
High Incidence of Invasive Fungal Diseases in Patients with FLT3-Mutated AML Treated with Midostaurin: Results of a Multicenter Observational SEIFEM Study

 , ,
, ,  , , , , , , , , , , ,
, , , , , , , , , , , 
 ,
, 
 add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Definitions
3. Statistical Analysis
4. Results
4.1. Characteristics of Patients
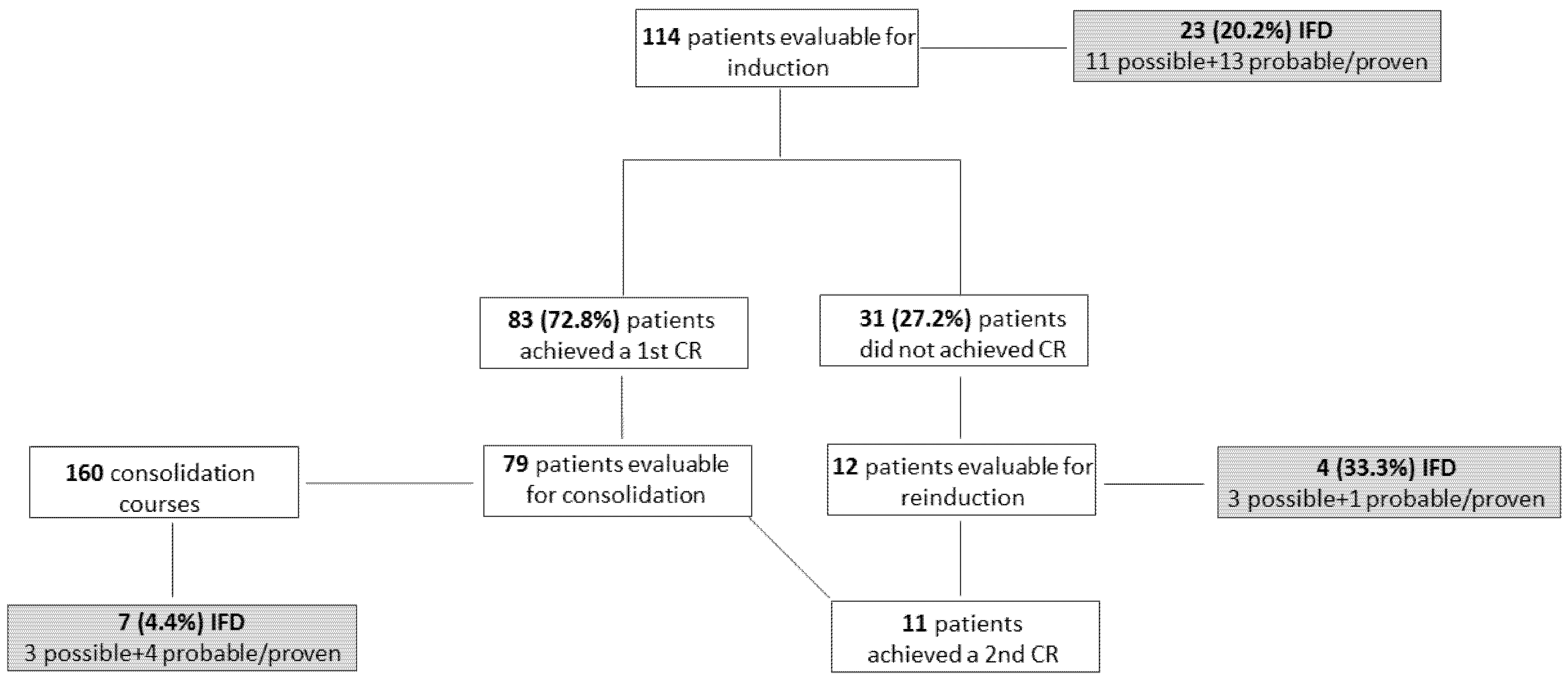
4.2. Incidence of IFD
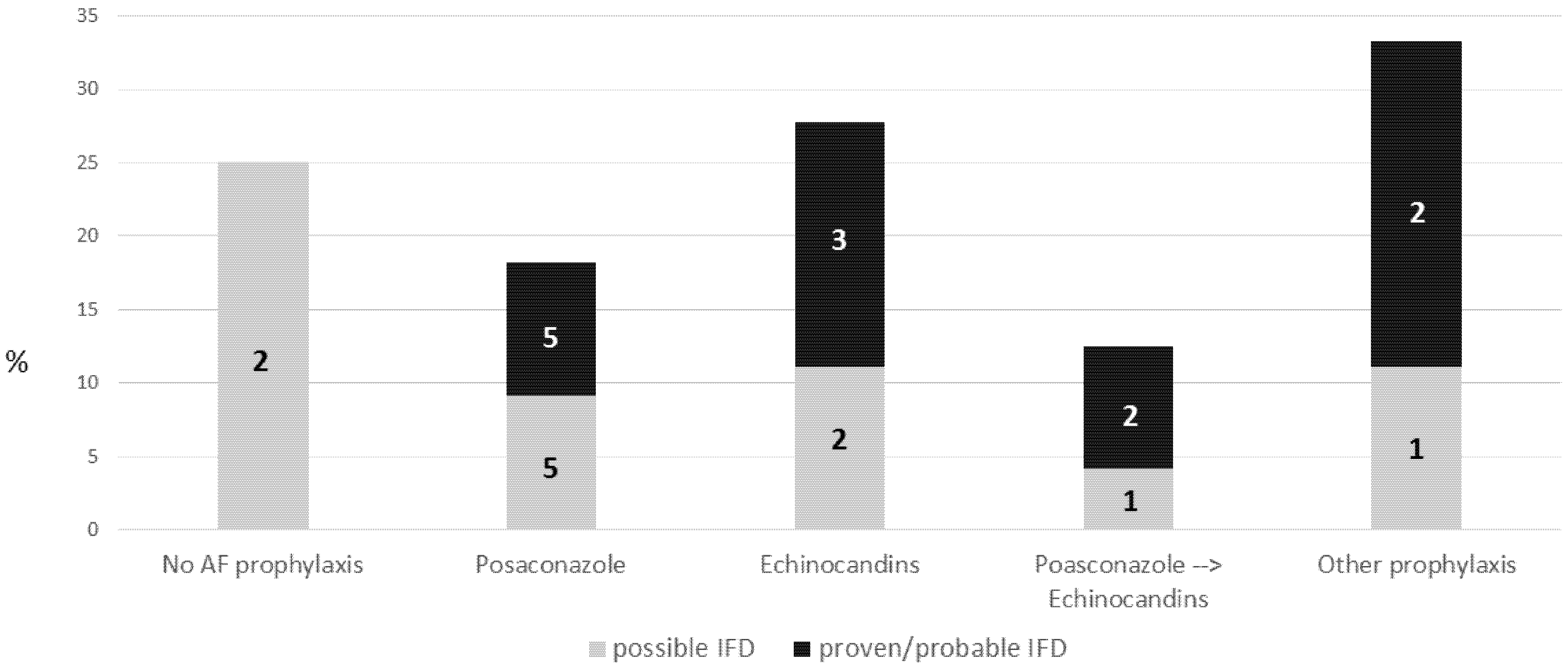
4.3. Association between IFD and AF Prophylaxis Strategy
4.4. Risk Factors for IFD
4.5. Midostaurin Discontinuation
4.6. Outcome
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yates, J.; Glidewell, O.; Wiernik, P.; Cooper, M.R.; Steinberg, D.; Dosik, H.; Levy, R.; Hoagland, C.; Henry, P.; Gottlieb, A.; et al. Cytosine arabinoside with daunorubicin or adriamycin for therapy of acute myelocytic leukemia: A CALGB study. Blood 1982, 60, 454–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, J.M.; Young, M.L.; Andersen, J.W.; Cassileth, P.A.; Tallman, M.S.; Paietta, E.; Wiernik, P.H.; Rowe, J.M. Long-term survival in acute myeloid leukemia: The Eastern Cooperative Oncology Group experience. Cancer 1997, 80 (Suppl. 11), 2205–2209. [Google Scholar] [CrossRef]
- Stone, R.M.; Mandrekar, S.J.; Sanford, B.L.; Laumann, K.; Geyer, S.; Bloomfield, C.D.; Thiede, C.; Prior, T.W.; Döhner, K.; Marcucci, G.; et al. Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation. N. Engl. J. Med. 2017, 377, 454–464. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Tran, P.; Gu, H.; Tedesco, V.; Zhang, J.; Lin, W.; Gatlik, E.; Klein, K.; Heimbach, T. Midostaurin, a Novel Protein Kinase Inhibitor for the Treatment of Acute Myelogenous Leukemia: Insights from Human Absorption, Metabolism, and Excretion Studies of a BDDCS II Drug. Drug Metab Dispos. 2017, 45, 540–555. [Google Scholar] [CrossRef] [Green Version]
- Gu, H.; Dutreix, C.; Rebello, S.; Ouatas, T.; Wang, L.; Chun, D.Y.; Einolf, H.J.; He, H. Simultaneous Physiologically Based Pharmacokinetic (PBPK) Modeling of Parent and Active Metabolites to Investigate Complex CYP3A4 Drug-Drug Interaction Potential: A Case Example of Midostaurin. Drug Metab Dispos. 2018, 46, 109–121. [Google Scholar] [CrossRef]
- Dragonetti, G.; Criscuolo, M.; Fianchi, L.; Pagano, L. Invasive aspergillosis in acute myeloid leukemia: Are we making progress in reducing mortality? Med. Mycol. 2017, 55, 82–86. [Google Scholar] [CrossRef] [Green Version]
- Candoni, A.; Farina, F.; Perruccio, K.; Di Blasi, R.; Criscuolo, M.; Cattaneo, C.; Delia, M.; Zannier, M.E.; Dragonetti, G.; Fanci, R.; et al. Impact of invasive aspergillosis occurring during first induction therapy on outcome of acute myeloid leukaemia (SEIFEM-12B study). Mycoses 2020, 63, 1094–1100. [Google Scholar] [CrossRef]
- Cattaneo, C.; Gramegna, D.; Malagola, M.; Pagani, C.; Borlenghi, E.; Cerqui, E.; Passi, A.; Sciumé, M.; Bernardi, S.; Crippa, C.; et al. Invasive pulmonary aspergillosis in acute leukemia: A still frequent condition with a negative impact on the overall treatment outcome. Leuk. Lymphoma 2019, 60, 3044–3050. [Google Scholar] [CrossRef]
- Cornely, O.A.; Maertens, J.; Winston, D.J.; Perfect, J.; Ullmann, A.J.; Walsh, T.J.; Helfgott, D.; Holowiecki, J.; Stockelberg, D.; Goh, Y.T.; et al. Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia. N. Engl. J. Med. 2007, 356, 348–359. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlenk, R.F.; Weber, D.; Fiedler, W.; Salih, H.R.; Wulf, G.; Salwender, H.; Schroeder, T.; Kindler, T.; Lübbert, M.; Wolf, D.; et al. Midostaurin added to chemotherapy and continued single-agent maintenance therapy in acute myeloid leukemia with FLT3-ITD. Blood 2019, 133, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Phoompoung, P.; Henry, B.; Daher-Reyes, G.; Sibai, H.; Husain, S. Invasive Mold Infections in FLT3-Mutated Acute Myeloid Leukemia. Clin. Lymphoma Myeloma Leuk. 2021, 21, e477–e482. [Google Scholar] [CrossRef] [PubMed]
- Michallet, M.; Sobh, M.; Morisset, S.; Kraghel, S.; Nicolini, F.E.; Thomas, X.; Bienvenu, A.L.; Picot, S.; Nicolle, M.C.; Vanhems, P. Risk factors for invasive aspergillosis in acute myeloid leukemia patients prophylactically treated with Posaconazole. Med. Mycol. 2011, 49, 681–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nucci, M.; Anaissie, E. How we treat invasive fungal diseases in patients with acute leukemia: The importance of an individualized approach. Blood 2014, 124, 3858–3869. [Google Scholar] [CrossRef] [Green Version]
- Whartenby, K.A.; Calabresi, P.A.; McCadden, E.; Nguyen, B.; Kardian, D.; Wang, T.; Mosse, C.; Pardoll, D.M.; Small, D. Inhibition of FLT3 signaling targets DCs to ameliorate autoimmune disease. Proc. Natl. Acad. Sci. USA 2005, 102, 16741–16746. [Google Scholar] [CrossRef] [Green Version]
- Tussiwand, R.; Onai, N.; Mazzucchelli, L.; Manz, M.G. Inhibition of natural type I IFN-producing and dendritic cell development by a small molecule receptor tyrosine kinase inhibitor with Flt3 affinity. J. Immunol. 2005, 175, 3674–3680. [Google Scholar] [CrossRef]
- McNab, F.; Mayer-Barber, K.; Sher, A.; Wack, A.; O’Garra, A. Type I interferons in infectious disease. Nat. Rev. Immunol. 2015, 15, 87–103. [Google Scholar] [CrossRef]
- Del Principe, M.I.; Dragonetti, G.; Verga, L.; Candoni, A.; Marchesi, F.; Cattaneo, C.; Delia, M.; Potenza, L.; Farina, F.; Ballanti, S.; et al. ‘Real-life’ analysis of the role of antifungal prophylaxis in preventing invasive aspergillosis in AML patients undergoing consolidation therapy: Sorveglianza Epidemiologica Infezioni nelle Emopatie (SEIFEM) 2016 study. J. Antimicrob. Chemother. 2019, 74, 1062–1068. [Google Scholar] [CrossRef]
- Nicolle, M.C.; Bénet, T.; Thiebaut, A.; Bienvenu, A.L.; Voirin, N.; Duclos, A.; Sobh, M.; Cannas, G.; Thomas, X.; Nicolini, F.E.; et al. Invasive aspergillosis in patients with hematologic malignancies: Incidence and description of 127 cases enrolled in a single institution prospective survey from 2004 to 2009. Haematologica 2011, 96, 1685–1691. [Google Scholar] [CrossRef]
- Even, C.; Bastuji-Garin, S.; Hicheri, Y.; Pautas, C.; Botterel, F.; Maury, S.; Cabanne, L.; Bretagne, S.; Cordonnier, C. Impact of invasive fungal disease on the chemotherapy schedule and event-free survival in acute leukemia patients who survived fungal disease: A case-control study. Haematologica 2011, 96, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Ouatas, T.; Duval, V.; Sinclair, K.; Berkowitz, N. Concomitant use of midostaurin with strong CYP3A4 inhibitors: An analysis from the RATIFY trial. Blood 2017, 130 (Suppl. 1), 3814. [Google Scholar]
- Menna, P.; Salvatorelli, E.; Del Principe, M.I.; Perrone, S.; Pagano, L.; Marchesi, F.; Minotti, G. Choosing Antifungals for the Midostaurin-Treated Patient: Does CYP3A4 Outweigh Recommendations? A Brief Insight from Real Life. Chemotherapy 2021, 66, 47–52. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| M/F ratio | 49/65 |
| Median age, years (range) | 55 (18–78) |
| FLT3 ITD/TKD mutation (%) | 94 (82.5)/20(17.5) |
| NPM-1 mutation (%) | 70 (61.4) |
| ELN (low/not low) (%) | 34 (32.7)/70 (67.3) * |
AF prophylaxis (induction cht, n = 114) (%)
| 8 (7) 3 (2.6) 55 (48.2) 24 (21.1) 18 (15.8) 4 (3.5) 2 (1.8) |
AF prophylaxis (reinduction cht, n = 12) (%)
| 2 (1.7) 3 (25) 1 (7.3) 6 (50) |
AF prophylaxis (consolidation cht, n = 160)
| 87 (54.3) 8 (5) 20 (12.5) 6 (3.8) 27 (16.9) 1 (0.6) 6 (3.8) 5 (3.1) |
| Median duration of PMN<500/mmc (days) ** | 22 (range 8–180) |
| Midostaurin suspension (induction) (%) | 16/114 (14) |
| CR after first induction (%) | 83 (72.8%) |
| Median follow-up, months (range) | 5 (1–32) |
| Type of IFD | Microbiology/Biomarker | |
|---|---|---|
| Induction (active hematologic disease) | ||
| 1 | Pulmonary aspergillosis | GM serum |
| 2 | Pulmonary aspergillosis | GM BAL |
| 3 | Pulmonary + sinus aspergillosis | GM serum |
| 4 | Pulmonary aspergillosis | A. terreus (BAL) |
| 5 | Pulmonary aspergillosis | GM serum |
| 6 | Pulmonary aspergillosis | GM serum/BAL |
| 7 | Geothricosis | S. capitata (lung biopsy) |
| 8 | Pulmonary aspergillosis | GM serum |
| 9 | Candidemia | Candida spp. |
| 10 | Candidemia | C. krusei |
| 11 | Candidemia | C. krusei + C. incospicua |
| 12 | Candidemia | C. glabrata |
| Reinduction (active hematologic disease) | ||
| 1 | Pulmonary aspergillosis | GM serum |
| Consolidation (controlled hematologic disease) | ||
| 1 | Pulmonary aspergillosis | GM serum |
| 2 | Pulmonary + sinus aspergillosis | GM BAL |
| 3 | Pulmonary aspergillosis | GM serum |
| 4 | Candidemia | C. parapsilosis |
| (a) | |||
| IFD = 12 | Univariate | ||
| Comparison | OR (95% CI) | p-Value | |
| Age | Continuous | 1.10 (1.03–1.19) | 0.008 |
| Gender | Female vs. Male | 0.73 (0.22–2.42) | 0.605 |
| FLT3 | TKD vs. ITD | 2.50 (0.68–9.25) | 0.170 |
| NPM | Pos vs. Neg | 0.88 (0.26–2.97) | 0.838 |
| ELN | Not low vs. Low | 0.97 (0.27–3.47) | 0.960 |
| AF prophylaxis | Yes vs. No | not estim | not estim |
| Neutropenia (days) * | Continuous | 0.99 (0.95–1.03) | 0.665 |
| Posaconazole containing prophylaxis | Yes vs. No | 0.58 (0.17–1.98) | 0.388 |
| (b) | |||
| IFD = 23 | Univariate | ||
| Comparison | OR (95% CI) | p-Value | |
| Age | Continuous | 1.06 (1.01–1.10) | 0.021 |
| Gender | Female vs. Male | 0.98 (0.39–2.45) | 0.957 |
| FLT3 | TKD vs. ITD | 1.30 (0.42–4.02) | 0.647 |
| NPM | Pos vs. Neg | 0.79 (0.31–2.00) | 0.617 |
| ELN | Not low vs. Low | 1.05 (0.38–2.88) | 0.922 |
| AF prophylaxis | Yes vs. No | 0.74 (0.14–3.94) | 0.725 |
| Neutropenia (days) * | Continuous | 0.99 (0.97–1.02) | 0.861 |
| Posaconazole containing prophylaxis | Yes vs. No | 0.49 (0.19–1.27) | 0.141 |
| . | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| Comparison | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age | continuous | 1.03 (0.98–1.08) | 0.222 | ||
| Gender | Female vs. Male | 1.11 (0.40–3.02) | 0.846 | ||
| FLT3 | TKD vs. ITD | 0.73 (0.17–3.22) | 0.679 | ||
| NPM | Pos vs. Neg | 1.02 (0.39–2.63) | 0.974 | ||
| ELN | Not low vs. Low | 1.53 (0.51–4.58) | 0.452 | ||
| AF prophylaxis | Yes vs. No | 0.63 (0.14–2.80) | 0.539 | ||
| Neutropenia (days) * | continuous | 1.03 (1.01–1.05) | 0.002 | 1.02 (1.00–1.04) | 0.019 |
| Posaconazole containing prophylaxis | Yes vs. No | 1.64 (0.61–4.41) | 0.331 | ||
| IFD | Yes vs. No | 1.90 (0.66–5.47) | 0.235 | ||
| possible IFD | Yes vs. No | 1.86 (0.22–15.67) | 0.568 | ||
| probable IFD | Yes vs. No | 1.57 (0.35–6.98) | 0.554 | ||
| proven IFD | Yes vs. No | 1.81 (0.40–8.15) | 0.438 | ||
| Response to AML tratment | No CR vs. CR | 5.11 (1.92–13.60) | 0.001 | 4.68 (1.47–14.92) | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cattaneo, C.; Marchesi, F.; Terrenato, I.; Bonuomo, V.; Fracchiolla, N.S.; Delia, M.; Criscuolo, M.; Candoni, A.; Prezioso, L.; Facchinelli, D.; et al. High Incidence of Invasive Fungal Diseases in Patients with FLT3-Mutated AML Treated with Midostaurin: Results of a Multicenter Observational SEIFEM Study. J. Fungi 2022, 8, 583. https://doi.org/10.3390/jof8060583
Cattaneo C, Marchesi F, Terrenato I, Bonuomo V, Fracchiolla NS, Delia M, Criscuolo M, Candoni A, Prezioso L, Facchinelli D, et al. High Incidence of Invasive Fungal Diseases in Patients with FLT3-Mutated AML Treated with Midostaurin: Results of a Multicenter Observational SEIFEM Study. Journal of Fungi. 2022; 8(6):583. https://doi.org/10.3390/jof8060583
Chicago/Turabian StyleCattaneo, Chiara, Francesco Marchesi, Irene Terrenato, Valentina Bonuomo, Nicola Stefano Fracchiolla, Mario Delia, Marianna Criscuolo, Anna Candoni, Lucia Prezioso, Davide Facchinelli, and et al. 2022. "High Incidence of Invasive Fungal Diseases in Patients with FLT3-Mutated AML Treated with Midostaurin: Results of a Multicenter Observational SEIFEM Study" Journal of Fungi 8, no. 6: 583. https://doi.org/10.3390/jof8060583
APA StyleCattaneo, C., Marchesi, F., Terrenato, I., Bonuomo, V., Fracchiolla, N. S., Delia, M., Criscuolo, M., Candoni, A., Prezioso, L., Facchinelli, D., Pasciolla, C., Del Principe, M. I., Dargenio, M., Buquicchio, C., Mitra, M. E., Farina, F., Borlenghi, E., Nadali, G., Gagliardi, V. P., ... Pagano, L. (2022). High Incidence of Invasive Fungal Diseases in Patients with FLT3-Mutated AML Treated with Midostaurin: Results of a Multicenter Observational SEIFEM Study. Journal of Fungi, 8(6), 583. https://doi.org/10.3390/jof8060583