
Applications of Reflectance Confocal Microscopy in the Diagnosis of Fungal Infections: A Systematic Review

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
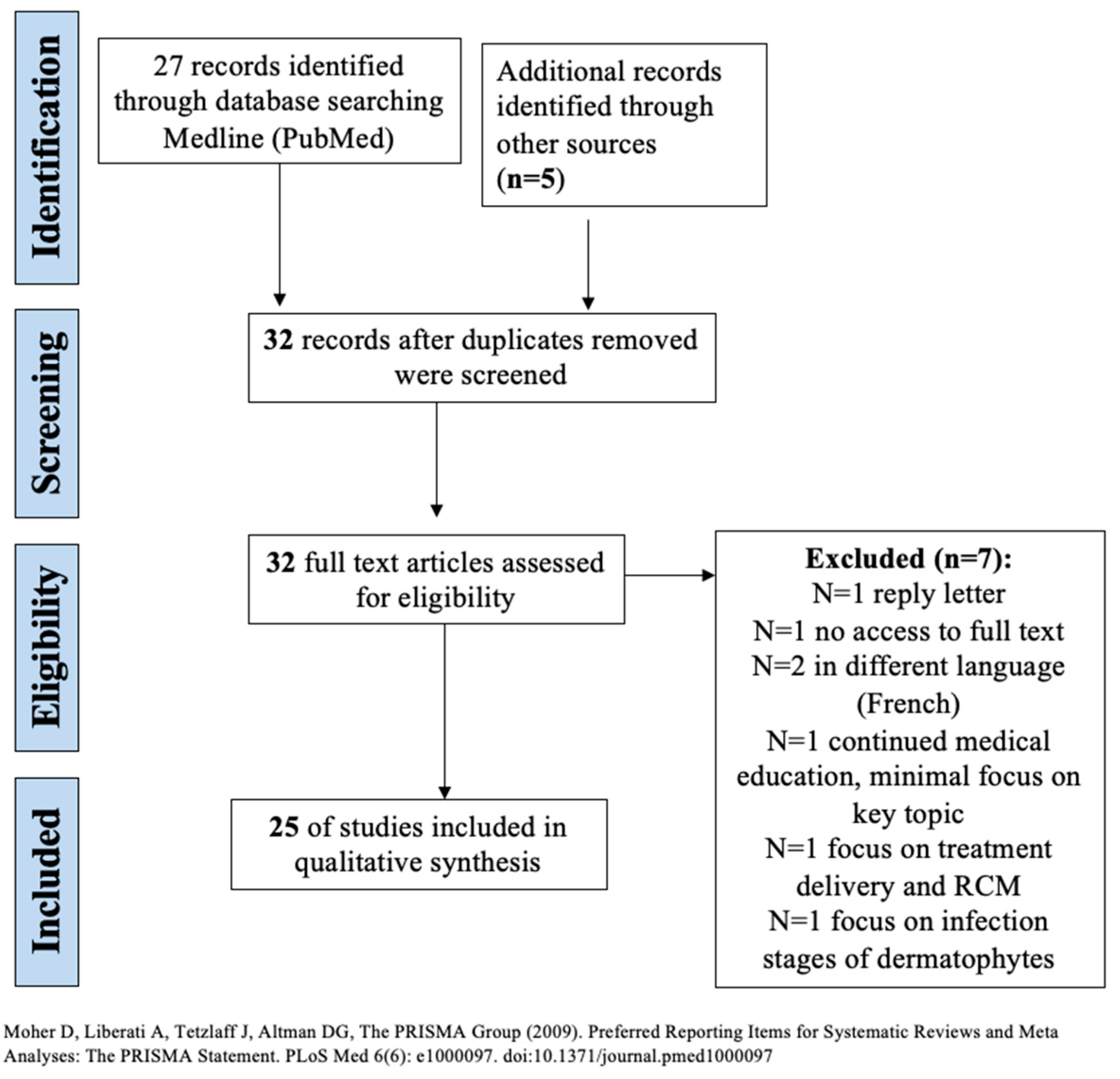
2.2. Information Sources, Search, and Study Selection
2.3. Data Collection and Extraction Process
2.4. Quality Assessment
3. Results
3.1. Visualization and Descriptions of Common Fungal Infections by RCM
3.2. Ex-Vivo RCM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cantelli, M.; Capasso, G.; Costanzo, L.; Fabbrocini, G.; Gallo, L. Tinea pedis in a child: How reflectance confocal microscopy can help in diagnosis of dermatophytosis. Pediatr. Dermatol. 2020, 38, 522–523. [Google Scholar] [CrossRef] [PubMed]
- Levitt, J.O.; Levitt, B.H.; Akhavan, A.; Yanofsky, H. The Sensitivity and Specificity of Potassium Hydroxide Smear and Fungal Culture Relative to Clinical Assessment in the Evaluation of Tinea Pedis: A Pooled Analysis. Dermatol. Res. Pr. 2010, 2010, 764843. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Xu, A.; Ai-e, X. Evaluation of reflectance confocal microscopy in dermatophytosis. Mycoses 2012, 56, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Pharaon, M.; Gari-Toussaint, M.; Khemis, A.; Zorzi, K.; Petit, L.; Martel, P.; Baran, R.; Ortonne, J.P.; Passeron, T.; Lacour, J.P.; et al. Diagnosis and treatment monitoring of toenail onychomycosis by reflectance confocal microscopy: Prospective cohort study in 58 patients. J. Am. Acad. Dermatol. 2014, 71, 56–61. [Google Scholar] [CrossRef]
- Rothmund, G.; Sattler, E.C.; Kaestle, R.; Fischer, C.; Haas, C.J.; Starz, H.; Welzel, J. Confocal laser scanning microscopy as a new valuable tool in the diagnosis of onychomycosis-comparison of six diagnostic methods. Mycoses 2012, 56, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Slutsky, J.B.; Rabinovitz, H.; Grichnik, J.M.; Marghoob, A.A. Reflectance confocal microscopic features of dermatophytes, scabies, and demodex. Arch. Dermatol. 2011, 147, 1008. [Google Scholar] [CrossRef]
- Liansheng, Z.; Zhiping, W.; Yanqun, L.; Xin, J.; Cheng, Q. Diagnostic applicability of confocal laser scanning microscopy in tinea corporis. Int. J. Dermatol. 2013, 52, 1281–1282. [Google Scholar] [CrossRef]
- Turan, E.; Erdemir, A.T.; Gurel, M.S.; Yurt, N. A new diagnostic technique for tinea incognito: In vivo reflectance confocal microscopy. Report of five cases. Ski. Res. Technol. 2013, 19, e103–e107. [Google Scholar] [CrossRef]
- Cinotti, E.; Perrot, J.L.; Labeille, B.; Moragues, A.; Raberin, H.; Flori, P.; Cambazard, F.; Groupe Imagerie Cutanée Non Invasive de la Société Française de Dermatologie. Tinea corporis diagnosed by reflectance confocal microscopy. Ann. Dermatol. Venereol. 2014, 141, 150–152. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, E.; Fouilloux, B.; Perrot, J.L.; Labeille, B.; Douchet, C.; Cambazard, F. Confocal microscopy for healthy and pathological nail. J. Eur. Acad. Dermatol. Venereol. 2013, 28, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Mateus, R.; Murzaku, E.C.; Rao, B.K. Atypical pigmented acral lesion proven to be fungal using reflectance confocal microscopy. J. Am. Acad. Dermatol. 2014, 70, e77–e79. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.; Friedman, P.C.; Gill, M. Reflectance confocal microscopy: An effective diagnostic tool for dermatophytic infections. Cutis 2015, 95, 93–97. [Google Scholar] [PubMed]
- Hoogedoorn, L.; Peppelman, M.; Van De Kerkhof, P.C.M.; Van Erp, P.E.J.; Gerritsen, M.J.P. The value of in vivo reflectance confocal microscopy in the diagnosis and monitoring of inflammatory and infectious skin diseases: A systematic review. Br. J. Dermatol. 2015, 172, 1222–1248. [Google Scholar] [CrossRef] [PubMed]
- Navarrete-Dechent, C.; Bajaj, S.; Marghoob, A.A.; Marchetti, M.A. Rapid diagnosis of tinea incognito using handheld reflectance confocal microscopy: A paradigm shift in dermatology? Mycoses 2015, 58, 383–386. [Google Scholar] [CrossRef]
- Leclercq, A.; Cinotti, E.; Labeille, B.; Perrot, J.L.; Cambazard, F. Ex vivo confocal microscopy: A new diagnostic technique for mucormycosis. Skin Res. Technol. 2016, 22, 203–207. [Google Scholar] [CrossRef]
- Uva, L.; Leal-Filipe, P.; Soares-De-Almeida, L.; Ferreira, J.; Oliveira, A. Reflectance confocal microscopy for the diagnosis of tinea nigra. Clin. Exp. Dermatol. 2017, 43, 332–334. [Google Scholar] [CrossRef]
- Veasey, J.V.; Meneses, O.M.S.; Da Silva, F.O. Reflectance confocal microscopy of tinea capitis: Comparing images with results of dermoscopy and mycological exams. Int. J. Dermatol. 2018, 58, 849–851. [Google Scholar] [CrossRef]
- Pimenta, R.; Soares-De-Almeida, L.; Arzberger, E.; Ferreira, J.; Leal-Filipe, P.; Bastos, P.M.; Oliveira, A.L. Reflectance confocal microscopy for the diagnosis of skin infections and infestations. Dermatol. Online J. 2020, 26, 13030. [Google Scholar] [CrossRef]
- Lim, S.S.; Ohn, J.; Mun, J.H. Diagnosis of Onychomycosis: From Conventional Techniques and Dermoscopy to Artificial Intelligence. Front. Med. 2021, 8, 637216. [Google Scholar] [CrossRef]
- Potestio, L.; Villani, A.; Ocampo-Garza, S.S.; Evangelista, E.; De Lucia, M.; Costanzo, L.; Camela, E.; Fabbrocini, G.; Gallo, L. Dermatophytid evaluated by in vivo reflectance confocal microscopy: A new approach? Int. J. Dermatol. 2022, 61, e394–e396. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, V.; Di Brizzi, E.V.; Russo, T.; Moscarella, E.; Diniz, T.; Alfano, R.; Argenziano, G. Majocchi’s granuloma on the face: Dermoscopy and reflectance confocal microscopy. Int. J. Dermatol. 2019, 58, e180–e182. [Google Scholar] [CrossRef]
- Liu, Z.H.; Xia, X.J.; Zhang, Y.; Zhong, Y.; Sang, B.; Li, Q.P.; Wang, M.; Lv, W.W.; Zhi, H.L.; Wang, X.D.; et al. Favus of Scrotum Due to Trichophyton rubrum in Immunocompetent Patients: A Clinical, Mycological and Ultrastructural Study. Mycopathologia 2019, 184, 433–439. [Google Scholar] [CrossRef]
- Cheng, H.M.; Thng, S.T.G.; Tan, W.P.; Chuah, S.Y. Handheld reflectance confocal microscopy: A useful tool to aid diagnosis of acral pigmented lesions. J. Dermatol. 2016, 43, 980–981. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, E.; Perrot, J.; Labeille, B.; Raberin, H.; Flori, P.; Cambazard, F. Hair dermatophytosis diagnosed by reflectance confocal microscopy: Six cases. J. Eur. Acad. Dermatol. Venereol. 2014, 29, 2257–2259. [Google Scholar] [CrossRef] [PubMed]
- Hongcharu, W.; Dwyer, P.; Gonzalez, S.; Anderson, R. Confirmation of onychomycosis by in vivo confocal microscopy. J. Am. Acad. Dermatol. 2000, 42, 214–216. [Google Scholar] [CrossRef]
- Markus, R.; Huzaira, M.; Anderson, R.R.; González, S. A better potassium hydroxide preparation? In vivo diagnosis of tinea with confocal microscopy. Arch. Dermatol. 2001, 137, 1076–1078. [Google Scholar]


{kind=link}
| Study | Risk of Bias | Applicability Concerns | |||||
|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | |
| Hui et al. [5] | Low | Low | Unclear | Low | Low | Low | Unclear |
| Pharaon et al. [6] | Low | Low | Unclear | Low | Low | Low | Unclear |
| Rothmund et al. [7] | Low | Low | Low | Low | Low | Low | Low |
| Study | Year Published | Study Type | # of Patients | Diagnosis | Fungal Description (Adapted) |
|---|---|---|---|---|---|
| Slutsky et al. [8] | 2011 | Review | N/A | Tinea | Branching fungal hyphae |
| Hui et al. [5] | 2013 | Prospective cohort study | 45 | Tinea manus, pedis, cruris | Hyphae: bright linear branching structures not found in uninvolved skin Mycelium: a variable number of bright linear structures distributed in the stratum corneum Blister: round-low refractive of the structure located in the stratum corneum or acanthosis and inflammatory infiltrate: higher refractive polymorphonuclear cell populations, accompanied by light flashes, located in the stratum corneum or the upper layer of acanthosis |
| Liansheng et al. [9] | 2013 | Review | N/A | Tinea corporis | Highly refractile, septate, linear structures |
| Turan et al. [10] | 2013 | Case series | 5 | Tinea incognito | Hyphae: bright, thin, linear, and branched structures at stratum corneum Aggregation of bright, small structures resembling inflammatory cells |
| Cinotti et al. [11] | 2014 | Case Report | 1 | Tinea corporis | Bright, thin, linear, and branched structures |
| Cinotti et al. [12] | 2014 | Review | N/A | Onychomycosis | Lengthy structures with high reflection and the typical shape of hyphae |
| Mateus et al. [13] | 2014 | Case Report | 1 | Tinea pedis | Hyphae: Numerous linear bright structures |
| Pharaon et al. [6] | 2014 | Prospective Cohort Study | 58 | Onychomycosis | Presence of filamentous and/or roundish structures in the nail plate, corresponding respectively to septate hyphae and/or arthroconidia |
| Friedman et al. [14] | 2015 | Case Series | 5 | Tinea | Branching hyphae in the epidermis |
| Hoogedoorn et al. [15] | 2015 | Review | N/A | Tinea incognito, tinea corposis, onychomycosis | Branched hyphae network |
| Navarete-Dechent et al. [16] | 2015 | Case Report | 1 | Tinea Incognito | Hyphae: refractive linear septate branching structures |
| Leclercq et al. [17] | 2016 | Case Series | 2 | Mucormycosis | Hyper-reflective elongated 20μm in diameter structures with perpendicular ramifications. |
| Uva et al. [18] | 2018 | Case Report | 1 | Tinea Nigra | Linear structures with high reflectivity and speckled appearance. Tortuous, irregular, and short hyphae structures, unlike thin and elongated dermatophytes. |
| Veasey et al. [19] | 2019 | Case Report | 1 | Tinea Capitis | Hyperreflectivity of structures with speckled appearance, as well as tortuous structures on the outside of hair |
| Pimenta et al. [20] | 2020 | Review | N/A | Tinea Candida Malassezia | Hyphae can be easily identified as bright, linear, branching and filamentous structures, whereas conidia appear as hyper-reflective small roundish bodies. Hyphae should be differentiated from the cell membranes of keratinocytes and from the normal structure of hair shafts. Candida is visualized with pseudo filaments and conidia in the skin, nails, and oral mucosa Malassezia appears as clusters of roundish bright structures with tortuous hyper- reflective structures corresponding to thick and short septa analogues of the typical spaghetti and meatballs description. |
| Cantelli et al. [1] | 2021 | Case Report | 1 | Tinea pedis | bright linear structures in the stratum corneum inflammatory infiltrate: high refractive polymorphonuclear clear clear cell populations, accompanied by light flashes in the epidermis |
| Lim et al. [21] | 2021 | Review | N/A | Onychomycosis | networks of bright filamentous septate hyphae |
| Potestio et al. [22] | 2022 | Case Report | 1 | Dermatophytid | several bright linear structures (mycelium) as well as inflammatory cells in the stratum corneum and in perivascular zones, as well as spongiosis. |
| Piccolo et al. [23] | 2019 | Letter | 1 | Majocchi granuloma | perifollicular inflammation, no hyphae |
| Ze-Hu Liu [24] | 2019 | Prospective study | 10 | Tinea favosa of the scrotum | septate branching hyphae |
| Cheng et al. [25] | 2016 | Letter/Case report | 1 | Tinea nigra | multiple, refractive, linear, filamentous structures at the stratum corneum |
| Cinotti et al. [26] | 2014 | Letter/Case Series | 6 | 4: tinea capitis 2: tinea barbae | roundish homogeneous (5–10 μm in size) hyper-reflective structures corresponding to conidia around the proximal part of the hair shaft sparse elongated hyper-reflective structures outside the hair shafts, corresponding to hyphae |
| Rothmund et al. [7] | 2012 | Comparative study | 60 | Onychomycosis | white lengthy or thready structures with high reflection and typical shape or spore-like bright aggregates |
| Hongcharu et al. [27] | 2000 | Case report | 1 | Onychomycosis | branched hyphae |
| Markus et al. [28] | 2001 | Case report | 1 | Onychomycosis | several linear hyphae in intercellular spaces in the upper epidermis; highly refractile, linear structures that were brighter than the background keratinized cells |
| Clinical/Microbiological Diagnosis | RCM Description |
|---|---|
| Tinea, unspecified [8,14,20] | bright [20], linear [20], branching [8,20], filamentous [20] fungal hyphae [8] in the epidermis [14], whereas conidia appear as hyper-reflective small roundish bodies [20] |
| Tinea manus [5] | bright linear branching structures not found in uninvolved skin (hyphae) with a variable number of bright linear structures distributed in the stratum corneum (mycelium) [5] |
| Tinea pedis [1,5,13] | bright [1,5,13], branching structures [1,5,13] not found in uninvolved skin (hyphae) with a variable number of bright linear structures distributed in the stratum corneum [1] (mycelium) [5]; inflammatory infiltrate: high refractive polymorphonuclear clear clear cell populations, accompanied by light flashes in the epidermis [1] |
| Tinea cruris [5] | bright linear branching structures not found in uninvolved skin (hyphae) with a variable number of bright linear structures distributed in the stratum corneum (mycelium) [5] |
| Tinea corporis [9,11] | bright [11], thin [11], branched [11], highly refractile [9], septate [9], linear structures [9,11] |
| Tinea incognito [10,16] | bright/refractive, linear, branching [10,16] thin structures at stratum corneum (hyphae) with aggregation of bright, small structures resembling inflammatory cells [10] |
| Onychomycosis [6,7,12,21,27,28] | several [28], bright [28], white [7], high reflective [7,12,21], lengthy [7,12], linear [28] or thready [7] or filamentous [6,21] structures in intercellular spaces in the upper epidermis [24] of the nail plate corresponding to septate hyphae [6,12,21]; spore-like, bright [7] roundish aggregates in the nail plate corresponding to arthroconidia [6] |
| Mucormycosis [17] | hyper-reflective elongated 20μm in diameter structures with perpendicular ramifications [17] |
| Tinea Nigra [18,25] | multiple [25], linear, filamentous structures with high reflectivity [18,25] and speckled appearance at the stratum corneum; tortuous, irregular, and short hyphae structures, unlike thin and elongated dermatophytes [18] |
| Tinea capitis [19,26] | roundish [26], homogeneous (5–10 μm in size) hyper-reflective [26] structures with speckled appearance [19] corresponding to conidia around the proximal part of the hair shaft [26]; sparse, elongated, hyper-reflective [26] tortuous structures outside of hair shafts, corresponding to hyphae [19] |
| Candida [20] | pseudo filaments and conidia in the skin, nails, and oral mucosa [20] |
| Malassezia [20] | clusters of roundish bright structures with tortuous hyper- reflective structures corresponding to thick and short septa analogues of the typical spaghetti and meatballs description [20] |
| Dermatophytid [22] | several bright linear structures (mycelium) as well as inflammatory cells in the stratum corneum and in perivascular zones, as well as spongiosis [22] |
| Majocchi Granuloma [23] | perifollicular inflammation, no hyphae [23] |
| Tinea favosa of the scrotum [15] | septate branching hyphae [15] |
| Tinea barbae [26] | roundish homogeneous (5–10 μm in size) hyper-reflective structures corresponding to conidia around the proximal part of the hair shaft [26] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, S.; Farabi, B.; Navarrete-Dechent, C.; Rao, B.; Safai, B. Applications of Reflectance Confocal Microscopy in the Diagnosis of Fungal Infections: A Systematic Review. J. Fungi 2023, 9, 39. https://doi.org/10.3390/jof9010039
Khan S, Farabi B, Navarrete-Dechent C, Rao B, Safai B. Applications of Reflectance Confocal Microscopy in the Diagnosis of Fungal Infections: A Systematic Review. Journal of Fungi. 2023; 9(1):39. https://doi.org/10.3390/jof9010039
Chicago/Turabian StyleKhan, Samavia, Banu Farabi, Cristian Navarrete-Dechent, Babar Rao, and Bijan Safai. 2023. "Applications of Reflectance Confocal Microscopy in the Diagnosis of Fungal Infections: A Systematic Review" Journal of Fungi 9, no. 1: 39. https://doi.org/10.3390/jof9010039
APA StyleKhan, S., Farabi, B., Navarrete-Dechent, C., Rao, B., & Safai, B. (2023). Applications of Reflectance Confocal Microscopy in the Diagnosis of Fungal Infections: A Systematic Review. Journal of Fungi, 9(1), 39. https://doi.org/10.3390/jof9010039