleMaaliw, Renato R., III. 2023. "SCOLIONET: An Automated Scoliosis Cobb Angle Quantification Using Enhanced X-ray Images and Deep Learning Models" Journal of Imaging 9, no. 12: 265. https://doi.org/10.3390/jimaging9120265
APA StyleMaaliw, R. R., III. (2023). SCOLIONET: An Automated Scoliosis Cobb Angle Quantification Using Enhanced X-ray Images and Deep Learning Models. Journal of Imaging, 9(12), 265. https://doi.org/10.3390/jimaging9120265