
White Spot Lesion Treatment Options: A Systematic Review of Different Techniques for Masking These Lesions

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Methods
2.1. Study Sources
2.2. Search Strategy
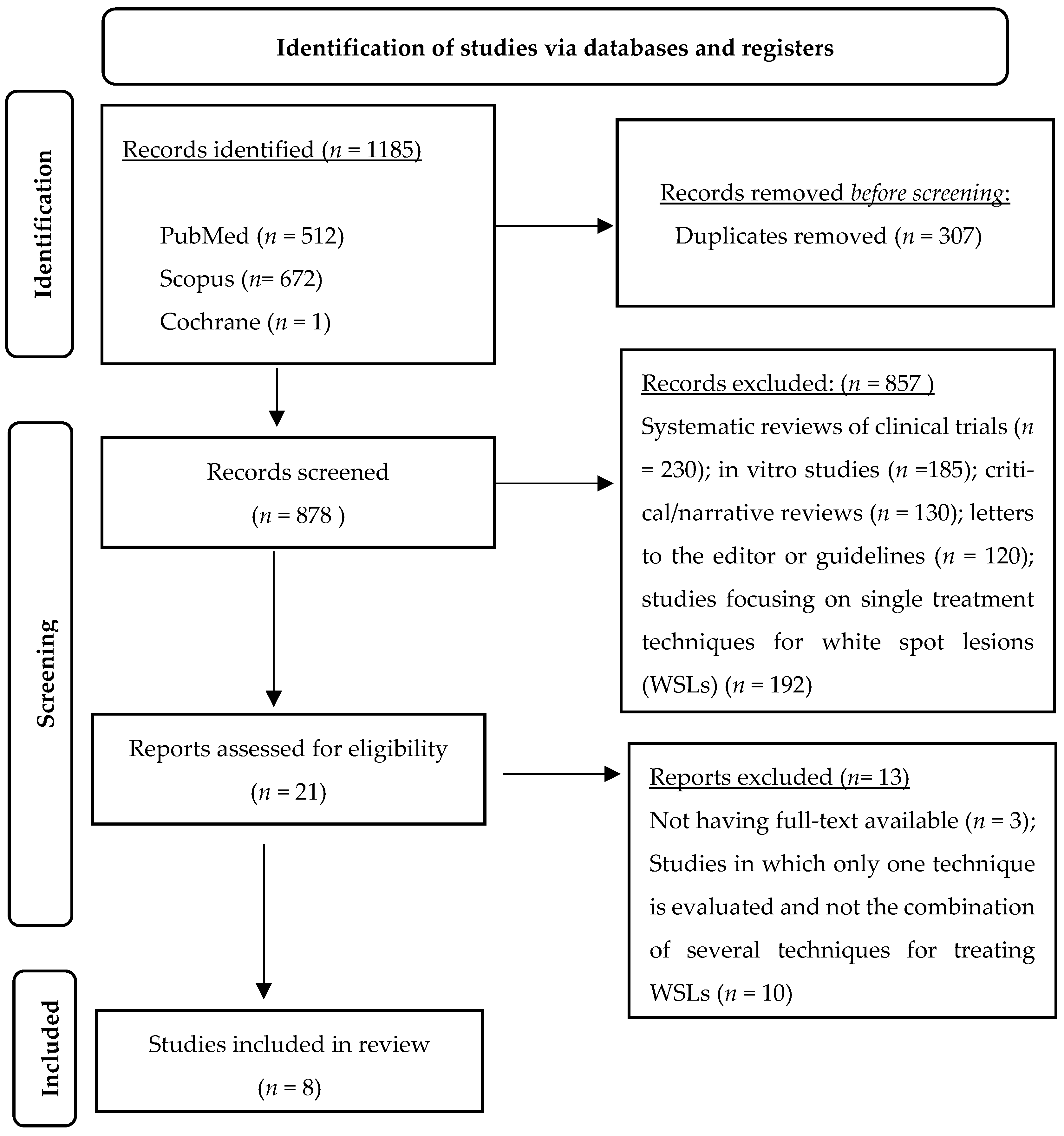
3. Results
3.1. Characteristics of the Studies
3.2. Risk of Bias Analysis
4. Discussion
4.1. Remineralizing Gels
4.2. Fluoride Gel Therapies
4.3. Ozone, Fluoride, and Octenidine
4.4. Resin Infiltration and Fluoride Varnish
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| WSLs | White Spot Lesions |
| CPP-ACP | Casein Phosphopeptide–Amorphous Calcium Phosphate |
| ICDAS | International Caries Detection and Assessment System |
| ECM | Electronic Caries Monitor |
| QLF | Quantitative Light-Induced Fluorescence |
| TEGDMA | Triethylene Glycol Dimethacrylate |
| DEJ | Dentin–Enamel Junction |
| MI Paste Plus | Casein Phosphopeptide–Amorphous Calcium Phosphate with Fluoride |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RCT | Randomized Clinical Trial |
References
- Xie, Z.; Yu, L.; Li, S.; Li, J.; Liu, Y. Comparison of therapies of white spot lesions: A systematic review and network meta-analysis. BMC Oral Health 2023, 23, 346. [Google Scholar] [CrossRef]
- Khoroushi, M.; Kachuie, M. Prevention and treatment of white spot lesions in orthodontic patients. Contemp. Clin. Dent. 2017, 8, 11–19. [Google Scholar] [CrossRef]
- Levy, F.M.; Braga, A.S.; Pelá, V.T.; Lavender, S.; Zhang, D.; Pilch, S.; Malheiros, Z.; Stewart, B.; Magalhães, A.C.; Buzalaf, M.A.R. Characterization of white spot lesions formed on human enamel under microcosm biofilm for different experimental periods. J. Appl. Oral Sci. 2022, 30, e20210560. [Google Scholar] [CrossRef] [PubMed]
- Dikmen, B. Icdas II Criteria (International Caries Detection and Assessment System). J. Istanb. Univ. Fac. Dent. 2015, 49, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Kidd, E.A.M.; Fejerskov, O. What Constitutes Dental Caries? Histopathology of Carious Enamel and Dentin Related to the Action of Cariogenic Biofilms. J. Dent. Res. 2010, 83, 35–38. [Google Scholar] [CrossRef]
- Cazzolla, A.P.; De Franco, A.R.; Lacaita, M.; Lacarbonara, V. Efficacy of 4-year treatment of icon infiltration resin on postorthodontic white spot lesions. BMJ Case Rep. 2018, 2018, 225639. [Google Scholar] [CrossRef] [PubMed]
- Gugnani, N.; Pandit, I.K.; Gupta, M.; Josan, R. Caries infiltration of noncavitated white spot lesions: A novel approach for immediate esthetic improvement. Contemp. Clin. Dent. 2012, 3, S199–S202. [Google Scholar] [CrossRef]
- Denis, M.; Atlan, A.; Vennat, E.; Tirlet, G.; Attal, J.-P.; Attal White, J.-P. White defects on enamel: Diagnosis and anatomopathology: Two essential factors for proper treatment (part 1). Int. Orthod. 2013, 11, 139–165. [Google Scholar] [CrossRef]
- Guerra, F.; Mazur, M.; Nardi, G.M. Dental hypomineralized enamel resin infiltration. Clinical indications and limits. Senses Sci. 2015, 2, 135–139. [Google Scholar] [CrossRef]
- De, J.; Farias, O.; Catarina, M.; Cunha, A.; Martins, V.L.; Mathias, P. Microinvasive esthetic approach for deep enamel white spot lesion. Dent. Res. J. 2022, 19, 29. [Google Scholar]
- Lopes, P.C.; Carvalho, T.; Gomes, A.T.P.C.; Veiga, N.; Blanco, L.; Correia, M.J.; Mello-Moura, A.C.V. White spot lesions: Diagnosis and treatment–A systematic review. BMC Oral Health 2024, 24, 58. [Google Scholar] [CrossRef] [PubMed]
- Al Dhubayb, S.; Al Sultan, M.; Al Sudairi, S.; Hakami, F.; Al Sweleh, F.S. Ability of dentists and students to detect caries by using the international caries detection and assessment system. Clin. Cosmet. Investig. Dent. 2021, 13, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Pretty, I.A.; Ellwood, R.P. The caries continuum: Opportunities to detect, treat and monitor the re-mineralization of early caries lesions. J. Dent. 2013, 41, S12–S21. [Google Scholar] [CrossRef] [PubMed]
- Pretty, I.A. Caries detection and diagnosis: Novel technologies. J. Dent. 2006, 34, 727–739. [Google Scholar] [CrossRef]
- Zandoná, A.F.; Santiago, E.; Eckert, G.; Fontana, M.; Ando, M.; Zero, D.T. Use of ICDAS combined with quantitative light-induced fluorescence as a caries detection method. Caries Res. 2010, 44, 317–322. [Google Scholar] [CrossRef]
- Paris, S.; Schwendicke, F.; Keltsch, J.; Dörfer, C.; Meyer-Lueckel, H. Masking of white spot lesions by resin infiltration in vitro. J. Dent. 2013, 41, e28–e34. [Google Scholar] [CrossRef]
- Gkavela, G.; Kakouris, V.; Pappa, E.; Rahiotis, C. Effect of Bleaching Agents on Healthy Enamel, White Spots, and Carious Lesions: A Systematic Review and Meta-Analysis. Dent. J. 2024, 12, 140. [Google Scholar] [CrossRef]
- Eimar, H.; Siciliano, R.; Abdallah, M.-N.; Nader, S.A.; Amin, W.M.; Martinez, P.-P.; Celemin, A.; Cerruti, M.; Tamimi, F. Hydrogen peroxide whitens teeth by oxidizing the organic structure. J. Dent. 2012, 40, e25–e33. [Google Scholar] [CrossRef]
- Araújo, G.S.A.; Naufel, F.S.; Alonso, R.C.B.; Lima, D.A.N.L.; Puppin-Rontani, R.M. Influence of staining solution and bleaching on color stability of resin used for caries infiltration. Oper. Dent. 2015, 40, E250–E256. [Google Scholar] [CrossRef]
- Bergstrand, F.; Twetman, S. A Review on Prevention and Treatment of Post-Orthodontic White Spot Lesions-Evidence-Based Methods and Emerging Technologies. Open Dent. J. 2011, 5, 158–162. [Google Scholar] [CrossRef]
- Paula, A.B.P.; Fernandes, A.R.; Coelho, A.S.; Marto, C.M.; Ferreira, M.M.; Caramelo, F.; Vale, F.D.; Carrilho, E. Therapies for White Spot Lesions—A Systematic Review. J. Evid.-Based Dent. Pract. 2017, 17, 23–38. [Google Scholar] [CrossRef] [PubMed]
- Tong, L.S.M.; Pang, M.K.M.; Mok, N.Y.C.; King, N.M.; Wei, S.H.Y. The Effects of Etching, Micro-abrasion, and Bleaching on Surface Enamel. J. Dent. Res. 1993, 72, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Khoroushi, M.; Mazaheri, H.; Saneie, T.; Samimi, P. Fracture toughness of bleached enamel: Effect of applying three different nanobiomaterials by nanoindentation test. Contemp. Clin. Dent. 2016, 7, 209–215. [Google Scholar] [CrossRef]
- Mota, S.M.; Enoki, C.; Ito, I.Y.; Elias, A.M.; Matsumoto, M.A.N. Streptococcus mutans counts in plaque adjacent to orthodontic brackets bonded with resin-modified glass ionomer cement or resin-based composite Orthodontics. Braz. Oral Res. 2008, 22, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Paris, S.; Meyer-Luecke’·, H.; Kielbassa, A.M. Resin Infiltration of Natural Caries Lesions. J. Dent. Res. 2007, 86, 662–666. [Google Scholar] [CrossRef]
- Senestraro, S.V.; Crowe, J.J.; Wang, M.; Vo, A.; Huang, G.; Ferracane, J.; Covell, D.A. Minimally invasive resin infiltration of arrested white-spot lesions: A randomized clinical trial. J. Am. Dent. Assoc. 2013, 144, 997–1005. [Google Scholar] [CrossRef]
- Ma, X.; Lin, X.; Zhong, T.; Xie, F. Evaluation of the efficacy of casein phosphopeptide-amorphous calcium phosphate on remineralization of white spot lesions in vitro and clinical research: A systematic review and meta-analysis. BMC Oral Health 2019, 19, 295. [Google Scholar] [CrossRef]
- Rose, R.K. Binding Characteristics of Streptococcus mutans for Calcium and Casein Phosphopeptide. Caries Res. 2000, 34, 427–431. [Google Scholar] [CrossRef]
- Karabekiroğlu, S.; Ünlü, N.; Küçükyilmaz, E.; Şener, S.; Botsali, M.S.; Malkoç, S. Treatment of post-orthodontic white spot lesions with CPP-ACP paste: A three year follow up study. Dent. Mater. J. 2017, 36, 791–797. [Google Scholar] [CrossRef]
- Marinho, V.C.C. Cochrane reviews of randomized trials of fluoride therapies for preventing dental caries. Eur. Arch. Paediatr. Dent. 2009, 10, 183–191. [Google Scholar] [CrossRef]
- Buzalaf, M.A.R.; Pessan, J.P.; Honório, H.M.; Ten Cate, J.M. Impact of Fluoride in the Prevention of Caries and Erosion Buzalaf MAR (ed): Fluoride and the Oral Mechanisms of Action of Fluoride for Caries Control. Monogr. Oral Sci. 2011, 22, 97–114. [Google Scholar] [PubMed]
- Urquhart, O.; Tampi, M.P.; Pilcher, L.; Slayton, R.L.; Araujo, M.; Fontana, M.; Guzmán-Armstrong, S.; Nascimento, M.M.; Nový, B.; Tinanoff, N.; et al. Nonrestorative Treatments for Caries: Systematic Review and Network Meta-analysis. J. Dent. Res. 2019, 98, 14–26. [Google Scholar] [CrossRef]
- Schiffner, U. Use of fluorides for caries prevention. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2021, 64, 830–837. [Google Scholar] [CrossRef]
- Grocholewicz, K.; Mikłasz, P.; Zawiślak, A.; Sobolewska, E.; Janiszewska-Olszowska, J. Fluoride varnish, ozone and octenidine reduce the incidence of white spot lesions and caries during orthodontic treatment: Randomized controlled trial. Sci. Rep. 2022, 12, 13985. [Google Scholar] [CrossRef] [PubMed]
- Rai, P.; Pandey, R.K.; Khanna, R. Qualitative and Quantitative Effect of a Protective Chlorhexidine Varnish Layer Over Resin-infiltrated Proximal Carious Lesions in Primary Teeth. Pediatr. Dent. 2016, 34, 40–45. [Google Scholar]
- Sonesson, M.; Twetman, S. Prevention of white spot lesions with fluoride varnish during orthodontic treatment with fixed appliances: A systematic review. Eur. J. Orthod. 2023, 45, 485–490. [Google Scholar] [CrossRef]
- Aboulnaga, M.A.; Akah, M.M.; Hassanein, O.E.S. Evaluation of Remineralization Potential of Remin Pro Forte vs Remin Pro on White Spot Lesions: A Randomized Clinical Trial. J. Contemp. Dent. Pract. 2022, 23, 520–526. [Google Scholar] [CrossRef]
- Heravi, F.; Ahrari, F.; Tanbakuchi, B. Effectiveness of MI Paste Plus and Remin Pro on remineralization and color improvement of postorthodontic white spot lesions. Dent. Res. J. 2018, 15, 95–103. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Julian Higgins, E.P.; Savović, J.; Page, M.J.; Sterne, J.A. Revised Cochrane Risk of Bias Tool for Randomized Trials (RoB 2.0). 2016. Available online: https://www.unisa.edu.au/contentassets/72bf75606a2b4abcaf7f17404af374ad/rob2-0_cluster_parallel_guidance.pdf (accessed on 12 May 2025).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Rechmann, P.; Bekmezian, S.; Rechmann, B.M.T.; Chaffee, B.W.; Featherstone, J.D.B. MI varnish and MI paste plus in a caries prevention and remineralization study: A randomized controlled trial. Clin. Oral Investig. 2018, 22, 2229–2239. [Google Scholar] [CrossRef]
- Turska-Szybka, A.; Gozdowski, D.; Mierzwińska-Nastalska, E.; Olczak-Kowalczyk, D. Randomised Clinical Trial on Resin Infiltration and Fluoride Varnish vs Fluoride Varnish Treatment Only of Smooth-surface Early Caries Lesions in Deciduous Teeth. Oral Health Prev. Dent. 2016, 14, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, M.; Mehrabkhani, M.; Ahrari, F.; Parisay, I.; Jahantigh, M. The effects of three remineralizing agents on regression of white spot lesions in children: A two-week, single-blind, randomized clinical trial. J. Clin. Exp. Dent. 2017, 9, e641–e648. [Google Scholar] [CrossRef] [PubMed]
- Güçlü, Z.A.; Alaçam, A.; Coleman, N.J. A 12-Week Assessment of the Treatment of White Spot Lesions with CPP-ACP Paste and/or Fluoride Varnish. BioMed Res. Int. 2016, 2016, 8357621. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, 14898. [Google Scholar] [CrossRef]
- Jones, R.S.; Fried, D. Remineralization of Enamel Caries Can Decrease Optical Reflectivity. J. Dent. Res. 2006, 85, 804–808. [Google Scholar] [CrossRef] [PubMed]
- Karlinsey, R.L.; Mackey, A.C.; Walker, E.R.; Amaechi, B.T.; Karthikeyan, R.; Najibfard, K.; Pfarrer, A.M. Remineralization potential of 5,000 ppm fluoride dentifrices evaluated in a pH cycling model. J. Dent. Oral Hyg. 2010, 2, A316A40869. [Google Scholar]
- Jayarajan, J.; Janardhanam, P.; Jayakumar, P.; Deepika. Efficacy of CPP-ACP and CPP-ACPF on enamel remineralization-An in vitro study using scanning electron microscope and DIAGNOdent®. Indian J. Dent. Res. 2011, 22, 77–82. [Google Scholar] [CrossRef]
- Paris, S.; Meyer-Lueckel, H. Masking of labial enamel white spot lesions by resin infiltration-A clinical report. Quintessence Int. 2009, 40, 713–718. [Google Scholar]
- Saxena, P.; Grewal, M.; Agarwal, P.; Kaur, G.; Verma, J.; Chhikara, V. Clinical efficacy of resin infiltration technique alone or in combination with micro abrasion and in-office bleaching in adults with mild-to-moderate fluorosis stains. J. Pharm. Bioallied Sci. 2021, 13, S301–S305. [Google Scholar] [CrossRef]
- Guzmán-Armstrong, S.; Chalmers, J.; Warren, J.J. White spot lesions: Prevention and treatment. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 690–696. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
|
Author/
Year |
Study
Design |
Participants
(nr/age) | Intervention Time | Treatment Techniques in Study | Results | Conclusions |
|---|---|---|---|---|---|---|
| Mennatallah Atef Aboulnaga et al., 2022 [37] | RCT | 40 participants, aged 15–25 | 3 months | Remin Pro (SF—1450 ppm, hydroxyapatite, xylitol) and Remin Pro Forte (SF—1450 ppm, hydroxyapatite, xylitol, ginger extracts, and curcuma) | Both were effective, with Remind Pro Forte showing superior performance. | The combination of additional bioactive ingredients, including ginger extracts and curcuma, in Remin Pro Forte provides enhanced remineralization, making it more effective for managing WSLs. |
| Peter Rechmann et al., 2017 [42] | RCT | 40 participants, age range 11–26 years | 12 months | Experimental group: twice-daily fluoride toothpaste, daily MI Paste Plus MIPP), quarterly MI Varnish (MIV) application | No significant differences in enamel decalcification or caries detection (ICDAS) scores between experimental and control groups at 12 months. | Varnish did not significantly reduce the incidence of WSLs during fixed orthodontic treatment. However, they delivered fluoride effectively. |
| Grocholewicz et al., 2022 [34] | RCT | 150 patients, aged 16–50 years | 12 months | Fluoride varnish, ozone therapy, octenidine mouthrinse | Lower incidence of WSLs with combined treatment techniques. | Combination of fluoride varnish, ozone, and octenidine reduced WSLs compared to control group. |
| Rai et al., 2016 [35] | Split-mouth randomized study | 45 children, age range 7–15 years | 9 months | Resin infiltration with or without chlorhexidine varnish | Slower progression of caries in test group (resin infiltration + chlorhexidine varnish). | Resin infiltration with chlorhexidine varnish over resin infiltration alone, improving caries control in more advanced lesions (ICDAS 3). |
| Turska-Szybka et al., 2016 [43] | RCT | 81 children, 18–71 months | 1 year | Resin infiltration with fluoride varnish vs. fluoride varnish only | Significantly reduced progression of early caries lesions with resin infiltration. | Resin infiltration combined with fluoride varnish is more effective than fluoride varnish alone in arresting caries. |
| Heravi et al., 2018 [38] | RCT | 36 participants (13–23 years) | 12 weeks | MI Paste Plus (containing CPP-ACPF), Remin Pro (containing hydroxyapatite and fluoride), control | Significant reduction in WSL area, increased mineral content, and improved aesthetics for MI Paste Plus and Remin Pro groups. | The combination of CPP-ACP and fluoride in MI Paste Plus, and hydroxyapatite, fluoride, and xylitol in Remin Pro provide effective remineralization and improved aesthetics for WSLs. |
| Ebrahimi et al., 2017 [44] | RCT | 80 children (7–12 years) | 10 days | MI Paste Plus (containing CPP-ACPF), Remin Pro (containing hydroxyapatite and fluoride), 2% SF gel | All remineralizing agents significantly reduced the area and increased the mineral content of WSLs. The control group showed no significant improvement. | The combination of bioactive ingredients in MI Paste Plus and Remin Pro was as effective as 2% SF, making them suitable alternatives for managing WSLs in children. |
| Güçlü et al., 2016 [45] | RCT | 21 children (8–15 years) | 12 weeks | Application of 10% CPP-ACP paste and 5% SF varnish | CPP-ACP and its combination with fluoride varnish significantly improved visual appearance and remineralization of WSLs. Fluoride varnish alone showed no additional advantage. | Twice-daily application of CPP-ACP significantly improves WSLs’ appearance and mineralization, making it effective as a standalone treatment. |
| Study (Author, Year) | D1: | D2: | D3: | D4: | D5: | Overall Risk of Bias |
|---|---|---|---|---|---|---|
| Aboulnaga et al., 2022 [37] | 🟢 Low | 🟢 Low | 🟢 Low | 🟢 Low | 🟢 Low | 🟢 Low |
| Rechmann et al., 2017 [42] | 🟢 Low | 🟢 Low | 🟡 Some Concerns | 🟢 Low | 🟡 Some Concerns | 🟢 Low |
| Grocholewicz et al., 2022 [34] | 🟢 Low | 🟢 Low | 🟡 Some Concerns | 🟡 Some Concerns | 🟢 Low | 🟢 Low |
| Rai et al., 2016 [35] | 🟢 Low | 🟢 Low | 🟢 Low | 🟢 Low | 🟢 Low | 🟢 Low |
| Turska-Szybka et al., 2016 [43] | 🟢 Low | 🟢 Low | 🟢 Low | 🟡 Some Concerns | 🟡 Some Concerns | 🟢 Low |
| Heravi et al., 2018 [38] | 🟡 Some Concerns | 🟢 Low | 🟢 Low | 🟡 Some Concerns | 🟢 Low | 🟢 Low |
| Ebrahimi et al., 2017 [44] | 🟢 Low | 🟡 Some Concerns | 🟡 Some Concerns | 🟡 Some Concerns | 🟢 Low | 🟡 Some Concerns |
| Güçlü et al., 2016 [45] | 🟢 Low | 🟢 Low | 🟡 Some Concerns | 🟢 Low | 🟢 Low | 🟢 Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamorgese, M.; Veiga, N.; Correia, M.J.; Gomes, A.T.P.C.; Lopes, S.; Lopes-Rocha, L.; Fidalgo-Pereira, R.; Lopes, P.C. White Spot Lesion Treatment Options: A Systematic Review of Different Techniques for Masking These Lesions. Gels 2025, 11, 371. https://doi.org/10.3390/gels11050371
Lamorgese M, Veiga N, Correia MJ, Gomes ATPC, Lopes S, Lopes-Rocha L, Fidalgo-Pereira R, Lopes PC. White Spot Lesion Treatment Options: A Systematic Review of Different Techniques for Masking These Lesions. Gels. 2025; 11(5):371. https://doi.org/10.3390/gels11050371
Chicago/Turabian StyleLamorgese, Michela, Nélio Veiga, Maria J. Correia, Ana T. P. C. Gomes, Sara Lopes, Lígia Lopes-Rocha, Rita Fidalgo-Pereira, and Pedro C. Lopes. 2025. "White Spot Lesion Treatment Options: A Systematic Review of Different Techniques for Masking These Lesions" Gels 11, no. 5: 371. https://doi.org/10.3390/gels11050371
APA StyleLamorgese, M., Veiga, N., Correia, M. J., Gomes, A. T. P. C., Lopes, S., Lopes-Rocha, L., Fidalgo-Pereira, R., & Lopes, P. C. (2025). White Spot Lesion Treatment Options: A Systematic Review of Different Techniques for Masking These Lesions. Gels, 11(5), 371. https://doi.org/10.3390/gels11050371