
Deep Learning for Pneumonia Detection in Chest X-ray Images: A Comprehensive Survey


Abstract
1. Introduction
2. Research Questions
3. Research Method
3.1. Inclusion Criteria
- Empirical studies that focus on solving the problem of pneumonia detection using CXRs using DL;
- Studies published in a peer-reviewed journal or conference proceeding;
- Studies published between 2020 and 2023 inclusively.
3.2. Exclusion Criteria
- If a paper or a publication fell into any of the following categories, it was excluded:
- All reviews and survey papers;
- All non-peer-reviewed publications;
- Short papers less than 5 pages long;
- Book chapters, as these are usually reviews of a research area;
- All papers that were scientifically unsound. Scientifically unsound papers include all papers in which methodology is not meticulously presented or in which the hypothesis or the solution is not methodically evaluated;
- All papers not written in English;
- Duplicate papers were removed. For example, only a single item was retained if the same item was returned by two or more different databases;
- Papers focusing on detection of some other chest disease like tuberculosis, pneumothorax, cardiomegaly, etc., in which pneumonia detection is not considered;
- All papers exclusively exploiting traditional ML approaches;
- All papers exclusively based on non-CXR modalities like CT scans, ultrasound scans, etc.
- Are the research objectives clear and well defined?
- Is the methodology comprehensively explained?
- Is the proposed solution thoroughly evaluated?
- Are the limitations of the research clearly stated?
- Is the research work published in a reputable journal or conference proceeding? For example, any relevant paper published in a journal that has an impact factor less than 3 is discarded.
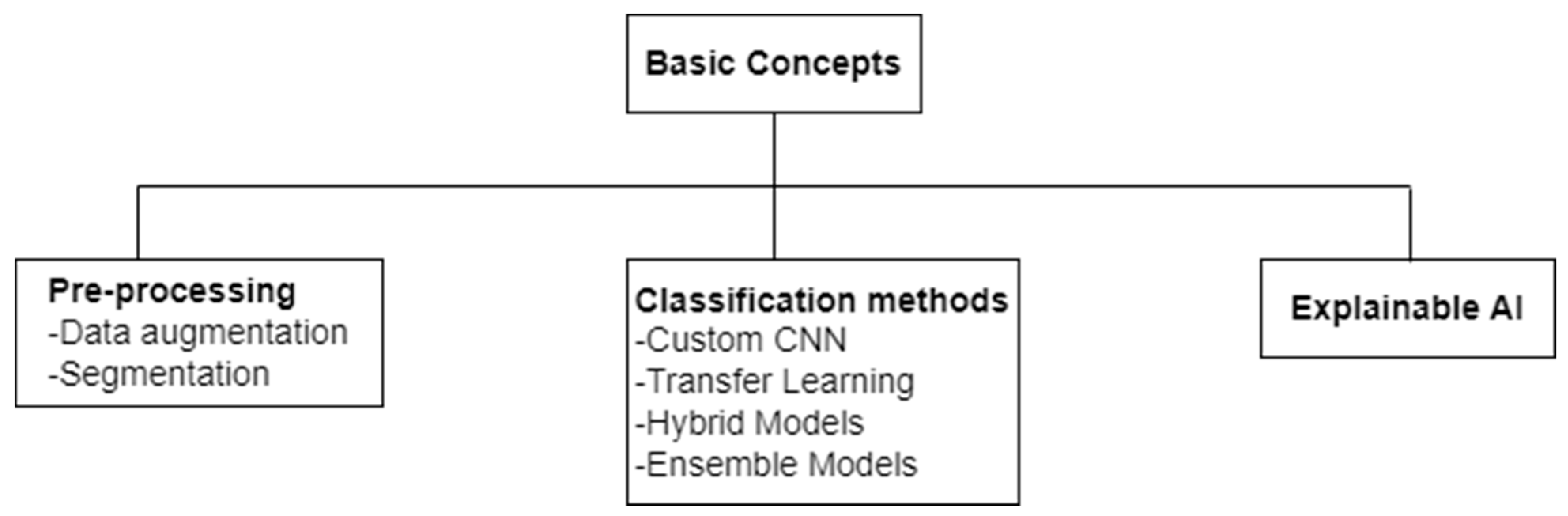
4. Basic Concepts
4.1. Data Augmentation
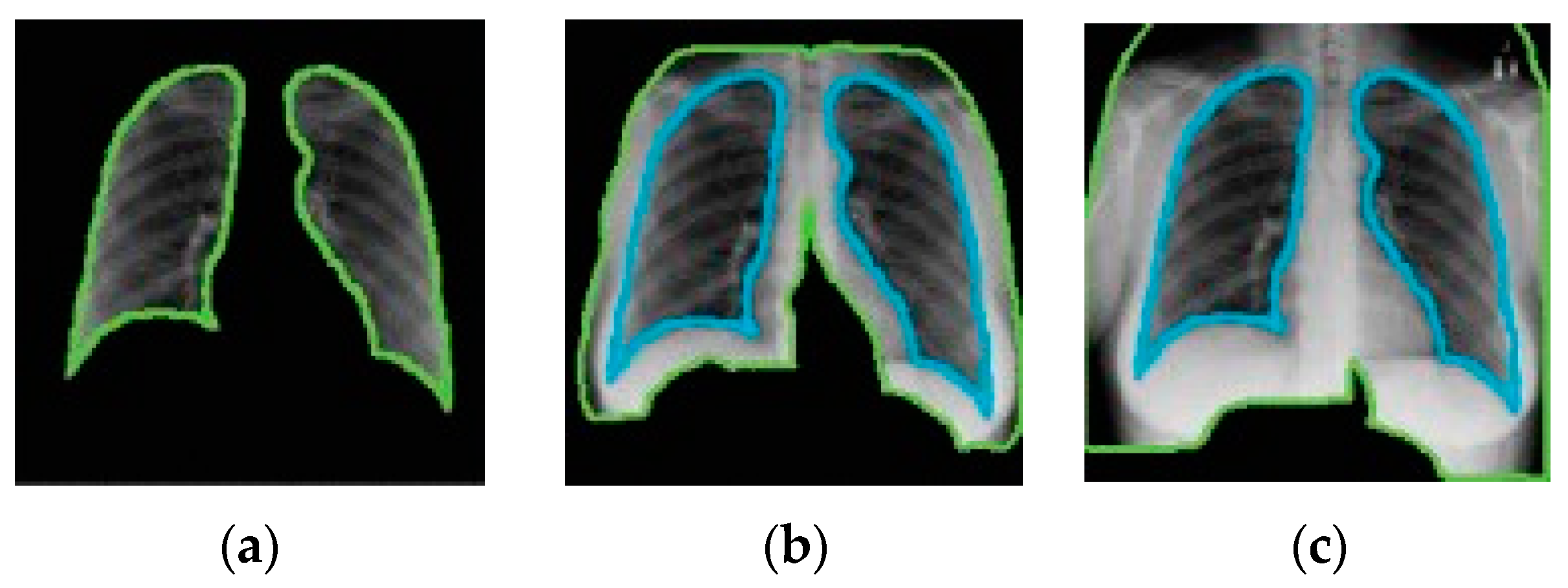
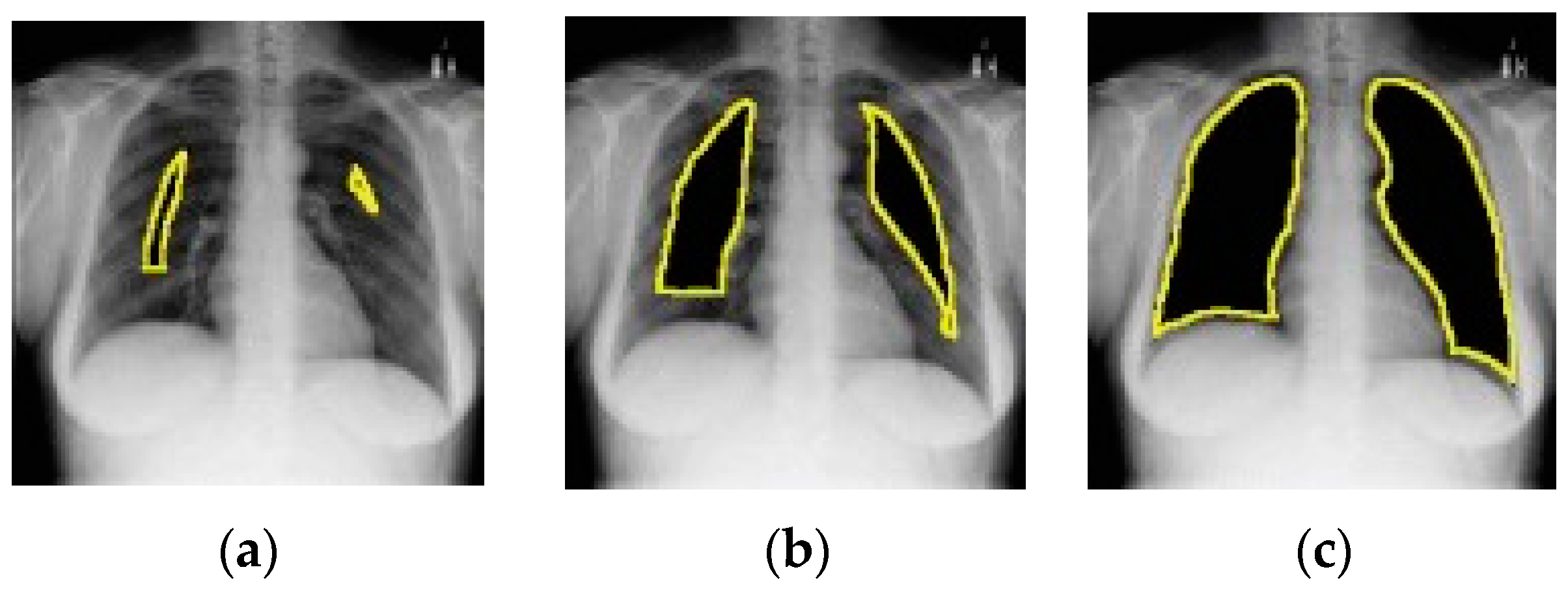
4.2. Segmentation
4.3. Convolutional Neural Networks
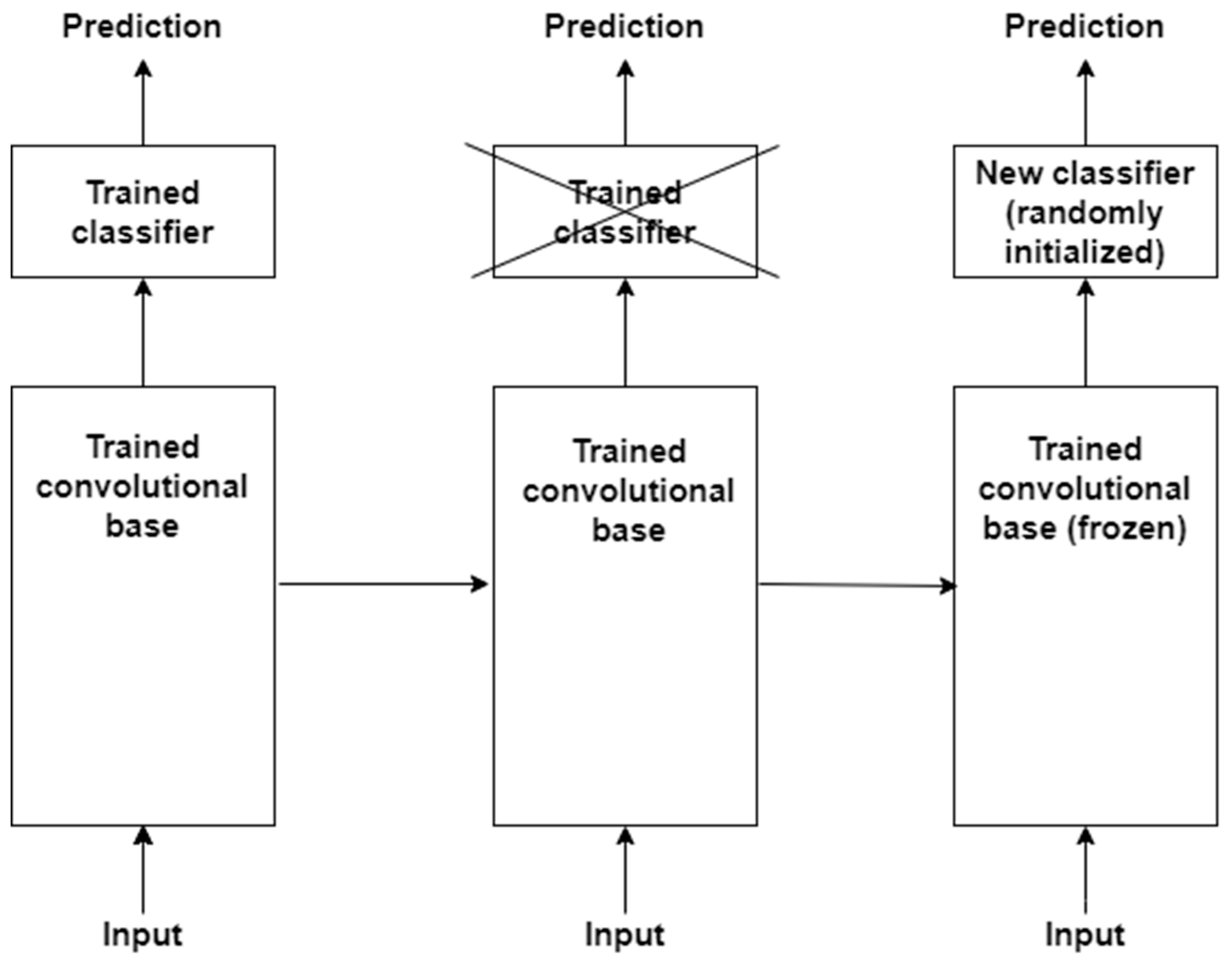
4.4. Transfer Learning
4.5. Hybrid Deep Learning Models
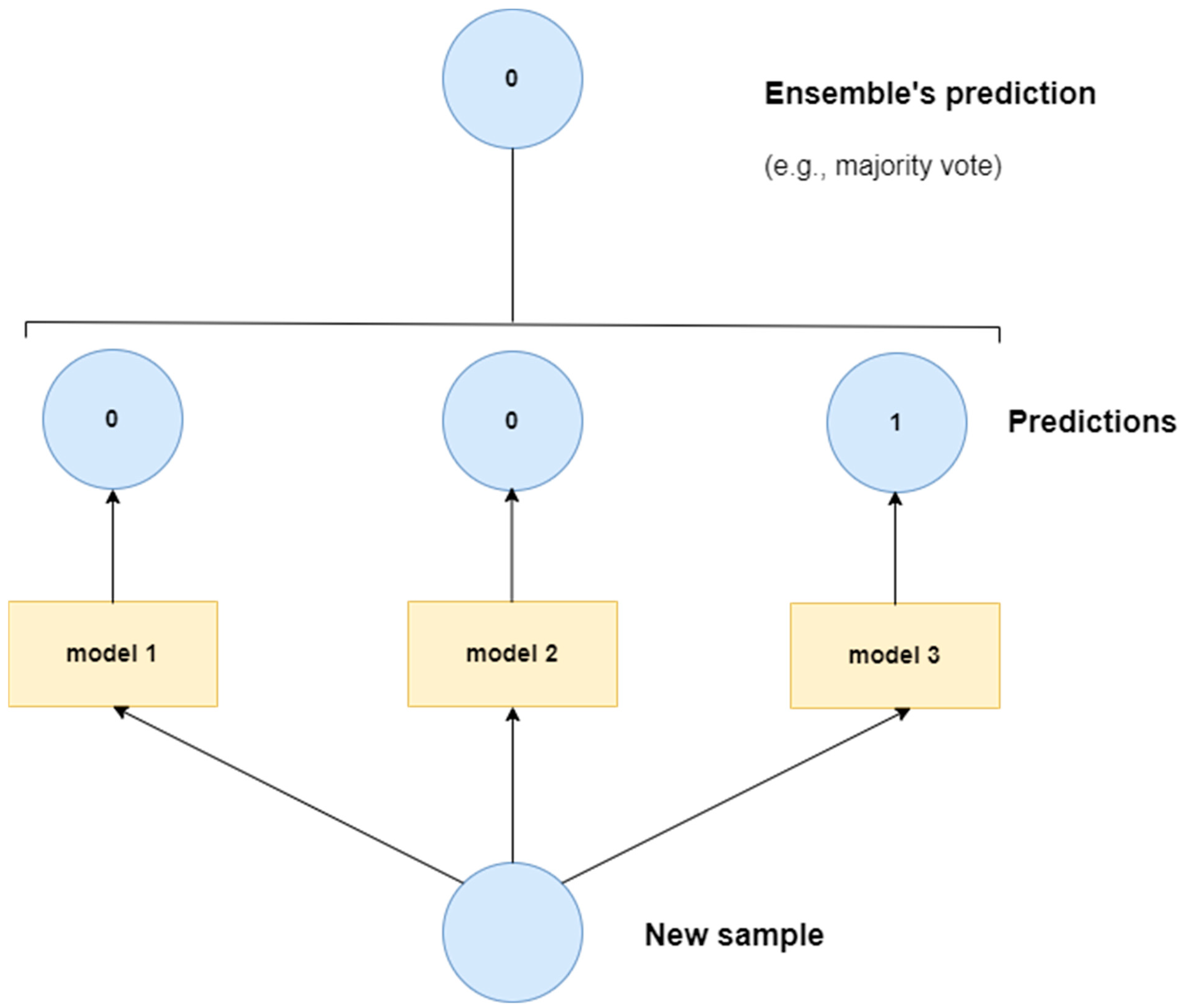
4.6. Ensemble Deep Learning Models
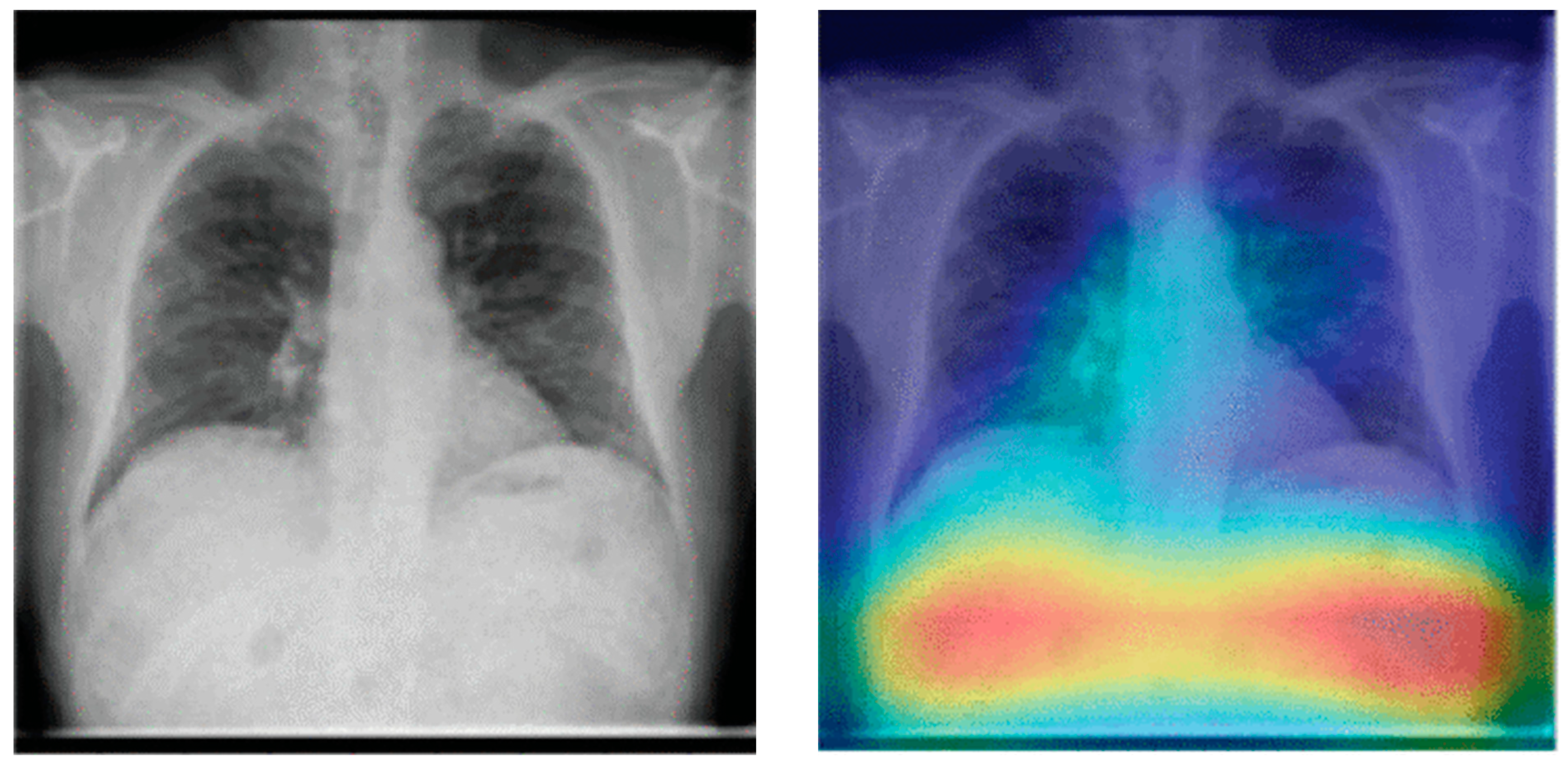
4.7. Explainable Artificial Intelligence (XAI)
5. Datasets
6. Key Statistics
7. Current Trends

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref./ Year | COVID/Non COVID Pneumonia | Binary/Multi Classification | Methodology | Results | Contribution | Research Gap |
|---|---|---|---|---|---|---|
| [189] 2023 | Both | Multi Classification | Transfer Learning, VGG-19+CNN | 96.48% | Good accuracy | Powerful segmentation models for precise ROI identification are required. |
| [194] 2023 | Non-COVID Pneumonia | Binary Classification | Hybrid technique | 97.9% | Simplified the model by reducing advance feature extraction. | Unbalanced data distribution |
| [143] 2023 | Both | Multi Classification | CDC_Net | 99.39% | Structured noise reduced | NA |
| [191] 2023 | Non-COVID Pneumonia | Binary Classification | Ensemble CNN+ Transformer Encoder | 99.21% | Self-attention mechanism provided more accurate results | Annotated text data required |
| [195] 2023 | COVID Pneumonia | Binary Classification | Multi-level self-attention mechanismTransforme r | 99.13% | Reduced computing complexity to increase the efficiency of the recognition process. | Multi-classification model could be enhanced |
| [187] 2023 | Non-COVID Pneumonia | Binary Classification | DCNN | 96.09% | Impactful preprocessing techniques | NA |
| [190] 2023 | Both | Multi Classification | DenseNet201 | 99.1% | DenseNet provides collective knowledge | NA |
| [192] 2023 | Both | Multi Classification | Ensemble Learning (EfficientNet) | 98% | NA | Attention-based feature fusion may reduce complexity |
| [188] 2023 | Non-COVID Pneumonia | Binary Classification | Enhanced CNN+ResNet-50 | 92.4% | NA | NA |
| [193] 2023 | Non-COVID Pneumonia | Multi Classification | Hybrid deep learning model (C+EffxNet) | 99.2% | The application of feature merging improved the decision support system. | To better predict chest infections, more classes can be included |
| [133] 2023 | Non-COVID Pneumonia | Multi Classification | Stacked ensemble learning | 98.3% | Reduced features are promoted to the stacking classifier. | Preprocessing and reinforment learning can improve results |
| [163] 2023 | Both | Multi Classification | Vision Transformer (PneuNet) | 94.96% | Binary pneumonia classification model achieved 99.29% accuracy | Channel-wise transformer encoder can enhance results |
- Transformer-based designs have been successfully employed in both multi-class and binary classification settings in studies. These models equipped with self-attention mechanisms have shown remarkable accuracies ranging from 94.96% to 99.39%.
- Several studies have shown that transformers minimize computational complexity without sacrificing accuracy. They promote efficient recognition processes, which are critical in medical applications in which prompt diagnosis is required.
- Despite its usefulness, some research using transformer models has presented interpretability difficulties. To improve interpretability and feature representation, there is a clear need to improve feature extraction approaches inside transformer designs.
- Transformers have demonstrated adaptability and resilience by being successfully deployed in both COVID and non-COVID pneumonia detection across many classification challenges.
- Handling Global Information: ViTs capture global relationships inside an image. This understanding of context and relationships between different regions may be especially important in medical imaging, for which the context of anomalies in an X-ray may be critical for diagnosis;
- Fewer Parameters: Because ViTs can process pictures without depending on complex convolutional procedures, they may require fewer parameters than typical CNNs, making them more efficient;
- Transfer Learning: ViTs have demonstrated promise in transfer learning. Pre-trained ViT models developed on large-scale datasets can be fine-tuned on smaller medical datasets, which is especially useful when labeled medical data are limited.
- Data Efficiency: ViTs frequently require significant amounts of data for training, and collecting labeled datasets in medical imaging can be difficult due to privacy concerns and data scarcity;
- Computational Needs: Training ViTs can be computationally demanding, necessitating significant resources and effort;
- Interpretability: Understanding why a ViT makes a certain decision may be more difficult than with typical CNNs, which may be a worry in essential applications such as medical diagnosis.
8. Discussion
8.1. Biased Datasets
8.2. Data and Code Availability
8.3. Explainability of Models
8.4. Fair Comparison
8.5. Class Imbalance in CXR Datasets
8.6. Adversarial Attacks
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kermany, D.S.; Goldbaum, M.; Cai, W.; Valentim, C.C.S.; Liang, H.; Baxter, S.L.; McKeown, A.; Yang, G.; Wu, X.; Yan, F.; et al. Identifying Medical Diagnoses and Treatable Diseases by Image-Based Deep Learning. Cell 2018, 172, 1122–1131.e9. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.U.; Ozsoz, M.; Serte, S.; Al-Turjman, F.; Yakoi, P.S. Pneumonia Classification Using Deep Learning from Chest X-ray Images During COVID-19. Cogn. Comput. 2024, 16, 1589–1601. [Google Scholar] [CrossRef]
- Pneumonia|CDC. Available online: https://www.cdc.gov/pneumonia/index.html (accessed on 14 September 2022).
- Ruuskanen, O.; Lahti, E.; Jennings, L.C.; Murdoch, D.R. Viral pneumonia. Lancet 2011, 377, 1264–1275. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Available online: https://www.who.int/ (accessed on 14 September 2022).
- Khan, W.; Zaki, N.; Ali, L. Intelligent Pneumonia Identification From Chest X-Rays: A Systematic Literature Review. IEEE Access 2021, 9, 51747–51771. [Google Scholar] [CrossRef]
- Johns Hopkins Coronavirus Resource Center. Johns Hopkins University & Medicine. Available online: https://coronavirus.jhu.edu/ (accessed on 14 September 2022).
- Ieracitano, C.; Mammone, N.; Versaci, M.; Varone, G.; Ali, A.-R.; Armentano, A.; Calabrese, G.; Ferrarelli, A.; Turano, L.; Tebala, C.; et al. A fuzzy-enhanced deep learning approach for early detection of COVID-19 pneumonia from portable chest X-ray images. Neurocomputing 2022, 481, 202–215. [Google Scholar] [CrossRef]
- D’Arienzo, M.; Coniglio, A. Assessment of the SARS-CoV-2 basic reproduction number, R0, based on the early phase of COVID-19 outbreak in Italy. Biosaf. Health 2020, 2, 57–59. [Google Scholar] [CrossRef] [PubMed]
- Rossman, H.; Meir, T.; Somer, J.; Shilo, S.; Gutman, R.; Ben Arie, A.; Segal, E.; Shalit, U.; Gorfine, M. Hospital load and increased COVID-19 related mortality in Israel. Nat. Commun. 2021, 12, 1904. [Google Scholar] [CrossRef]
- Yaseliani, M.; Hamadani, A.Z.; Maghsoodi, A.I.; Mosavi, A. Pneumonia Detection Proposing a Hybrid Deep Convolutional Neural Network Based on Two Parallel Visual Geometry Group Architectures and Machine Learning Classifiers. IEEE Access 2022, 10, 62110–62128. [Google Scholar] [CrossRef]
- Self, W.H.; Courtney, D.M.; McNaughton, C.D.; Wunderink, R.G.; Kline, J.A. High discordance of chest X-ray and computed tomography for detection of pulmonary opacities in ED patients: Implications for diagnosing pneumonia. Am. J. Emerg. Med. 2013, 31, 401–405. [Google Scholar] [CrossRef]
- Ticinesi, A.; Lauretani, F.; Nouvenne, A.; Mori, G.; Chiussi, G.; Maggio, M.; Meschi, T. Lung ultrasound and chest X-ray for detecting pneumonia in an acute geriatric ward. Medicine 2016, 95, e4153. [Google Scholar] [CrossRef]
- Htun, T.P.; Sun, Y.; Chua, H.L.; Pang, J. Clinical features for diagnosis of pneumonia among adults in primary care setting: A systematic and meta-review. Sci. Rep. 2019, 9, 7600. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, R. Efficient Pediatric Pneumonia Diagnosis Using Depthwise Separable Convolutions. SN Comput. Sci. 2020, 1, 343. [Google Scholar] [CrossRef]
- Mettler, F.A.; Huda, W.; Yoshizumi, T.T.; Mahesh, M. Effective Doses in Radiology and Diagnostic Nuclear Medicine: A Catalog. Radiology 2008, 248, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Çallı, E.; Sogancioglu, E.; van Ginneken, B.; van Leeuwen, K.G.; Murphy, K. Deep learning for chest X-ray analysis: A survey. Med. Image Anal. 2021, 72, 102125. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Lin, Z.Q.; Wong, A. COVID-Net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci. Rep. 2020, 10, 19549. [Google Scholar] [CrossRef] [PubMed]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, A.; Chung, M.; Bernheim, A.; Eber, C. Portable chest X-ray in coronavirus disease-19 (COVID-19): A pictorial review. Clin. Imaging 2020, 64, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Pal, B.; Gupta, D.; Rashed-Al-Mahfuz, M.; Alyami, S.A.; Moni, M.A. Vulnerability in Deep Transfer Learning Models to Adversarial Fast Gradient Sign Attack for COVID-19 Prediction from Chest Radiography Images. Appl. Sci. 2021, 11, 4233. [Google Scholar] [CrossRef]
- Rajaraman, S.; Guo, P.; Xue, Z.; Antani, S.K. A Deep Modality-Specific Ensemble for Improving Pneumonia Detection in Chest X-rays. Diagnostics 2022, 12, 1442. [Google Scholar] [CrossRef]
- Kundu, R.; Das, R.; Geem, Z.W.; Han, G.-T.; Sarkar, R. Pneumonia detection in chest X-ray images using an ensemble of deep learning models. PLoS ONE 2021, 16, e0256630. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, Z.; Shahini, N.; Sheykhivand, S.; Mojtahedi, S.; Arshadi, A. COVID-19 detection using chest X-ray images based on a developed deep neural network. SLAS Technol. 2022, 27, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Cha, S.-M.; Lee, S.-S.; Ko, B. Attention-Based Transfer Learning for Efficient Pneumonia Detection in Chest X-ray Images. Appl. Sci. 2021, 11, 1242. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Sarker, I.H. Deep Learning: A Comprehensive Overview on Techniques, Taxonomy, Applications and Research Directions. SN Comput. Sci. 2021, 2, 420. [Google Scholar] [CrossRef]
- Zhou, S.K.; Greenspan, H.; Davatzikos, C.; Duncan, J.S.; Van Ginneken, B.; Madabhushi, A.; Prince, J.L.; Rueckert, D.; Summers, R.M. A Review of Deep Learning in Medical Imaging: Imaging Traits, Technology Trends, Case Studies With Progress Highlights, and Future Promises. Proc. IEEE 2021, 109, 820–838. [Google Scholar] [CrossRef]
- Yamashita, R.; Nishio, M.; Do, R.K.G.; Togashi, K. Convolutional neural networks: An overview and application in radiology. Insights Imaging 2018, 9, 611–629. [Google Scholar] [CrossRef]
- Irvin, J.; Rajpurkar, P.; Ko, M.; Yu, Y.; Ciurea-Ilcus, S.; Chute, C.; Marklund, H.; Haghgoo, B.; Ball, R.; Shpanskaya, K.; et al. CheXpert: A Large Chest Radiograph Dataset with Uncertainty Labels and Expert Comparison. Proc. AAAI Conf. Artif. Intell. 2019, 33, 590–597. [Google Scholar] [CrossRef]
- Wang, X.; Peng, Y.; Lu, L.; Lu, Z.; Bagheri, M.; Summers, R.M. ChestX-Ray8: Hospital-Scale Chest X-Ray Database and Benchmarks on Weakly-Supervised Classification and Localization of Common Thorax Diseases. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 3462–3471. [Google Scholar]
- Johnson, A.E.W.; Pollard, T.J.; Berkowitz, S.J.; Greenbaum, N.R.; Lungren, M.P.; Deng, C.; Mark, R.G.; Horng, S. MIMIC-CXR, a de-identified publicly available database of chest radiographs with free-text reports. Sci. Data 2019, 6, 317. [Google Scholar] [CrossRef]
- Bustos, A.; Pertusa, A.; Salinas, J.-M.; de la Iglesia-Vayá, M. PadChest: A large chest X-ray image dataset with multi-label annotated reports. Med. Image Anal. 2020, 66, 101797. [Google Scholar] [CrossRef]
- Tabik, S.; Gómez-Ríos, A.; Martín-Rodríguez, J.L.; Sevillano-García, I.; Rey-Area, M.; Charte, D.; Guirado, E.; Suárez, J.L.; Luengo, J.; Valero-González, M.A.; et al. COVIDGR Dataset and COVID-SDNet Methodology for Predicting COVID-19 Based on Chest X-Ray Images. IEEE J. Biomed. Health Inform. 2020, 24, 3595–3605. [Google Scholar] [CrossRef] [PubMed]
- Srivastav, D.; Bajpai, A.; Srivastava, P. Improved Classification for Pneumonia Detection using Transfer Learning with GAN based Synthetic Image Augmentation. In Proceedings of the 2021 11th International Conference on Cloud Computing, Data Science & Engineering, Noida, India, 28–29 January 2021; pp. 433–437. [Google Scholar]
- Motamed, S.; Rogalla, P.; Khalvati, F. Data augmentation using Generative Adversarial Networks (GANs) for GAN-based detection of Pneumonia and COVID-19 in chest X-ray images. Inform. Med. Unlocked 2021, 27, 100779. [Google Scholar] [CrossRef] [PubMed]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. ImageNet Large Scale Visual Recognition Challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Sousa, R.T.; Marques, O.; Soares, F.A.A.M.N.; Sene, I.I.G.; de Oliveira, L.L.G.; Spoto, E.S. Comparative Performance Analysis of Machine Learning Classifiers in Detection of Childhood Pneumonia Using Chest Radiographs. Procedia Comput. Sci. 2013, 18, 2579–2582. [Google Scholar] [CrossRef]
- Khobragade, S.; Tiwari, A.; Patil, C.Y.; Narke, V. Automatic detection of major lung diseases using Chest Radiographs and classification by feed-forward artificial neural network. In Proceedings of the 2016 IEEE 1st International Conference on Power Electronics, Intelligent Control and Energy Systems (ICPEICES), Delhi, India, 4–6 July 2016; pp. 1–5. [Google Scholar]
- Hussain, K.; Mohd Salleh, M.N.; Cheng, S.; Shi, Y. Metaheuristic research: A comprehensive survey. Artif. Intell. Rev. 2019, 52, 2191–2233. [Google Scholar] [CrossRef]
- Meedeniya, D.; Kumarasinghe, H.; Kolonne, S.; Fernando, C.; Díez, I.D.l.T.; Marques, G. Chest X-ray analysis empowered with deep learning: A systematic review. Appl. Soft Comput. 2022, 126, 109319. [Google Scholar] [CrossRef]
- Alghamdi, H.S.; Amoudi, G.; Elhag, S.; Saeedi, K.; Nasser, J. Deep Learning Approaches for Detecting COVID-19 From Chest X-Ray Images: A Survey. IEEE Access 2021, 9, 20235–20254. [Google Scholar] [CrossRef] [PubMed]
- Shorten, C.; Khoshgoftaar, T.M. A survey on Image Data Augmentation for Deep Learning. J. Big Data 2019, 6, 60. [Google Scholar] [CrossRef]
- Ahmed, K.B.; Goldgof, G.M.; Paul, R.; Goldgof, D.B.; Hall, L.O. Discovery of a Generalization Gap of Convolutional Neural Networks on COVID-19 X-Rays Classification. IEEE Access 2021, 9, 72970–72979. [Google Scholar] [CrossRef]
- El-Kenawy, E.-S.M.; Mirjalili, S.; Ibrahim, A.; Alrahmawy, M.; El-Said, M.; Zaki, R.M.; Eid, M.M. Advanced Meta-Heuristics, Convolutional Neural Networks, and Feature Selectors for Efficient COVID-19 X-Ray Chest Image Classification. IEEE Access 2021, 9, 36019–36037. [Google Scholar] [CrossRef]
- Karaddi, S.H.; Sharma, L.D. Automated multi-class classification of lung diseases from CXR-images using pre-trained convolutional neural networks. Expert Syst. Appl. 2023, 211, 118650. [Google Scholar] [CrossRef]
- Wong, S.C.; Gatt, A.; Stamatescu, V.; McDonnell, M.D. Understanding Data Augmentation for Classification: When to Warp? In Proceedings of the 2016 International Conference on Digital Image Computing: Techniques and Applications (DICTA), Gold Coast, Australia, 30 November–2 December 2016; pp. 1–6. [Google Scholar]
- Wang, Q.; Zhou, X.; Wang, C.; Liu, Z.; Huang, J.; Zhou, Y.; Li, C.; Zhuang, H.; Cheng, J.-Z. WGAN-Based Synthetic Minority Over-Sampling Technique: Improving Semantic Fine-Grained Classification for Lung Nodules in CT Images. IEEE Access 2019, 7, 18450–18463. [Google Scholar] [CrossRef]
- Zhong, Z.; Zheng, L.; Kang, G.; Li, S.; Yang, Y. Random Erasing Data Augmentation. Proc. AAAI Conf. Artif. Intell. 2020, 34, 13001–13008. [Google Scholar] [CrossRef]
- Siddiqi, R. Fruit-classification model resilience under adversarial attack. SN Appl. Sci. 2021, 4, 31. [Google Scholar] [CrossRef]
- Chlap, P.; Min, H.; Vandenberg, N.; Dowling, J.; Holloway, L.; Haworth, A. A review of medical image data augmentation techniques for deep learning applications. J. Med. Imaging Radiat. Oncol. 2021, 65, 545–563. [Google Scholar] [CrossRef]
- Wang, K.; Gou, C.; Duan, Y.; Lin, Y.; Zheng, X.; Wang, F.-Y. Generative adversarial networks: Introduction and outlook. IEEECAA J. Autom. Sin. 2017, 4, 588–598. [Google Scholar] [CrossRef]
- Gui, J.; Sun, Z.; Wen, Y.; Tao, D.; Ye, J. A Review on Generative Adversarial Networks: Algorithms, Theory, and Applications. IEEE Trans. Knowl. Data Eng. 2021, 35, 3313–3332. [Google Scholar] [CrossRef]
- Gulakala, R.; Markert, B.; Stoffel, M. Rapid diagnosis of Covid-19 infections by a progressively growing GAN and CNN optimisation. Comput. Methods Programs Biomed. 2023, 229, 107262. [Google Scholar] [CrossRef]
- Gulakala, R.; Markert, B.; Stoffel, M. Generative adversarial network based data augmentation for CNN based detection of COVID-19. Sci. Rep. 2022, 12, 19186. [Google Scholar] [CrossRef]
- Khalifa, N.E.M.; Taha, M.H.N.; Hassanien, A.E.; Elghamrawy, S. Detection of Coronavirus (COVID-19) Associated Pneumonia Based on Generative Adversarial Networks and a Fine-Tuned Deep Transfer Learning Model Using Chest X-ray Dataset. In Proceedings of the 8th International Conference on Advanced Intelligent Systems and Informatics 2022, Cairo, Egypt, 20–22 November 2022; Hassanien, A.E., Snášel, V., Tang, M., Sung, T.-W., Chang, K.-C., Eds.; Springer International Publishing: Cham, Switzerland, 2023; pp. 234–247. [Google Scholar]
- Loey, M.; Smarandache, F.; Khalifa, N.E.M. Within the Lack of Chest COVID-19 X-ray Dataset: A Novel Detection Model Based on GAN and Deep Transfer Learning. Symmetry 2020, 12, 651. [Google Scholar] [CrossRef]
- Jabbar, A.; Li, X.; Omar, B. A Survey on Generative Adversarial Networks: Variants, Applications, and Training. ACM Comput. Surv. 2022, 54, 1–49. [Google Scholar] [CrossRef]
- Aggarwal, P.; Mishra, N.K.; Fatimah, B.; Singh, P.; Gupta, A.; Joshi, S.D. COVID-19 image classification using deep learning: Advances, challenges and opportunities. Comput. Biol. Med. 2022, 144, 105350. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y. Chapter 11—Applications. In Gpu-Based Parallel Implementation of Swarm Intelligence Algorithms; Tan, Y., Ed.; Morgan Kaufmann: Burlington, MA, USA, 2016; pp. 167–177. ISBN 978-0-12-809362-7. [Google Scholar]
- Narayanan, B.N.; Davuluru, V.S.P.; Hardie, R.C. Two-stage deep learning architecture for pneumonia detection and its diagnosis in chest radiographs. In Proceedings of the Medical Imaging 2020: Imaging Informatics for Healthcare, Research, and Applications, Houston, TX, USA, 16–17 February 2020; SPIE: Bellingham, WA, USA, 2020; Volume 11318, pp. 130–139. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention–MICCAI 2015, Munich, Germany, 5–9 October 2015; Navab, N., Hornegger, J., Wells, W.M., Frangi, A.F., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Long, J.; Shelhamer, E.; Darrell, T. Fully Convolutional Networks for Semantic Segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition 2015, Boston, MA, USA, 7–12 June 2015; pp. 3431–3440. [Google Scholar]
- Milletari, F.; Navab, N.; Ahmadi, S.-A. V-Net: Fully Convolutional Neural Networks for Volumetric Medical Image Segmentation. In Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar]
- Chen, J.; Cai, Z.; Heidari, A.A.; Liu, L.; Chen, H.; Pan, J. Dynamic mechanism-assisted artificial bee colony optimization for image segmentation of COVID-19 chest X-ray. Displays 2023, 79, 102485. [Google Scholar] [CrossRef]
- Al-Zyoud, W.; Erekat, D.; Saraiji, R. COVID-19 chest X-ray image analysis by threshold-based segmentation. Heliyon 2023, 9, e14453. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.F.; Zhuang, Y.; Tseng, T.-L.B.; Pokojovy, M.; McCaffrey, P.; Walser, E.; Moen, S.; Vo, A. Improving lung region segmentation accuracy in chest X-ray images using a two-model deep learning ensemble approach. J. Vis. Commun. Image Represent. 2022, 85, 103521. [Google Scholar] [CrossRef]
- Manickam, A.; Jiang, J.; Zhou, Y.; Sagar, A.; Soundrapandiyan, R.; Dinesh Jackson Samuel, R. Automated pneumonia detection on chest X-ray images: A deep learning approach with different optimizers and transfer learning architectures. Measurement 2021, 184, 109953. [Google Scholar] [CrossRef]
- Ortiz-Toro, C.; García-Pedrero, A.; Lillo-Saavedra, M.; Gonzalo-Martín, C. Automatic detection of pneumonia in chest X-ray images using textural features. Comput. Biol. Med. 2022, 145, 105466. [Google Scholar] [CrossRef] [PubMed]
- Karthik, R.; Menaka, R.; Hariharan, M. Learning distinctive filters for COVID-19 detection from chest X-ray using shuffled residual CNN. Appl. Soft Comput. 2021, 99, 106744. [Google Scholar] [CrossRef] [PubMed]
- Chollet, F. Deep Learning with Python, 2nd ed.; Simon and Schuster: New York, NY, USA, 2021; ISBN 978-1-61729-686-4. [Google Scholar]
- Khan, M.; Mehran, M.T.; Haq, Z.U.; Ullah, Z.; Naqvi, S.R.; Ihsan, M.; Abbass, H. Applications of artificial intelligence in COVID-19 pandemic: A comprehensive review. Expert Syst. Appl. 2021, 185, 115695. [Google Scholar] [CrossRef]
- Babukarthik, R.G.; Adiga, V.A.K.; Sambasivam, G.; Chandramohan, D.; Amudhavel, J. Prediction of COVID-19 Using Genetic Deep Learning Convolutional Neural Network (GDCNN). IEEE Access 2020, 8, 177647–177666. [Google Scholar] [CrossRef]
- Singh, G.; Yow, K.-C. An Interpretable Deep Learning Model for COVID-19 Detection With Chest X-Ray Images. IEEE Access 2021, 9, 85198–85208. [Google Scholar] [CrossRef]
- Rozenberg, E.; Freedman, D.; Bronstein, A.A. Learning to Localize Objects Using Limited Annotation, with Applications to Thoracic Diseases. IEEE Access 2021, 9, 67620–67633. [Google Scholar] [CrossRef]
- Advance Warning Methodologies for COVID-19 Using Chest X-ray Images. IEEE Access 2021, 9, 41052–41065. [CrossRef] [PubMed]
- Singh, G.; Yow, K.-C. These do not Look Like Those: An Interpretable Deep Learning Model for Image Recognition. IEEE Access 2021, 9, 41482–41493. [Google Scholar] [CrossRef]
- Ismael, A.M.; Şengür, A. Deep learning approaches for COVID-19 detection based on chest X-ray images. Expert Syst. Appl. 2021, 164, 114054. [Google Scholar] [CrossRef]
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Rajendra Acharya, U. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput. Biol. Med. 2020, 121, 103792. [Google Scholar] [CrossRef] [PubMed]
- Reis, H.C.; Turk, V. COVID-DSNet: A novel deep convolutional neural network for detection of coronavirus (SARS-CoV-2) cases from CT and Chest X-Ray images. Artif. Intell. Med. 2022, 134, 102427. [Google Scholar] [CrossRef] [PubMed]
- Szepesi, P.; Szilágyi, L. Detection of pneumonia using convolutional neural networks and deep learning. Biocybern. Biomed. Eng. 2022, 42, 1012–1022. [Google Scholar] [CrossRef]
- Kusk, M.W.; Lysdahlgaard, S. The effect of Gaussian noise on pneumonia detection on chest radiographs, using convolutional neural networks. Radiography 2023, 29, 38–43. [Google Scholar] [CrossRef]
- Umer, M.; Ashraf, I.; Ullah, S.; Mehmood, A.; Choi, G.S. COVINet: A convolutional neural network approach for predicting COVID-19 from chest X-ray images. J. Ambient Intell. Humaniz. Comput. 2022, 13, 535–547. [Google Scholar] [CrossRef]
- Rajawat, N.; Hada, B.S.; Meghawat, M.; Lalwani, S.; Kumar, R. C-COVIDNet: A CNN Model for COVID-19 Detection Using Image Processing. Arab. J. Sci. Eng. 2022, 47, 10811–10822. [Google Scholar] [CrossRef] [PubMed]
- Sedik, A.; Hammad, M.; Abd El-Samie, F.E.; Gupta, B.B.; Abd El-Latif, A.A. Efficient deep learning approach for augmented detection of Coronavirus disease. Neural Comput. Appl. 2022, 34, 11423–11440. [Google Scholar] [CrossRef]
- Subramanian, N.; Elharrouss, O.; Al-Maadeed, S.; Chowdhury, M. A review of deep learning-based detection methods for COVID-19. Comput. Biol. Med. 2022, 143, 105233. [Google Scholar] [CrossRef] [PubMed]
- Avola, D.; Bacciu, A.; Cinque, L.; Fagioli, A.; Marini, M.R.; Taiello, R. Study on transfer learning capabilities for pneumonia classification in chest-x-rays images. Comput. Methods Programs Biomed. 2022, 221, 106833. [Google Scholar] [CrossRef] [PubMed]
- Katsamenis, I.; Protopapadakis, E.; Voulodimos, A.; Doulamis, A.; Doulamis, N. Transfer Learning for COVID-19 Pneumonia Detection and Classification in Chest X-ray Images. In Proceedings of the 24th Pan-Hellenic Conference on Informatics, Volos, Greece, 26–28 November 2021; Association for Computing Machinery: New York, NY, USA, 2021; pp. 170–174. [Google Scholar]
- Pan, S.J.; Yang, Q. A Survey on Transfer Learning. IEEE Trans. Knowl. Data Eng. 2010, 22, 1345–1359. [Google Scholar] [CrossRef]
- Chamseddine, E.; Mansouri, N.; Soui, M.; Abed, M. Handling class imbalance in COVID-19 chest X-ray images classification: Using SMOTE and weighted loss. Appl. Soft Comput. 2022, 129, 109588. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, M.M.; Ahad, M.T.; Soma, F.A.; Paul, S.; Chowdhury, A.; Luna, S.A.; Yazdan, M.S.; Rahman, A.; Siddique, Z.; Huebner, P. Detecting SARS-CoV-2 From Chest X-ray Using Artificial Intelligence. IEEE Access 2021, 9, 35501–35513. [Google Scholar] [CrossRef] [PubMed]
- Aslan, M.F.; Unlersen, M.F.; Sabanci, K.; Durdu, A. CNN-based transfer learning–BiLSTM network: A novel approach for COVID-19 infection detection. Appl. Soft Comput. 2021, 98, 106912. [Google Scholar] [CrossRef] [PubMed]
- Karacı, A. VGGCOV19-NET: Automatic detection of COVID-19 cases from X-ray images using modified VGG19 CNN architecture and YOLO algorithm. Neural Comput. Appl. 2022, 34, 8253–8274. [Google Scholar] [CrossRef]
- Tahir, A.M.; Qiblawey, Y.; Khandakar, A.; Rahman, T.; Khurshid, U.; Musharavati, F.; Islam, M.T.; Kiranyaz, S.; Al-Maadeed, S.; Chowdhury, M.E.H. Deep Learning for Reliable Classification of COVID-19, MERS, and SARS from Chest X-ray Images. Cogn. Comput. 2022, 14, 1752–1772. [Google Scholar] [CrossRef]
- Chouat, I.; Echtioui, A.; Khemakhem, R.; Zouch, W.; Ghorbel, M.; Hamida, A.B. COVID-19 detection in CT and CXR images using deep learning models. Biogerontology 2022, 23, 65–84. [Google Scholar] [CrossRef] [PubMed]
- Dialameh, M.; Hamzeh, A.; Rahmani, H.; Radmard, A.R.; Dialameh, S. Proposing a novel deep network for detecting COVID-19 based on chest images. Sci. Rep. 2022, 12, 3116. [Google Scholar] [CrossRef] [PubMed]
- Shoaib, M.R.; Emara, H.M.; Elwekeil, M.; El-Shafai, W.; Taha, T.E.; El-Fishawy, A.S.; El-Rabaie, E.-S.M.; El-Samie, F.E.A. Hybrid classification structures for automatic COVID-19 detection. J. Ambient Intell. Humaniz. Comput. 2022, 13, 4477–4492. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, S.G.; Aloyuni, S.A.; Alharbi, R.A.; Alqahtani, T.; Sikkandar, M.Y.; Subbiah, C. Deep Transfer Learning Based Unified Framework for COVID19 Classification and Infection Detection from Chest X-Ray Images. Arab. J. Sci. Eng. 2022, 47, 1675–1692. [Google Scholar] [CrossRef] [PubMed]
- Heidari, M.; Mirniaharikandehei, S.; Khuzani, A.Z.; Danala, G.; Qiu, Y.; Zheng, B. Improving the performance of CNN to predict the likelihood of COVID-19 using chest X-ray images with preprocessing algorithms. Int. J. Med. Inf. 2020, 144, 104284. [Google Scholar] [CrossRef] [PubMed]
- Imagawa, K.; Shiomoto, K. Performance change with the number of training data: A case study on the binary classification of COVID-19 chest X-ray by using convolutional neural networks. Comput. Biol. Med. 2022, 142, 105251. [Google Scholar] [CrossRef] [PubMed]
- Gazda, M.; Plavka, J.; Gazda, J.; Drotár, P. Self-Supervised Deep Convolutional Neural Network for Chest X-Ray Classification. IEEE Access 2021, 9, 151972–151982. [Google Scholar] [CrossRef]
- Jena, B.; Saxena, S.; Nayak, G.K.; Saba, L.; Sharma, N.; Suri, J.S. Artificial intelligence-based hybrid deep learning models for image classification: The first narrative review. Comput. Biol. Med. 2021, 137, 104803. [Google Scholar] [CrossRef]
- Shouman, M.A.; El-Fiky, A.; Hamada, S.; El-Sayed, A.; Karar, M.E. Computer-assisted lung diseases detection from pediatric chest radiography using long short-term memory networks. Comput. Electr. Eng. 2022, 103, 108402. [Google Scholar] [CrossRef]
- Sourab, S.Y.; Kabir, M.A. A comparison of hybrid deep learning models for pneumonia diagnosis from chest radiograms. Sens. Int. 2022, 3, 100167. [Google Scholar] [CrossRef]
- Jin, W.; Dong, S.; Dong, C.; Ye, X. Hybrid ensemble model for differential diagnosis between COVID-19 and common viral pneumonia by chest X-ray radiograph. Comput. Biol. Med. 2021, 131, 104252. [Google Scholar] [CrossRef] [PubMed]
- Nandi, R.; Mulimani, M. Detection of COVID-19 from X-rays using hybrid deep learning models. Res. Biomed. Eng. 2021, 37, 687–695. [Google Scholar] [CrossRef]
- Shah, P.M.; Ullah, F.; Shah, D.; Gani, A.; Maple, C.; Wang, Y.; Shahid; Abrar, M.; Islam, S.U. Deep GRU-CNN Model for COVID-19 Detection From Chest X-rays Data. IEEE Access 2022, 10, 35094–35105. [Google Scholar] [CrossRef] [PubMed]
- Kaya, M. Feature fusion-based ensemble CNN learning optimization for automated detection of pediatric pneumonia. Biomed. Signal Process. Control 2024, 87, 105472. [Google Scholar] [CrossRef]
- Bhatt, H.; Shah, M. A Convolutional Neural Network ensemble model for Pneumonia Detection using chest X-ray images. Healthc. Anal. 2023, 3, 100176. [Google Scholar] [CrossRef]
- Srivastava, G.; Pradhan, N.; Saini, Y. Ensemble of Deep Neural Networks based on Condorcet’s Jury Theorem for screening COVID-19 and Pneumonia from radiograph images. Comput. Biol. Med. 2022, 149, 105979. [Google Scholar] [CrossRef]
- Mabrouk, A.; Díaz Redondo, R.P.; Abd Elaziz, M.; Kayed, M. Ensemble Federated Learning: An approach for collaborative pneumonia diagnosis. Appl. Soft Comput. 2023, 144, 110500. [Google Scholar] [CrossRef]
- Sahoo, P.; Saha, S.; Sharma, S.K.; Mondal, S.; Gowda, S. A Multi-stage framework for COVID-19 detection and severity assessment from chest radiography images using advanced fuzzy ensemble technique. Expert Syst. Appl. 2023, 238, 121724. [Google Scholar] [CrossRef]
- Balasubramaniam, S.; Satheesh Kumar, K. Optimal Ensemble learning model for COVID-19 detection using chest X-ray images. Biomed. Signal Process. Control 2023, 81, 104392. [Google Scholar] [CrossRef]
- Kushal, K.S.; Ahmed, T.; Uddin, M.A.; Uddin, M.N. A Blockchain-Based Framework for COVID-19 Detection Using Stacking Ensemble of Pre-Trained Models. Comput. Methods Programs Biomed. Update 2023, 4, 100116. [Google Scholar] [CrossRef]
- Zhang, Y.; Weng, Y.; Lund, J. Applications of Explainable Artificial Intelligence in Diagnosis and Surgery. Diagnostics 2022, 12, 237. [Google Scholar] [CrossRef] [PubMed]
- Tjoa, E.; Guan, C. A Survey on Explainable Artificial Intelligence (XAI): Toward Medical XAI. IEEE Trans. Neural Netw. Learn. Syst. 2021, 32, 4793–4813. [Google Scholar] [CrossRef] [PubMed]
- Adadi, A.; Berrada, M. Peeking Inside the Black-Box: A Survey on Explainable Artificial Intelligence (XAI). IEEE Access 2018, 6, 52138–52160. [Google Scholar] [CrossRef]
- Zou, L.; Goh, H.L.; Liew, C.J.Y.; Quah, J.L.; Gu, G.T.; Chew, J.J.; Prem Kumar, M.; Ang, C.G.L.; Ta, A. Ensemble image explainable AI (XAI) algorithm for severe community-acquired pneumonia and COVID-19 respiratory infections. IEEE Trans. Artif. Intell. 2022, 4, 242–254. [Google Scholar] [CrossRef]
- Ren, H.; Wong, A.B.; Lian, W.; Cheng, W.; Zhang, Y.; He, J.; Liu, Q.; Yang, J.; Zhang, C.J.; Wu, K.; et al. Interpretable Pneumonia Detection by Combining Deep Learning and Explainable Models With Multisource Data. IEEE Access 2021, 9, 95872–95883. [Google Scholar] [CrossRef]
- Catalá, O.D.T.; Igual, I.S.; Pérez-Benito, F.J.; Escrivá, D.M.; Castelló, V.O.; Llobet, R.; Peréz-Cortés, J.-C. Bias Analysis on Public X-Ray Image Datasets of Pneumonia and COVID-19 Patients. IEEE Access 2021, 9, 42370–42383. [Google Scholar] [CrossRef] [PubMed]
- Minaee, S.; Kafieh, R.; Sonka, M.; Yazdani, S.; Jamalipour Soufi, G. Deep-COVID: Predicting COVID-19 from chest X-ray images using deep transfer learning. Med. Image Anal. 2020, 65, 101794. [Google Scholar] [CrossRef] [PubMed]
- Marques, G.; Agarwal, D.; de la Torre Díez, I. Automated medical diagnosis of COVID-19 through EfficientNet convolutional neural network. Appl. Soft Comput. 2020, 96, 106691. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.; Park, S.; Ye, J.C. Deep Learning COVID-19 Features on CXR Using Limited Training Data Sets. IEEE Trans. Med. Imaging 2020, 39, 2688–2700. [Google Scholar] [CrossRef]
- Das, D.; Santosh, K.C.; Pal, U. Truncated inception net: COVID-19 outbreak screening using chest X-rays. Phys. Eng. Sci. Med. 2020, 43, 915–925. [Google Scholar] [CrossRef]
- Mukherjee, H.; Ghosh, S.; Dhar, A.; Obaidullah, S.M.; Santosh, K.C.; Roy, K. Shallow Convolutional Neural Network for COVID-19 Outbreak Screening Using Chest X-rays. Cogn. Comput. 2021, 16, 1695–1708. [Google Scholar] [CrossRef]
- Ghassemi, M.; Oakden-Rayner, L.; Beam, A.L. The false hope of current approaches to explainable artificial intelligence in health care. Lancet Digit. Health 2021, 3, e745–e750. [Google Scholar] [CrossRef] [PubMed]
- Bodapati, J.D.; Rohith, V.N.; Dondeti, V. Ensemble of deep capsule neural networks: An application to pediatric pneumonia prediction. Phys. Eng. Sci. Med. 2022, 45, 949–959. [Google Scholar] [CrossRef]
- Bodapati, J.D.; Rohith, V.N. ChxCapsNet: Deep capsule network with transfer learning for evaluating pneumonia in paediatric chest radiographs. Measurement 2022, 188, 110491. [Google Scholar] [CrossRef]
- Kör, H.; Erbay, H.; Yurttakal, A.H. Diagnosing and differentiating viral pneumonia and COVID-19 using X-ray images. Multimed. Tools Appl. 2022, 81, 39041–39057. [Google Scholar] [CrossRef]
- Sasikaladevi, N.; Revathi, A. Intelligent prognostic system for pediatric pneumonia based on sustainable IoHT. Multimed. Tools Appl. 2023, 82, 26901–26917. [Google Scholar] [CrossRef]
- Liz, H.; Sánchez-Montañés, M.; Tagarro, A.; Domínguez-Rodríguez, S.; Dagan, R.; Camacho, D. Ensembles of Convolutional Neural Network models for pediatric pneumonia diagnosis. Future Gener. Comput. Syst. 2021, 122, 220–233. [Google Scholar] [CrossRef]
- Prakash, J.A.; Ravi, V.; Sowmya, V.; Soman, K.P. Stacked ensemble learning based on deep convolutional neural networks for pediatric pneumonia diagnosis using chest X-ray images. Neural Comput. Appl. 2023, 35, 8259–8279. [Google Scholar] [CrossRef]
- Arun Prakash, J.; Asswin, C.R.; Dharshan Kumar, K.S.; Avinash, D.; Vinayakumar, R.; Sowmya, V.; Gopalakrishnan, E.A.; Soman, K.P. Transfer learning approach for pediatric pneumonia diagnosis using channel attention deep CNN architectures. Eng. Appl. Artif. Intell. 2023, 123, 106416. [Google Scholar] [CrossRef]
- Arun Prakash, J.; Asswin, C.; Ravi, V.; Sowmya, V.; Soman, K. Pediatric pneumonia diagnosis using stacked ensemble learning on multi-model deep CNN architectures. Multimed. Tools Appl. 2023, 82, 21311–21351. [Google Scholar] [CrossRef]
- Gaur, L.; Bhatia, U.; Jhanjhi, N.Z.; Muhammad, G.; Masud, M. Medical image-based detection of COVID-19 using Deep Convolution Neural Networks. Multimed. Syst. 2023, 29, 1729–1738. [Google Scholar] [CrossRef] [PubMed]
- Paul, A.; Basu, A.; Mahmud, M.; Kaiser, M.S.; Sarkar, R. Inverted bell-curve-based ensemble of deep learning models for detection of COVID-19 from chest X-rays. Neural Comput. Appl. 2023, 35, 16113–16127. [Google Scholar] [CrossRef] [PubMed]
- Mondal, A.K. COVID-19 prognosis using limited chest X-ray images. Appl. Soft Comput. 2022, 122, 108867. [Google Scholar] [CrossRef] [PubMed]
- RSNA Pneumonia Detection Challenge. Available online: https://kaggle.com/competitions/rsna-pneumonia-detection-challenge (accessed on 8 September 2023).
- Lakhani, P.; Mongan, J.; Singhal, C.; Zhou, Q.; Andriole, K.P.; Auffermann, W.F.; Prasanna, P.M.; Pham, T.X.; Peterson, M.; Bergquist, P.J.; et al. The 2021 SIIM-FISABIO-RSNA Machine Learning COVID-19 Challenge: Annotation and Standard Exam Classification of COVID-19 Chest Radiographs. J. Digit. Imaging 2023, 36, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Xue, P.; Zhang, Z.; Dong, E. PKA2-Net: Prior Knowledge-Based Active Attention Network for Accurate Pneumonia Diagnosis on Chest X-ray Images. IEEE J. Biomed. Health Inform. 2023, 27, 3513–3524. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Wang, Z.; Xu, X.; Wang, Y.; Fu, H.; Li, S.; Zhen, L.; Lei, X.; Cui, Y.; Sim Zheng Ting, J.; et al. Contrastive domain adaptation with consistency match for automated pneumonia diagnosis. Med. Image Anal. 2023, 83, 102664. [Google Scholar] [CrossRef] [PubMed]
- Malik, H.; Anees, T.; Din, M.; Naeem, A. CDC_Net: Multi-classification convolutional neural network model for detection of COVID-19, pneumothorax, pneumonia, lung Cancer, and tuberculosis using chest X-rays. Multimed. Tools Appl. 2023, 82, 13855–13880. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Bajwa, U.I.; Mehmood, Y.; Anwar, M.W. Lightweight ResGRU: A deep learning-based prediction of SARS-CoV-2 (COVID-19) and its severity classification using multimodal chest radiography images. Neural Comput. Appl. 2023, 35, 9637–9655. [Google Scholar] [CrossRef] [PubMed]
- Elhanashi, A.; Saponara, S.; Zheng, Q. Classification and Localization of Multi-Type Abnormalities on Chest X-rays Images. IEEE Access 2023, 11, 83264–83277. [Google Scholar] [CrossRef]
- Khero, K.; Usman, M.; Fong, A. Deep learning framework for early detection of COVID-19 using X-ray images. Multimed. Tools Appl. 2023, 83, 6883–6908. [Google Scholar] [CrossRef]
- NIH Chest X-rays. Available online: https://www.kaggle.com/datasets/nih-chest-xrays/data (accessed on 8 September 2023).
- Santomartino, S.M.; Hafezi-Nejad, N.; Parekh, V.S.; Yi, P.H. Performance and Usability of Code-Free Deep Learning for Chest Radiograph Classification, Object Detection, and Segmentation. Radiol. Artif. Intell. 2023, 5, e220062. [Google Scholar] [CrossRef]
- Sheu, R.-K.; Pardeshi, M.S.; Pai, K.-C.; Chen, L.-C.; Wu, C.-L.; Chen, W.-C. Interpretable Classification of Pneumonia Infection Using eXplainable AI (XAI-ICP). IEEE Access 2023, 11, 28896–28919. [Google Scholar] [CrossRef]
- Chetoui, M.; Akhloufi, M.A.; Bouattane, E.M.; Abdulnour, J.; Roux, S.; Bernard, C.D. Explainable COVID-19 Detection Based on Chest X-rays Using an End-to-End RegNet Architecture. Viruses 2023, 15, 1327. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Lu, X.; Yuan, J. MHA-CoroCapsule: Multi-Head Attention Routing-Based Capsule Network for COVID-19 Chest X-Ray Image Classification. IEEE Trans. Med. Imaging 2022, 41, 1208–1218. [Google Scholar] [CrossRef] [PubMed]
- de Moura, J.; Novo, J.; Ortega, M. Fully automatic deep convolutional approaches for the analysis of COVID-19 using chest X-ray images. Appl. Soft Comput. 2022, 115, 108190. [Google Scholar] [CrossRef] [PubMed]
- Nahiduzzaman; Goni, O.F.; Hassan, R.; Islam, R.; Syfullah, M.K.; Shahriar, S.M.; Anower, S.; Ahsan, M.; Haider, J.; Kowalski, M. Parallel CNN-ELM: A multiclass classification of chest X-ray images to identify seventeen lung diseases including COVID-19. Expert Syst. Appl. 2023, 229, 120528. [Google Scholar] [CrossRef]
- Rajagopal, R.; Karthick, R.; Meenalochini, P.; Kalaichelvi, T. Deep Convolutional Spiking Neural Network optimized with Arithmetic optimization algorithm for lung disease detection using chest X-ray images. Biomed. Signal Process. Control 2023, 79, 104197. [Google Scholar] [CrossRef]
- Bhosale, Y.H.; Patnaik, K.S. PulDi-COVID: Chronic obstructive pulmonary (lung) diseases with COVID-19 classification using ensemble deep convolutional neural network from chest X-ray images to minimize severity and mortality rates. Biomed. Signal Process. Control 2023, 81, 104445. [Google Scholar] [CrossRef] [PubMed]
- Xin, K.Z.; Li, D.; Yi, P.H. Limited generalizability of deep learning algorithm for pediatric pneumonia classification on external data. Emerg. Radiol. 2022, 29, 107–113. [Google Scholar] [CrossRef]
- Cohen, J.P. Ieee8023/Covid-Chestxray-Dataset. Available online: https://github.com/ieee8023/covid-chestxray-dataset (accessed on 8 September 2023).
- Cohen, J.P.; Morrison, P.; Dao, L. COVID-19 Image Data Collection. arxiv 2020, arXiv:2003.11597. [Google Scholar]
- Cohen, J.P.; Morrison, P.; Dao, L.; Roth, K.; Duong, T.Q.; Ghassemi, M. COVID-19 Image Data Collection: Prospective Predictions Are the Future. Mach. Learn. Biomed. Imaging 2020, 1, 1–38. [Google Scholar] [CrossRef]
- Pham, T.D. Classification of COVID-19 chest X-rays with deep learning: New models or fine tuning? Health Inf. Sci. Syst. 2020, 9, 2. [Google Scholar] [CrossRef] [PubMed]
- Patro, K.K.; Allam, J.P.; Hammad, M.; Tadeusiewicz, R.; Pławiak, P. SCovNet: A skip connection-based feature union deep learning technique with statistical approach analysis for the detection of COVID-19. Biocybern. Biomed. Eng. 2023, 43, 352–368. [Google Scholar] [CrossRef] [PubMed]
- Raghavendran, P.S.; Ragul, S.; Asokan, R.; Loganathan, A.K.; Muthusamy, S.; Mishra, O.P.; Ramamoorthi, P.; Sundararajan, S.C.M. A new method for chest X-ray images categorization using transfer learning and CovidNet_2020 employing convolution neural network. Soft Comput. 2023, 27, 14241–14251. [Google Scholar] [CrossRef]
- Wang, T.; Nie, Z.; Wang, R.; Xu, Q.; Huang, H.; Xu, H.; Xie, F.; Liu, X.-J. PneuNet: Deep learning for COVID-19 pneumonia diagnosis on chest X-ray image analysis using Vision Transformer. Med. Biol. Eng. Comput. 2023, 61, 1395–1408. [Google Scholar] [CrossRef] [PubMed]
- Novel COVID-19 Chestxray Repository. Available online: https://www.kaggle.com/datasets/subhankarsen/novel-covid19-chestxray-repository (accessed on 11 September 2023).
- Bhowal, P.; Sen, S.; Yoon, J.H.; Geem, Z.W.; Sarkar, R. Choquet Integral and Coalition Game-Based Ensemble of Deep Learning Models for COVID-19 Screening From Chest X-ray Images. IEEE J. Biomed. Health Inform. 2021, 25, 4328–4339. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Chest X-ray. Available online: https://www.kaggle.com/datasets/ahmedtronic/covid-19-chest-x-ray (accessed on 12 September 2023).
- Haghanifar, A.; Majdabadi, M.M.; Choi, Y.; Deivalakshmi, S.; Ko, S. COVID-CXNet: Detecting COVID-19 in frontal chest X-ray images using deep learning. Multimed. Tools Appl. 2022, 81, 30615–30645. [Google Scholar] [CrossRef] [PubMed]
- Sait, U.; Lal KV, G.; Prakash Prajapati, S.; Bhaumik, R.; Kumar, T.; Shivakumar, S.; Bhalla, K. Curated Dataset for COVID-19 Posterior-Anterior Chest Radiography Images (X-rays). 2021, Version 3. Available online: https://data.mendeley.com/datasets/9xkhgts2s6/3 (accessed on 9 June 2024).
- Mahmud, T.; Rahman, M.A.; Fattah, S.A. CovXNet: A multi-dilation convolutional neural network for automatic COVID-19 and other pneumonia detection from chest X-ray images with transferable multi-receptive feature optimization. Comput. Biol. Med. 2020, 122, 103869. [Google Scholar] [CrossRef] [PubMed]
- Sait, U.; Lal K.V., G.; Shivakumar, S.; Kumar, T.; Bhaumik, R.; Prajapati, S.; Bhalla, K.; Chakrapani, A. A deep-learning based multimodal system for COVID-19 diagnosis using breathing sounds and chest X-ray images. Appl. Soft Comput. 2021, 109, 107522. [Google Scholar] [CrossRef]
- Hariri, M.; Avşar, E. COVID-19 and pneumonia diagnosis from chest X-ray images using convolutional neural networks. Netw. Model. Anal. Health Inform. Bioinform. 2023, 12, 17. [Google Scholar] [CrossRef]
- Kumar, S. COVID-19-Pneumonia-Normal Chest X-Ray Images. 2022, Version 1. Available online: https://www.sciencedirect.com/science/article/pii/S1568494621004452?via%3Dihub (accessed on 9 June 2024).
- Shastri, S.; Kansal, I.; Kumar, S.; Singh, K.; Popli, R.; Mansotra, V. CheXImageNet: A novel architecture for accurate classification of COVID-19 with chest X-ray digital images using deep convolutional neural networks. Health Technol. 2022, 12, 193–204. [Google Scholar] [CrossRef]
- Kumar, S.; Shastri, S.; Mahajan, S.; Singh, K.; Gupta, S.; Rani, R.; Mohan, N.; Mansotra, V. LiteCovidNet: A lightweight deep neural network model for detection of COVID-19 using X-ray images. Int. J. Imaging Syst. Technol. 2022, 32, 1464–1480. [Google Scholar] [CrossRef] [PubMed]
- Podder, P.; Das, S.R.; Mondal, M.R.H.; Bharati, S.; Maliha, A.; Hasan, M.J.; Piltan, F. LDDNet: A Deep Learning Framework for the Diagnosis of Infectious Lung Diseases. Sensors 2023, 23, 480. [Google Scholar] [CrossRef]
- Hamad, Q.S.; Samma, H.; Suandi, S.A. Feature selection of pre-trained shallow CNN using the QLESCA optimizer: COVID-19 detection as a case study. Appl. Intell. 2023, 53, 18630–18652. [Google Scholar] [CrossRef]
- Asraf, A.; Islam, Z. COVID19, Pneumonia and Normal Chest X-ray PA Dataset. 2021, Version 1. Available online: https://www.mdpi.com/1424-8220/23/1/480 (accessed on 9 June 2024).
- Wahid, F.; Azhar, S.; Ali, S.; Zia, M.S.; Abdulaziz Almisned, F.; Gumaei, A. Pneumonia Detection in Chest X-Ray Images Using Enhanced Restricted Boltzmann Machine. J. Healthc. Eng. 2022, 2022, 1678000. [Google Scholar] [CrossRef]
- COVID-19 Radiography Database. Available online: https://www.kaggle.com/datasets/tawsifurrahman/covid19-radiography-database (accessed on 12 September 2023).
- Visuña, L.; Yang, D.; Garcia-Blas, J.; Carretero, J. Computer-aided diagnostic for classifying chest X-ray images using deep ensemble learning. BMC Med. Imaging 2022, 22, 178. [Google Scholar] [CrossRef] [PubMed]
- Lasker, A.; Ghosh, M.; Obaidullah, S.M.; Chakraborty, C.; Roy, K. LWSNet—A novel deep-learning architecture to segregate Covid-19 and pneumonia from X-ray imagery. Multimed. Tools Appl. 2023, 82, 21801–21823. [Google Scholar] [CrossRef]
- Danilov, V.V.; Litmanovich, D.; Proutski, A.; Kirpich, A.; Nefaridze, D.; Karpovsky, A.; Gankin, Y. Automatic scoring of COVID-19 severity in X-ray imaging based on a novel deep learning workflow. Sci. Rep. 2022, 12, 12791. [Google Scholar] [CrossRef]
- Shazia, A.; Xuan, T.Z.; Chuah, J.H.; Usman, J.; Qian, P.; Lai, K.W. A comparative study of multiple neural network for detection of COVID-19 on chest X-ray. EURASIP J. Adv. Signal Process. 2021, 2021, 50. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.R.; Armando Cardona Cardenas, D.; Moreno, R.A.; de Fátima de Sá Rebelo, M.; Krieger, J.E.; Antonio Gutierrez, M. Multi-View Ensemble Convolutional Neural Network to Improve Classification of Pneumonia in Low Contrast Chest X-Ray Images. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 1238–1241. [Google Scholar]
- Chharia, A.; Upadhyay, R.; Kumar, V.; Cheng, C.; Zhang, J.; Wang, T.; Xu, M. Deep-Precognitive Diagnosis: Preventing Future Pandemics by Novel Disease Detection With Biologically-Inspired Conv-Fuzzy Network. IEEE Access 2022, 10, 23167–23185. [Google Scholar] [CrossRef]
- Nahiduzzaman; Goni, O.F.; Anower, S.; Islam, R.; Ahsan, M.; Haider, J.; Gurusamy, S.; Hassan, R.; Islam, R. A Novel Method for Multivariant Pneumonia Classification Based on Hybrid CNN-PCA Based Feature Extraction Using Extreme Learning Machine With CXR Images. IEEE Access 2021, 9, 147512–147526. [Google Scholar] [CrossRef]
- Yi, R.; Tang, L.; Tian, Y.; Liu, J.; Wu, Z. Identification and classification of pneumonia disease using a deep learning-based intelligent computational framework. Neural Comput. Appl. 2023, 35, 14473–14486. [Google Scholar] [CrossRef] [PubMed]
- Aljawarneh, S.A.; Al-Quraan, R. Pneumonia Detection Using Enhanced Convolutional Neural Network Model on Chest X-Ray Images. Big Data 2023. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Alshmrani, G.M.M.; Ni, Q.; Jiang, R.; Pervaiz, H.; Elshennawy, N.M. A deep learning architecture for multi-class lung diseases classification using chest X-ray (CXR) images. Alex. Eng. J. 2023, 64, 923–935. [Google Scholar] [CrossRef]
- Sanghvi, H.A.; Patel, R.H.; Agarwal, A.; Gupta, S.; Sawhney, V.; Pandya, A.S. A deep learning approach for classification of COVID and pneumonia using DenseNet-201. Int. J. Imaging Syst. Technol. 2023, 33, 18–38. [Google Scholar] [CrossRef] [PubMed]
- Ukwuoma, C.C.; Qin, Z.; Belal Bin Heyat, M.; Akhtar, F.; Bamisile, O.; Muaad, A.Y.; Addo, D.; Al-antari, M.A. A hybrid explainable ensemble transformer encoder for pneumonia identification from chest X-ray images. J. Adv. Res. 2023, 48, 191–211. [Google Scholar] [CrossRef] [PubMed]
- Ravi, V.; Acharya, V.; Alazab, M. A multichannel EfficientNet deep learning-based stacking ensemble approach for lung disease detection using chest X-ray images. Clust. Comput. 2023, 26, 1181–1203. [Google Scholar] [CrossRef] [PubMed]
- Erdogan Yildirim, A.; Canayaz, M. A novel deep learning-based approach for prediction of neonatal respiratory disorders from chest X-ray images. Biocybern. Biomed. Eng. 2023, 43, 635–655. [Google Scholar] [CrossRef]
- Bal, U.; Bal, A.; Moral, Ö.T.; Düzgün, F.; Gürbüz, N. A deep learning feature extraction-based hybrid approach for detecting pediatric pneumonia in chest X-ray images. Phys. Eng. Sci. Med. 2024, 47, 109–117. [Google Scholar] [CrossRef]
- Chen, S.; Ren, S.; Wang, G.; Huang, M.; Xue, C. Interpretable CNN-Multilevel Attention Transformer for Rapid Recognition of Pneumonia from Chest X-Ray Images. IEEE J. Biomed. Health Inform. 2024, 28, 753–764. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv 2015, arXiv:1409.1556. [Google Scholar] [CrossRef]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Fei-Fei, L. ImageNet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. Int. J. Comput. Vis. 2020, 128, 336–359. [Google Scholar] [CrossRef]
- Garcia Santa Cruz, B.; Bossa, M.N.; Sölter, J.; Husch, A.D. Public COVID-19 X-ray datasets and their impact on model bias–A systematic review of a significant problem. Med. Image Anal. 2021, 74, 102225. [Google Scholar] [CrossRef] [PubMed]
- Zunaed, M.; Haque, A.; Hasan, T. Learning to Generalize Towards Unseen Domains via a Content-Aware Style Invariant Model for Disease Detection From Chest X-rays. IEEE J. Biomed. Health Inform. 2024, 28, 3626–3636. [Google Scholar] [CrossRef] [PubMed]
- Horry, M.J.; Chakraborty, S.; Pradhan, B.; Paul, M.; Zhu, J.; Loh, H.W.; Barua, P.D.; Acharya, U.R. Development of Debiasing Technique for Lung Nodule Chest X-ray Datasets to Generalize Deep Learning Models. Sensors 2023, 23, 6585. [Google Scholar] [CrossRef]
- Arias-Garzón, D.; Tabares-Soto, R.; Bernal-Salcedo, J.; Ruz, G.A. Biases associated with database structure for COVID-19 detection in X-ray images. Sci. Rep. 2023, 13, 3477. [Google Scholar] [CrossRef]
- Afshar, P.; Heidarian, S.; Naderkhani, F.; Oikonomou, A.; Plataniotis, K.N.; Mohammadi, A. COVID-CAPS: A capsule network-based framework for identification of COVID-19 cases from X-ray images. Pattern Recognit. Lett. 2020, 138, 638–643. [Google Scholar] [CrossRef]
- Pereira, R.M.; Bertolini, D.; Teixeira, L.O.; Silla, C.N.; Costa, Y.M.G. COVID-19 identification in chest X-ray images on flat and hierarchical classification scenarios. Comput. Methods Programs Biomed. 2020, 194, 105532. [Google Scholar] [CrossRef]
- Jia, L.-L.; Zhao, J.-X.; Pan, N.-N.; Shi, L.-Y.; Zhao, L.-P.; Tian, J.-H.; Huang, G. Artificial intelligence model on chest imaging to diagnose COVID-19 and other pneumonias: A systematic review and meta-analysis. Eur. J. Radiol. Open 2022, 9, 100438. [Google Scholar] [CrossRef]
- Aslani, S.; Jacob, J. Utilisation of deep learning for COVID-19 diagnosis. Clin. Radiol. 2023, 78, 150–157. [Google Scholar] [CrossRef]
- Wang, Z.; Xiao, Y.; Li, Y.; Zhang, J.; Lu, F.; Hou, M.; Liu, X. Automatically discriminating and localizing COVID-19 from community-acquired pneumonia on chest X-rays. Pattern Recognit. 2021, 110, 107613. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Anjum; Gupta, S.; Katarya, R. InstaCovNet-19: A deep learning classification model for the detection of COVID-19 patients using Chest X-ray. Appl. Soft Comput. 2021, 99, 106859. [Google Scholar] [CrossRef] [PubMed]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Explainable Deep Learning for Pulmonary Disease and Coronavirus COVID-19 Detection from X-rays. Comput. Methods Programs Biomed. 2020, 196, 105608. [Google Scholar] [CrossRef]
- Nazir, S.; Dickson, D.M.; Akram, M.U. Survey of explainable artificial intelligence techniques for biomedical imaging with deep neural networks. Comput. Biol. Med. 2023, 156, 106668. [Google Scholar] [CrossRef]
- Jangam, E.; Annavarapu, C.S.R.; Barreto, A.A.D. A multi-class classification framework for disease screening and disease diagnosis of COVID-19 from chest X-ray images. Multimed. Tools Appl. 2023, 82, 14367–14401. [Google Scholar] [CrossRef]
- Ong, J.H.; Goh, K.M.; Lim, L.L. Comparative Analysis of Explainable Artificial Intelligence for COVID-19 Diagnosis on CXR Image. In Proceedings of the 2021 IEEE International Conference on Signal and Image Processing Applications (ICSIPA), Kuala Terengganu, Malaysia, 13–15 September 2021; pp. 185–190. [Google Scholar]
- Karim, R.; Döhmen, T.; Cochez, M.; Beyan, O.; Rebholz-Schuhmann, D.; Decker, S. DeepCOVIDExplainer: Explainable COVID-19 Diagnosis from Chest X-ray Images. In Proceedings of the 2020 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Seoul, Republic of Korea, 16–19 December 2020; pp. 1034–1037. [Google Scholar]
- Guidotti, R.; Monreale, A.; Ruggieri, S.; Turini, F.; Giannotti, F.; Pedreschi, D. A Survey of Methods for Explaining Black Box Models. ACM Comput. Surv. 2018, 51, 1–42. [Google Scholar] [CrossRef]
- Gillmann, C.; Smit, N.N.; Gröller, E.; Preim, B.; Vilanova, A.; Wischgoll, T. Ten Open Challenges in Medical Visualization. IEEE Comput. Graph. Appl. 2021, 41, 7–15. [Google Scholar] [CrossRef]
- Nour, M.; Cömert, Z.; Polat, K. A Novel Medical Diagnosis model for COVID-19 infection detection based on Deep Features and Bayesian Optimization. Appl. Soft Comput. 2020, 97, 106580. [Google Scholar] [CrossRef]
- Li, Z.; Kamnitsas, K.; Glocker, B. Overfitting of Neural Nets Under Class Imbalance: Analysis and Improvements for Segmentation. In Proceedings of the Medical Image Computing and Computer Assisted Intervention–MICCAI 2019, Shenzhen, China, 13–17 October 2019; Shen, D., Liu, T., Peters, T.M., Staib, L.H., Essert, C., Zhou, S., Yap, P.-T., Khan, A., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 402–410. [Google Scholar]
- Fernández, A.; García, S.; Herrera, F. Addressing the Classification with Imbalanced Data: Open Problems and New Challenges on Class Distribution. In Proceedings of the Hybrid Artificial Intelligent Systems; Corchado, E., Kurzyński, M., Woźniak, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 1–10. [Google Scholar]
- Hertel, R.; Benlamri, R. Deep Learning Techniques for COVID-19 Diagnosis and Prognosis Based on Radiological Imaging. ACM Comput. Surv. 2023, 55, 39. [Google Scholar] [CrossRef]
- Rajaraman, S.; Siegelman, J.; Alderson, P.O.; Folio, L.S.; Folio, L.R.; Antani, S.K. Iteratively Pruned Deep Learning Ensembles for COVID-19 Detection in Chest X-rays. IEEE Access 2020, 8, 115041–115050. [Google Scholar] [CrossRef]
- Alom, M.Z.; Rahman, M.M.S.; Nasrin, M.S.; Taha, T.M.; Asari, V.K. COVID_MTNet: COVID-19 Detection with Multi-Task Deep Learning Approaches. arXiv 2020, arXiv:2004.03747. [Google Scholar] [CrossRef]
- Khattab, R.; Abdelmaksoud, I.R.; Abdelrazek, S. Automated detection of COVID-19 and pneumonia diseases using data mining and transfer learning algorithms with focal loss from chest X-ray images. Appl. Soft Comput. 2024, 162, 111806. [Google Scholar] [CrossRef]
- Siddiqi, R.; Ahraf, S.N.; Kandhro, I.A. Susceptibility of paediatric pneumonia detection model under projected gradient descent adversarial attacks. Int. J. Electron. Secur. Digit. Forensics 2023, 15, 322–331. [Google Scholar] [CrossRef]
- Kaviani, S.; Han, K.J.; Sohn, I. Adversarial attacks and defenses on AI in medical imaging informatics: A survey. Expert Syst. Appl. 2022, 198, 116815. [Google Scholar] [CrossRef]
- Asgari Taghanaki, S.; Das, A.; Hamarneh, G. Vulnerability Analysis of Chest X-ray Image Classification Against Adversarial Attacks. In Understanding and Interpreting Machine Learning in Medical Image Computing Applications; Stoyanov, D., Taylor, Z., Kia, S.M., Oguz, I., Reyes, M., Martel, A., Maier-Hein, L., Marquand, A.F., Duchesnay, E., Löfstedt, T., et al., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 87–94. [Google Scholar]
- Xu, M.; Zhang, T.; Zhang, D. MedRDF: A Robust and Retrain-Less Diagnostic Framework for Medical Pretrained Models Against Adversarial Attack. IEEE Trans. Med. Imaging 2022, 41, 2130–2143. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.; Liu, F.; Xu, K.; Shi, X. Why does batch normalization induce the model vulnerability on adversarial images? World Wide Web 2023, 26, 1073–1091. [Google Scholar] [CrossRef]
- Das, D.; Biswas, S.K.; Bandyopadhyay, S. Perspective of AI system for COVID-19 detection using chest images: A review. Multimed. Tools Appl. 2022, 81, 21471–21501. [Google Scholar] [CrossRef] [PubMed]
- Paschali, M.; Conjeti, S.; Navarro, F.; Navab, N. Generalizability vs. Robustness: Investigating Medical Imaging Networks Using Adversarial Examples. In Proceedings of the Medical Image Computing and Computer Assisted Intervention–MICCAI 2018, Granada, Spain, 16–20 September 2018; Frangi, A.F., Schnabel, J.A., Davatzikos, C., Alberola-López, C., Fichtinger, G., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 493–501. [Google Scholar]
- Ma, X.; Niu, Y.; Gu, L.; Wang, Y.; Zhao, Y.; Bailey, J.; Lu, F. Understanding adversarial attacks on deep learning based medical image analysis systems. Pattern Recognit. 2021, 110, 107332. [Google Scholar] [CrossRef]
- Hirano, H.; Minagi, A.; Takemoto, K. Universal adversarial attacks on deep neural networks for medical image classification. BMC Med. Imaging 2021, 21, 9. [Google Scholar] [CrossRef]
- Moosavi-Dezfooli, S.-M.; Fawzi, A.; Fawzi, O.; Frossard, P. Universal Adversarial Perturbations. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; IEEE Computer Society: Washington, DC, USA, 2017; pp. 86–94. [Google Scholar] [CrossRef]
- Dai, Y.; Qian, Y.; Lu, F.; Wang, B.; Gu, Z.; Wang, W.; Wan, J.; Zhang, Y. Improving adversarial robustness of medical imaging systems via adding global attention noise. Comput. Biol. Med. 2023, 164, 107251. [Google Scholar] [CrossRef]
- Sheikh, B.U.H.; Zafar, A. Removing Adversarial Noise in X-ray Images via Total Variation Minimization and Patch-Based Regularization for Robust Deep Learning-based Diagnosis. J. Imaging Inform. Med. 2024. ahead of print. [Google Scholar] [CrossRef] [PubMed]




| Electronic Research Database | Search Results (Number of Items) |
|---|---|
| IEEE Xplore | 304 |
| ScienceDirect | 160 |
| SpringerLink | 240 |
| ACM Digital Library | 85 |
| Dataset | Link | Studies Using the Dataset | Features | ||
|---|---|---|---|---|---|
| No. of Images | No. of Classes | Classes | |||
| Kermany’s Dataset [1] | https://data.mendeley.com/datasets/rscbjbr9sj/3 (accessed on 2 February 2024) | [128,129,130,131,132,133,134,135,136,137,138] | 5858 | 3 | Viral pneumonia, bacterial pneumonia, normal lungs |
| RSNA pneumonia dataset [139] | https://www.kaggle.com/c/rsna-pneumonia-detection-challenge (accessed on 3 April 2024) | [140,141,142,143,144,145,146] | 26,684 | 2 | Pneumonia and non-pneumonia |
| NIH Chest X-ray Dataset [147] | https://www.kaggle.com/datasets/nih-chest-xrays/data (accessed on 24 March 2024) | [70,148,149,150,151,152,153,154,155,156] | 112,000 | 15 | Atelectasis, consolidation, infiltration, pneumothorax, edema, emphysema, fibrosis, effusion, pneumonia, pleural thickening, cardiomegaly, nodule mass, hernia, no findings |
| Cohen et al.’s COVID chest X-ray dataset [157,158,159] | https://github.com/ieee8023/covid-chestxray-dataset (accessed on 22 March 2024) | [160,161,162,163] | 1314 | 05 | COVID-19 or other viral and bacterial pneumonias (MERS, SARS, and ARDS) |
| Novel COVID-19 Chestxray Repository [164,165] | https://www.kaggle.com/datasets/subhankarsen/novel-covid19-chestxray-repository (accessed on 14 March 2024) | [165] | 3975 | 3 | COVID-19, pneumonia and normal |
| COVID-19 chest X-ray [166] | https://www.kaggle.com/datasets/ahmedtronic/covid-19-chest-x-ray (accessed on 3 April 2024) | [167] | 930 | 3 | COVID-19, pneumonia and normal |
| Sait et al.’s curated CXR dataset [168] | https://data.mendeley.com/datasets/9xkhgts2s6/4 (accessed on 4 April 2024) | [169,170,171] | 9208 | 4 | COVID-19, normal, viral pneumonia and bacterial pneumonia. |
| Kumar’s COVID-19-Pneumonia-Normal CXR Images dataset [172] | https://data.mendeley.com/datasets/dvntn9yhd2/1 (accessed on 4 April 2024) | [173,174,175,176] | 5228 | 3 | COVID-19, pneumonia and normal |
| Asraf and Islam’s COVID-19, Pneumonia and Normal Chest X-ray PA Dataset [177] | https://data.mendeley.com/datasets/jctsfj2sfn/1 (accessed on 3 April 2024) | [178] | 4575 | 3 | COVID-19, pneumonia and normal |
| COVID-19 Radiography Database [179] | https://www.kaggle.com/datasets/tawsifurrahman/covid19-radiography-database (accessed on 14 March 2024) | [67,160,180,181,182,183] | 21,165 | 4 | COVID-19, normal, lung opacity (non-COVID lung infection) and viral pneumonia |
| Pneumonia Type | Frequency (Number of Papers) |
|---|---|
| Non-COVID Pneumonia | 22 |
| COVID Pneumonia | 48 |
| Both | 70 |
| Binary Classification | Multiclass Classification |
|---|---|
| “COVID-19 pneumonia” vs. “non-COVID-19 interstitial pneumonia” [8] | “COVID-19 infected pneumonia” vs. “community acquired no COVID-19 infected pneumonia” vs. “normal” [100] |
| “COVID” vs. “non-COVID” [100] | “COVID” vs. “no findings” vs. “pneumonia” [80] |
| “COVID” vs. “normal” [79] | “COVID” vs. “normal” vs. “bacterial” vs. “viral” [71,81] |
| “COVID” vs. “no findings” [80] | “COVID-19” vs. “normal” vs. “viral pneumonia” [91] |
| “pneumonia” vs. “normal” [83] | “COVID” vs. “normal” vs. “pneumonia” [78] |
| “bacterial” vs. “viral” [184] | “COVID-19” vs. “pneumonia” vs. “pneumothorax” vs. “tuberculosis” vs. “normal” [47] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siddiqi, R.; Javaid, S. Deep Learning for Pneumonia Detection in Chest X-ray Images: A Comprehensive Survey. J. Imaging 2024, 10, 176. https://doi.org/10.3390/jimaging10080176
Siddiqi R, Javaid S. Deep Learning for Pneumonia Detection in Chest X-ray Images: A Comprehensive Survey. Journal of Imaging. 2024; 10(8):176. https://doi.org/10.3390/jimaging10080176
Chicago/Turabian StyleSiddiqi, Raheel, and Sameena Javaid. 2024. "Deep Learning for Pneumonia Detection in Chest X-ray Images: A Comprehensive Survey" Journal of Imaging 10, no. 8: 176. https://doi.org/10.3390/jimaging10080176
APA StyleSiddiqi, R., & Javaid, S. (2024). Deep Learning for Pneumonia Detection in Chest X-ray Images: A Comprehensive Survey. Journal of Imaging, 10(8), 176. https://doi.org/10.3390/jimaging10080176