miR-625-3p and lncRNA GAS5 in Liquid Biopsies for Predicting the Outcome of Malignant Pleural Mesothelioma Patients Treated with Neo-Adjuvant Chemotherapy and Surgery


 ,
, 
Abstract
:1. Introduction
2. Results
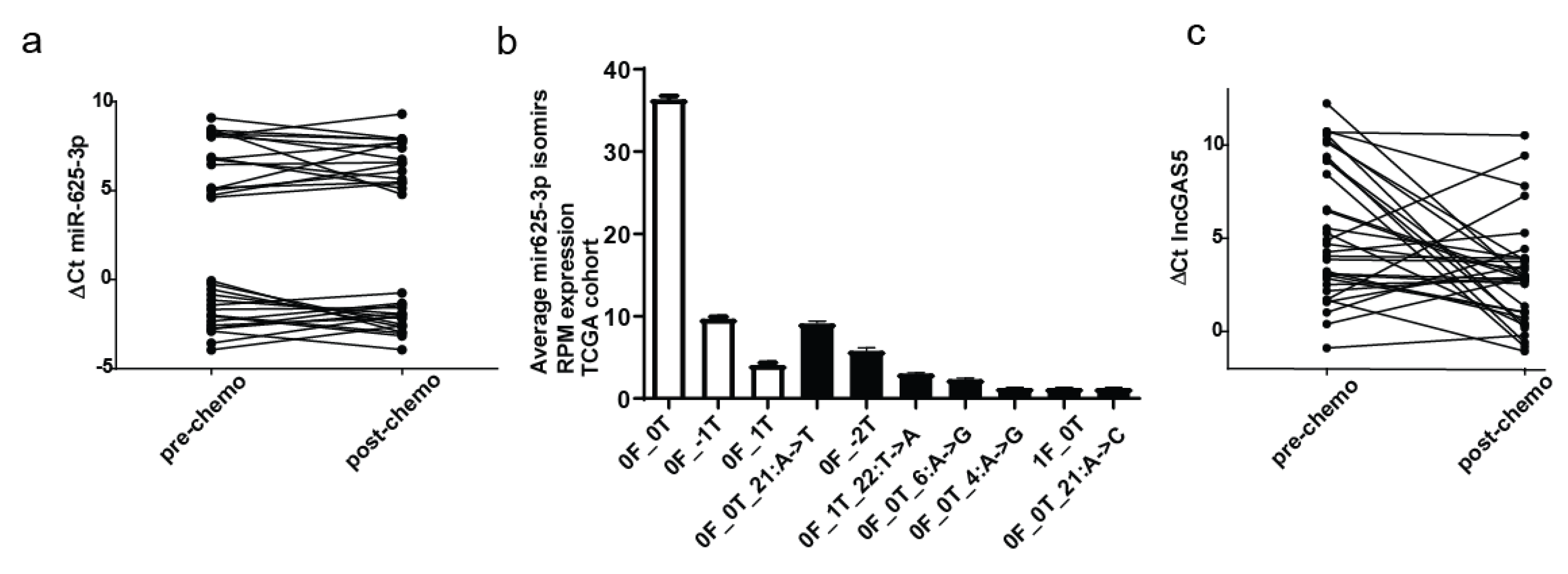
2.1. Plasma Levels of Circulating miR-625-3p and GAS5 in the Cohort of MPM Patients
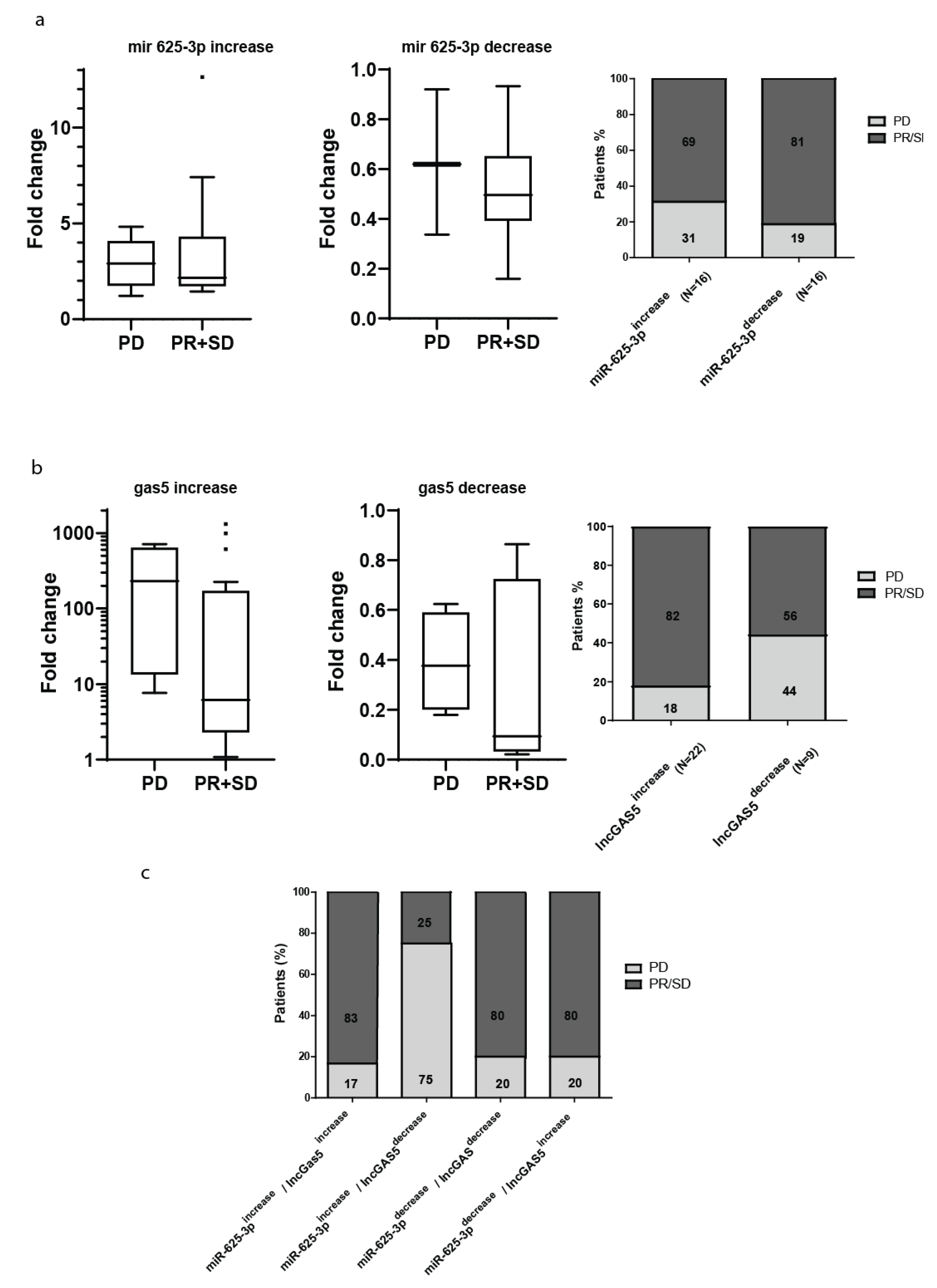
2.2. Post-Chemotherapy Changes in the Plasma Level of miR-625-3p and GAS5 and Response to Treatment
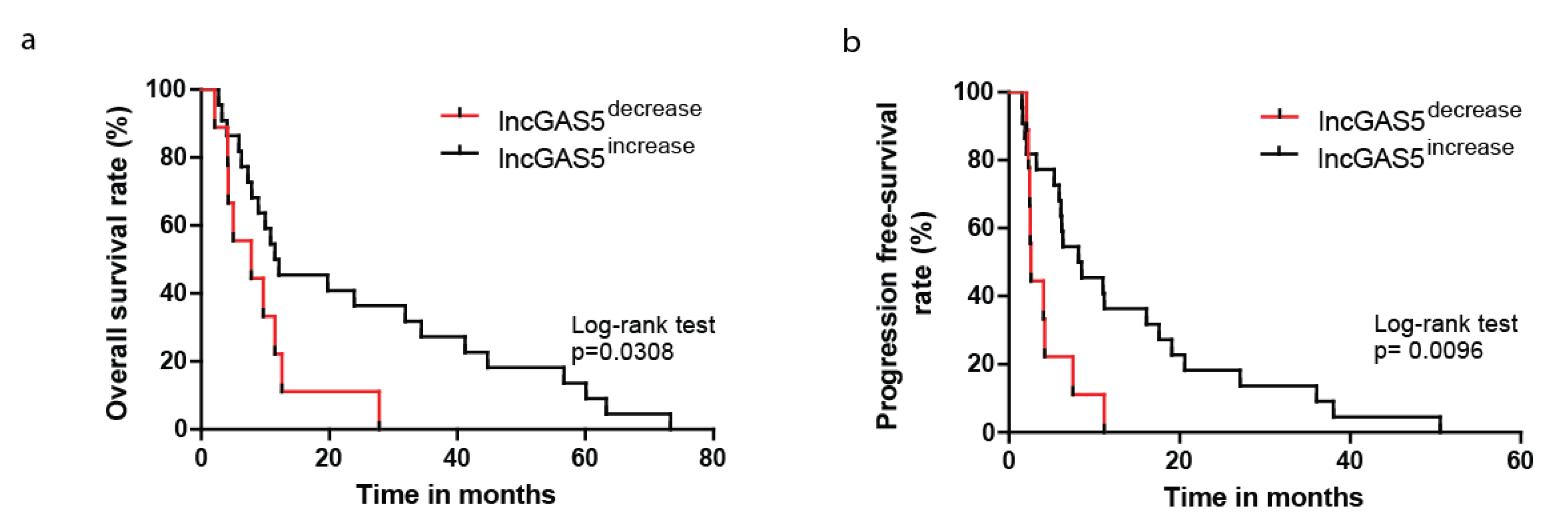
2.3. Decrease in Circulating GAS5 Associates with Shorter Progression-Free and Overall Survival
3. Discussion
4. Materials and Methods
4.1. Blood Collection and Preparation of Plasma
4.2. RNA Extraction from Plasma
4.3. Reverse Transcription of miRNA and qRT-PCR Measurement
4.4. TA Cloning
4.5. miR-625 isomiR Detection in Mesothelioma Samples from TCGA
4.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pasel, G.; Ceresoli, G.L.; Favaretto, A. An overview of neoadjuvant chemotherapy in the multimodality treatment of malignant pleural mesothelioma. Cancer Treat. Rev. 2013, 39, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Weder, W.; Stahel, R.A.; Bernhard, J.; Bodis, S.; Vogt, P.; Ballabeni, P.; Lardinois, D.; Betticher, D.; Schmid, R.; Stupp, R.; et al. Multicenter trial of neo-adjuvant chemotherapy followed by extrapleural pneumonectomy in malignant pleural mesothelioma. Ann. Oncol. 2007, 18, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Krug, L.M.; Pass, H.I.; Rusch, V.W.; Kindler, H.L.; Sugarbaker, D.J.; Rosenzweig, K.E.; Flores, R.; Friedberg, J.S.; Pisters, K.; Monberg, M.; et al. Multicenter phase ii trial of neoadjuvant pemetrexed plus cisplatin followed by extrapleural pneumonectomy and radiation for malignant pleural mesothelioma. J. Clin. Oncol. 2009, 27, 3007–3013. [Google Scholar] [CrossRef] [PubMed]
- Opitz, I.; Friess, M.; Kestenholz, P.; Schneiter, D.; Frauenfelder, T.; Nguyen-Kim, T.D.; Seifert, B.; Hoda, M.A.; Klepetko, W.; Stahel, R.A.; et al. A new prognostic score supporting treatment allocation for multimodality therapy for malignant pleural mesothelioma: A review of 12 years’ experience. J. Thorac. Oncol. 2015, 10, 1634–1641. [Google Scholar] [CrossRef] [PubMed]
- Fennell, D.A.; Parmar, A.; Shamash, J.; Evans, M.T.; Sheaff, M.T.; Sylvester, R.; Dhaliwal, K.; Gower, N.; Steele, J.; Rudd, R. Statistical validation of the eortc prognostic model for malignant pleural mesothelioma based on three consecutive phase ii trials. J. Clin. Oncol. 2005, 23, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Quinn, L.; Finn, S.P.; Cuffe, S.; Gray, S.G. Non-coding rna repertoires in malignant pleural mesothelioma. Lung Cancer 2015, 90, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Pass, H.I.; Goparaju, C.; Ivanov, S.; Donington, J.; Carbone, M.; Hoshen, M.; Cohen, D.; Chajut, A.; Rosenwald, S.; Dan, H.; et al. Hsa-mir-29c* is linked to the prognosis of malignant pleural mesothelioma. Cancer Res. 2010, 70, 1916–1924. [Google Scholar] [CrossRef]
- Moody, H.L.; Lind, M.J.; Maher, S.G. Microrna-31 regulates chemosensitivity in malignant pleural mesothelioma. Mol. Ther. Nucleic Acids 2017, 8, 317–329. [Google Scholar] [CrossRef]
- Kirschner, M.B.; Cheng, Y.Y.; Armstrong, N.J.; Lin, R.C.; Kao, S.C.; Linton, A.; Klebe, S.; McCaughan, B.C.; van Zandwijk, N.; Reid, G. Mir-score: A novel 6-microrna signature that predicts survival outcomes in patients with malignant pleural mesothelioma. Mol. Oncol. 2015, 9, 715–726. [Google Scholar] [CrossRef]
- Busacca, S.; Germano, S.; De Cecco, L.; Rinaldi, M.; Comoglio, F.; Favero, F.; Murer, B.; Mutti, L.; Pierotti, M.; Gaudino, G. Microrna signature of malignant mesothelioma with potential diagnostic and prognostic implications. Am. J. Respir Cell Mol. Biol. 2010, 42, 312–319. [Google Scholar] [CrossRef]
- Weber, J.A.; Baxter, D.H.; Zhang, S.; Huang, D.Y.; Huang, K.H.; Lee, M.J.; Galas, D.J.; Wang, K. The microrna spectrum in 12 body fluids. Clin. Chem. 2010, 56, 1733–1741. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Rivera, V.; Negrete-Garcia, M.C.; Avila-Moreno, F.; Ortiz-Quintero, B. Secreted and tissue mirnas as diagnosis biomarkers of malignant pleural mesothelioma. Int. J. Mol. Sci. 2018, 19, 595. [Google Scholar] [CrossRef] [PubMed]
- Kirschner, M.B.; Cheng, Y.Y.; Badrian, B.; Kao, S.C.; Creaney, J.; Edelman, J.J.; Armstrong, N.J.; Vallely, M.P.; Musk, A.W.; Robinson, B.W.; et al. Increased circulating mir-625-3p: A potential biomarker for patients with malignant pleural mesothelioma. J. Thorac. Oncol. 2012, 7, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Renganathan, A.; Kresoja-Rakic, J.; Echeverry, N.; Ziltener, G.; Vrugt, B.; Opitz, I.; Stahel, R.A.; Felley-Bosco, E. Gas5 long non-coding rna in malignant pleural mesothelioma. Mol. Cancer 2014, 13, 119. [Google Scholar] [CrossRef]
- Rasmussen, M.H.; Jensen, N.F.; Tarpgaard, L.S.; Qvortrup, C.; Romer, M.U.; Stenvang, J.; Hansen, T.P.; Christensen, L.L.; Lindebjerg, J.; Hansen, F.; et al. High expression of microrna-625-3p is associated with poor response to first-line oxaliplatin based treatment of metastatic colorectal cancer. Mol. Oncol. 2013, 7, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, M.H.; Lyskjaer, I.; Jersie-Christensen, R.R.; Tarpgaard, L.S.; Primdal-Bengtson, B.; Nielsen, M.M.; Pedersen, J.S.; Hansen, T.P.; Hansen, F.; Olsen, J.V.; et al. Mir-625-3p regulates oxaliplatin resistance by targeting map2k6-p38 signalling in human colorectal adenocarcinoma cells. Nat. Commun. 2016, 7, 12436. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Kong, D.; Xu, W. Microrna-625-3p promotes the proliferation, migration and invasion of thyroid cancer cells by up-regulating astrocyte elevated gene 1. Biomed. Pharmacother. 2018, 102, 203–211. [Google Scholar] [CrossRef]
- Smith, C.M.; Steitz, J.A. Classification of gas5 as a multi-small-nucleolar-rna (snorna) host gene and a member of the 5’-terminal oligopyrimidine gene family reveals common features of snorna host genes. Mol. Cell Biol. 1998, 18, 6897–6909. [Google Scholar] [CrossRef]
- Schneider, C.; King, R.M.; Philipson, L. Genes specifically expressed at growth arrest of mammalian cells. Cell 1988, 54, 787–793. [Google Scholar] [CrossRef]
- Stahel, R.A.; Riesterer, O.; Xyrafas, A.; Opitz, I.; Beyeler, M.; Ochsenbein, A.; Fruh, M.; Cathomas, R.; Nackaerts, K.; Peters, S.; et al. Neoadjuvant chemotherapy and extrapleural pneumonectomy of malignant pleural mesothelioma with or without hemithoracic radiotherapy (sakk 17/04): A randomised, international, multicentre phase 2 trial. Lancet Oncol. 2015, 16, 1651–1658. [Google Scholar] [CrossRef]
- Kirschner, M.B.; Kao, S.C.; Edelman, J.J.; Armstrong, N.J.; Vallely, M.P.; van Zandwijk, N.; Reid, G. Haemolysis during sample preparation alters microrna content of plasma. PLoS ONE 2011, 6, e24145. [Google Scholar] [CrossRef]
- Blondal, T.; Jensby Nielsen, S.; Baker, A.; Andreasen, D.; Mouritzen, P.; Wrang Teilum, M.; Dahlsveen, I.K. Assessing sample and mirna profile quality in serum and plasma or other biofluids. Methods 2013, 59, S1–S6. [Google Scholar] [CrossRef]
- Neilsen, C.T.; Goodall, G.J.; Bracken, C.P. Isomirs--the overlooked repertoire in the dynamic micrornaome. Trends Genet. 2012, 28, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Martinez, V.D.; Marshall, E.A.; Anderson, C.; Ng, C.S.; Minatel, B.C.; Sage, A.P.; Enfield, K.S.S.; Xu, Z.; Lam, W.L. Discovery of previously undetected micrornas in mesothelioma and their use as tissue-of-origin markers. Am. J. Respir Cell Mol. Biol. 2019, in press. [Google Scholar]
- Hmeljak, J.; Sanchez-Vega, F.; Hoadley, K.A.; Shih, J.; Stewart, C.; Heiman, D.; Tarpey, P.; Danilova, L.; Drill, E.; Gibb, E.A.; et al. Integrative molecular characterization of malignant pleural mesothelioma. Cancer Dis. 2018, 8, 1548–1565. [Google Scholar] [CrossRef] [PubMed]
- Mourtada-Maarabouni, M.; Pickard, M.R.; Hedge, V.L.; Farzaneh, F.; Williams, G.T. Gas5, a non-protein-coding rna, controls apoptosis and is downregulated in breast cancer. Oncogene 2009, 28, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Xie, H.; Zhan, H.; Li, J.; Liu, Y.; Huang, W. Prognostic values of long noncoding rna gas5 in various carcinomas: An updated systematic review and meta-analysis. Front. Physiol. 2017, 8, 814. [Google Scholar] [CrossRef] [PubMed]
- Permuth, J.B.; Chen, D.T.; Yoder, S.J.; Li, J.; Smith, A.T.; Choi, J.W.; Kim, J.; Balagurunathan, Y.; Jiang, K.; Coppola, D.; et al. Linc-ing circulating long non-coding rnas to the diagnosis and malignant prediction of intraductal papillary mucinous neoplasms of the pancreas. Sci. Rep. 2017, 7, 10484. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Hodges, T.R.; Song, R.; Gong, Y.; Calin, G.A.; Heimberger, A.B.; Zhao, H. Serum hotair and gas5 levels as predictors of survival in patients with glioblastoma. Mol. Carcinog. 2018, 57, 137–141. [Google Scholar] [CrossRef]
- Magbanua, M.J.M.; Rugo, H.S.; Wolf, D.M.; Hauranieh, L.; Roy, R.; Pendyala, P.; Sosa, E.V.; Scott, J.H.; Lee, J.S.; Pitcher, B.; et al. Expanded genomic profiling of circulating tumor cells in metastatic breast cancer patients to assess biomarker status and biology over time (calgb 40502 and calgb 40503, alliance). Clin. Cancer Res. 2018, 24, 1486–1499. [Google Scholar] [CrossRef]
- Budczies, J.; Klauschen, F.; Sinn, B.V.; Gyorffy, B.; Schmitt, W.D.; Darb-Esfahani, S.; Denkert, C. Cutoff finder: A comprehensive and straightforward web application enabling rapid biomarker cutoff optimization. PLoS ONE 2012, 7, e51862. [Google Scholar] [CrossRef]
- Ertel, A. Bimodal gene expression and biomarker discovery. Cancer Inform. 2010, 9, 11–14. [Google Scholar] [CrossRef]
- Zuo, Z.; Calin, G.A.; de Paula, H.M.; Medeiros, L.J.; Fernandez, M.H.; Shimizu, M.; Garcia-Manero, G.; Bueso-Ramos, C.E. Circulating micrornas let-7a and mir-16 predict progression-free survival and overall survival in patients with myelodysplastic syndrome. Blood 2011, 118, 413–415. [Google Scholar] [CrossRef]
- Nejad, C.; Pepin, G.; Behlke, M.A.; Gantier, M.P. Modified polyadenylation-based rt-qpcr increases selectivity of amplification of 3′-microrna isoforms. Front. Genet. 2018, 9, 11. [Google Scholar] [CrossRef]
- Loher, P.; Londin, E.R.; Rigoutsos, I. Isomir expression profiles in human lymphoblastoid cell lines exhibit population and gender dependencies. Oncotarget 2014, 5, 8790–8802. [Google Scholar] [CrossRef]
- Telonis, A.G.; Magee, R.; Loher, P.; Chervoneva, I.; Londin, E.; Rigoutsos, I. Knowledge about the presence or absence of mirna isoforms (isomirs) can successfully discriminate amongst 32 tcga cancer types. Nucleic Acids Res. 2017, 45, 2973–2985. [Google Scholar] [CrossRef]
- Telonis, A.G.; Loher, P.; Jing, Y.; Londin, E.; Rigoutsos, I. Beyond the one-locus-one-mirna paradigm: Microrna isoforms enable deeper insights into breast cancer heterogeneity. Nucleic Acids Res. 2015, 43, 9158–9175. [Google Scholar] [CrossRef]
- Umu, S.U.; Langseth, H.; Bucher-Johannessen, C.; Fromm, B.; Keller, A.; Meese, E.; Lauritzen, M.; Leithaug, M.; Lyle, R.; Rounge, T.B. A comprehensive profile of circulating rnas in human serum. RNA Biol. 2018, 15, 242–250. [Google Scholar] [CrossRef]
- Llorens, F.; Banez-Coronel, M.; Pantano, L.; del Rio, J.A.; Ferrer, I.; Estivill, X.; Marti, E. A highly expressed mir-101 isomir is a functional silencing small rna. BMC Genom. 2013, 14, 104. [Google Scholar] [CrossRef]
- Magee, R.; Telonis, A.G.; Cherlin, T.; Rigoutsos, I.; Londin, E. Assessment of isomir discrimination using commercial qpcr methods. Noncoding RNA 2017, 3, 18. [Google Scholar] [CrossRef]
- Heo, I.; Ha, M.; Lim, J.; Yoon, M.J.; Park, J.E.; Kwon, S.C.; Chang, H.; Kim, V.N. Mono-uridylation of pre-microrna as a key step in the biogenesis of group ii let-7 micrornas. Cell 2012, 151, 521–532. [Google Scholar] [CrossRef]
- Boele, J.; Persson, H.; Shin, J.W.; Ishizu, Y.; Newie, I.S.; Sokilde, R.; Hawkins, S.M.; Coarfa, C.; Ikeda, K.; Takayama, K.; et al. Papd5-mediated 3′ adenylation and subsequent degradation of mir-21 is disrupted in proliferative disease. Proc. Natl Acad Sci. USA 2014, 111, 11467–11472. [Google Scholar] [CrossRef]
- Westholm, J.O.; Ladewig, E.; Okamura, K.; Robine, N.; Lai, E.C. Common and distinct patterns of terminal modifications to mirtrons and canonical micrornas. RNA 2012, 18, 177–192. [Google Scholar] [CrossRef]
- Burroughs, A.M.; Ando, Y.; de Hoon, M.J.; Tomaru, Y.; Nishibu, T.; Ukekawa, R.; Funakoshi, T.; Kurokawa, T.; Suzuki, H.; Hayashizaki, Y.; et al. A comprehensive survey of 3′ animal mirna modification events and a possible role for 3′ adenylation in modulating mirna targeting effectiveness. Genome Res. 2010, 20, 1398–1410. [Google Scholar] [CrossRef]
- Liu, T.; Shen, S.K.; Xiong, J.G.; Xu, Y.; Zhang, H.Q.; Liu, H.J.; Lu, Z.G. Clinical significance of long noncoding rna spry4-it1 in melanoma patients. FEBS Open Bio 2016, 6, 147–154. [Google Scholar] [CrossRef]
- Dong, L.; Qi, P.; Xu, M.D.; Ni, S.J.; Huang, D.; Xu, Q.H.; Weng, W.W.; Tan, C.; Sheng, W.Q.; Zhou, X.Y.; et al. Circulating cudr, lsinct-5 and ptenp1 long noncoding rnas in sera distinguish patients with gastric cancer from healthy controls. Int. J. Cancer 2015, 137, 1128–1135. [Google Scholar] [CrossRef]
- Rykova, E.Y.; Wunsche, W.; Brizgunova, O.E.; Skvortsova, T.E.; Tamkovich, S.N.; Senin, I.S.; Laktionov, P.P.; Sczakiel, G.; Vlassov, V.V. Concentrations of circulating rna from healthy donors and cancer patients estimated by different methods. Ann. N. Y. Acad. Sci. 2006, 1075, 328–333. [Google Scholar] [CrossRef]
- Minatel, B.C.; Martinez, V.D.; Ng, K.W.; Sage, A.P.; Tokar, T.; Marshall, E.A.; Anderson, C.; Enfield, K.S.S.; Stewart, G.L.; Reis, P.P.; et al. Large-scale discovery of previously undetected micrornas specific to human liver. Hum. Genom. 2018, 12, 16. [Google Scholar] [CrossRef]
- Martinez, V.D.; Vucic, E.A.; Thu, K.L.; Hubaux, R.; Enfield, K.S.; Pikor, L.A.; Becker-Santos, D.D.; Brown, C.J.; Lam, S.; Lam, W.L. Unique somatic and malignant expression patterns implicate piwi-interacting rnas in cancer-type specific biology. Sci. Rep. 2015, 5, 10423. [Google Scholar] [CrossRef]
- Fehlmann, T.; Backes, C.; Kahraman, M.; Haas, J.; Ludwig, N.; Posch, A.E.; Wurstle, M.L.; Hubenthal, M.; Franke, A.; Meder, B.; et al. Web-based ngs data analysis using mirmaster: A large-scale meta-analysis of human mirnas. Nucleic Acids Res. 2017, 45, 8731–8744. [Google Scholar] [CrossRef]
- Kozomara, A.; Griffiths-Jones, S. Mirbase: Annotating high confidence micrornas using deep sequencing data. Nucleic Acids Res. 2014, 42, D68–D73. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Total | Epithelioid | Sarcomatoid | Mixed | Other |
|---|---|---|---|---|---|
| Number | 36 | 29 | 2 | 4 | 1 |
| Age (Mean ± SD) | 62.4 ± 5.04 | 62.5 ± 4.4 | 61.5 ± 0.7 | 62.6 ± 2.06 | 60 |
| Gender (M/F) | 33/3 | 26/3 | 2/0 | 4/0 | 1/0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kresoja-Rakic, J.; Szpechcinski, A.; Kirschner, M.B.; Ronner, M.; Minatel, B.; Martinez, V.D.; Lam, W.L.; Weder, W.; Stahel, R.; Früh, M.; et al. miR-625-3p and lncRNA GAS5 in Liquid Biopsies for Predicting the Outcome of Malignant Pleural Mesothelioma Patients Treated with Neo-Adjuvant Chemotherapy and Surgery. Non-Coding RNA 2019, 5, 41. https://doi.org/10.3390/ncrna5020041
Kresoja-Rakic J, Szpechcinski A, Kirschner MB, Ronner M, Minatel B, Martinez VD, Lam WL, Weder W, Stahel R, Früh M, et al. miR-625-3p and lncRNA GAS5 in Liquid Biopsies for Predicting the Outcome of Malignant Pleural Mesothelioma Patients Treated with Neo-Adjuvant Chemotherapy and Surgery. Non-Coding RNA. 2019; 5(2):41. https://doi.org/10.3390/ncrna5020041
Chicago/Turabian StyleKresoja-Rakic, Jelena, Adam Szpechcinski, Michaela B. Kirschner, Manuel Ronner, Brenda Minatel, Victor D. Martinez, Wan L. Lam, Walter Weder, Rolf Stahel, Martin Früh, and et al. 2019. "miR-625-3p and lncRNA GAS5 in Liquid Biopsies for Predicting the Outcome of Malignant Pleural Mesothelioma Patients Treated with Neo-Adjuvant Chemotherapy and Surgery" Non-Coding RNA 5, no. 2: 41. https://doi.org/10.3390/ncrna5020041
APA StyleKresoja-Rakic, J., Szpechcinski, A., Kirschner, M. B., Ronner, M., Minatel, B., Martinez, V. D., Lam, W. L., Weder, W., Stahel, R., Früh, M., Cerciello, F., & Felley-Bosco, E. (2019). miR-625-3p and lncRNA GAS5 in Liquid Biopsies for Predicting the Outcome of Malignant Pleural Mesothelioma Patients Treated with Neo-Adjuvant Chemotherapy and Surgery. Non-Coding RNA, 5(2), 41. https://doi.org/10.3390/ncrna5020041