
Decoding Salivary ncRNAomes as Novel Biomarkers for Oral Cancer Detection and Prognosis



Abstract
1. Introduction
2. Saliva in Diagnostic Application and the Emergence of Saliva Omics
3. Crosstalk Between ncRNAome and Oral Microbiota in OSCC
4. Targeting Salivary ncRNAome for Oral Cancer Detection
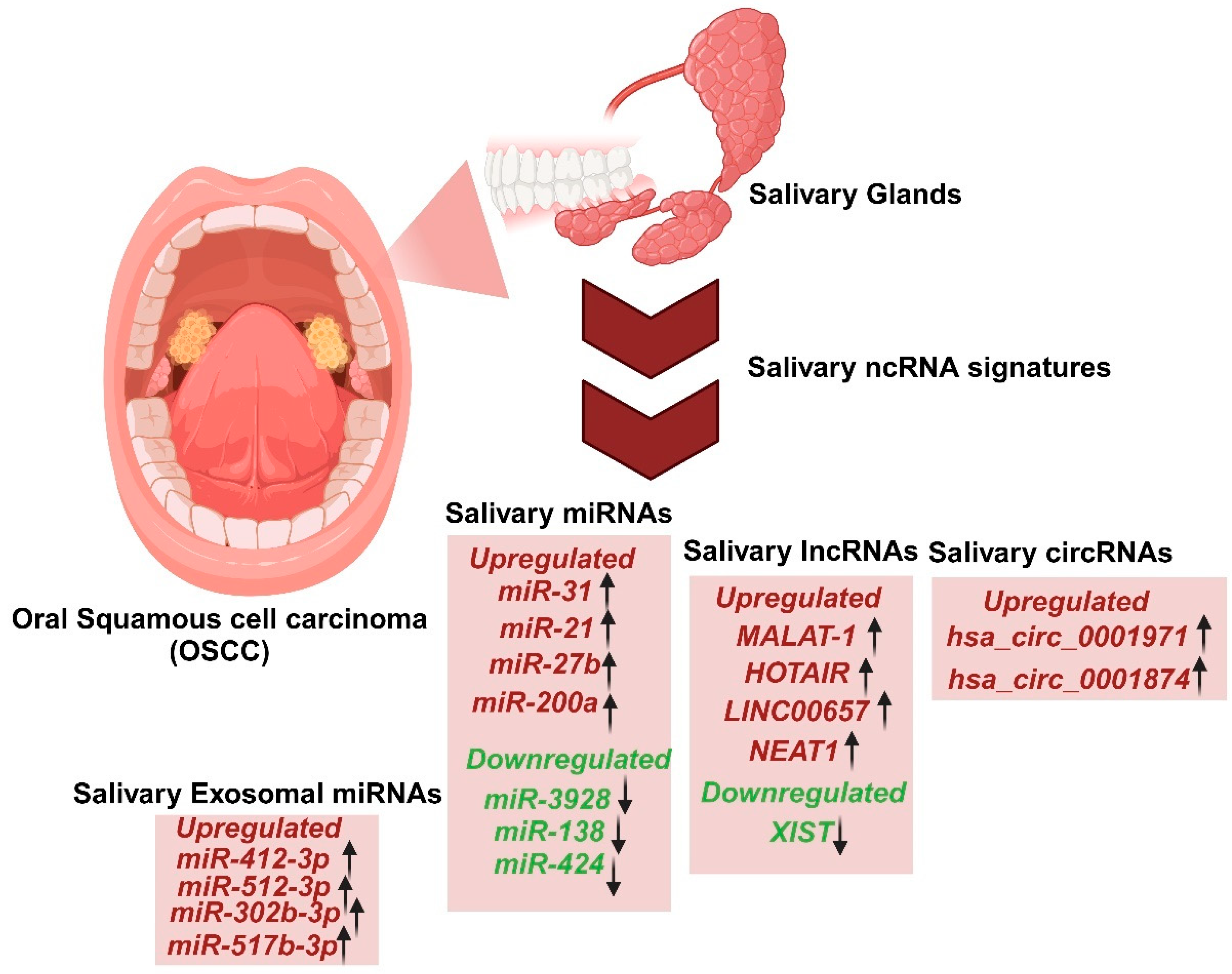
5. Role of Salivary ncRNAome as Potential Diagnostic Biomarkers
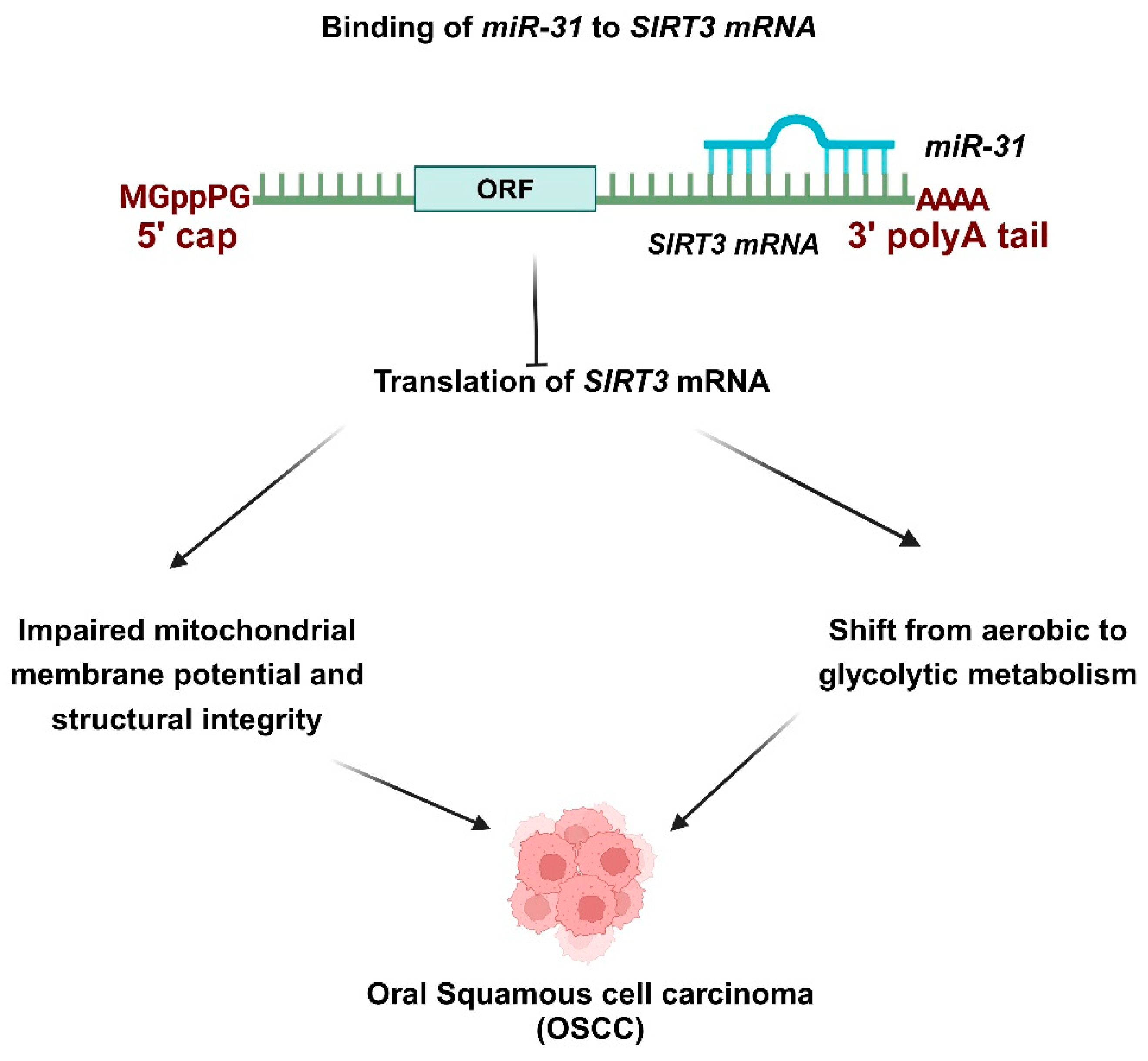
5.1. Role of Salivary miRNAs as a Biomarker for OSCC
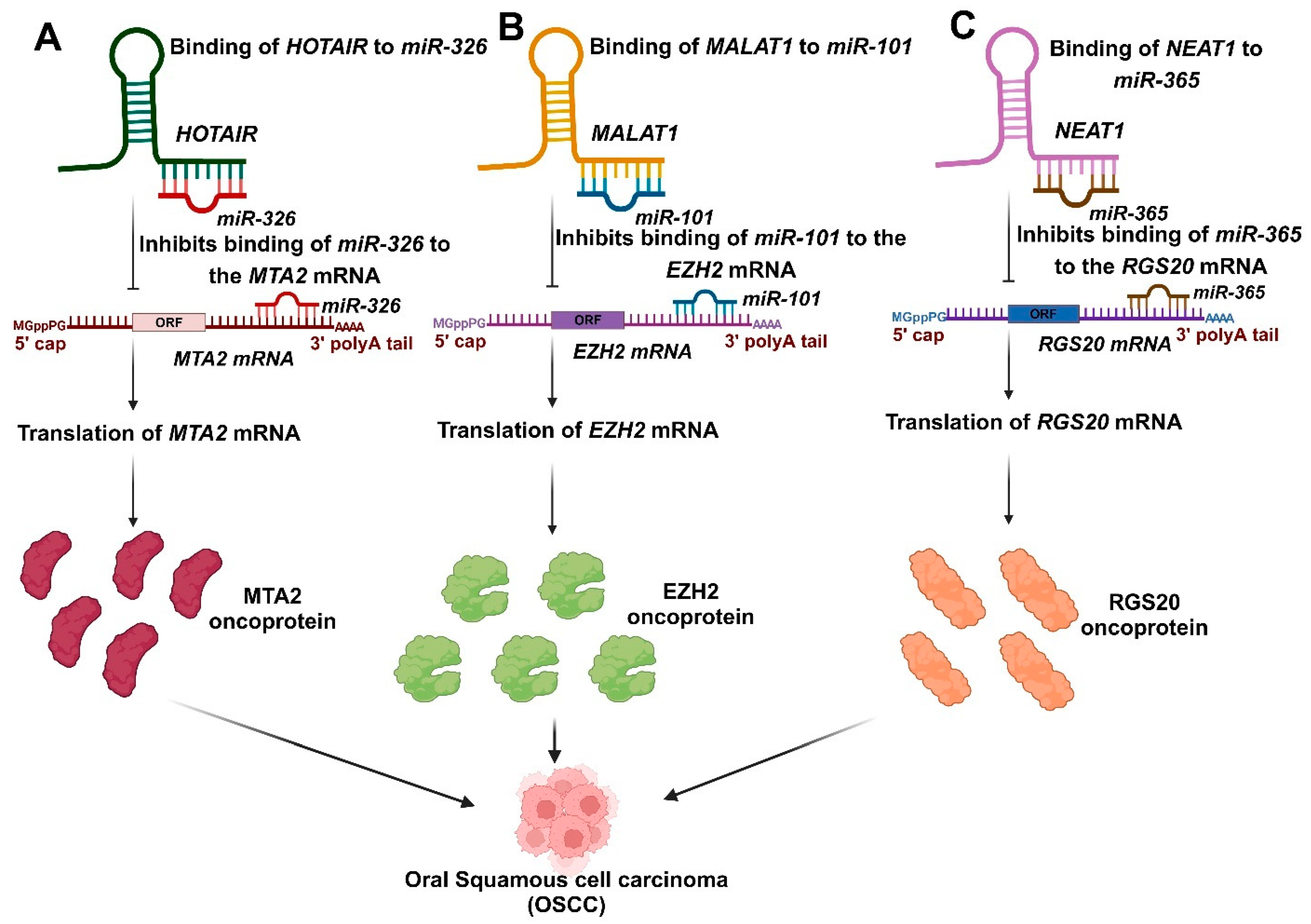
5.2. Role of Salivary lncRNAs as a Biomarker for OSCC
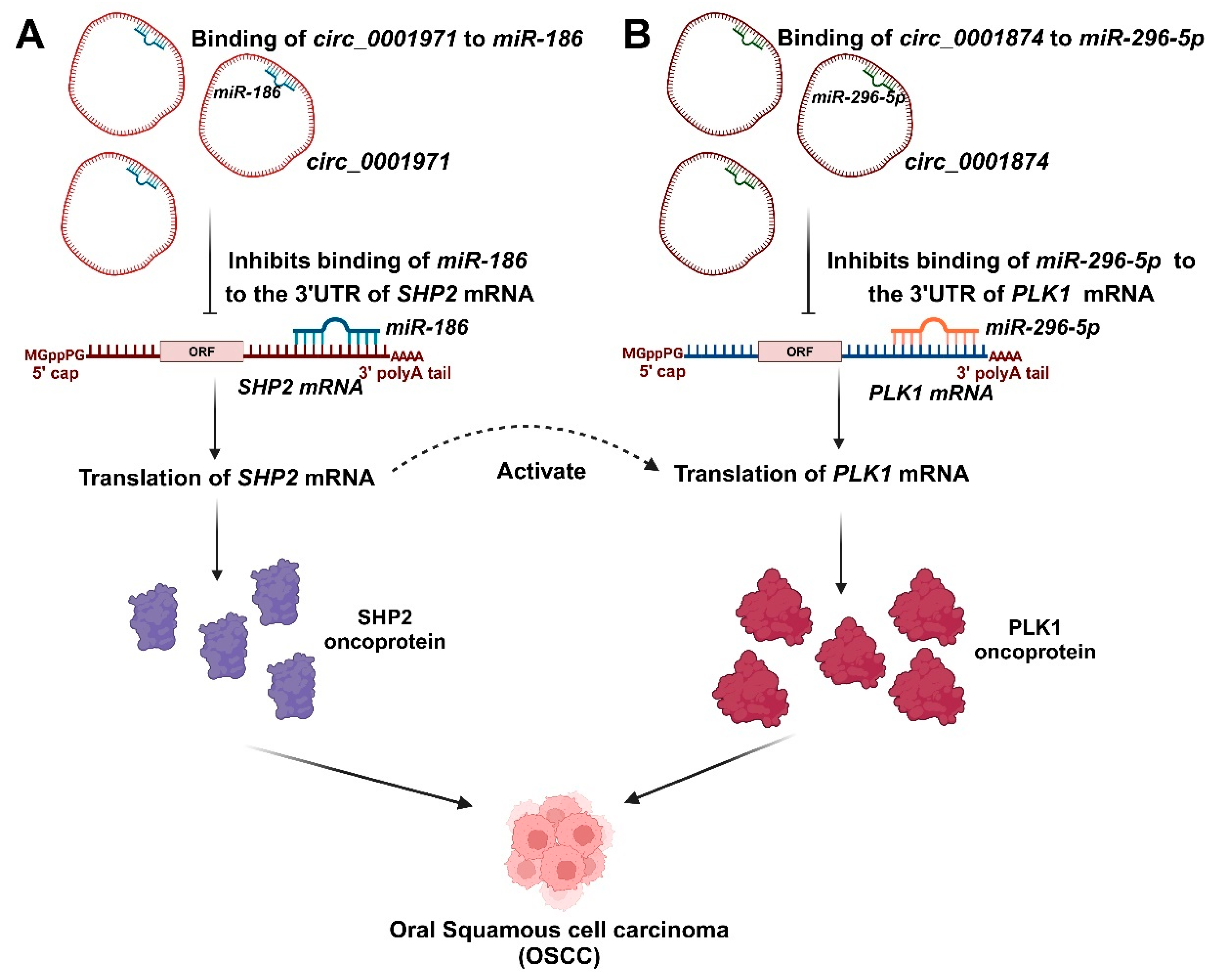
5.3. Role of Salivary circRNAs as a Biomarker for OSCC
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Dey, S.; Biswas, B.; Manoj Appadan, A.; Shah, J.; Pal, J.K.; Basu, S.; Sur, S. Non-Coding RNAs in Oral Cancer: Emerging Roles and Clinical Applications. Cancers 2023, 15, 3752. [Google Scholar] [CrossRef] [PubMed]
- Kalmatte, A.; Rekha, P.D.; Ratnacaram, C.K. Emerging Cell Cycle Related Non-Coding RNA Biomarkers from Saliva and Blood for Oral Squamous Cell Carcinoma. Mol. Biol. Rep. 2023, 50, 9479–9496. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Satyanarayana, L.; Asthana, S.; Shivalingesh, K.K.; Goutham, B.S.; Ramachandra, S. Oral Cancer Statistics in India on the Basis of First Report of 29 Population-Based Cancer Registries. J. Oral Maxillofac. Pathol. 2018, 22, 18–26. [Google Scholar] [CrossRef]
- Kumar, M.; Nanavati, R.; Modi, T.G.; Dobariya, C. Oral Cancer: Etiology and Risk Factors: A Review. J. Cancer Res. Ther. 2016, 12, 458–463. [Google Scholar] [CrossRef]
- Dey Ghosh, R.; Guha Majumder, S. Circulating Long Non-Coding RNAs Could Be the Potential Prognostic Biomarker for Liquid Biopsy for the Clinical Management of Oral Squamous Cell Carcinoma. Cancers 2022, 14, 5590. [Google Scholar] [CrossRef]
- Leemans, C.R.; Braakhuis, B.J.M.; Brakenhoff, R.H. The Molecular Biology of Head and Neck Cancer. Nat. Rev. Cancer 2011, 11, 9–22. [Google Scholar] [CrossRef]
- Rischin, D.; Ferris, R.L.; Le, Q.-T. Overview of Advances in Head and Neck Cancer. J. Clin. Oncol. 2015, 33, 3225–3226. [Google Scholar] [CrossRef]
- Sarkar, P.; Malik, S.; Laha, S.; Das, S.; Bunk, S.; Ray, J.G.; Chatterjee, R.; Saha, A. Dysbiosis of Oral Microbiota during Oral Squamous Cell Carcinoma Development. Front. Oncol. 2021, 11, 614448. [Google Scholar] [CrossRef]
- Sujir, N.; Ahmed, J.; Pai, K.; Denny, C.; Shenoy, N. Challenges in Early Diagnosis of Oral Cancer: Cases Series. Acta Stomatol. Croat. 2019, 53, 174–180. [Google Scholar] [CrossRef]
- Ai, L.; Chen, J.; Yan, H.; He, Q.; Luo, P.; Xu, Z.; Yang, X. Research Status and Outlook of PD-1/PD-L1 Inhibitors for Cancer Therapy. Drug Des. Devel. Ther. 2020, 14, 3625–3649. [Google Scholar] [CrossRef] [PubMed]
- Gharat, S.A.; Momin, M.; Bhavsar, C. Oral Squamous Cell Carcinoma: Current Treatment Strategies and Nanotechnology-Based Approaches for Prevention and Therapy. Crit. Rev. Ther. Drug Carrier Syst. 2016, 33, 363–400. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Liu, S.; Cai, G.; Kong, L.; Zhang, T.; Ren, Y.; Wu, Y.; Mei, M.; Zhang, L.; Wang, X. Long Non Coding RNA MALAT1 Promotes Tumor Growth and Metastasis by Inducing Epithelial-Mesenchymal Transition in Oral Squamous Cell Carcinoma. Sci. Rep. 2015, 5, 15972. [Google Scholar] [CrossRef] [PubMed]
- Yan, G.; Wang, X.; Yang, M.; Lu, L.; Zhou, Q. Long Non-Coding RNA TUG1 Promotes Progression of Oral Squamous Cell Carcinoma through Upregulating FMNL2 by Sponging MiR-219. Am. J. Cancer Res. 2017, 7, 1899–1912. [Google Scholar]
- Xiao, L.; Wang, W.; Zhao, J.; Xu, H.; Li, S.; Yang, X. LncRNA MALAT1 Promotes Cell Proliferation and Invasion by Regulating the MiR-101/EZH2 Axis in Oral Squamous Cell Carcinoma. Oncol. Lett. 2020, 20, 164. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, L.; Zhang, L.; Wang, Y.; Li, H.; Ren, X.; Wei, F.; Yu, W.; Liu, T.; Wang, X.; et al. Long Non-Coding RNA HOTAIR Promotes Tumor Cell Invasion and Metastasis by Recruiting EZH2 and Repressing E-Cadherin in Oral Squamous Cell Carcinoma. Int. J. Oncol. 2015, 46, 2586–2594. [Google Scholar] [CrossRef]
- Wu, J.; Xie, H. Expression of Long Noncoding RNA-HOX Transcript Antisense Intergenic RNA in Oral Squamous Cell Carcinoma and Effect on Cell Growth. Tumour Biol. 2015, 36, 8573–8578. [Google Scholar] [CrossRef]
- Liang, J.; Liang, L.; Ouyang, K.; Li, Z.; Yi, X. MALAT1 Induces Tongue Cancer Cells’ EMT and Inhibits Apoptosis through Wnt/β-Catenin Signaling Pathway. J. Oral Pathol. Med. 2017, 46, 98–105. [Google Scholar] [CrossRef]
- Ostenfeld, M.S.; Bramsen, J.B.; Lamy, P.; Villadsen, S.B.; Fristrup, N.; Sørensen, K.D.; Ulhøi, B.; Borre, M.; Kjems, J.; Dyrskjøt, L.; et al. MiR-145 Induces Caspase-Dependent and -Independent Cell Death in Urothelial Cancer Cell Lines with Targeting of an Expression Signature Present in Ta Bladder Tumors. Oncogene 2010, 29, 1073–1084. [Google Scholar] [CrossRef]
- Zahran, F.; Ghalwash, D.; Shaker, O.; Al-Johani, K.; Scully, C. Salivary MicroRNAs in Oral Cancer. Oral Dis. 2015, 21, 739–747. [Google Scholar] [CrossRef]
- Akao, Y.; Nakagawa, Y.; Naoe, T. MicroRNA-143 and -145 in Colon Cancer. DNA Cell Biol. 2007, 26, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Ozen, M.; Creighton, C.J.; Ozdemir, M.; Ittmann, M. Widespread Deregulation of MicroRNA Expression in Human Prostate Cancer. Oncogene 2008, 27, 1788–1793. [Google Scholar] [CrossRef]
- Ichimi, T.; Enokida, H.; Okuno, Y.; Kunimoto, R.; Chiyomaru, T.; Kawamoto, K.; Kawahara, K.; Toki, K.; Kawakami, K.; Nishiyama, K.; et al. Identification of Novel MicroRNA Targets Based on MicroRNA Signatures in Bladder Cancer. Int. J. Cancer 2009, 125, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Wang, X.-Y.; Gong, R.-G.; Li, A.; Yang, S.; Cao, Y.-T.; Wen, Y.-M.; Wang, C.-M.; Yi, X.-Z. The Expression Profile of MicroRNAs in a Model of 7,12-Dimethyl-Benz[a]Anthrance-Induced Oral Carcinogenesis in Syrian Hamster. J. Exp. Clin. Cancer Res. 2009, 28, 64. [Google Scholar] [CrossRef]
- Liu, Z.; Wei, S.; Ma, H.; Zhao, M.; Myers, J.N.; Weber, R.S.; Sturgis, E.M.; Wei, Q. A Functional Variant at the MiR-184 Binding Site in TNFAIP2 and Risk of Squamous Cell Carcinoma of the Head and Neck. Carcinogenesis 2011, 32, 1668–1674. [Google Scholar] [CrossRef]
- Wong, T.-S.; Liu, X.-B.; Wong, B.Y.-H.; Ng, R.W.-M.; Yuen, A.P.-W.; Wei, W.I. Mature MiR-184 as Potential Oncogenic MicroRNA of Squamous Cell Carcinoma of Tongue. Clin. Cancer Res. 2008, 14, 2588–2592. [Google Scholar] [CrossRef]
- Punj, A. Secretions of Human Salivary Gland. In Salivary Glands—New Approaches in Diagnostics and Treatment; IntechOpen: London, UK, 2019; ISBN 9781789849882. [Google Scholar]
- Rajendran, P.; Sekar, R.; Zahra, H.A.; Jayaraman, S.; Rajagopal, P.; Abdallah, B.M.; Ali, E.M.; Abdelsalam, S.A.; Veeraraghavan, V. Salivaomics to Decode Non-Coding RNAs in Oral Cancer. A Narrative Review. Noncoding RNA Res. 2023, 8, 376–384. [Google Scholar] [CrossRef]
- Chicharro, J.L.; Lucía, A.; Pérez, M.; Vaquero, A.F.; Ureña, R. Saliva Composition and Exercise. Sports Med. 1998, 26, 17–27. [Google Scholar] [CrossRef]
- Ziobro, A.; Bartosz, G. A Comparison of the Total Antioxidant Capacity of Some Human Body Fluids. Cell. Mol. Biol. Lett. 2003, 8, 415–419. [Google Scholar]
- Nagler, R.M.; Klein, I.; Zarzhevsky, N.; Drigues, N.; Reznick, A.Z. Characterization of the Differentiated Antioxidant Profile of Human Saliva. Free Radic. Biol. Med. 2002, 32, 268–277. [Google Scholar] [CrossRef]
- Burke, J.C.; Evans, C.A.; Crosby, T.R.; Mednieks, M.I. Expression of Secretory Proteins in Oral Fluid after Orthodontic Tooth Movement. Am. J. Orthod. Dentofacial Orthop. 2002, 121, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Dozic, I.; Todorovic, T. Antimicrobial Peptides of Human Saliva. Stomatol. Glas. Srb. 2005, 52, 208–216. [Google Scholar] [CrossRef]
- Todorović, T.; Dozić, I.; Mandić, B.; Marjanović, M. Antioxidant role of saliva in maintaining oral health. Vojnosanit. Pregl. 2005, 62, 575–579. [Google Scholar] [CrossRef]
- Andjelski-Radicevic, B.; Dozic, I. Biochemical Markers in Saliva in Patients with Oral Cancer. Stomatol. Glas. Srb. 2020, 67, 201–207. [Google Scholar] [CrossRef]
- Contucci, A.M.; Inzitari, R.; Agostino, S.; Vitali, A.; Fiorita, A.; Cabras, T.; Scarano, E.; Messana, I. Statherin Levels in Saliva of Patients with Precancerous and Cancerous Lesions of the Oral Cavity: A Preliminary Report. Oral Dis. 2005, 11, 95–99. [Google Scholar] [CrossRef]
- Shintani, S.; Hamakawa, H.; Ueyama, Y.; Hatori, M.; Toyoshima, T. Identification of a Truncated Cystatin SA-I as a Saliva Biomarker for Oral Squamous Cell Carcinoma Using the SELDI ProteinChip Platform. Int. J. Oral Maxillofac. Surg. 2010, 39, 68–74. [Google Scholar] [CrossRef]
- Bernardes, V.F.; Gleber-Netto, F.O.; Sousa, S.F.; Silva, T.A.; Abreu, M.H.N.G.; Aguiar, M.C.F. EGF in Saliva and Tumor Samples of Oral Squamous Cell Carcinoma. Appl. Immunohistochem. Mol. Morphol. 2011, 19, 528–533. [Google Scholar] [CrossRef]
- Balicki, R.; Grabowska, S.Z.; Citko, A. Salivary Epidermal Growth Factor in Oral Cavity Cancer. Oral Oncol. 2005, 41, 48–55. [Google Scholar] [CrossRef]
- Ghallab, N.A.; Shaker, O.G. Serum and Salivary Levels of Chemerin and MMP-9 in Oral Squamous Cell Carcinoma and Oral Premalignant Lesions. Clin. Oral Investig. 2017, 21, 937–947. [Google Scholar] [CrossRef]
- Shpitzer, T.; Hamzany, Y.; Bahar, G.; Feinmesser, R.; Savulescu, D.; Borovoi, I.; Gavish, M.; Nagler, R.M. Salivary Analysis of Oral Cancer Biomarkers. Br. J. Cancer 2009, 101, 1194–1198. [Google Scholar] [CrossRef]
- Ha, N.H.; Park, D.G.; Woo, B.H.; Kim, D.J.; Choi, J.I.; Park, B.S.; Kim, Y.D.; Lee, J.H.; Park, H.R. Porphyromonas Gingivalis Increases the Invasiveness of Oral Cancer Cells by Upregulating IL-8 and MMPs. Cytokine 2016, 86, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Atanasova, K.R.; Yilmaz, Ö. Prelude to Oral Microbes and Chronic Diseases: Past, Present and Future. Microbes Infect. 2015, 17, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Tan, X.; Cheng, J.; Liu, Z.; Zhou, H.; Liao, J.; Wang, X.; Liu, H. Oral Microbiome and Its Relationship with Oral Cancer. J. Cancer Res. Ther. 2024, 20, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Arunkumar, G.; Deva Magendhra Rao, A.K.; Manikandan, M.; Arun, K.; Vinothkumar, V.; Revathidevi, S.; Rajkumar, K.S.; Rajaraman, R.; Munirajan, A.K. Expression Profiling of Long Non-Coding RNA Identifies Linc-RoR as a Prognostic Biomarker in Oral Cancer. Tumour Biol. 2017, 39, 1010428317698366. [Google Scholar] [CrossRef]
- Williamson, S.; Munro, C.; Pickler, R.; Grap, M.J.; Elswick, R.K., Jr. Comparison of Biomarkers in Blood and Saliva in Healthy Adults. Nurs. Res. Pract. 2012, 2012, 246178. [Google Scholar] [CrossRef]
- Hofman, L.F. Human Saliva as a Diagnostic Specimen. J. Nutr. 2001, 131, 1621S–1625S. [Google Scholar] [CrossRef]
- Sindhu, S.; Jagannathan, N. Saliva: A Cutting Edge in Diagnostic Procedures. J. Oral Dis. 2014, 2014, 168584. [Google Scholar] [CrossRef]
- Cui, Y.; Yang, M.; Zhu, J.; Zhang, H.; Duan, Z.; Wang, S.; Liao, Z.; Liu, W. Developments in Diagnostic Applications of Saliva in Human Organ Diseases. Med. Nov. Technol. Devices 2022, 13, 100115. [Google Scholar] [CrossRef]
- Shah, F.D.; Begum, R.; Vajaria, B.N.; Patel, K.R.; Patel, J.B.; Shukla, S.N.; Patel, P.S. A Review on Salivary Genomics and Proteomics Biomarkers in Oral Cancer. Indian J. Clin. Biochem. 2011, 26, 326–334. [Google Scholar] [CrossRef]
- Patil, S.; Arakeri, G.; Alamir, A.W.H.; Awan, K.H.; Baeshen, H.; Ferrari, M.; Patil, S.; Fonseca, F.P.; Brennan, P.A. Role of Salivary Transcriptomics as Potential Biomarkers in Oral Cancer: A Systematic Review. J. Oral Pathol. Med. 2019, 48, 871–879. [Google Scholar] [CrossRef]
- Esperouz, F.; Ciavarella, D.; Santarelli, A.; Lorusso, M.; Lo Muzio, L.; Laino, L.; Lo Russo, L. Saliva-Based Biomarkers in Oral Squamous Cell Carcinoma Using OMICS Technologies: A Systematic Review. Oral 2024, 4, 293–302. [Google Scholar] [CrossRef]
- Gibb, E.A.; Enfield, K.S.S.; Stewart, G.L.; Lonergan, K.M.; Chari, R.; Ng, R.T.; Zhang, L.; MacAulay, C.E.; Rosin, M.P.; Lam, W.L. Long Non-Coding RNAs Are Expressed in Oral Mucosa and Altered in Oral Premalignant Lesions. Oral Oncol. 2011, 47, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Tarrad, N.A.F.; Hassan, S.; Shaker, O.G.; AbdelKawy, M. Salivary LINC00657 and MiRNA-106a as Diagnostic Biomarkers for Oral Squamous Cell Carcinoma, an Observational Diagnostic Study. BMC Oral Health 2023, 23, 994. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Wu, Z.; Zhang, J.; Su, B. Salivary LncRNA as a Potential Marker for Oral Squamous Cell Carcinoma Diagnosis. Mol. Med. Rep. 2013, 7, 761–766. [Google Scholar] [CrossRef]
- Zhao, S.-Y.; Wang, J.; Ouyang, S.-B.; Huang, Z.-K.; Liao, L. Salivary Circular RNAs Hsa_circ_0001874 and Hsa_circ_0001971 as Novel Biomarkers for the Diagnosis of Oral Squamous Cell Carcinoma. Cell. Physiol. Biochem. 2018, 47, 2511–2521. [Google Scholar] [CrossRef]
- Mazumder, S.; Datta, S.; Ray, J.G.; Chaudhuri, K.; Chatterjee, R. Liquid Biopsy: MiRNA as a Potential Biomarker in Oral Cancer. Cancer Epidemiol. 2019, 58, 137–145. [Google Scholar] [CrossRef]
- Momen-Heravi, F.; Trachtenberg, A.J.; Kuo, W.P.; Cheng, Y.S. Genomewide Study of Salivary MicroRNAs for Detection of Oral Cancer. J. Dent. Res. 2014, 93, 86S–93S. [Google Scholar] [CrossRef]
- Koneru, S.; Tanikonda, R. Salivaomics—A Promising Future in Early Diagnosis of Dental Diseases. Dent. Res. J. 2014, 11, 11–15. [Google Scholar]
- Duz, M.B.; Karatas, O.F.; Guzel, E.; Turgut, N.F.; Yilmaz, M.; Creighton, C.J.; Ozen, M. Identification of MiR-139-5p as a Saliva Biomarker for Tongue Squamous Cell Carcinoma: A Pilot Study. Cell. Oncol. 2016, 39, 187–193. [Google Scholar] [CrossRef]
- Jia, G.; Zhi, A.; Lai, P.F.H.; Wang, G.; Xia, Y.; Xiong, Z.; Zhang, H.; Che, N.; Ai, L. The Oral Microbiota—A Mechanistic Role for Systemic Diseases. Br. Dent. J. 2018, 224, 447–455. [Google Scholar] [CrossRef]
- Kilian, M.; Chapple, I.L.C.; Hannig, M.; Marsh, P.D.; Meuric, V.; Pedersen, A.M.L.; Tonetti, M.S.; Wade, W.G.; Zaura, E. The Oral Microbiome—An Update for Oral Healthcare Professionals. Br. Dent. J. 2016, 221, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.; Kolodziejczyk, A.A.; Thaiss, C.A.; Elinav, E. Dysbiosis and the Immune System. Nat. Rev. Immunol. 2017, 17, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Saikia, P.J.; Pathak, L.; Mitra, S.; Das, B. The Emerging Role of Oral Microbiota in Oral Cancer Initiation, Progression and Stemness. Front. Immunol. 2023, 14, 1198269. [Google Scholar] [CrossRef] [PubMed]
- Su, S.-C.; Chang, L.-C.; Huang, H.-D.; Peng, C.-Y.; Chuang, C.-Y.; Chen, Y.-T.; Lu, M.-Y.; Chiu, Y.-W.; Chen, P.-Y.; Yang, S.-F. Oral Microbial Dysbiosis and Its Performance in Predicting Oral Cancer. Carcinogenesis 2021, 42, 127–135. [Google Scholar] [CrossRef]
- Irfan, M.; Delgado, R.Z.R.; Frias-Lopez, J. The Oral Microbiome and Cancer. Front. Immunol. 2020, 11, 591088. [Google Scholar] [CrossRef]
- Mager, D.L.; Haffajee, A.D.; Devlin, P.M.; Norris, C.M.; Posner, M.R.; Goodson, J.M. The Salivary Microbiota as a Diagnostic Indicator of Oral Cancer: A Descriptive, Non-Randomized Study of Cancer-Free and Oral Squamous Cell Carcinoma Subjects. J. Transl. Med. 2005, 3, 27. [Google Scholar] [CrossRef]
- Kakabadze, M.Z.; Paresishvili, T.; Karalashvili, L.; Chakhunashvili, D.; Kakabadze, Z. Oral Microbiota and Oral Cancer: Review. Oncol. Rev. 2020, 14, 476. [Google Scholar] [CrossRef]
- Perera, M.; Al-Hebshi, N.N.; Perera, I.; Ipe, D.; Ulett, G.C.; Speicher, D.J.; Chen, T.; Johnson, N.W. Inflammatory Bacteriome and Oral Squamous Cell Carcinoma. J. Dent. Res. 2018, 97, 725–732. [Google Scholar] [CrossRef]
- Zhao, H.; Chu, M.; Huang, Z.; Yang, X.; Ran, S.; Hu, B.; Zhang, C.; Liang, J. Variations in Oral Microbiota Associated with Oral Cancer. Sci. Rep. 2017, 7, 11773. [Google Scholar] [CrossRef]
- Al-Hebshi, N.N.; Nasher, A.T.; Idris, A.M.; Chen, T. Robust Species Taxonomy Assignment Algorithm for 16S RRNA NGS Reads: Application to Oral Carcinoma Samples. J. Oral Microbiol. 2015, 7, 28934. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Yeh, Y.-M.; Yu, H.-Y.; Chin, C.-Y.; Hsu, C.-W.; Liu, H.; Huang, P.-J.; Hu, S.-N.; Liao, C.-T.; Chang, K.-P.; et al. Oral Microbiota Community Dynamics Associated with Oral Squamous Cell Carcinoma Staging. Front. Microbiol. 2018, 9, 862. [Google Scholar] [CrossRef] [PubMed]
- Hardefeldt, H.A.; Cox, M.R.; Eslick, G.D. Association between Human Papillomavirus (HPV) and Oesophageal Squamous Cell Carcinoma: A Meta-Analysis. Epidemiol. Infect. 2014, 142, 1119–1137. [Google Scholar] [CrossRef] [PubMed]
- Liyanage, S.S.; Rahman, B.; Ridda, I.; Newall, A.T.; Tabrizi, S.N.; Garland, S.M.; Segelov, E.; Seale, H.; Crowe, P.J.; Moa, A.; et al. The Aetiological Role of Human Papillomavirus in Oesophageal Squamous Cell Carcinoma: A Meta-Analysis. PLoS ONE 2013, 8, e69238. [Google Scholar] [CrossRef]
- Petrick, J.L.; Wyss, A.B.; Butler, A.M.; Cummings, C.; Sun, X.; Poole, C.; Smith, J.S.; Olshan, A.F. Prevalence of Human Papillomavirus among Oesophageal Squamous Cell Carcinoma Cases: Systematic Review and Meta-Analysis. Br. J. Cancer 2014, 110, 2369–2377. [Google Scholar] [CrossRef]
- Syrjänen, K.; Syrjänen, S. Detection of Human Papillomavirus in Esophageal Papillomas: Systematic Review and Meta-Analysis. Apmis 2013, 121, 363–374. [Google Scholar] [CrossRef]
- Carpén, T.; Syrjänen, S.; Jouhi, L.; Randen-Brady, R.; Haglund, C.; Mäkitie, A.; Mattila, P.S.; Hagström, J. Epstein-Barr Virus (EBV) and Polyomaviruses Are Detectable in Oropharyngeal Cancer and EBV May Have Prognostic Impact. Cancer Immunol. Immunother. 2020, 69, 1615–1626. [Google Scholar] [CrossRef]
- Drop, B.; Strycharz-Dudziak, M.; Kliszczewska, E.; Polz-Dacewicz, M. Coinfection with Epstein-Barr Virus (EBV), Human Papilloma Virus (HPV) and Polyoma BK Virus (BKPyV) in Laryngeal, Oropharyngeal and Oral Cavity Cancer. Int. J. Mol. Sci. 2017, 18, 2752. [Google Scholar] [CrossRef]
- Jalouli, J.; Jalouli, M.M.; Sapkota, D.; Ibrahim, S.O.; Larsson, P.-A.; Sand, L. Human Papilloma Virus, Herpes Simplex Virus and Epstein Barr Virus in Oral Squamous Cell Carcinoma from Eight Different Countries. Anticancer Res. 2012, 32, 571–580. [Google Scholar]
- Djuric, M.; Jankovic, L.; Jovanovic, T.; Pavlica, D.; Brkic, S.; Knezevic, A.; Markovic, D.; Milasin, J. Prevalence of Oral Herpes Simplex Virus Reactivation in Cancer Patients: A Comparison of Different Techniques of Viral Detection. J. Oral Pathol. Med. 2009, 38, 167–173. [Google Scholar] [CrossRef]
- Lou, E.; Kellman, R.M.; Shillitoe, E.J. Effect of Herpes Simplex Virus Type-1 on Growth of Oral Cancer in an Immunocompetent, Orthotopic Mouse Model. Oral Oncol. 2002, 38, 349–356. [Google Scholar] [CrossRef]
- Koivikko, T.; Rodrigues, P.C.; Vehviläinen, M.; Hyvönen, P.; Sundquist, E.; Arffman, R.K.; Al-Samadi, A.; Välimaa, H.; Salo, T.; Risteli, M. Detection of Herpes Simplex Virus in Oral Tongue Squamous Cell Carcinoma. Front. Pharmacol. 2023, 14, 1182152. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, N.; Litlekalsøy, J.; Ahmed, I.A.; Martinsen, E.M.H.; Furriol, J.; Javier-Lopez, R.; Elsheikh, M.; Gaafar, N.M.; Morgado, L.; Mundra, S.; et al. Analysis of Salivary Mycobiome in a Cohort of Oral Squamous Cell Carcinoma Patients from Sudan Identifies Higher Salivary Carriage of Malassezia as an Independent and Favorable Predictor of Overall Survival. Front. Cell. Infect. Microbiol. 2021, 11, 673465. [Google Scholar] [CrossRef] [PubMed]
- Mohd Bakri, M.; Mohd Hussaini, H.; Rachel Holmes, A.; David Cannon, R.; Mary Rich, A. Revisiting the Association between Candidal Infection and Carcinoma, Particularly Oral Squamous Cell Carcinoma. J. Oral Microbiol. 2010, 2, 5780. [Google Scholar] [CrossRef]
- Salgado, R.; Fonseca, D.; Marques, A.; Napoleao, S.; França, T.; Akashi, K.; Prado, C.; Baiocchi, G.; Plaça, D.; Filgueiras, I.; et al. The Network Interplay of Type 1 Interferon and Toll-like Receptor Signaling Cascades Hallmarks the Immune Response against Candida spp. Infections. Res. Sq. 2021, 11, 10–21203. [Google Scholar]
- Gholizadeh, P.; Eslami, H.; Yousefi, M.; Asgharzadeh, M.; Aghazadeh, M.; Kafil, H.S. Role of Oral Microbiome on Oral Cancers, a Review. Biomed. Pharmacother. 2016, 84, 552–558. [Google Scholar] [CrossRef]
- Pushalkar, S.; Ji, X.; Li, Y.; Estilo, C.; Yegnanarayana, R.; Singh, B.; Li, X.; Saxena, D. Comparison of Oral Microbiota in Tumor and Non-Tumor Tissues of Patients with Oral Squamous Cell Carcinoma. BMC Microbiol. 2012, 12, 144. [Google Scholar] [CrossRef]
- Chang, C.; Geng, F.; Shi, X.; Li, Y.; Zhang, X.; Zhao, X.; Pan, Y. The Prevalence Rate of Periodontal Pathogens and Its Association with Oral Squamous Cell Carcinoma. Appl. Microbiol. Biotechnol. 2019, 103, 1393–1404. [Google Scholar] [CrossRef]
- Zhang, S.; Li, C.; Zhang, Z.; Li, Y.; Li, Q.; Geng, F.; Liu, J.; Pan, Y. Analysis of Differentially Expressed Genes in Oral Epithelial Cells Infected with Fusobacterium Nucleatum for Revealing Genes Associated with Oral Cancer. J. Cell. Mol. Med. 2021, 25, 892–904. [Google Scholar] [CrossRef]
- Sales, C.B.S.; Buim, M.E.C.; de Souza, R.O.; de Faro Valverde, L.; Mathias Machado, M.C.; Reis, M.G.; Soares, F.A.; Ramos, E.A.G.; Gurgel Rocha, C.A. Elevated VEGFA MRNA Levels in Oral Squamous Cell Carcinomas and Tumor Margins: A Preliminary Study. J. Oral Pathol. Med. 2016, 45, 481–485. [Google Scholar] [CrossRef]
- Huang, S.; Sun, Y. Long Noncoding RNA MNX1-AS1 Functions as a Competing Endogenous RNA to Regulate Epithelial-Mesenchymal Transition by Sponging MiR-744-5p in Colorectal Cancer. Biosci. Biotechnol. Biochem. 2021, 85, 568–578. [Google Scholar] [CrossRef]
- Gao, Y.; Xu, Y.; Wang, J.; Yang, X.; Wen, L.; Feng, J. LncRNA MNX1-AS1 Promotes Glioblastoma Progression through Inhibition of MiR-4443. Oncol. Res. 2019, 27, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Pan, Y.; Pan, Y.; Wang, O. MNX1-AS1 Is a Functional Oncogene That Induces EMT and Activates the AKT/MTOR Pathway and MNX1 in Breast Cancer. Cancer Manag. Res. 2019, 11, 803–812. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Li, C.; Liu, J.; Geng, F.; Shi, X.; Li, Q.; Lu, Z.; Pan, Y. Fusobacterium Nucleatum Promotes Epithelial-Mesenchymal Transiton through Regulation of the LncRNA MIR4435-2HG/MiR-296-5p/Akt2/SNAI1 Signaling Pathway. FEBS J. 2020, 287, 4032–4047. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Wang, H.; Liu, J.; Pan, C.; Zhang, D.; Li, X.; Pan, Y. Porphyromonas Gingivalis Infection Promoted the Proliferation of Oral Squamous Cell Carcinoma Cells through the MiR-21/PDCD4/AP-1 Negative Signaling Pathway. ACS Infect. Dis. 2019, 5, 1336–1347. [Google Scholar] [CrossRef]
- Liu, D.; Liu, S.; Liu, J.; Miao, L.; Zhang, S.; Pan, Y. SRNA23392 Packaged by Porphyromonas Gingivalis Outer Membrane Vesicles Promotes Oral Squamous Cell Carcinomas Migration and Invasion by Targeting Desmocollin-2. Mol. Oral Microbiol. 2021, 36, 182–191. [Google Scholar] [CrossRef]
- Choi, J.-W.; Um, J.-H.; Cho, J.-H.; Lee, H.-J. Tiny RNAs and Their Voyage via Extracellular Vesicles: Secretion of Bacterial Small RNA and Eukaryotic MicroRNA. Exp. Biol. Med. 2017, 242, 1475–1481. [Google Scholar] [CrossRef]
- Tran, N.; Khoury, S. Biomarkers of Oral, Pharyngeal and Laryngeal Cancers. U.S. Patent 17/888, 20 July 2023. [Google Scholar]
- Chu, H.-W.; Chang, K.-P.; Hsu, C.-W.; Chang, I.Y.-F.; Liu, H.-P.; Chen, Y.-T.; Wu, C.-C. Identification of Salivary Biomarkers for Oral Cancer Detection with Untargeted and Targeted Quantitative Proteomics Approaches. Mol. Cell. Proteom. 2019, 18, 1796–1806. [Google Scholar] [CrossRef]
- Markopoulos, A.K.; Michailidou, E.Z.; Tzimagiorgis, G. Salivary Markers for Oral Cancer Detection. Open Dent. J. 2010, 4, 172–178. [Google Scholar] [CrossRef]
- Kolenda, T.; Ryś, M.; Guglas, K.; Teresiak, A.; Bliźniak, R.; Mackiewicz, J.; Lamperska, K. Quantification of Long Non-Coding RNAs Using QRT-PCR: Comparison of Different CDNA Synthesis Methods and RNA Stability. Arch. Med. Sci. 2021, 17, 1006–1015. [Google Scholar] [CrossRef]
- Lee, M.R.; Mantel, C.; Lee, S.A.; Moon, S.-H.; Broxmeyer, H.E. MiR-31/SDHA Axis Regulates Reprogramming Efficiency through Mitochondrial Metabolism. Stem Cell Rep. 2016, 7, 1–10. [Google Scholar] [CrossRef]
- Hung, P.-S.; Tu, H.-F.; Kao, S.-Y.; Yang, C.-C.; Liu, C.-J.; Huang, T.-Y.; Chang, K.-W.; Lin, S.-C. MiR-31 Is Upregulated in Oral Premalignant Epithelium and Contributes to the Immortalization of Normal Oral Keratinocytes. Carcinogenesis 2014, 35, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Farshbaf, A.; Mohajertehran, F.; Aghaee-Bakhtiari, S.H.; Ayatollahi, H.; Douzandeh, K.; Pakfetrat, A.; Mohtasham, N. Downregulation of Salivary MiR-3928 as a Potential Biomarker in Patients with Oral Squamous Cell Carcinoma and Oral Lichen Planus. Clin. Exp. Dent. Res. 2024, 10, e877. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.; Qu, Y.; Dang, S.; Yao, B.; Ji, M. MiR-145 Inhibits Oral Squamous Cell Carcinoma (OSCC) Cell Growth by Targeting c-Myc and Cdk6. Cancer Cell Int. 2013, 13, 51. [Google Scholar] [CrossRef]
- Shalaby, R.; Ibrahim, S.; Kotb, A.A.W.; Baz, S.; Hafed, L.; Shaker, O.; Afifi, S. MALAT1 as a Potential Salivary Biomarker in Oral Squamous Cell Carcinoma through Targeting MiRNA-124. Oral Dis. 2024, 30, 2075–2083. [Google Scholar] [CrossRef]
- Zhang, C.-Z. Long Intergenic Non-Coding RNA 668 Regulates VEGFA Signaling through Inhibition of MiR-297 in Oral Squamous Cell Carcinoma. Biochem. Biophys. Res. Commun. 2017, 489, 404–412. [Google Scholar] [CrossRef]
- Xu, F.-Y.; Xu, X.; Hu, X.-D. LINC00657 Promotes Malignant Progression of Oral Squamous Cell Carcinoma via Regulating MicroRNA-150. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2482–2490. [Google Scholar]
- He, K.; Zhu, Z.-B.; Shu, R.; Hong, A. LncRNA NEAT1 Mediates Progression of Oral Squamous Cell Carcinoma via VEGF-A and Notch Signaling Pathway. World J. Surg. Oncol. 2020, 18, 261. [Google Scholar] [CrossRef]
- Huang, G.; He, X.; Wei, X.-L. LncRNA NEAT1 Promotes Cell Proliferation and Invasion by Regulating MiR-365/RGS20 in Oral Squamous Cell Carcinoma. Oncol. Rep. 2018, 39, 1948–1956. [Google Scholar] [CrossRef]
- Wang, J.; Ouyang, S.; Zhang, X.; Zhao, S.; Cheng, M.; Fan, X.; Cai, Y.; Liao, L. Deregulation of Hsa_circ_0001971/MiR-186 and Hsa_circ_0001874/MiR-296 Signaling Pathways Promotes the Proliferation of Oral Squamous Carcinoma Cells by Synergistically Activating SHP2/PLK1 Signals. Sci. Rep. 2021, 11, 20561. [Google Scholar]
- Ghafouri-Fard, S.; Shoorei, H.; Anamag, F.T.; Taheri, M. The Role of Non-Coding RNAs in Controlling Cell Cycle Related Proteins in Cancer Cells. Front. Oncol. 2020, 10, 608975. [Google Scholar] [CrossRef]
- Jia, H.; Wang, X.; Sun, Z. Screening and Validation of Plasma Long Non-Coding RNAs as Biomarkers for the Early Diagnosis and Staging of Oral Squamous Cell Carcinoma. Oncol. Lett. 2021, 21, 172. [Google Scholar] [CrossRef] [PubMed]
- Bolha, L.; Ravnik-Glavač, M.; Glavač, D. Long Noncoding RNAs as Biomarkers in Cancer. Dis. Markers 2017, 2017, 7243968. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-J.; Lin, S.-C.; Yang, C.-C.; Cheng, H.-W.; Chang, K.-W. Exploiting Salivary MiR-31 as a Clinical Biomarker of Oral Squamous Cell Carcinoma. Head Neck 2012, 34, 219–224. [Google Scholar] [CrossRef]
- Singh, P.; Srivastava, A.N.; Sharma, R.; Mateen, S.; Shukla, B.; Singh, A.; Chandel, S. Circulating MicroRNA-21 Expression as a Novel Serum Biomarker for Oral Sub-Mucous Fibrosis and Oral Squamous Cell Carcinoma. Asian Pac. J. Cancer Prev. 2018, 19, 1053–1057. [Google Scholar]
- Zhu, B.; Cao, X.; Zhang, W.; Pan, G.; Yi, Q.; Zhong, W.; Yan, D. MicroRNA-31-5p Enhances the Warburg Effect via Targeting FIH. FASEB J. 2019, 33, 545–556. [Google Scholar] [CrossRef]
- Huang, F.; Xin, C.; Lei, K.; Bai, H.; Li, J.; Chen, Q. Noncoding RNAs in Oral Premalignant Disorders and Oral Squamous Cell Carcinoma. Cell. Oncol. 2020, 43, 763–777. [Google Scholar] [CrossRef]
- Xu, H.; Liu, X.; Zhao, J. Down-Regulation of MiR-3928 Promoted Osteosarcoma Growth. Cell. Physiol. Biochem. 2014, 33, 1547–1556. [Google Scholar] [CrossRef]
- Mulcahy, E.Q.X.; Zhang, Y.; Colόn, R.R.; Cain, S.R.; Gibert, M.K., Jr.; Dube, C.J.; Hafner, M.; Abounader, R. MicroRNA 3928 Suppresses Glioblastoma through Downregulation of Several Oncogenes and Upregulation of P53. Int. J. Mol. Sci. 2022, 23, 3930. [Google Scholar] [CrossRef]
- Rocchetti, F.; Tenore, G.; Macali, F.; Vicidomini, T.; Podda, G.M.; Fantozzi, P.J.; Silvestri, V.; Porzio, V.; Valentini, V.; Ottini, L.; et al. Expression Analysis of Circulating MicroRNAs in Saliva and Plasma for the Identification of Clinically Relevant Biomarkers for Oral Squamous Cell Carcinoma and Oral Potentially Malignant Disorders. Cancers 2024, 16, 2990. [Google Scholar] [CrossRef]
- Arunkumar, G.; Deva Magendhra Rao, A.; Manikandan, M.; Prasanna Srinivasa Rao, H.; Subbiah, S.; Ilangovan, R.; Murugan, A.; Munirajan, A. Dysregulation of MiR-200 Family MicroRNAs and Epithelial-Mesenchymal Transition Markers in Oral Squamous Cell Carcinoma. Oncol. Lett. 2017, 15, 649–657. [Google Scholar] [CrossRef]
- Koopaie, M.; Akhbari, P.; Fatahzadeh, M.; Kolahdooz, S. Identification of Common Salivary MiRNA in Oral Lichen Planus and Oral Squamous Cell Carcinoma: Systematic Review and Meta-Analysis. BMC Oral Health 2024, 24, 1177. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, E.D.; Gao, S.; Hulf, T.; Sibbritt, T.; Nair, S.; Costea, D.E.; Villadsen, S.B.; Bakholdt, V.; Bramsen, J.B.; Sørensen, J.A.; et al. MicroRNA Alterations and Associated Aberrant DNA Methylation Patterns across Multiple Sample Types in Oral Squamous Cell Carcinoma. PLoS ONE 2011, 6, e27840. [Google Scholar] [CrossRef] [PubMed]
- Park, N.J.; Zhou, H.; Elashoff, D.; Henson, B.S.; Kastratovic, D.A.; Abemayor, E.; Wong, D.T. Salivary MicroRNA: Discovery, Characterization, and Clinical Utility for Oral Cancer Detection. Clin. Cancer Res. 2009, 15, 5473–5477. [Google Scholar] [CrossRef] [PubMed]
- Mehdipour, M.; Shahidi, M.; Manifar, S.; Jafari, S.; Mashhadi Abbas, F.; Barati, M.; Mortazavi, H.; Shirkhoda, M.; Farzanegan, A.; Elmi Rankohi, Z. Diagnostic and Prognostic Relevance of Salivary MicroRNA-21, -125a, -31 and -200a Levels in Patients with Oral Lichen Planus—A Short Report. Cell. Oncol. 2018, 41, 329–334. [Google Scholar] [CrossRef]
- Bahrami, N.; Pirrafiee, M.; Azadi, F.; Azimnejad, R.; Fotook Kiaei, S.Z.; Abbasi, A.J.; Kazempour Dizaji, M.; Lookzadeh, S.; Nejatollahi, S.M.R.; Daustani, M.; et al. Biomarkers for Oral Squamous Cell Carcinoma (MiR-24, MiR-200, and MiR-34): Screening and Detection MicroRNA. Asian Pac. J. Cancer Prev. 2024, 25, 2265–2269. [Google Scholar] [CrossRef]
- Saikishore, R.; Velmurugan, P.; Ranjithkumar, D.; Latha, R.; Sathiamoorthi, T.; Arun, A.; Ravi, A.V.; Sivakumar, S. The Circular RNA-MiRNA Axis: A Special RNA Signature Regulatory Transcriptome as a Potential Biomarker for OSCC. Mol. Ther. Nucleic Acids 2020, 22, 352–361. [Google Scholar] [CrossRef]
- Gai, C.; Camussi, F.; Broccoletti, R.; Gambino, A.; Cabras, M.; Molinaro, L.; Carossa, S.; Camussi, G.; Arduino, P.G. Salivary Extracellular Vesicle-Associated MiRNAs as Potential Biomarkers in Oral Squamous Cell Carcinoma. BMC Cancer 2018, 18, 439. [Google Scholar] [CrossRef]
- Scapoli, L.; Palmieri, A.; Lo Muzio, L.; Pezzetti, F.; Rubini, C.; Girardi, A.; Farinella, F.; Mazzotta, M.; Carinci, F. MicroRNA Expression Profiling of Oral Carcinoma Identifies New Markers of Tumor Progression. Int. J. Immunopathol. Pharmacol. 2010, 23, 1229–1234. [Google Scholar] [CrossRef]
- Tao, D.; Zhang, Z.; Liu, X.; Zhang, Z.; Fu, Y.; Zhang, P.; Yuan, H.; Liu, L.; Cheng, J.; Jiang, H. LncRNA HOTAIR Promotes the Invasion and Metastasis of Oral Squamous Cell Carcinoma through Metastasis-Associated Gene 2. Mol. Carcinog. 2020, 59, 353–364. [Google Scholar] [CrossRef]
- Zhang, B.; Zhang, H.; Shen, G. Metastasis-Associated Protein 2 (MTA2) Promotes the Metastasis of Non-Small-Cell Lung Cancer through the Inhibition of the Cell Adhesion Molecule Ep-CAM and E-Cadherin. Jpn. J. Clin. Oncol. 2015, 45, 755–766. [Google Scholar] [CrossRef]
- Cheng, C.-Y.; Chou, Y.-E.; Ko, C.-P.; Yang, S.-F.; Hsieh, S.-C.; Lin, C.-L.; Hsieh, Y.-H.; Chen, K.-C. Metastasis Tumor-Associated Protein-2 Knockdown Suppresses the Proliferation and Invasion of Human Glioma Cells in Vitro and in Vivo. J. Neurooncol. 2014, 120, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Ji, J.; Cai, Q.; Shi, M.; Chen, X.; Yu, Y.; Liu, B.; Zhu, Z.; Zhang, J. MTA2 Promotes Gastric Cancer Cells Invasion and Is Transcriptionally Regulated by Sp1. Mol. Cancer 2013, 12, 102. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Xu, X.-J.; Lin, Y.; Chen, Q.-Y.; Sun, W.-J.; Tang, L.; Liang, Q.-X. LncRNA MALAT1 Expression Inhibition Suppresses Tongue Squamous Cell Carcinoma Proliferation, Migration and Invasion by Inactivating PI3K/Akt Pathway and Downregulating MMP-9 Expression. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 198–206. [Google Scholar] [PubMed]
- Iwai, S.; Yonekawa, A.; Harada, C.; Hamada, M.; Katagiri, W.; Nakazawa, M.; Yura, Y. Involvement of the Wnt-β-Catenin Pathway in Invasion and Migration of Oral Squamous Carcinoma Cells. Int. J. Oncol. 2010, 37, 1095–1103. [Google Scholar] [CrossRef]
- Shieh, T.-M.; Liu, C.-J.; Hsia, S.-M.; Ningrum, V.; Liao, C.-C.; Lan, W.-C.; Shih, Y.-H. Lack of Salivary Long Non-Coding RNA XIST Expression Is Associated with Increased Risk of Oral Squamous Cell Carcinoma: A Cross-Sectional Study. J. Clin. Med. 2021, 10, 4622. [Google Scholar] [CrossRef]
- Bahn, J.H.; Zhang, Q.; Li, F.; Chan, T.-M.; Lin, X.; Kim, Y.; Wong, D.T.W.; Xiao, X. The Landscape of MicroRNA, Piwi-Interacting RNA, and Circular RNA in Human Saliva. Clin. Chem. 2015, 61, 221–230. [Google Scholar] [CrossRef]
- Panta, P.; Wong, D.T.W. Salivary Biomarkers in Oral Cancer. In Oral Cancer Detection; Springer International Publishing: Cham, Switzerland, 2019; pp. 265–295. ISBN 9783319612546. [Google Scholar]
- Meng, S.; Zhou, H.; Feng, Z.; Xu, Z.; Tang, Y.; Li, P.; Wu, M. CircRNA: Functions and Properties of a Novel Potential Biomarker for Cancer. Mol. Cancer 2017, 16, 94. [Google Scholar] [CrossRef]
- Wang, F.; Nazarali, A.J.; Ji, S. Circular RNAs as Potential Biomarkers for Cancer Diagnosis and Therapy. Am. J. Cancer Res. 2016, 6, 1167–1176. [Google Scholar]
- Cai, Z.; Hao, X.-Y.; Liu, F.-X. MicroRNA-186 Serves as a Tumor Suppressor in Oral Squamous Cell Carcinoma by Negatively Regulating the Protein Tyrosine Phosphatase SHP2 Expression. Arch. Oral Biol. 2018, 89, 20–25. [Google Scholar] [CrossRef]
- Xu, C.; Li, S.; Chen, T.; Hu, H.; Ding, C.; Xu, Z.; Chen, J.; Liu, Z.; Lei, Z.; Zhang, H.-T.; et al. MiR-296-5p Suppresses Cell Viability by Directly Targeting PLK1 in Non-Small Cell Lung Cancer. Oncol. Rep. 2016, 35, 497–503. [Google Scholar] [CrossRef]
- Vittal, K.; Pandian, S.S.; Joseph, L.D.; Raj, S.G. Immunohistochemical Expression of Polo-like Kinase 1 in Oral Squamous Cell Carcinoma and Oral Submucous Fibrosis. Indian J. Dent. Res. 2018, 29, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Dhamija, S.; Menon, M.B. Non-Coding Transcript Variants of Protein-Coding Genes—What Are They Good For? RNA Biol. 2018, 15, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Winkle, M.; El-Daly, S.M.; Fabbri, M.; Calin, G.A. Noncoding RNA Therapeutics—Challenges and Potential Solutions. Nat. Rev. Drug Discov. 2021, 20, 629–651. [Google Scholar] [CrossRef]
- Yang, C.; Xiao, F. Biomarkers Related to Oral Squamous Cell Carcinoma and Methods of Diagnosis and Treatment Thereof. U.S. Patent 18/000,197, 29 June 2023. [Google Scholar]
- Wong, D.T.W. Salivary Extracellular Noncoding RNA: Emerging Biomarkers for Molecular Diagnostics. Clin. Ther. 2015, 37, 540–551. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Salivary microRNAs | |||
|---|---|---|---|
| Name | Level of Expression | Results | References |
| miR-31 | Upregulation |
| [102,103] |
| miR-3928 | Downregulation |
| [104,105] |
| Salivary lncRNAs | |||
| MALAT 1 | Upregulation |
| [15,106,107] |
| HOTAIR | Upregulation |
| [55] |
| LINC00657 | Upregulation |
| [54,108] |
| NEAT1 | Upregulation |
| [55,109,110] |
| Salivary circRNAs | |||
| hsa_circ_0001874 | Upregulation |
| [56,111] |
| hsa_circ_0001971 | Upregulation |
| [56,111] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Das, S.; Basak, S.; Sarkar, S. Decoding Salivary ncRNAomes as Novel Biomarkers for Oral Cancer Detection and Prognosis. Non-Coding RNA 2025, 11, 28. https://doi.org/10.3390/ncrna11020028
Das S, Basak S, Sarkar S. Decoding Salivary ncRNAomes as Novel Biomarkers for Oral Cancer Detection and Prognosis. Non-Coding RNA. 2025; 11(2):28. https://doi.org/10.3390/ncrna11020028
Chicago/Turabian StyleDas, Subhadeep, Sampad Basak, and Soumyadev Sarkar. 2025. "Decoding Salivary ncRNAomes as Novel Biomarkers for Oral Cancer Detection and Prognosis" Non-Coding RNA 11, no. 2: 28. https://doi.org/10.3390/ncrna11020028
APA StyleDas, S., Basak, S., & Sarkar, S. (2025). Decoding Salivary ncRNAomes as Novel Biomarkers for Oral Cancer Detection and Prognosis. Non-Coding RNA, 11(2), 28. https://doi.org/10.3390/ncrna11020028