
Healthcare Waste Management in Nigeria: A Review

Abstract
1. Introduction
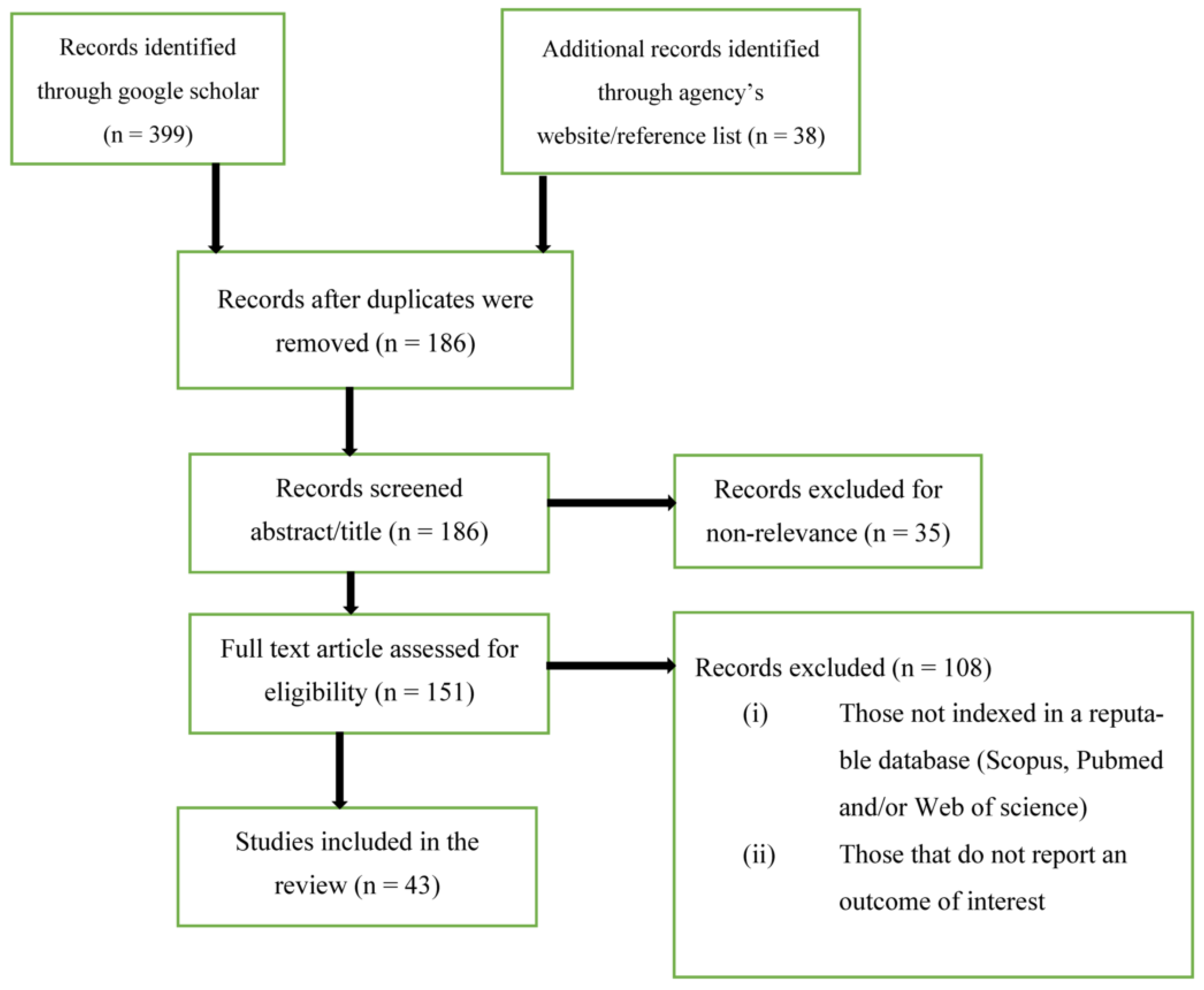
2. Materials and Methods
- (i)
- What are the motivations for rising global concern on healthcare waste management?
- (ii)
- What are the composition/characteristics of healthcare waste generated in Nigeria?
- (iii)
- What is the status of healthcare waste management practices in Nigeria in terms of collection, storage, segregation/sorting, transportation, treatment, and disposal?
- (iv)
- What are the healthcare waste management policy landscapes, financing mechanisms, and institutional arrangements in Nigeria?
- (v)
- What are the prospects and challenges for the implementation of sustainable measures in healthcare waste management in Nigeria?
3. Results
Motivations for Rising Global Concern over Healthcare Waste Management
4. Characterization/Composition of Healthcare Waste Generated in Nigeria
5. Healthcare Waste Management Practices in Nigeria
5.1. Waste Generation
5.2. Waste Segregation
5.3. Training and Awareness
5.4. Collection and Storage
5.5. Waste Transportation
5.6. Disposal and Treatment
6. Policy Landscapes, Financing Mechanisms, and Institutional Arrangement
7. Prospects and Challenges for Healthcare Waste Management in Nigeria
- Inadequate financing: Managing solid waste in cities across the world is a great challenge because of the economic resources required for both capital and recurrent expenditure [10]. Capital expenditures are incurred when procuring waste management facilities such as incinerators, waste vehicles, autoclaves, construction of landfills, etc. Recurrent expenditures are in the form of the cost of maintaining equipment, the cost of energy for powering the equipment, the cost of training, wages, and working tools for waste workers, etc. The ability of a nation to tackle its waste management issues is, therefore largely dependent on the availability of economic funds. Adequate provision of materials and resources for healthcare waste management will ensure proper collection, segregation, treatment, and disposal and will also minimize the incidence of nosocomial infection [46]. There is no budget allocation by hospitals and the government specifically devoted to healthcare waste management in Nigeria. Rather, budgets are allocated for general municipal solid waste management that involves only solid waste collection and disposal without consideration for other components of waste management such as training, segregation, waste characterization, etc. Hospitals across the country usually pay only monthly fees to the waste management authorities/agencies for the collection of the municipal solid waste component of their waste. The hazardous component of healthcare waste is not the responsibility of the agency to handle (except for Lagos state). This is because they are not properly equipped to handle hazardous waste. Because of this, healthcare facilities handle this waste by either burning or burying it. Only a few hospitals have incinerators. Incineration is the most widely used technology for hospital waste disposal in developing countries [60]. Disposal of hospital waste through incineration has its advantages such as occupying limited land space, over 90% of the waste can be diminished, and generated heat can be channeled to useful purposes such as burning of boilers and energy generation [71]. However, when not properly operated, waste incinerators can be a major source of air pollution [71]. The harmful emissions from incineration, which include dioxins and heavy metals, can remain in the air for a long time constituting environmental and public health risks [60].
- Training, sensitization, and awareness: Implementation of proper training and awareness has several positive impacts on the optimal management outcome of healthcare waste [5]. The foregoing review indicated that the level of training and awareness on healthcare waste management in the country is still poor. Partly affecting this poor training outcome is the absence and/or poor availability of funds. In many healthcare facilities where training and awareness programs exist, it happens once without a subsequent program for continuous retraining of the staff. There is also an indication that the quality of the training in some instances is below standard. Another area where training is effective is in healthcare waste minimization. It means adopting processes and practices that will prevent waste before it is generated. It will help in increasing the amount of clean waste stream, which will eventually reduce the cost of disposal and the adverse impact on the environment. One way to achieve waste minimization in healthcare facilities is by training the hospital management on the source reduction measures such as the adoption of a supply method that is less wasteful and prone to produce less hazardous material [72].
- Effective Legislature: There is an inadequate legislative framework for healthcare waste management in Nigeria. Apart, from Lagos state, which issues and enforces guidelines on the proper management of healthcare waste. No other state in Nigeria has implemented a law on healthcare waste management. Even with the recent guideline on healthcare waste delivery issued by NESREA, there is a need for appropriate laws to be made for effective implementation and enforcement. The absence of this law has led to indiscriminate disposal of medical waste by healthcare facilities across the country since there are no attached sanctions for noncompliance. Healthcare legislature should also enforce the provisioning of adequate working tools and an enabling work environment for the waste workers. It was reported in Malaysia that even after the provision of a healthcare waste management policy and training to the staff, poor waste segregation continued in the healthcare facilities because of the absence of tools required for the segregation [73]. Effective healthcare waste management law should also enforce the creation of waste management teams/committees within healthcare facilities. This will ensure that healthcare waste-related issues receive quick and adequate attention. The absence of policy and poor policy regimes contributes to the fact that there is no waste management committee available in health facilities in the country [44].
- Data Collection: Accurate mining of data is essential in waste management planning and execution. Data on waste management in Africa, such as collection and generation, are relatively scant [74,75]. There is no documented data on healthcare waste management in Nigeria at the national, state, and local government levels. The non-documentation of healthcare waste management data is because of the absence of effective and operational guidelines. Effective healthcare waste management data collection will include quantitative and qualitative information on waste management, such as waste collection rate, waste generation rate, waste composition, waste characterization, level of training and awareness, waste management staff strength, quantities of healthcare waste incinerated, quantity landfilled, the quantity of recyclables collected, etc. Proper training on healthcare waste workers, adequate funding, and the creation of waste management committees within health facilities are factors that could promote adequate and prompt waste data collection and documentation across the country.
- Efficient waste treatment techniques: High capital, maintenance, and operational costs are one of the major factors that impede the acquisition and use of novel waste treatment technologies in developing countries such as incinerators, and biochemical waste conversion equipment [76]. However, there are reasonable ranges of technologies for the treatment of medical waste that may be appropriate for use in low and middle-income countries. A typical example is a cost-effective mechanical–biological treatment technology suggested by [77] for the pre-treatment of waste before disposal or landfilling. This technology was specifically designed for low- and middle-income countries. It stabilizes organic waste and ensures the production of waste-derived fuels as it converts waste to energy in the form of fuel [10]. It promotes the concept of circular economy, by simultaneously ensuring energy production, solid waste management, as well as other socioeconomic and environmental health advantages, such as reduction of landfill gas emission, leachates pollution, and unpleasant odor. With the appropriate collaboration between hospitals and indigenous research institutes in Nigeria, these technologies can be locally produced to make them cost-effective. To achieve this, there should be a collaborative assessment of the contextual problems and the devising of a management strategy that would be suitable to their economic circumstance and also sustainable for use based on local contextual conditions.
8. Recommendations and Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Safe Management of Health Care Wastes from Health-Care Activities, 2nd ed.; WHO: Geneva, Switzerland, 2014.
- World Health Organization. Health Care Waste-Fact Sheet; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/news-room/fact-sheets/detail/health-care-waste (accessed on 23 December 2020).
- Chisholm, J.M.; Zamani, R.; Negm, A.M.; Said, N.; Abdeldaiem, M.M.; Dibaj, M.; Akrami, M. Sustainable waste management of medical waste in African developing countries: A narrative review. Waste Manag. Res. 2021, 39, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Zafar, S. Waste-to-Energy. In Medical Waste Management in Developing Countries; Thiel, S., Thomé-Kozmiensky, E., Winter, F., Juchelková, D., Eds.; Waste Management: Houston, TX, USA, 2019; p. 9. [Google Scholar]
- Awodele, O.; Adewoye, A.A.; Oparah, A.C. Assessment of medical waste management in seven hospitals in Lagos, Nigeria. BMC Public Health 2016, 16, 269. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Wang, W.; Chaudhry, N.; Geng, Y. Hospital waste management in developing countries: A mini review. Waste Manag. Res. 2017, 35, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Adusei-Gyamfi, J.; Boateng, K.S.; Sulemana, A.; Hogarh, J.N. Post COVID-19 recovery: Challenges and opportunities for solid waste management in Africa. Environ. Chall. 2022, 6, 100442. [Google Scholar] [CrossRef]
- Health Professions Council of South Africa. Guidelines for the Management of Healthcare Waste, 2008. Available online: http://www.hpcsa.co.za/Uploads/editor/UserFiles/downloads/conduct_ethics/rules/generic_ethical_rules/booklet_16_booklet_on_the_health_care_waste_management.pdf (accessed on 1 October 2022).
- Oyekale, A.S.; Oyekale, T.O. Healthcare waste management practices and safety indicators in Nigeria. BMC Public Health 2017, 17, 740. [Google Scholar] [CrossRef] [PubMed]
- Ezeudu, O.B.; Agunwamba, J.C.; Ugochukwu, U.C.; Ezeudu, T.S. Temporal assessment of municipal solid waste management in Nigeria: Prospects for circular economy adoption. Rev. Environ. Health 2020, 36, 327–344. [Google Scholar] [CrossRef] [PubMed]
- Ezeudu, O.B. Urban sanitation in Nigeria: The past, current and future status of access, policies and institutions. Rev. Environ. Health 2019, 35, 123–137. [Google Scholar] [CrossRef]
- Chima, G.N.; Ezekwe, I.C.; Digha, N.O. An assessment of medical waste management in health institutions in Yenogoa, South-South Nigeria. World Rev. Sci. Technol. Sustain. Dev. 2011, 8, 224–233. [Google Scholar] [CrossRef]
- Ananth, A.P.; Prashanthini, V.; Visvanathan, C. Healthcare Waste Management in Asia. Waste Manag. 2010, 30, 154–161. [Google Scholar] [CrossRef]
- Ferronato, N.; Ragazzi, M.; Elias, M.S.; Portillo, M.A.; Lizarazu, E.G.; Torreta, V. Application of healthcare waste indicators for assessing infectious waste management in Bolivia. Waste Manag. Res. 2019, 38, 1–15. [Google Scholar] [CrossRef]
- Sefouhi, L.; Kalla, M.; Bahmed, L.; Aouragh, L. The risk assessment for the healthcare waste in the hospital of Batna city, Algeria. Int. J. Environ. Sci. Dev. 2013, 4, 442–445. [Google Scholar] [CrossRef]
- De Titto, E.; Savino, A.; Townend, W.K. Healthcare waste management: The current issues in developing countries. Waste Manag. Res. 2012, 30, 559–561. [Google Scholar] [CrossRef] [PubMed]
- Townend, B.; Vallini, G. Healthcare waste management: The global paradox. Waste Manag. Res. 2008, 26, 215–216. [Google Scholar] [CrossRef] [PubMed]
- Harhay, M.O.; Halpern, S.D.; Harhay, J.S.; Olliaro, P.L. Health care waste management: A neglected and growing public health problem worldwide. Trop. Med. Int. Health 2009, 14, 1414–1417. [Google Scholar] [CrossRef] [PubMed]
- Solberg, K.E. Trade in medical waste causes deaths in India. Lancet 2009, 373, 1067. [Google Scholar] [CrossRef]
- Reliefweb. Afghanistan: Medical Waste Poses Health Risk in Urban Areas. 14 October 2008. Available online: https://reliefweb.int/report/afghanistan/afghanistan-medical-waste-poses-health-risk-urban-areas (accessed on 18 November 2022).
- Coker, A.O.; Sikiru, K.A.; Sridhar, M.K.C.; Sangodoyin, A.Y. Characterization and management of solid hospital wastes. In Proceedings of the 25th WEDC Conference: Integrated Development for Water Supply and Sanitation, Addis Ababa, Ethiopia, 1 January 1999. [Google Scholar]
- Odewumi, S.G.; Onyemkpa, C.S. Characterization and Management of solid hospital waste—Comparative analysis of private and public institutions. Eur. J. Sci. Res. 2013, 104, 30–52. [Google Scholar]
- Ugwu, E.I.; Ekeleme, A.C.; Okolie, S.T.A.; Ibe, O.P.; Chieke, C.F.; Ibearugbulem, H.O.; Omeje, M.; Ede, A.N.; Awoyera, P.O.; Ugwu, E.C. Characterization of medical wastes from selected hospitals in Umuahia, Nigeria. J. Phys. Conf. Ser. 2019, 1378, 042058. [Google Scholar] [CrossRef]
- Afolabi, A.S.; Agbabiaka, H.I.; Afon, A.O.; Akinbinu, A.A.; Adefisoye, E.A. Solid waste management practice in Obafemi Awolowo University Teaching Hospital Complex (OAUTHC), Ile-Ife Nigeria. Manag. Environ. Qual. Int. J. 2017, 29, 547–571. [Google Scholar] [CrossRef]
- Sawyerr, H.O.; Adeolu, A.T.; Salami, O.O.; Adejoh, P.O. Evaluation of biomedical waste in Kogi State University Teaching Hospital, Anyigba, Kogi state Nigeria. Toxicol. Environ. Health Sci. 2017, 9, 29–34. [Google Scholar] [CrossRef]
- Bassey, B.E.; Ben-Coker, M.O.; Aliyu, H.S.A. Characterization and Management of solid medical wastes in Federal Capital Territory, Abuja Nigeria. Afr. Health Sci. 2006, 6, 59–63. [Google Scholar]
- Ali, M.; Wang, W.; Chaudhry, N. Management of wastes from hospitals: A case study in Pakistan. Waste Manag. Res. 2015, 34, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Idowu, I.; Alo, B.; Atherton, W.; Al khaddar, R. Profile of medical waste management in two healthcare facilities in Lagos, Nigeria: A case study. Waste Manag. Res. 2013, 31, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Alves, S.B.; e Souza, A.C.S.; Tipple, A.F.V.; Rezende, K.C.A.D.; de Resende, F.R.; Rodrigues, E.G.; Pereira, M.S. The reality of waste management in primary health care units in Brazil. Waste Manag. Res. 2014, 32, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Mugambe, R.K.; Ssempebwa, J.C.; Tumwesigye, N.M.; van Vliet, B.; Adedimeji, A. Healthcare waste management in Uganda: Management and generation rates in public and private hospitals in Kampala. J. Public Health 2011, 20, 245–251. [Google Scholar] [CrossRef]
- Tadesse, M.L.; Kummie, A. Healthcare waste generation and management practices in government health centers of Addis Ababa, Ethiopia. BMC Public Health 2014, 14, 1221. [Google Scholar] [CrossRef]
- Abah, S.O.; Ohimain, E.I. Healthcare waste management in Nigeria: A case study. J. Public Health Epidemiol. 2011, 3, 99–110. [Google Scholar]
- Ojuolape, O.T.; Afon, A.O. Solid waste characterization in private health institutions: Empirical evidence from Ibadan metropolis. Manag. Res. Pract. 2016, 8, 50–60. [Google Scholar]
- Coker, A.O.; Sangodoyin, A.; Sridhar, M.; Booth, C.; Olomolaiye, P.; Hammond, F. Medical waste management in Ibadan, Nigeria: Obstacles and Prospects. Waste Manag. 2009, 29, 804–811. [Google Scholar] [CrossRef]
- Longe, E.O.; Williams, A. A preliminary study of medical waste management in Lagos metropolis, Nigeria. Iran. J. Environ. Health Sci. Eng. 2006, 3, 133–139. [Google Scholar]
- Umegbolu, E.I.; Ozoejike, I.N. Management of solid healthcare wastes in some government healthcare facilities in Enugu State, Southeast Nigeria: A cross-sectional study. Int. J. Community Med. Public Health 2017, 4, 4031–4041. [Google Scholar] [CrossRef]
- Oke, I.A.; Otun, J.A.; Adie, D.B.; Asani, M.A.; Lukman, S.; Ismail, A. Characterization and management of medical solid wastes from selected private hospitals in Ile-Ife, Nigeria. In Solid Waste Management and Environmental Remediation; Faerber, T., Herzog, J., Eds.; Nova science publishers: Hauppauge, NY, USA, 2009; Chapter 7; p. 38. [Google Scholar]
- Etim, M.A.; Academe, S.; Emenike, P.; Omole, D. Applications of multi-criteria decision approach in the assessment of medical waste management systems in Nigeria. Sustainability 2021, 13, 10914. [Google Scholar] [CrossRef]
- Oli, A.N.; Ekejindu, C.C.; Adje, D.U.; Ezeobi, I.; Ejiofor, O.S.; Ibeh, C.C.; Ubajaka, C.F. Healthcare waste management in selected government and private hospitals in Southeast Nigeria. Asian Pac. J. Trop. Biomed. 2015, 6, 84–89. [Google Scholar] [CrossRef]
- Marinkovic, N.; Vitale, K.; Holcer, N.J.; Dzakular, A.; Pavic, T. Management of Hazardous medical waste in Croatia. Waste Manag. 2008, 28, 1049–1056. [Google Scholar] [CrossRef]
- Gupta, S.; Boojh, R. Report: Biomedical Waste Management practices at Balrampur Hospital, Lucknow, India. Waste Manag. Res. 2006, 24, 584–591. [Google Scholar] [CrossRef] [PubMed]
- ICRC—International Committee of the Red Cross. Medical Waste Management. 2011. Available online: https://www.icrc.org/en/doc/assets/files/publications/icrc-002-4032.pdf (accessed on 20 September 2022).
- Adedigba, M.A.; Nwhator, S.O.; Afon, A.; Abegunde, A.A.; Bamise, C.T. Assessment of dental waste management in a Nigerian tertiary hospital. Waste Manag. Res. 2010, 28, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Ezirim, I.; Agbo, F. Role of national policy in improving healthcare waste management in Nigeria. J. Health Pollut. 2018, 8, 180913. [Google Scholar] [CrossRef]
- Nwankwo, C. Knowledge and practice of waste management among hospital cleaners. Occup. Med. 2018, 68, 360–363. [Google Scholar] [CrossRef]
- Macaulay, B.M.; Odiase, F.M. Medical waste management practices in developing countries; A case study of health facilities in Akure, Nigeria. Int. J. Environ. Waste Manag. 2016, 17, 103–127. [Google Scholar] [CrossRef]
- Uwa, C.U. Assessment of healthcare waste management practices in Enugu Metropolis, Nigeria. Int. J. Environ. Sci. Dev. 2014, 5, 370–374. [Google Scholar] [CrossRef]
- Denloye, A.A.; Ojuromi, O.T.; Ochei, K.; Ade-Serrano, E.A. Biosafety knowledge, waste disposal practices and identification of parasites in biomedical waste from healthcare establishments in Lagos and Abuja Nigeria. Anim. Res. Int. 2019, 16, 3144–3150. [Google Scholar]
- Bazrafshan, E.; Mostafapoor, F.K. Survey of medical waste characterization and management in Iran: A case study of Sistan and Bauchestan Province. Waste Manag. Res. 2011, 29, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Al-Emad, A.A. Assessment of medical waste management in the main hospitals in Yemen. East. Mediterr. Health J. 2011, 17, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Ezeoke, E.U.; Omotowo, I.B.; Ndu, A. Investigating knowledge, attitude and healthcare waste management by health workers in Nigerian tertiary health institutions. Glob. J. Health Sci. 2017, 9, 222–232. [Google Scholar]
- Onoh, R.C.; Adeke, A.S.; Umeokonkwo, C.D.; Ekwedigwe, K.C.; Agboeze, J.; Ogah, E.O. Knowledge and practices of healthcare waste management among health workers in Lassa Fever treatment facility in Southeast Nigeria. Niger. Med. J. 2019, 60, 257–261. [Google Scholar] [CrossRef]
- Okechukwu, E.; Onyenwenyi, A. P170: Evaluation of knowledge and practices of hospital waste management in Nigeria: Implications for the control of healthcare associated infections. Antimicrob. Resist. Infect. Control 2013, 2, P170. [Google Scholar] [CrossRef]
- Oke, A.O. Management of immunization solid wastes in Kano state. Waste Manag. 2008, 28, 2512–2521. [Google Scholar] [CrossRef]
- Anozie, O.B.; Lawani, L.O.; Eze, J.N.; Mamah, E.J.; Onoh, R.C.; Ogah, E.O.; Umezurike, D.A.; Anozie, R.O. Knowledge, attitude and practice of healthcare managers to medical waste management and occupational safety practices: Findings from southeast, Nigeria. J. Clin. Diagn. Res. 2017, 11, 1C01–1C04. [Google Scholar] [CrossRef]
- WHO. Safe Management of Waste from Healthcare Activities: A Summary; World Health Organization: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/bitstream/handle/10665/259491/WHO-FWC-WSH-17.05-eng.pdf (accessed on 22 September 2022).
- Pruss, A.; Townend, W.K. Management of Waste from Healthcare Activities; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Baaki, T.K.; Baharum, M.R.; Akashah, F.W. Critical success factors of medical waste management in healthcare facilities in Nigeria: A case study. J. Des. Built Environ. 2017, 17, 18–35. [Google Scholar] [CrossRef]
- Oketola, A.A.; Ogundiran, M.B.; Adefolu, O.R.; Mojeed, O.A.; Itiveh, S.E. Medical waste management practices in Nigeria; The cases of Lagos and Ibadan. In Proceedings of the The 26th International Conference on Solid Waste Technology and Management, Philadelphia, PA, USA, 27–30 March 2011. [Google Scholar]
- Ansari, M.; Ehrampoush, M.H.; Farzadkia Ahmadi, E. Dynamic assessment of economic and environmental performance index and generation, composition and environmental and human health risks of hospital solid waste in developing countries; a state of the art review. Environ. Int. 2019, 132, 105073. [Google Scholar] [CrossRef]
- LAWMA. Lagos. Statistics of Healthcare Facilities in Lagos State Accreditated by LAWMA, 2020. Available online: https://www.lawma.gov.ng/ (accessed on 27 December 2020).
- Iweh, M.; Ogbonna, B.; Nduka, S.; Anetoh, M.; Okonta, M. Assessment of disposal practices of expired and unused medications among community pharmacies in Anambra state, southeast Nigeria: A mixed study design. J. Pharm. Policy Pract. 2019, 12, 12. [Google Scholar]
- Ola, C.S. Town and Country Planning and Environmental Laws in Nigeria; University Press Ibadan: Ibadan, Nigeria, 1984; p. 275. [Google Scholar]
- Chokor, B.A. Government policy and environmental protection in the developing world: The example of Nigeria. Environ. Manag. 1993, 17, 15–30. [Google Scholar] [CrossRef]
- FEPA. Guideline for the Management of Solid Hazardous Waste in Guideline and Standards in Environmental Pollution Control in Nigeria; FEPA: Lagos, Nigeria, 1991. [Google Scholar]
- NESREA. National Environmental (Sanitation and Waste Control) Regulation. 2009. Available online: https://www.nesrea.gov.ng/wp-content/uploads/2020/02/Sanitation_and_Wastes_Control_Regulations%202009.pdf (accessed on 2 October 2022).
- Federal Republic of Nigeria Official Gazette. National Environmental (Healthcare Waste Control), Regulations, 2021. Available online: https://gazettes.africa/archive/ng/2021/ng-government-gazette-supplement-dated-2021-04-30-no-70.pdf (accessed on 19 October 2022).
- The National Healthcare Waste Management Plan. 2006. Available online: https://documents1.worldbank.org/curated/ar/164291468110649200/E16340NHCWMP10Sophie0version0170April.doc (accessed on 19 October 2022).
- National Healthcare Waste Management Policy. FGN, National Healthcare Waste Policy. 2013. Available online: https://www.technet-21.org/media/com_resources/trl/6133/multi_upload/NationalHealthcareWasteManagementPolicy(2013).pdf (accessed on 9 October 2022).
- Uzochukwu, B.; Ughasoro, M.D.; Etiaba, E.; Okwuosa, C.; Anvuladu, E.; Onwujekwe, O.E. Healthcare financing in Nigeria: Implications for achieving universal health coverages. Nigeria. J. Clin. Pract. 2015, 18, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Makarichi, L.; Jutidamrongphan, W.; Techato, K. The evolution of waste-to-energy incineration: A review. Renew. Sust. Energy Rev. 2018, 91, 812–821. [Google Scholar] [CrossRef]
- Maroufi, M.; Javadi, M.; Yaghoubi, M.; Karimi, S. Function of nurses and other staff to minimize hospital waste in selected hospitals in Isfahan. Iran. J. Nurs. Midwifery Res. 2012, 17, 445–450. [Google Scholar]
- Hamadan, N.; Sapri, M.; Mohammed, A.H.; Awang, M.; Rahman, M.S.A.; Rosli, N.W.; Lah, N.M. The implementation of clinical waste handling in hospital Sultanah Aminah Johor Bahru (HSAJB). Procedia-Soc. Behav. Sci. 2012, 65, 802–807. [Google Scholar] [CrossRef]
- UNEP. Municipal Solid Waste: Is It Garbage or Gold? UNEP Global Environmental Alert Series. 2013. Available online: http://www.unep.org/pdf/UNEP_GEAS_oct_2013.pdf (accessed on 16 October 2022).
- UN-Habitat. Collection of Municipal Solid Waste in Developing Countries; United Nations Human Settlements Programme (UN-Habitat): Nairobi, Kenya, 2010. [Google Scholar]
- Scarlet, N.; Motola, V.; Dallemend, J.F.; Monforti- Ferrario, F.; Mofor, L. Evaluation of energy potential of municipal solid waste from African urban areas. Renew. Sust. Energy Rev. 2015, 50, 1269–1286. [Google Scholar] [CrossRef]
- Munnich, K.; Mahler, C.F.; Fricke, K. Pilot project of mechanical-biological treatment of waste in Brazil. Waste Manag. 2006, 26, 150–157. [Google Scholar] [CrossRef]
- Oteri, J.; Bawa, S.; Christopher, E.; Nsubuga, P.; Dieng, B.; Braka, F.; Shuaib, F. Potential for improving routine immunization waste management using measles vaccination campaign 2017 in Kebbi State, Nigeria. Vaccine 2021, 39, C60–C65. [Google Scholar] [CrossRef]


{kind=link}
| City | Type/Size of Facilities | The Number of Facilities Studied | Waste Generation Rate | References | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tertiary | Secondary | Primary | Private | Public | kg/bed/day | kg/Person/Day | kg/Head/Day | kg/Ward/Day | |||
| Lagos | 1 | 1 | 2 | 0.01–3.98 | - | [28] | |||||
| Edo | 1 | 1 | 0.81 | 0.62 | [32] | ||||||
| Lagos | 5 | 2 | 7 | 0.181 | [5] | ||||||
| Lagos | 2 | 2 | 4 | 0.573 | [35] | ||||||
| Enugu State | 5 | 5 | 10 | 0.16 | [36] | ||||||
| Ibadan | - | 52 | 0.15 | [34] | |||||||
| Ibadan | 6 | 6 | 0.01 | [33] | |||||||
| Umuahia | 10 | 31.53–59.81 | [23] | ||||||||
| Ile-Ife | 2 | 4 | 4 | 10 | 1.49 | [37] | |||||
| Yenagoa | - | - | 2.78 | [12] | |||||||
| Abuja | 1 | 4 | 5 | 2.78 | [26] | ||||||
| Disposal Method | Locations of Practice | Description | References |
|---|---|---|---|
| Incineration | Across the country | Few (About 2.06%) hospitals have incinerators | [9] |
| Open Dumping/Burning and Burying | Across the country/Rampant in the northern part of the country | Hospitals maintain open dumpsites where medical wastes are dumped, burnt, and/or buried | [21,24,35,37,43] |
| Hydroclave | Lagos State | LAWMA adopts hydroclave for treatment of medical waste before landfilling | [5] |
| Landfill | Lagos State | The medical waste is landfilled after treatment with the hydroclave technology | [5] |
| Dumping with Municipal Solid Waste (MSW) | Abuja | Medical waste is disposed of at the municipal solid waste dumpsites without segregation or pre-treatment | [26] |
| NAFDAC | Across the country | NAFDAC participates in the collection and disposal of expired drug | [62] |
| Scheme. | Law/Decree/Act/Regulation | Year | Area Covered |
|---|---|---|---|
| 1 | Public Health Act/Ordinance | 1917 | Food administration, hygiene in public places, urban sanitation, noise and odor control, waste management, etc. |
| 2 | Public health Service Act | 1958 (Amendment of 1917) | Food administration, hygiene in public places, urban sanitation, noise and odor control, waste management, etc. |
| 3 | Decree No 58 | 1988 | Established FEPA, with the mandate to (i) monitor and enforce environmental protection measures (ii) liaise with other government agencies on environmental protection (iii) establish standards and prosecute offenders |
| 4 | Decree No 42 | 1988 | Harmful Waste Special Criminal provision. It prohibits carrying, depositing, and dumping harmful waste and injurious, poisonous, toxic, and noxious substances. It also prescribes penalties for offenders |
| 5 | Decree No 86 | 1992 | It sets out a procedure and methods for environmental impact assessment (EIA) on both public and private projects. It also stipulates that the construction of incinerators requires EIA |
| 6 | National Effluent Limitation (S.I.8) | 1991 | It establishes effluent discharge limits and makes it mandatory for firms to install anti-pollution infrastructures for the treatment of their effluents |
| 7 | National Pollution Abatement in Industries and facilities generating wastes | 1991 | Established permissible limit for industrial pollution and puts restrictions on the release of pollution to the environment |
| 8 | Management of Solid and Hazardous Waste Regulation | 1991 | Tracking of waste from the point of generation to the point of disposal with specific details (ii) Hazardous waste treatment, disposal, and the required facilities |
| 9. | NESREA ACT | 2007 | Establishes NESREA to implement and enforce environmental quality standards and enforce compliance |
| 10 | National Environmental (Sanitation and Waste Control) Regulation (S.I.28) | 2009 | Environmental waste and sanitation, Control of medical and healthcare waste |
| 11 | National Environmental Health Practice Regulation | 2016 | Prevention and control of incidence of contagious diseases through environmental health interventions. Provides for the creation of a waste management advisory committee |
| 12 | National Radioactive Waste Management Regulations | 2006 | Nuclear safety and radiological protection regulation |
| 13 | National Environmental (Healthcare Waste Control) Regulations | 2021 | Regulation of Healthcare waste management |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ezeudu, O.B.; Ezeudu, T.S.; Ugochukwu, U.C.; Tenebe, I.T.; Ajogu, A.P.; Nwadi, U.V.; Ajaero, C.C. Healthcare Waste Management in Nigeria: A Review. Recycling 2022, 7, 87. https://doi.org/10.3390/recycling7060087
Ezeudu OB, Ezeudu TS, Ugochukwu UC, Tenebe IT, Ajogu AP, Nwadi UV, Ajaero CC. Healthcare Waste Management in Nigeria: A Review. Recycling. 2022; 7(6):87. https://doi.org/10.3390/recycling7060087
Chicago/Turabian StyleEzeudu, Obiora B., Tochukwu S. Ezeudu, Uzochukwu C. Ugochukwu, Imokhai Theophilus Tenebe, Agbaji P. Ajogu, Uchenna V. Nwadi, and Charles C. Ajaero. 2022. "Healthcare Waste Management in Nigeria: A Review" Recycling 7, no. 6: 87. https://doi.org/10.3390/recycling7060087
APA StyleEzeudu, O. B., Ezeudu, T. S., Ugochukwu, U. C., Tenebe, I. T., Ajogu, A. P., Nwadi, U. V., & Ajaero, C. C. (2022). Healthcare Waste Management in Nigeria: A Review. Recycling, 7(6), 87. https://doi.org/10.3390/recycling7060087