
Fungal Infections in the ICU during the COVID-19 Era: Descriptive and Comparative Analysis of 178 Patients

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Fungal Infection Patients’ Characteristics
3.2. COVID-19 Associated Candidemia
3.3. COVID-19 Associated Pulmonary Aspergillosis
3.4. Risk Factor Differences
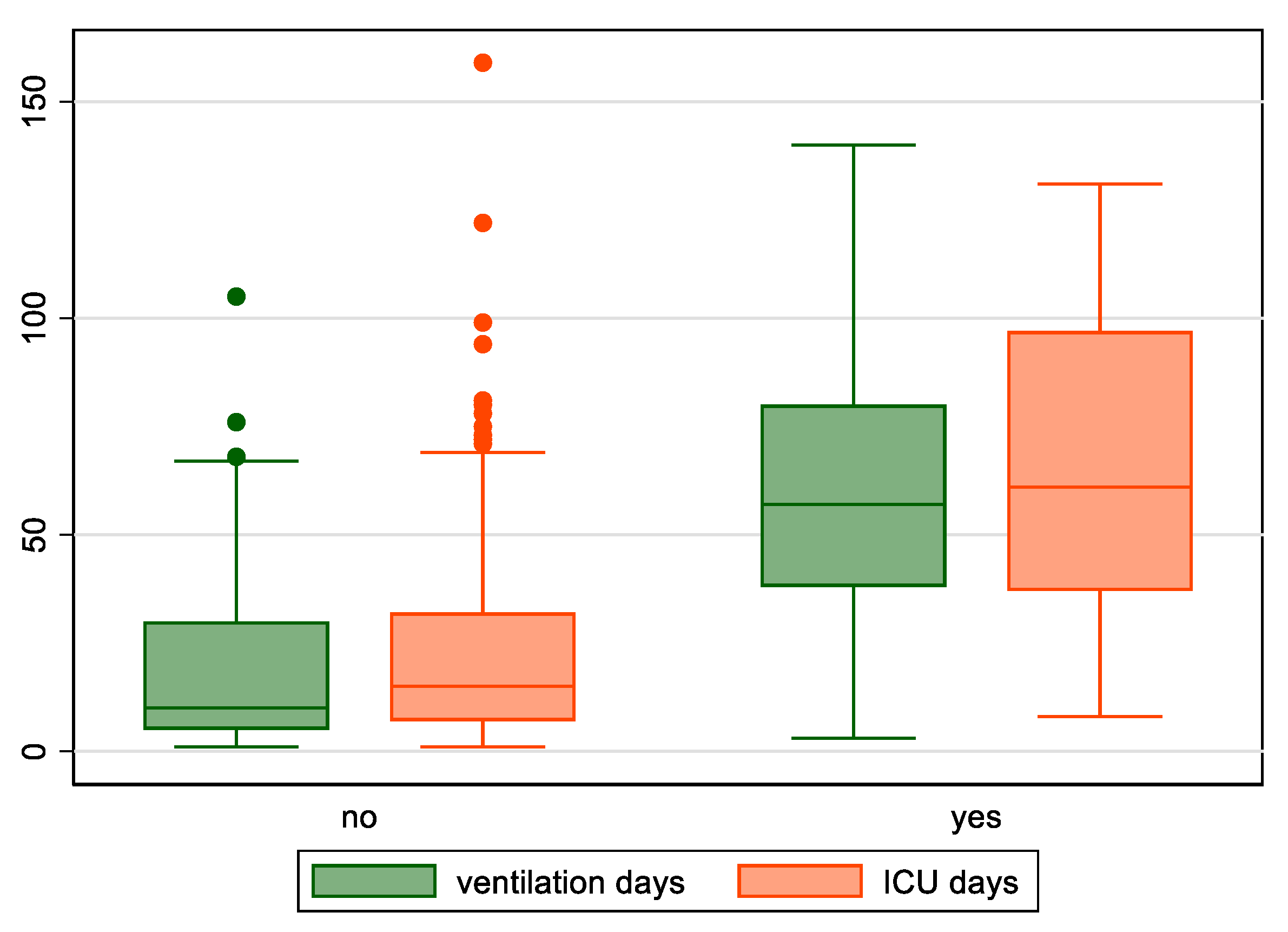
3.5. Outcome Differences
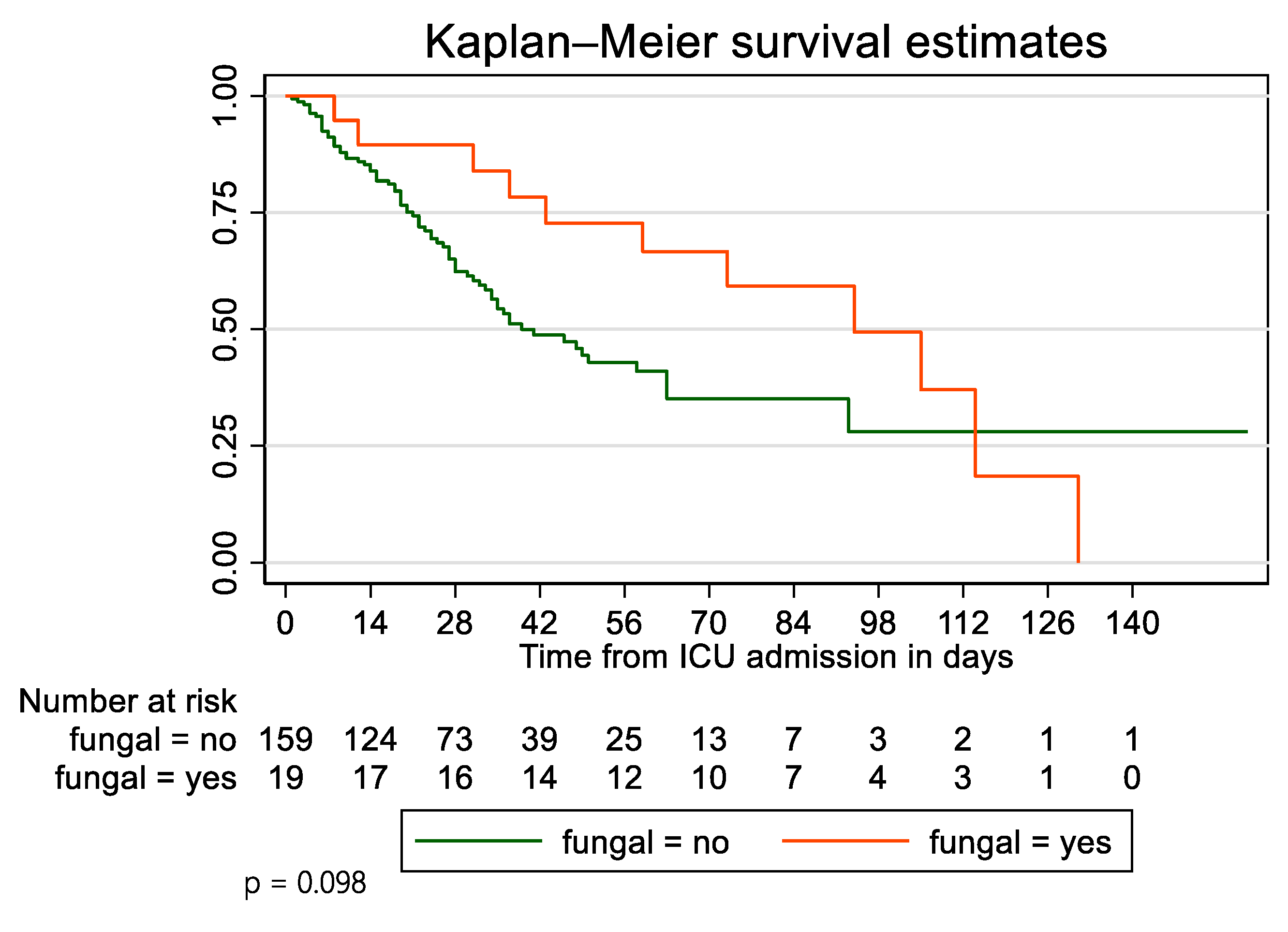
3.6. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carbonell, R.; Urgelés, S.; Rodríguez, A.; Bodí, M.; Martín-Loeches, I.; Solé-Violán, J.; Díaz, E.; Gómez, J.; Trefler, S.; Vallverdú, M.; et al. Mortality comparison between the first and second/third waves among 3795 critical COVID-19 patients with pneumonia admitted to the ICU: A multicentre retrospective cohort study. Lancet Reg. Health Eur. 2021, 11, 100243. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Cattaneo, E.; Florio, G.; Ippolito, M.; Zanella, A.; Cortegiani, A.; Huang, J.; Pesenti, A.; Einav, S. Mechanical ventilation parameters in critically ill COVID-19 patients: A scoping review. Crit. Care. 2021, 25, 115. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, Y.; Wu, J.; Li, Y.; Zhou, X.; Li, X.; Chen, H.; Guo, M.; Chen, S.; Sun, F.; et al. Risks and features of secondary infections in severe and critical ill COVID-19 patients. Emerg. Microbes Infect. 2020, 9, 1958–1964. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Cornely, O.A.; Böttiger, B.W.; Dusse, F.; Eichenauer, D.A.; Fuchs, F.; Hallek, M.; Jung, N.; Persigehl, F.K.T.; Rybniker , J.; et al. COVID-19 associated pulmonary aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [CrossRef] [PubMed]
- van Arkel, A.L.E.; Rijpstra, T.A.; Belderbos, H.N.A.; van Wijngaarden, P.; Verweij, P.E.; Bentvelsen, R.G. COVID-19-associated Pulmonary Aspergillosis. Am. J. Respir. Crit. Care Med. 2020, 202, 132–135. [Google Scholar] [CrossRef]
- Alanio, A.; Dellière, S.; Fodil, S.; Bretagne, S.; Mégarbane, B. Prevalence of putative invasive pulmonary aspergillosis in critically ill patients with COVID-19. Lancet Respir. Med. 2020, 8, e48–e49. [Google Scholar] [CrossRef]
- Rutsaert, L.; Steinfort, N.; Van Hunsel, T.; Bomans, P.; Naesens, R.; Mertes, H.; Dits, H.; van Regenmortel, N. COVID-19-associated invasive pulmonary aspergillosis. Ann. Intensive Care 2020, 10, 71. [Google Scholar] [CrossRef]
- Bartoletti, M.; Pascale, R.; Cricca, M.; Rinaldi, M.; Maccaro, A.; Bussini, L.; Fornaro, G.; Tonetti, T.; Pizzilli, G.; Francalanci, E.; et al. Epidemiology of Invasive Pulmonary Aspergillosis Among Intubated Patients With COVID-19: A Prospective Study. Clin. Infect Dis. 2021, 73, e3606–e3614. [Google Scholar] [CrossRef]
- Machado, M.; Valerio, M.; Álvarez-Uría, A.; Olmedo, M.; Veintimilla, C.; Padilla, B.; de la Villa, S.; Guinea, J.; Escribano, P.; Ruiz-Serrano, M.J.; et al. Invasive pulmonary aspergillosis in the COVID-19 era: An expected new entity. Mycoses 2021, 64, 132–143. [Google Scholar] [CrossRef]
- Blaize, M.; Raoelina, A.; Kornblum, D.; Kamus, L.; Lampros, A.; Berger, M.; Demeret, S.; Constantin, J.; Monsel, A.; Mayaux, J.; et al. Occurrence of Candidemia in Patients with COVID-19 Admitted to Five ICUs in France. J. Fungi 2022, 8, 678. [Google Scholar] [CrossRef]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Gangneux, J.P.; Dannaoui, E.; Fekkar, A.; Luyt, C.E.; Botterel, F.; De Prost, N.; Tadié, J.; Reizine, F.; Houzé, S.; Timsit, J.; et al. Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: The French multicentre MYCOVID study. Lancet Respir. Med. 2022, 10, 180–190. [Google Scholar] [CrossRef]
- Kayaaslan, B.; Eser, F.; Kaya Kalem, A.; Bilgic, Z.; Asilturk, D.; Hasanoglu, I.; Ayhan, M.; Tekce, Y.T.; Erdem, D.; Turan, S.; et al. Characteristics of candidemia in COVID-19 patients; increased incidence, earlier occurrence and higher mortality rates compared to non-COVID-19 patients. Mycoses 2021, 64, 1083–1091. [Google Scholar] [CrossRef] [PubMed]
- Rovina, N.; Koukaki, E.; Romanou, V.; Ampelioti, S.; Loverdos, K.; Chantziara, V.; Koutsoukou, A.; Dimopoulos, G. Fungal Infections in Critically Ill COVID-19 Patients: Inevitabile Malum. J. Clin. Med. 2022, 11, 2017. [Google Scholar] [CrossRef]
- Prattes, J.; Wauters, J.; Giacobbe, D.R.; Salmanton-García, J.; Maertens, J.; Bourgeois, M.; Reynders, M.; Rutsaert, L.; van Regenmortel, N.; Lormans, P.; et al. Risk factors and outcome of pulmonary aspergillosis in critically ill coronavirus disease 2019 patients-a multinational observational study by the European Confederation of Medical Mycology. Clin. Microbiol. Infect. 2022, 28, 580–587. [Google Scholar] [CrossRef]
- Verweij, P.E.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Buil, J.B.; Calandra, T.; Chiller, T.; Clancy, C.J.; Cornely, O.A.; et al. Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensive Care Med. 2021, 47, 819–834. [Google Scholar] [CrossRef]
- Dellière, S.; Dudoignon, E.; Fodil, S.; Voicu, S.; Collet, M.; Oillic, P.A.; Salmona, M.; Dépret, F.; Ghelfenstein-Ferreira, T.; Plaud, B.; et al. Risk factors associated with COVID-19-associated pulmonary aspergillosis in ICU patients: A French multicentric retrospective cohort. Clin. Microbiol. Infect. 2020, 27, 790.e1–790.e5. [Google Scholar] [CrossRef]
- Ergün, M.; Brüggemann, R.J.M.; Alanio, A.; Dellière, S.; van Arkel, A.; Bentvelsen, R.G.; Rijpstra, T.; der Brugge, S.va.; Lagrou, K.; Janssen, N.A.F.; et al. Aspergillus Test Profiles and Mortality in Critically Ill COVID-19 Patients. J. Clin. Microbiol. 2021, 59, e0122921. [Google Scholar] [CrossRef]
- Permpalung, N.; Chiang, T.P.; Massie, A.B.; Zhang, S.X.; Avery, R.K.; Nematollahi, S.; Ostrander, D.; Segev, D.L.; Marr, K.A. Coronavirus Disease 2019-Associated Pulmonary Aspergillosis in Mechanically Ventilated Patients. Clin. Infect Dis. 2022, 74, 83–91. [Google Scholar] [CrossRef]
- Avkan-Oğuz, V.; Çelİk, M.; Eren-Kutsoylu, O.Ö.; Nazli, A.; Uğur, Y.L.; Taylan, A.; Ergan, B.; Irmak, Ç.; Duğral, E.; Özkütük, A.A. Fungal colonization and infections in patients with COVID-19 in intensive care units: A real-life experience at a tertiary-care hospital. Respir. Med. Res. 2022, 82, 100937. [Google Scholar] [CrossRef]
- Bell, J.; Heyer, N.; Greenstein, A.; Fragkos, K.; Baxter-Derrington, C.; Mehta, S. A retrospective analysis of malnutrition risk, nutritional support and outcomes in COVID-19 patients. Clin. Nutr. ESPEN 2022, 50, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, P.; Varpaei, H.A.; Khafaee Pour Khamseh, A.; Mohammadi, M.; Rahimi, M.; Orandi, A. Evaluation of the Relationship between Nutritional Status of COVID-19 Patients Admitted to the ICU and Patients’ Prognosis: A Cohort Study. J. Nutr. Metab. 2022, 2022, 5016649. [Google Scholar] [CrossRef] [PubMed]
- Shabanpur, M.; Pourmahmoudi, A.; Nicolau, J.; Veronese, N.; Roustaei, N.; Jahromi, A.J.; Hosseinikia, M. The importance of nutritional status on clinical outcomes among both ICU and Non-ICU patients with COVID-19. Clin. Nutr. ESPEN 2022, 49, 225–231. [Google Scholar] [CrossRef] [PubMed]
- White, P.L.; Dhillon, R.; Cordey, A.; Hughes, H.; Faggian, F.; Soni, S.; Pandey, M.; Whitaker, H.; May, A.; Morgan, M.; et al. A National Strategy to Diagnose Coronavirus Disease 2019-Associated Invasive Fungal Disease in the Intensive Care Unit. Clin Infect Dis. 2021, 73, e1634–e1644. [Google Scholar] [CrossRef] [PubMed]
- Meijer, E.F.J.; Dofferhoff, A.S.M.; Hoiting, O.; Meis, J.F. COVID-19-associated pulmonary aspergillosis: A prospective single-center dual case series. Mycoses 2021, 64, 457–464. [Google Scholar] [CrossRef]
- Dimopoulos, G.; Almyroudi, M.P.; Myrianthefs, P.; Rello, J. COVID-19-Associated Pulmonary Aspergillosis (CAPA). J. Intensive Med. 2020, 6, 91. [Google Scholar] [CrossRef]
- Prattes, J.; Wauters, J.; Giacobbe, D.R.; Lagrou, K.; Hoenigl, M. ECMM-CAPA Study Group. Diagnosis and treatment of COVID-19 associated pulmonary aspergillosis in critically ill patients: Results from a European confederation of medical mycology registry. Intensive Care Med. 2021, 47, 1158–1160. [Google Scholar] [CrossRef]
- Santacroce, L.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Luperto, P.; De Nitto, E.; Topi, S. The Human Respiratory System and its Microbiome at a Glimpse. Biology 2020, 9, 318. [Google Scholar] [CrossRef]
- Kullberg, R.F.J.; de Brabander, J.; Boers, L.S.; Biemond, J.J.; Nossent, E.J.; Heunks, L.M.A.; Vlaar, A.P.J.; Bonta, P.I.; van der Poll, T.; Duitman, J.; et al. Lung Microbiota of Critically Ill COVID-19 Patients are Associated with Non-Resolving Acute Respiratory Distress Syndrome. Am. J. Respir. Crit Care Med. 2022; online ahead of print. [Google Scholar] [CrossRef]
- McGuinness, G.; Zhan, C.; Rosenberg, N.; Azour, L.; Wickstrom, M.; Mason, D.M.; Thomas, K.M.; Moore, W.H. Increased Incidence of Barotrauma in Patients with COVID-19 on Invasive Mechanical Ventilation. Radiology 2020, 297, E252–E262. [Google Scholar] [CrossRef]
- Udi, J.; Lang, C.N.; Zotzmann, V.; Krueger, K.; Fluegler, A.; Bamberg, F.; Bode, C.; Duerschmied, D.; Wengenmayer, T.; Staudacher, D.L. Incidence of Barotrauma in Patients With COVID-19 Pneumonia During Prolonged Invasive Mechanical Ventilation—A Case-Control Study. J. Intensive Care Med. 2021, 36, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Alhumaid, S.; Al Mutair, A.; Alghazal, H.A.; Alhaddad, A.J.; Al-Helal, H.; Al Salman, S.A.; Alali, J.; Almahmoud, S.; Alhejy, Z.M.; Albagshi, A.A.; et al. Extracorporeal membrane oxygenation support for SARS-CoV-2: A multi-centered, prospective, observational study in critically ill 92 patients in Saudi Arabia. Eur. J. Med. Res. 2021, 26, 141. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Characteristics | Total (n = 178) | Fungal Infection | p-Value | ||
|---|---|---|---|---|---|
| No | Yes | ||||
| Age (median, IQR) | 66 (55–73) | 66 (57–74) | 52 (43–70) | 0.008 | |
| Gender (n, %) | Male | 131 (73.6) | 117 (73.6) | 14 (73.7) | 0.99 |
| Female | 47 (26.4) | 42 (26.4) | 5 (26.3) | ||
| BMI (median, IQR) | 29 (26–33.9) | 29.3 (26–34) | 27.3 (25.7–31.2) | 0.24 | |
| Smoking habit (n, %) | Never | 105 (59) | 93 (58.5) | 12 (63.2) | 0.65 |
| Current | 22 (12.4) | 19 (12) | 3 (15.8) | ||
| Former | 51 (28.6) | 47 (29.5) | 4 (21) | ||
| Charlson Comorbidity Index (median, IQR) | 3 (1–4) | 3 (1–4) | 1 (0–3) | 0.016 | |
| Respiratory disease (n, %) | 29 (16.3) | 26 (16.4) | 3 (15.8) | >0.99 | |
| Diabetes (n, %) | 44 (24.7) | 42 (26.4) | 2 (10.5) | 0.17 | |
| Hypertension (n, %) | 88 (49.4) | 81 (50.9) | 7 (36.8) | 0.25 | |
| Thyroid disease (n, %) | 21 (11.8) | 18 (11.3) | 3 (15.8) | 0.47 | |
| Chronic Heart Disease (n, %) | 25 (14) | 25 (15.7) | 0 (0) | 0.079 | |
| Stroke (n, %) | 3 (1.7) | 2 (1.3) | 1 (5.3) | 0.29 | |
| Asthma (n, %) | 10 (5.6) | 9 (5.7) | 1 (5.3) | >0.99 | |
| Dyslipidemia (n, %) | 44 (24.7) | 39 (24.5) | 5 (26.3) | 0.86 | |
| COPD (n, %) | 15 (8.4) | 14 (8.8) | 1 (5.3) | >0.99 | |
| SAPS III (median, IQR) | 50 (45–55) | 50 (45–55) | 47 (41–53) | 0.11 | |
| APACHE II (median, IQR) | 12 (10–17) | 12 (10–17) | 13 (8–15) | 0.41 | |
| SOFA (median, IQR) | 6 (3–7) | 6 (3–7) | 6 (2–7) | 0.56 | |
| Arrived Intubated (n, %) | 135 (75.8) | 124 (78) | 11 (57.9) | 0.053 | |
| Intubation in the ICU (n, %) | 43 (24.2) | 35 (22) | 8 (42.1) | ||
| PF ratio day 1 (median, IQR) | 109 (78.3–149.5) | 110.9 (80–152) | 84 (63–129.1) | 0.013 | |
| PF ratio day 4 (median, IQR) | 141.7 (102.8–184) | 144.5 (106.3–184) | 117.8 (83.2–164.6) | 0.08 | |
| PF ratio day 7 (median, IQR) | 128.3 (97.1–173) | 128.3 (100.5–173.2) | 126.8 (81.1–154) | 0.4 | |
| PF ratio day 10 (median, IQR) | 123.3 (87.9–162) | 132.3 (96.3–170.4) | 86.9 (75.6–148.6) | 0.038 | |
| PF ratio day 15 (median, IQR) | 129.1 (90.3–172.2) | 127.7 (95.3–181.5) | 133.9 (79.3–171.5) | 0.48 | |
| Total (n = 178) | Fungal Infection | p-Value | ||
|---|---|---|---|---|
| No | Yes | |||
| White blood cells | 10.3 (6.8–14.6) | 10.3 (6.6–14.7) | 9.7 (7.6–13.6) | 0.99 |
| Neutrophils | 9.1 (5.5–13) | 9.1 (5.4–13.2) | 9.1 (6.6–12.3) | 0.89 |
| Lymphocytes | 0.7 (0.5–1) | 0.7 (0.5–1.01) | 0.6 (0.4–1) | 0.56 |
| NLR | 13.2 (8.1–23.3) | 13 (8.1–22.7) | 14.5 (7.4–25.5) | 0.53 |
| Monocytes | 0.5 (0.3–0.7) | 0.5 (0.3–0.7) | 0.4 (0.2–0.6) | 0.23 |
| Eosinophils | 0.01 (0–0.03) | 0.01 (0–0.03) | 0.03 (0–0.1) | 0.049 |
| Platelets | 237.4 (183.8–291.3) | 238.5 (184.5–288.1) | 234 (164–310.4) | 0.94 |
| Hemoglobin | 12.8 (11.4–14.1) | 12.8 (11.5–14.1) | 12.5 (10–14.5) | 0.41 |
| d-dimers | 1.4 (0.7–3.2) | 1.4 (0.7–2.8) | 3 (1–3.6) | 0.09 |
| Fibrinogen | 563 (461–659) | 563 (464–660) | 560 (450–610) | 0.59 |
| CRP | 10.2 (5.6–16.1) | 10.5 (5.8–16.1) | 6.7 (4–17.1) | 0.12 |
| Urea | 53 (41.5–70) | 53 (40–70) | 50 (45–73) | 0.5 |
| Creatinine | 0.9 (0.8–1.2) | 0.9 (0.8–1.2) | 0.9 (0.7–1.3) | 0.93 |
| AST | 41 (28–63) | 42 (28–68) | 36 (27–50) | 0.21 |
| ALT | 44 (29–81) | 45 (29–84) | 41 (27–65) | 0.47 |
| ALP | 60 (45–80) | 60 (46–80) | 52 (41–72) | 0.4 |
| γGT | 59 (36–102) | 59 (34–102) | 57.5 (37–92) | 0.91 |
| Albumin | 3.4 (3.1–3.6) | 3.4 (3.1–3.7) | 3.1 (2.8–3.5) | 0.026 |
| LDH | 438 (344–592) | 426.5 (334–568.5) | 549 (413–592) | 0.102 |
| CPK | 108.5 (55–258) | 107 (55–278) | 110 (73–204) | 0.6 |
| PCT | 0.2 (0.1–0.5) | 0.2 (0.1–0.5) | 0.1 (0.06–0.3) | 0.31 |
| Troponin | 21.4 (5.8–96.8) | 23.2 (6.2–120.1) | 12.2 (3.4–26.3) | 0.08 |
| Ferritin | 1143.5 (705.8–1830) | 1130 (704.7–1942) | 1297 (730.8) | 0.97 |
| Total (n = 178) | Fungal Infection | p-Value | |||
|---|---|---|---|---|---|
| Treatment | No | Yes | |||
| High dose corticosteroids (n, %) | 64 (36) | 52 (32.7) | 12 (63.2) | 0.009 | |
| Tocilizumab (n, %) | 39 (21.9) | 31 (19.5) | 8 (42.1) | 0.024 | |
| Remdesivir (n, %) | 135 (75.8) | 118 (74.2) | 17 (89.5) | 0.17 | |
| Anakinra (n, %) | 11 (6.2) | 9 (5.7) | 2 (10.5) | 0.33 | |
| Monoclonal antibodies (n, %) | 40 (22.5) | 36 (22.6) | 4 (21.1) | >0.99 | |
| CRRT (n, %) | 67 (37.6) | 53 (33.3) | 14 (73.7) | 0.001 | |
| ECMO (n, %) | 11 (6.2) | 5 (3.1) | 6 (31.6) | <0.001 | |
| Outcomes | |||||
| Barotrauma (n, %) | 43 (24.2) | 30 (18.9) | 13 (68.4) | <0.001 | |
| Pneumothorax (n, %) | 27 (15.2) | 18 (11.3) | 9 (47.4) | <0.001 | |
| Thromboembolism (n, %) | 28 (15.7) | 22 (13.8) | 6 (31.6) | 0.05 | |
| Hyperglycemia (n, %) | 83 (46.6) | 77 (48.4) | 6 (31.6) | 0.14 | |
| Septic shock (n, %) | 92 (51.7) | 75 (47.2) | 17 (89.5) | <0.001 | |
| Positive Culture (n, %) | Blood | 63 (35.4) | 47 (29.6) | 16 (84.2) | <0.001 |
| Central line | 36 (20.2) | 26 (16.4) | 10 (52.6) | <0.001 | |
| Bronchial secretions | 125 (70.2) | 107 (67.3) | 18 (94.7) | 0.015 | |
| Urine | 47 (26.4) | 38 (23.9) | 9 (47.4) | 0.036 | |
| Length of ICU stay (median, IQR) | 18 (8–37) | 15 (7–32) | 61 (37–97) | <0.001 | |
| Length of mechanical ventilation (median, IQR) | 4 (0–19) | 4 (0–14) | 42.5 (12–78) | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koukaki, E.; Rovina, N.; Tzannis, K.; Sotiropoulou, Z.; Loverdos, K.; Koutsoukou, A.; Dimopoulos, G. Fungal Infections in the ICU during the COVID-19 Era: Descriptive and Comparative Analysis of 178 Patients. J. Fungi 2022, 8, 881. https://doi.org/10.3390/jof8080881
Koukaki E, Rovina N, Tzannis K, Sotiropoulou Z, Loverdos K, Koutsoukou A, Dimopoulos G. Fungal Infections in the ICU during the COVID-19 Era: Descriptive and Comparative Analysis of 178 Patients. Journal of Fungi. 2022; 8(8):881. https://doi.org/10.3390/jof8080881
Chicago/Turabian StyleKoukaki, Evangelia, Nikoletta Rovina, Kimon Tzannis, Zoi Sotiropoulou, Konstantinos Loverdos, Antonia Koutsoukou, and George Dimopoulos. 2022. "Fungal Infections in the ICU during the COVID-19 Era: Descriptive and Comparative Analysis of 178 Patients" Journal of Fungi 8, no. 8: 881. https://doi.org/10.3390/jof8080881
APA StyleKoukaki, E., Rovina, N., Tzannis, K., Sotiropoulou, Z., Loverdos, K., Koutsoukou, A., & Dimopoulos, G. (2022). Fungal Infections in the ICU during the COVID-19 Era: Descriptive and Comparative Analysis of 178 Patients. Journal of Fungi, 8(8), 881. https://doi.org/10.3390/jof8080881