
Detection of Pneumocystis jirovecii in Patients with Severe COVID-19: Diagnostic and Therapeutic Challenges

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Gangneux, J.-P.; Bougnoux, M.-E.; Dannaoui, E.; Cornet, M.; Zahar, J.R. Invasive fungal diseases during COVID-19: We should be prepared. J. Mycol. Med. 2020, 30, 100971. [Google Scholar] [CrossRef] [PubMed]
- Baddley, J.W. COVID-19 Associated Pulmonary Aspergillosis: Do We Have the CAPAcity to Improve Outcomes? Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, ciab259. [Google Scholar] [CrossRef] [PubMed]
- Mang, S.; Kaddu-Mulindwa, D.; Metz, C.; Becker, A.; Seiler, F.; Smola, S.; Maßmann, A.; Becker, S.L.; Papan, C.; Bals, R.; et al. Pneumocystis jirovecii Pneumonia and SARS-CoV-2 Co-Infection in newly diagnosed HIV-1 infection. Clin. Infect. Dis. 2020, 72, 1487–1489. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, M.A.; Alberici, F.; Bossini, N.; Scolari, F.; Pascucci, F.; Tomasoni, G.; Caruso, A. Pneumocystis jirevocii and SARS-CoV-2 Co-Infection: A Common Feature in Transplant Recipients? Vaccines 2020, 8, 544. [Google Scholar] [CrossRef] [PubMed]
- Menon, A.A.; Berg, D.D.; Brea, E.J.; Deutsch, A.J.; Kidia, K.K.; Thurber, E.G.; Polsky, S.B.; Yeh, T.; Duskin, J.A.; Holliday, A.M.; et al. A Case of COVID-19 and Pneumocystis jirovecii Coinfection. Am. J. Respir. Crit. Care Med. 2020, 202, 136–138. [Google Scholar] [CrossRef] [PubMed]
- Blaize, M.; Mayaux, J.; Luyt, C.-E.; Lampros, A.; Fekkar, A. COVID-19-related Respiratory Failure and Lymphopenia Do Not Seem Associated with Pneumocystosis. Am. J. Respir. Crit. Care Med. 2020, 202, 1734–1736. [Google Scholar] [CrossRef] [PubMed]
- Alanio, A.; Dellière, S.; Voicu, S.; Bretagne, S.; Mégarbane, B. The presence of Pneumocystis jirovecii in critically ill patients with COVID-19. J. Infect. 2020, 82, 84–123. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Permpalung, N.; Kittipibul, V.; Mekraksakit, P.; Rattanawong, P.; Nematollahi, S.; Zhang, S.X.; Mehta Steinke, S. A Comprehensive evaluation of risk factors for Pneumocystis Jirovecii Pneumonia in adult solid organ transplant recipient. Transplantation 2020. [Google Scholar] [CrossRef]
- Menon, A.A.; Berg, D.D.; Gay, E.B. Reply to Blaize et al.: COVID-19–related Respiratory Failure and Lymphopenia Do Not Seem Associated with Pneumocystosis. Am. J. Respir. Crit. Care Med. 2020, 202, 1736–1737. [Google Scholar] [CrossRef]

{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | |
|---|---|---|---|---|
| Sex | F | M | M | M |
| Age | 80 | 70 | 83 | 80 |
| BMI | 36 | 35 | 28 | 28 |
| Underlying disease | Rheumatoid arthritis | Renal cell carcinoma in 2008, Autologous HSCT in 2013 for IgA myeloma complicated by amylosis, Ewing sarcoma with pulmonary metastases ongoing treatment, chronic kidney disease, pulmonary pneumocystosis six month ago | Diabetes mellitus, chronic heart failure, chronic kidney disease, atrial fibrillation, asthma | Diabetes mellitus, pacemaker for atrioventricular block, hypertension, transitory ischemic attack |
| Immunosuppressive treatment | Prednisone, Celecoxib | Cyclophosphamide, Doxorubicine | No | No |
| Pneumocystosis prophylaxis | No | TMP-SMX | No | No |
| Microbiological diagnosis | ||||
| COVID-19 | PCR on NPS | PCR on NPS | PCR on NPS | PCR on NPS |
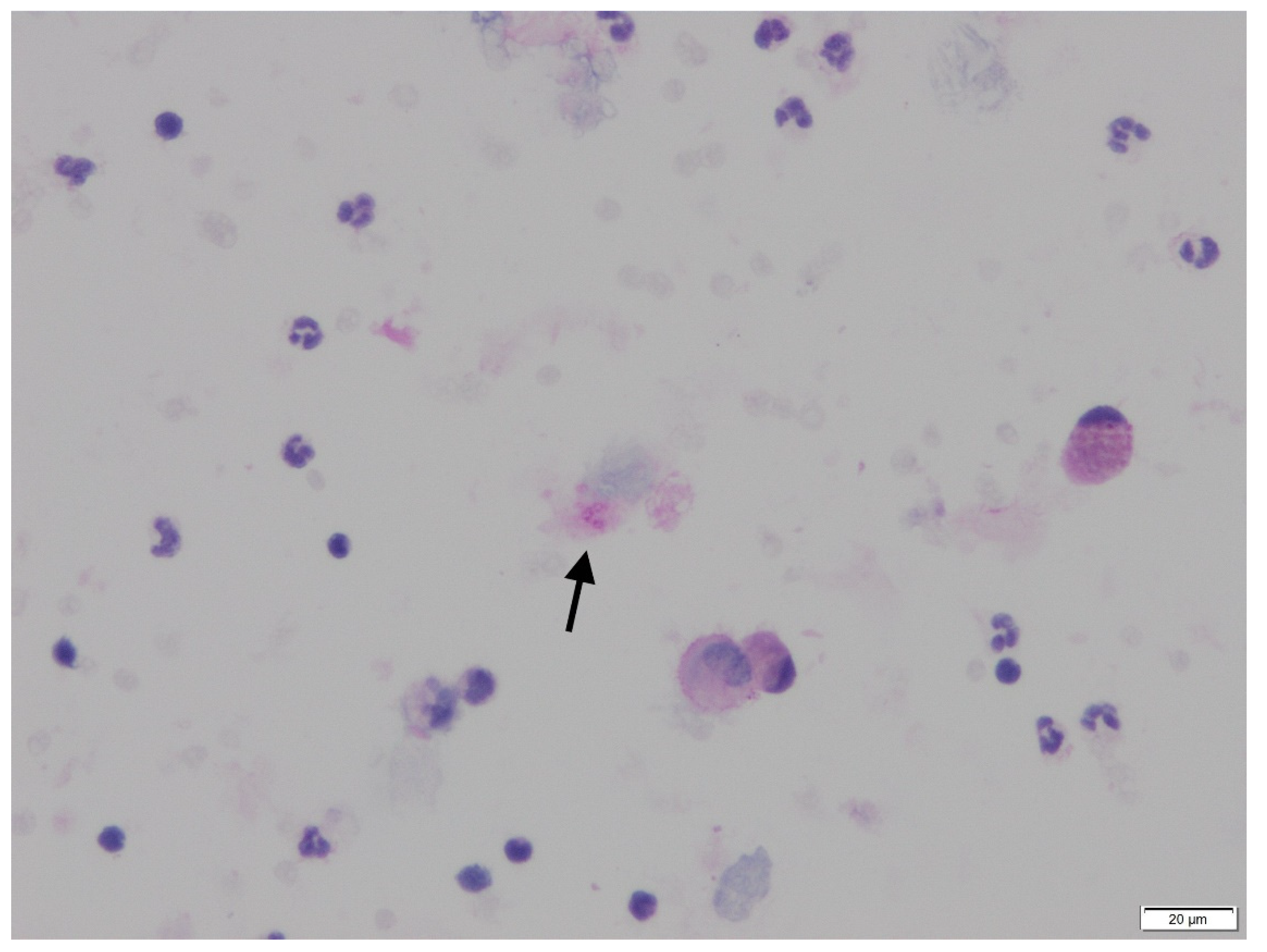
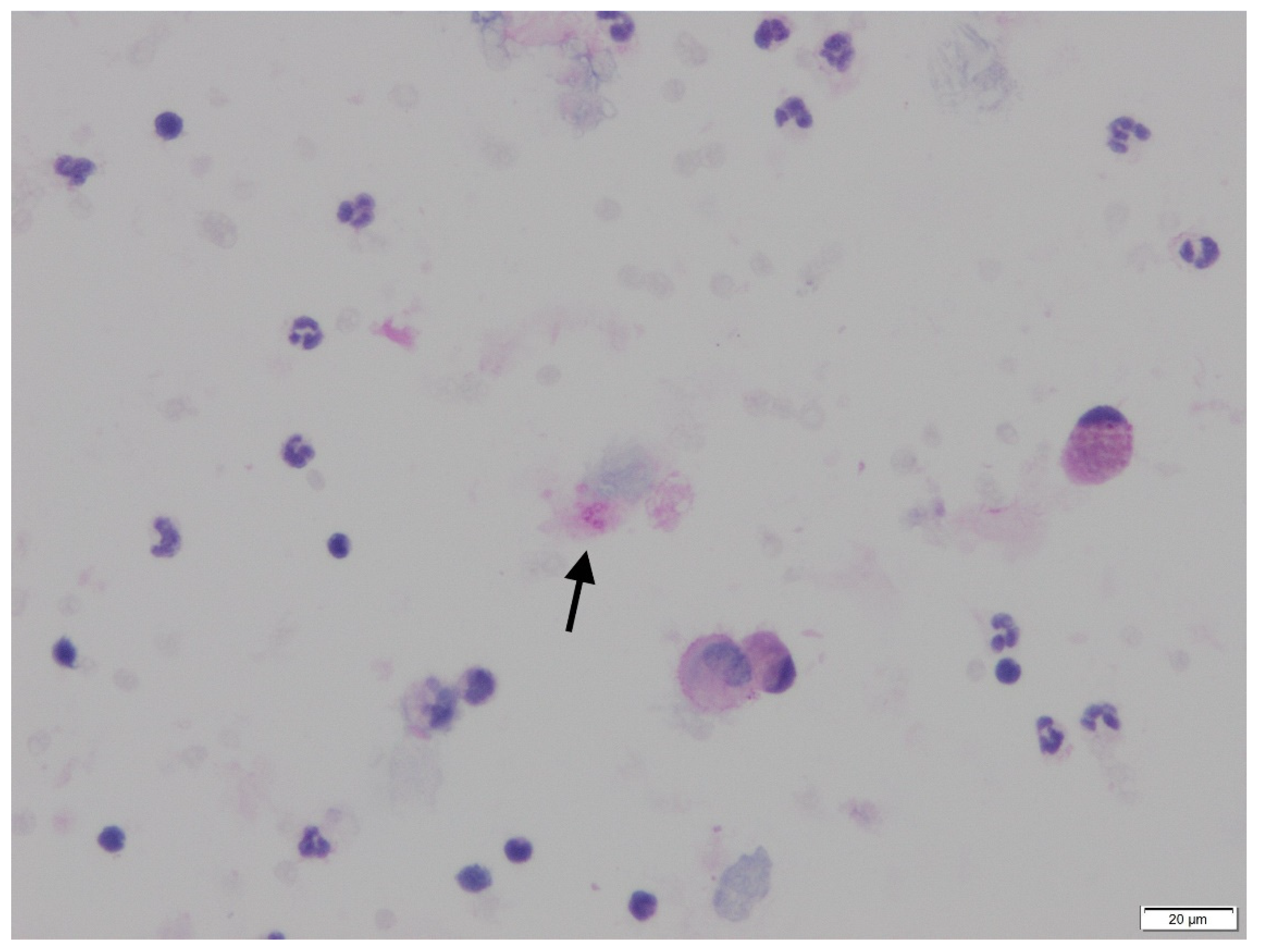
| P. jirovecii | PCR on BAL | PCR on tracheal aspirate | PCR and cytology on BAL | PCR on tracheal aspirate |
| Time between hospitalization and P. jirovecii PCR (days) | 1 | 1 | 40 | 25 |
| BDG (Fungitell Cape Cod.) | NR | NR | 123 pg/mL | 137 pg/mL |
| Biological data | ||||
| Lymphocytes count (cells/mmc) | 300 | 222 | 570 | 600 |
| LDH (IU/L) | NR | 811 | 437 | 267 |
| Clinical data | ||||
| Time from symptom onset to hospitalization | 5 days | 5 days | 5 days | 7 days |
| CT-scann | GGO >75%; AC | GGO > 75%; AC; nodules | GGO 50%; PE; crazy paving | GGO > 50%; AC; PE |
| ICU transfer * | Yes, day 1 | Yes, day 1 | No | Yes, day 30 |
| Ventilation | Mechanical | Mechanical | Low flow nasal oxygen | HFNC then mechanical |
| Steroid therapy | Yes | No | Yes | Yes |
| Pneumocystosis treatment | Yes, TMP-SMX | Yes, TMP-SMX | Yes, TMP-SMX | Yes, TMP-SMX, then atovaquone |
| Outcome | Death 18 days after admission | Death 3 days after admission | Death 44 days after admission | Death 44 days after admission |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerber, V.; Ruch, Y.; Chamaraux-Tran, T.-N.; Oulehri, W.; Schneider, F.; Lindner, V.; Greigert, V.; Denis, J.; Brunet, J.; Danion, F. Detection of Pneumocystis jirovecii in Patients with Severe COVID-19: Diagnostic and Therapeutic Challenges. J. Fungi 2021, 7, 585. https://doi.org/10.3390/jof7080585
Gerber V, Ruch Y, Chamaraux-Tran T-N, Oulehri W, Schneider F, Lindner V, Greigert V, Denis J, Brunet J, Danion F. Detection of Pneumocystis jirovecii in Patients with Severe COVID-19: Diagnostic and Therapeutic Challenges. Journal of Fungi. 2021; 7(8):585. https://doi.org/10.3390/jof7080585
Chicago/Turabian StyleGerber, Victor, Yvon Ruch, Thiên-Nga Chamaraux-Tran, Walid Oulehri, Francis Schneider, Veronique Lindner, Valentin Greigert, Julie Denis, Julie Brunet, and François Danion. 2021. "Detection of Pneumocystis jirovecii in Patients with Severe COVID-19: Diagnostic and Therapeutic Challenges" Journal of Fungi 7, no. 8: 585. https://doi.org/10.3390/jof7080585
APA StyleGerber, V., Ruch, Y., Chamaraux-Tran, T.-N., Oulehri, W., Schneider, F., Lindner, V., Greigert, V., Denis, J., Brunet, J., & Danion, F. (2021). Detection of Pneumocystis jirovecii in Patients with Severe COVID-19: Diagnostic and Therapeutic Challenges. Journal of Fungi, 7(8), 585. https://doi.org/10.3390/jof7080585