
COVID-19 Associated Pulmonary Aspergillosis (CAPA): Hospital or Home Environment as a Source of Life-Threatening Aspergillus fumigatus Infection?

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Microbiology Data Collection
2.3. Antifungal Drugs Susceptibility Testing
2.4. Environmental Surveillance
2.5. Aspergillus fumigatus Strains
2.5.1. Cyp51A Amplification, PCR Conditions and Sequencing
2.5.2. Strains Genotyping
3. Results
3.1. Clinical A. fumigatus Genotypes
3.2. Hospital Environmental A. fumigatus Genotypes
3.3. Correlation between Clinical and Environmental A. fumigatus Genotypes
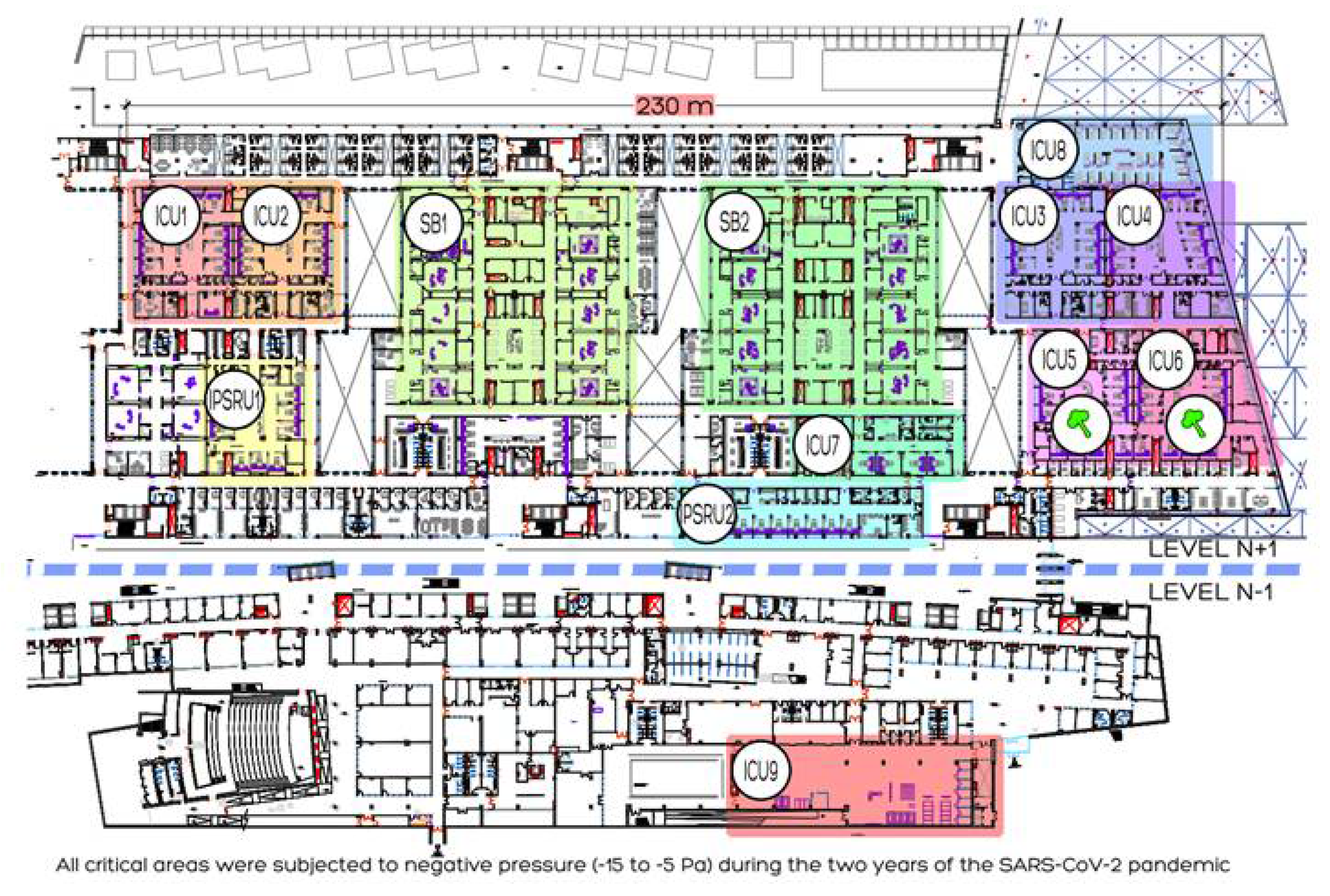
- Patient 8 admitted to Pneumology SE 2° B on 8 October 2020, exhibited the same A. fumigatus genotype (t03m1.1g05A.e09) as patient 19 admitted to box 36 on 20 November 2020; however, there was a significant difference over time (44 days) and in unit location (2 floors).
- Patient 9 admitted to box 39 on 8 October 2020, exhibited the same A. fumigatus genotype (t02m1.1g09.e16) as patient 14 was admitted to box 47 on 7 November 2020; however, there was a significant difference over time (31 days) and in unit location (different ICUs).
- Four patients (2, 18, 27 and 28) share the same genotype (t02m1.1g09.e05). Analyzing the patients individually, we observed that there is no correlation neither in time nor in their location in the hospital. The first patient (2) diagnosed on 30 March 2020, in box 10 presents a significant difference of 228 days with the second patient (18) admitted in box 91. The difference with the third patient (27) admitted in box 57 was 254 days, and the difference in time with the fourth patient (28) admitted in box 18 was 279 days. The four patients were admitted to different ICUs.
3.4. Aspergillus PCR in the Primary Respiratory Sample
3.5. Antifungal Susceptibility and Cyp51A Amplification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ARDS | Acute respiratory distress syndrome |
| BAL | Bronchoalveolar lavage. |
| B-D-G | Beta-D glucan. |
| CAPA | COVID-19 Associated Pulmonary Aspergillosis) |
| COVID | Coronavirus disease. |
| ECMM/ISHAM | European Confederation of Medical Mycology/International Society for Human and Animal Mycology |
| Study | Group Education and Research Consortium. |
| GM | Galactomannan. |
| ICU | Intensive care unit. |
| LFA | Lateral flow assays |
| LFD | Lateral flow device. |
| MALDI-TOF | Matrix-assisted laser desorption ionization-time of -light |
| NBL | Non-bronchoscopic lavage |
| OR | Odds ratio |
| PCR | Polymerase chain reaction. |
| TA | Tracheal aspirate. |
References
- Brenier-Pinchart, M.P.; Lebeau, B.; Borel, J.L.; Quesada, J.L.; Mallaret, M.R.; Garban, F.; Brion, J.P.; Molina, L.; Bosson, J.L.; Thiebaut-Bertrand, A.; et al. Community-acquired invasive aspergillosis and outdoor filamentous fungal spore load: A relationship? Clin. Microbiol. Infect. 2011, 17, 1387–1390. [Google Scholar] [CrossRef] [PubMed]
- García Clemente, M.; Madrid Carbajal, C.; Iscar Urrutia, M. Influenza, SARS-CoV-2 y aspergilosis pulmonar invasiva [Influenza, SARS-CoV-2 and Invasive Pulmonary Aspergillosis]. Arch. Bronconeumol. 2021, 57, 11–12. [Google Scholar] [CrossRef] [PubMed]
- Schauwvlieghe, A.F.A.D.; Rijnders, B.J.A.; Philips, N.; Verwijs, R.; Vanderbeke, L.; Van Tienen, C.; Lagrou, K.; Verweij, P.E.; Van de Veerdonk, F.L.; Gommers, D.; et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: A retrospective cohort study. Lancet Respir. Med. 2018, 6, 782–792. [Google Scholar] [CrossRef]
- Wauters, J.; Baar, I.; Meersseman, P.; Meersseman, W.; Dams, K.; De Paep, R.; Lagrou, K.; Wilmer, A.; Jorens, P.; Hermans, G. Invasive pulmonary aspergillosis is a frequent complication of critically ill H1N1 patients: A retrospective study. Intensiv. Care Med. 2012, 38, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- Prattes, J.; Wauters, J.; Giacobbe, D.R.; Salmanton-García, J.; Maertens, J.; Bourgeois, M.; Reynders, M.; Rutsaert, L.; Van Regenmortel, N.; Lormans, P.; et al. Risk factors and outcome of pulmonary aspergillosis in critically ill coronavirus disease 2019 patients-a multinational observational study by the European Confederation of Medical Mycology. Clin. Microbiol. Infect. 2021, 26, S1198-743X(21)00474-2. [Google Scholar] [CrossRef] [PubMed]
- Verweij, P.E.; Rijnders, B.J.A.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Calandra, T.; Clancy, C.J.; Cornely, O.A.; Chiller, T.; et al. Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: An expert opinion. Intensiv. Care Med. 2020, 46, 1524–1535. [Google Scholar] [CrossRef] [PubMed]
- Alanio, A.; Dellière, S.; Fodil, S.; Bretagne, S.; Mégarbane, B. Prevalence of putative invasive pulmonary aspergillosis in critically ill patients with COVID-19. Lancet Respir. Med. 2020, 8, e48–e49. [Google Scholar] [CrossRef]
- Segrelles-Calvo, G.; Araújo, G.R.S.; Llopis-Pastor, E.; Carrillo, J.; Hernández-Hernández, M.; Rey, L.; Rodríguez Melean, N.; Escribano, I.; Antón, E.; Zamarro, C.; et al. Prevalence of opportunistic invasive aspergillosis in COVID-19 patients with severe pneumonia. Mycoses 2021, 64, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.; Valerio, M.; Álvarez-Uría, A.; Olmedo, M.; Veintimilla, C.; Padilla, B.; De la Villa, S.; Guinea, J.; Escribano, P.; Ruiz-Serrano, M.J.; et al. Invasive pulmonary aspergillosis in the COVID-19 era: An expected new entity. Mycoses 2021, 64, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Jenks, J.D.; Nam, H.H.; Hoenigl, M. Invasive aspergillosis in critically ill patients: Review of definitions and diagnostic approaches. Mycoses 2021, 64, 1002–1014. [Google Scholar] [CrossRef] [PubMed]
- Marta, G.-C.; Lorena, F.-E.; Laura, M.-V.; Angela, L.-M.; Blanca, L.-G.; Rodrigo, A.-A.; Marta, S.-G.; Santiago, M.-G.; Liliana, P.-M.; Luisa, S.-N.M.; et al. COVID-19 Associated Pulmonary Aspergillosis in a tertiary hospital. J. Fungi 2022, 82, 97. [Google Scholar] [CrossRef] [PubMed]
- Waldeck, F.; Boroli, F.; Suh, N.; Wendel Garcia, P.D.; Flury, D.; Notter, J.; Iten, A.; Kaiser, L.; Schrenzel, J.; Boggian, K.; et al. Influenza-associated aspergillosis in a critically-ill patients-a retrospective bicentric cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1915–1923. [Google Scholar] [CrossRef] [PubMed]
- Mahieu, L.M.; De Dooy, J.J.; Van Laer, F.A.; Jansens, H.; Ieven, M.M. A prospective study on factors influencing aspergillus spore load in the air during renovation works in a neonatal intensive care unit. J. Hosp. Infect. 2000, 45, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Alberti, C.; Bouakline, A.; Ribaud, P.; Lacroix, C.; Rousselot, P.; Leblanc, T.; Derouin, F. Relationship between environmental fungal contamination and the incidence of invasive aspergillosis in hematology patients. J. Hosp. Infect. 2001, 48, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Gangneux, J.P.; Bretagne, S.; Cordonnier, C.; Datry, A.; Derouin, F.; Grillot, R.; Kauffmann-Lacroix, C.; Lebeau, B.; Morin, O.; Nicolle, M.C.; et al. Prevention of nosocomial fungal infection: The French approach. Clin. Infect. Dis. 2002, 35, 343–346. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Peláez, T.; Muñoz, P.; Guinea, J.; Valerio, M.; Giannella, M.; Klaasen, H.W.; Bouza, E. Outbreak of Invasive Aspergillosis after Major Heart Surgery Caused by Spores in the Air of the Intensive Care Unit. Clin. Infect. Dis. 2012, 54, e24–e31. [Google Scholar] [CrossRef] [PubMed]
- Fourneret-Vivier, A.; Lebeau, B.; Mallaret, M.R.; Brenier-Pinchart, M.P.; Brion, J.P.; Pinel, C.; Garban, F.; Pison, C.; Hamidfar, R.; Plantaz, D.; et al. Hospital-wide prospective mandatory surveillance of invasive aspergillosis in a French teaching hospital (2000–2002). J. Hosp. Infect. 2006, 62, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Hajjeh, R.A.; Warnock, D.W. Counterpoint: Invasive aspergillosis and the environment—rethinking our approach to prevention. Clin. Infect. Dis. 2001, 33, 1549–1552. [Google Scholar] [CrossRef] [PubMed]
- Panackal, A.A.; Li, H.; Kontoyiannis, D.P.; Mori, M.; Perego, C.A.; Boeckh, M.; Marr, K.A. Geoclimatic influences on invasive aspergillosis after hematopoietic stem cell transplantation. Clin. Infect. Dis. 2010, 50, 1588–1597. [Google Scholar] [CrossRef] [PubMed]
- Verweij, P.E.; Gangneux, J.P.; Bassetti, M.; Brüggemann, R.J.M.; Cornely, O.A.; Koehler, P.; Lass-Flörl, C.; van de Veerdonk, F.L.; Chakrabarti, A.; Hoenigl, M. Diagnosing COVID-19-associated pulmonary aspergillosis. Lancet Microbe 2020, 1, e53–e55. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Cuenca-Estrella, M.; Lass-Flörl, C.; Hope, W.W. European Committee on Antimicrobial Susceptibility Testing Subcommittee on Antifungal Susceptibility Testing (EUCAST-AFST). EUCAST technical note on Aspergillusand amphotericin B, itraconazole, and posaconazole. Clin. Microbiol. Infect. 2012, 18, E248–E250. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing. Antifungal Agents. Breakpoint Tables for Interpretation of MICs. Version 9.0. Available online: https://www.eucast.org/astoffungi/clinicalbreakpointsforantifungals/ (accessed on 7 December 2020).
- Vandecasteele, S.J.; Boelaert, J.R.; Verrelst, P.; Graulus, E.; Gordts, B.Z. Diagnosis and treatment of Aspergillus flavus sternal wound infections after cardiac surgery. Clin. Infect. Dis 2002, 35, 887–890. [Google Scholar] [CrossRef] [PubMed]
- Alcazar-Fuoli, L.; Mellado, E.; Alastruey-Izquierdo, A.; Cuenca-Estrella, M.; Rodriguez-Tudela, J.L. Aspergillus section Fumigati: Antifungal susceptibility patterns and sequence-based identification. Antimicrob. Agents Chemother. 2008, 52, 1244–1251. [Google Scholar] [CrossRef]
- Blanco, J.L.; Hontecillas, R.; Bouza, E.; Blanco, I.; Pelaez, T.; Muñoz, P.; Molina, J.P.; Garcia, M.E. Correlation between the Elastase Activity Index and Invasiveness of Clinical Isolates of Aspergillus fumigatus. J. Clin. Microbiol. 2002, 40, 1811–1813. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tang, C.M.; Cohen, J.; Holden, D.W. An Aspergillusfumigatus alkaline protease mutant constructed by gene disruption is deficient in extracellular elastase activity. Mol. Microbiol. 1992, 6, 1663–1671. [Google Scholar] [CrossRef] [PubMed]
- Mellado, E.; Diaz-Guerra, T.M.; Cuenca-Estrella, M.; Rodriguez-Tudela, J.L. Identification of two different 14-alpha sterol demethylase-related genes (cyp51A and cyp51B) in Aspergillusfumigatus and other Aspergillus species. J. Clin. Microbiol. 2001, 39, 2431–2438. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Rubio, R.; Gil, H.; Monteiro, M.C.; Peláez, T.; Mellado, E. A new Aspergillus fumigatus typing method based on hypervariable tandem repeats located within exons of surface protein-coding genes (TRESP). PLoS ONE 2016, 11, e0163869. [Google Scholar] [CrossRef]
- Garcia-Rubio, R.; Escribano, P.; Gomez, A.; Guinea, J.; Mellado, E. Comparison of Two Highly Discriminatory Typing Methods to Analyze Aspergillus fumigatus Azole Resistance. Front. Microbiol. 2018, 9, 1626. [Google Scholar] [CrossRef] [PubMed]
- Hunter, P.R.; Gaston, M.A. Numerical index of the discriminatory ability of typing systems: An application of Simpson’s index of diversity. J. Clin. Microbiol. 1988, 26, 2465–2466. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.E.; Zidouh, A.; Miniter, P.; Andriole, V.T.; Patterson, T.F. Hospital epidemiological surveillancefor invasive aspergillosis: Patient demographics and the utility of antigen detection. Infect. Control. Hosp. Epidemiol. 1997, 18, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Vandewoude, K.H.; I Blot, S.; Depuydt, P.; Benoit, D.; Temmerman, W.; Colardyn, F.; Vogelaers, D. Clinical relevance of Aspergillus isolation from respiratory tract samples in critically ill patients. Crit. Care 2006, 10, R31. [Google Scholar] [CrossRef] [PubMed]
- Nicolle, M.C.; Benet, T.; Vanhems, P. Aspergillosis: Nosocomial or community-acquired? Med. Micol. 2011, 49, S24–S29. [Google Scholar] [CrossRef] [PubMed]
- Sulahian, A.; Boutboul, F.; Ribaud, P.; Leblanc, T.; Lacroix, C.; Derouin, F. Value of antigen detection using an enzyme immunoassay in diagnosing and predicting invasive aspergillosis in two adult and pediatric hematology units during a 4-year prospective study. Cancer 2001, 91, 311–318. [Google Scholar] [CrossRef]
- Hope, W.W.; Walsh, T.J.; Denning, D.W. Laboratory diagnosis of invasive aspergillosis. Lancet Infect. Dis. 2005, 50, 609–622. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| SAMPLE | PATIENT | DATE | LOCATION | GENOTYPE |
|---|---|---|---|---|
| H-1880 | 1 | 23 March 2020 | BOX 45 | t18bm6.3g09.e09 |
| H-1882 | 2 | 30 March 2020 | BOX 10 | t02m1.1g09.e05 |
| H-1883 | 3 | 31 March 2020 | BOX 44 | t01m1.1g09.e07 |
| H-1885 | 4 | 4 April 2020 | 915 B | t01m5.1g09.e07 |
| H-1891 | 5 | 4 April 2020 | BOX 29 | t09m1.1g08A.e07 |
| H-1918 | 6 | 27 April 2020 | BOX 54 | t28m1.1g09.e20 |
| H-1935 | 7 | 16 May 2020 | 513 A | t03m1.3g08A.e07 |
| H-2096 | 8 | 8 October 2020 | SE 2° B | t03m1.1g05A.e09 |
| H-2097 | 9 | 8 October 2020 | BOX 39 | t02m1.1g09.e16 |
| H-2104 | 10 | 14 October 2020 | BOX 54 | t03m3.3g05A.e07 |
| H-2129 | 11 | 23 October 2020 | BOX 32 | t04Am1.1g05A.e07 |
| H-2135 | 12 | 25 October 2020 | BOX 14 | t11m1.2g09.e13 |
| H-2136 | 12 | 25 October 2020 | BOX 14 | t03m1.1g10.e06 |
| H-2159 | 12 | 3 November 2020 | BOX 14 | t02m1.8g09.e05 |
| H-2152 | 13 | 30 October 2020 | BOX 49 | t06Bm6.1g08A.e09 |
| H-2158 | 14 | 4 November 2020 | BOX 47 | t06Bm3.4g08A.e11 |
| H-2169 | 14 | 7 November 2020 | BOX 47 | t02m1.1g09.e16 |
| H-2167 | 15 | 5 November 2020 | BOX 33 | t03m1.1g04.e07 |
| H-2175 | 16 | 9 November 2020 | BOX 24 | t04Bm1.2g12.e15 |
| H-2184 | 17 | 13 November 2020 | BOX 89 | t04Am3.4g08A.e11 |
| H-2185 | 17 | 13 November 2020 | BOX 89 | t01m5.1g09.e06 |
| H-2186 | 18 | 13 November 2020 | BOX 91 | t02m1.1g09.e05 |
| H-2194 | 19 | 20 November 2020 | BOX 36 | t03m1.1g05A.e09 |
| H-2203 | 20 | 19 November 2020 | 925 A | t03m1.1g10.e09 |
| H-2211 | 21 | 31 November 2020 | 631 B | t02m14.1g09.e05 |
| H-2217 | 22 | 24 November 2020 | 532 B | t01m1.1g08A.e07 |
| H-2224 | 22 | 27 November 2020 | 306 B | t03m1.1g09.e07 |
| H-2238 | 23 | 3 December 2020 | BOX 67 | t02m1.2g09.e05 |
| H-2239 | 24 | 4 December 2020 | BOX 26 | t04Am3.3g17.eND |
| H-2267 | 24 | 16 December 2020 | BOX 31 | t04Am3.3g24.eND |
| H-2244 | 25 | 8 December 2020 | BOX 84 | t01m3.4g05A.e07 |
| H-2245 | 26 | 9 December 2020 | BOX 40S | t11m13.1g08A.e16 |
| H-2257 | 26 | 13 December 2020 | BOX 40S | t01m5.1g09.e13 |
| H-2246 | 27 | 8 December 2020 | BOX 57 | t02m1.1g09.e05 |
| H-2279 | 28 | 1 January 2021 | BOX 18 | t02m1.1g09.e05 |
| SAMPLE | DATE | LOCATION | CFU/m3 | GENOTYPE |
|---|---|---|---|---|
| HUCA-1800 | 23 January 2020 | HB 902 | 1 | 04Am1.3g08A.e07 |
| HUCA-1801 | 23 January 2020 | HB 902 | 1 | t04Am1.1g04.e07 |
| HUCA-1903 | 14 April 2020 | UCI 6 | 1 | t03m1.1g09.e09 |
| HUCA-2011 | 29 July 2020 | HB 902 | 1 | t02m11.1g09.e16 |
| HUCA-2061 | 10 September 2020 | Cytogenetics | 1 | t03m1.3g08A.e09 |
| HUCA-2130 | 19 October 2020 | Hb 903 | 1 | t02m1.1g09.e13 |
| HUCA-2151 | 30 October 2020 | UCI 5 | 1 | t01m1.1g08A.e07 |
| SAMPLE | ORIGIN | DATE | LOCATION | GENOTYPE |
|---|---|---|---|---|
| HUCA-2151 | Air Sample | 30 October 2020 | UCI-5 BOX 54 | t01m1.1g08A.e07 |
| H-2217 | Patient 22 | 24 November 2020 | 532 B | t01m1.1g08A.e07 |
| H-2096 | Patient 8 | 8 October 2020 | SE 2° B | t03m1.1g05A.e09 |
| H-2194 | Patient 19 | 20 November 2020 | BOX 36 | t03m1.1g05A.e09 |
| H-2097 | Patient 9 | 8 October 2020 | BOX 39 | t02m1.1g09.e16 |
| H-2169 | Patient 14 | 7 November 2020 | BOX 47 | t02m1.1g09.e16 |
| H-1882 | Patient 2 | 30 March 2020 | BOX 10 | t02m1.1g09.e05 |
| H-2186 | Patient 18 | 13 November 2020 | BOX 91 | t02m1.1g09.e05 |
| H-2246 | Patient 27 | 8 December 2020 | BOX 57 | t02m1.1g09.e05 |
| H-2279 | Patient 28 | 1 January 2021 | BOX 18 | t02m1.1g09.e05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peláez-García de la Rasilla, T.; González-Jiménez, I.; Fernández-Arroyo, A.; Roldán, A.; Carretero-Ares, J.L.; García-Clemente, M.; Telenti-Asensio, M.; García-Prieto, E.; Martínez-Suarez, M.; Vázquez-Valdés, F.; et al. COVID-19 Associated Pulmonary Aspergillosis (CAPA): Hospital or Home Environment as a Source of Life-Threatening Aspergillus fumigatus Infection? J. Fungi 2022, 8, 316. https://doi.org/10.3390/jof8030316
Peláez-García de la Rasilla T, González-Jiménez I, Fernández-Arroyo A, Roldán A, Carretero-Ares JL, García-Clemente M, Telenti-Asensio M, García-Prieto E, Martínez-Suarez M, Vázquez-Valdés F, et al. COVID-19 Associated Pulmonary Aspergillosis (CAPA): Hospital or Home Environment as a Source of Life-Threatening Aspergillus fumigatus Infection? Journal of Fungi. 2022; 8(3):316. https://doi.org/10.3390/jof8030316
Chicago/Turabian StylePeláez-García de la Rasilla, Teresa, Irene González-Jiménez, Andrea Fernández-Arroyo, Alejandra Roldán, Jose Luis Carretero-Ares, Marta García-Clemente, Mauricio Telenti-Asensio, Emilio García-Prieto, Mar Martínez-Suarez, Fernando Vázquez-Valdés, and et al. 2022. "COVID-19 Associated Pulmonary Aspergillosis (CAPA): Hospital or Home Environment as a Source of Life-Threatening Aspergillus fumigatus Infection?" Journal of Fungi 8, no. 3: 316. https://doi.org/10.3390/jof8030316
APA StylePeláez-García de la Rasilla, T., González-Jiménez, I., Fernández-Arroyo, A., Roldán, A., Carretero-Ares, J. L., García-Clemente, M., Telenti-Asensio, M., García-Prieto, E., Martínez-Suarez, M., Vázquez-Valdés, F., Melón-García, S., Caminal-Montero, L., Fernández-Simón, I., Mellado, E., & Sánchez-Núñez, M. L., on behalf of the HUCAPA Group. (2022). COVID-19 Associated Pulmonary Aspergillosis (CAPA): Hospital or Home Environment as a Source of Life-Threatening Aspergillus fumigatus Infection? Journal of Fungi, 8(3), 316. https://doi.org/10.3390/jof8030316