
Trichoderma longibrachiatum and Aspergillus fischeri Infection as a Cause of Skin Graft Failure in a Patient with Critical Burns after Liver Transplantation

 , and
, and 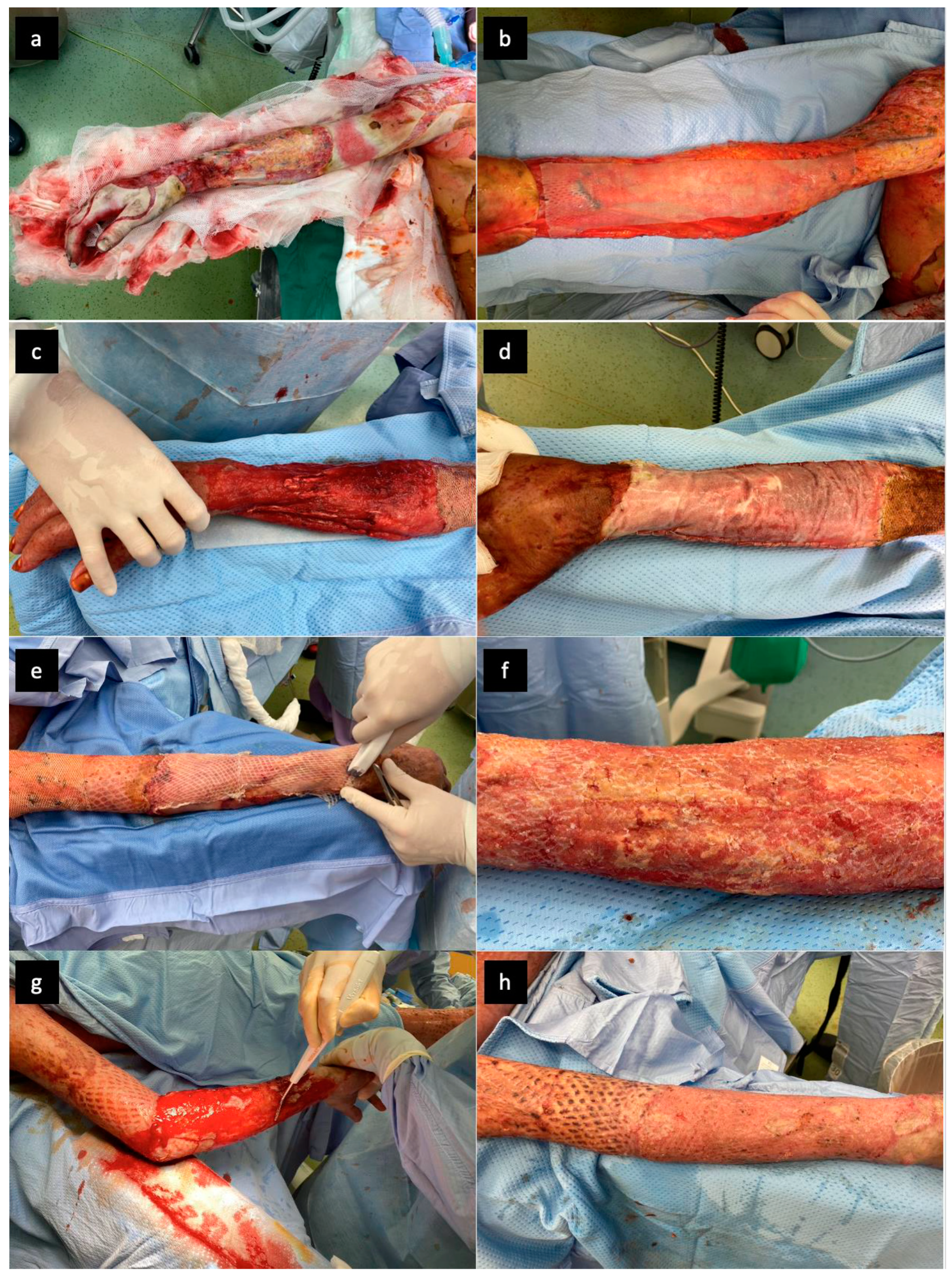{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
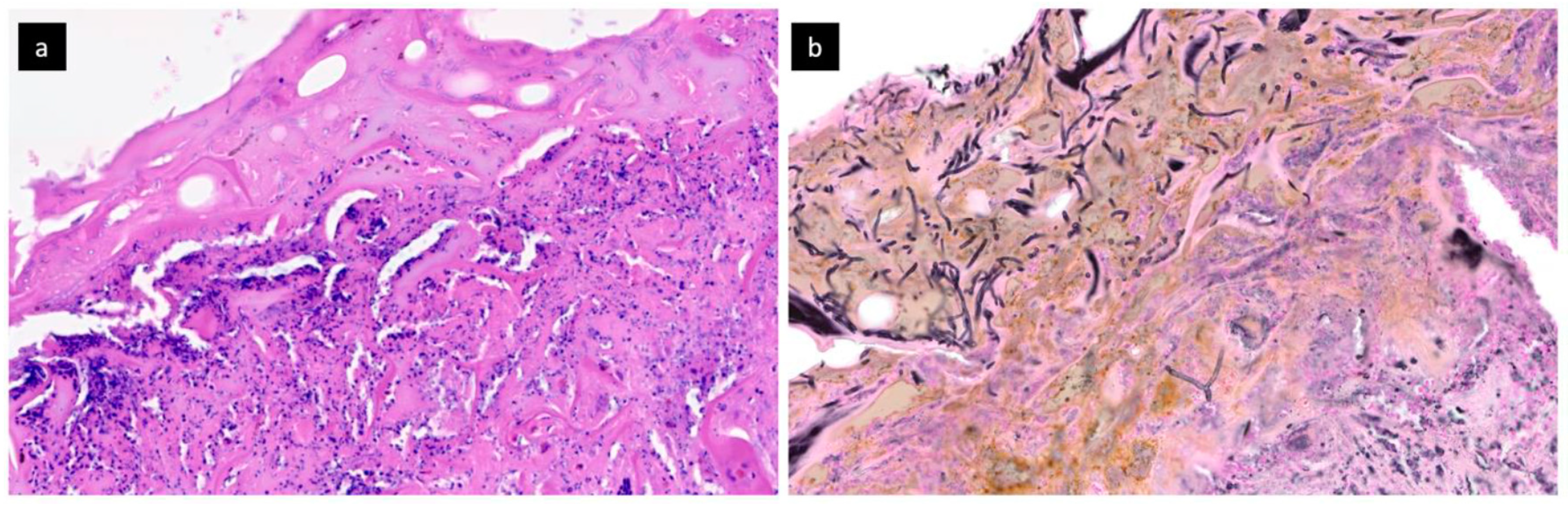
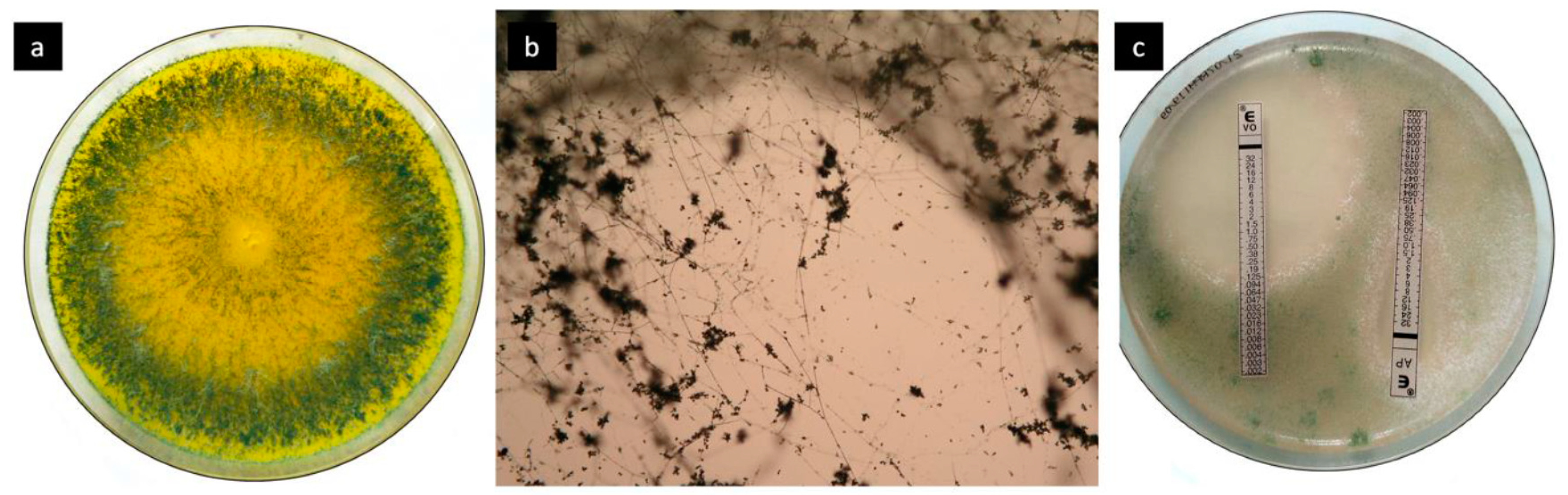
2. Case Report and Results
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kao, Y.; Loh, E.; Hsu, C.; Lin, H.; Huang, C.; Chou, Y.; Lien, C.; Tam, K. Fluid Resuscitation in Patients With Severe Burns: A Meta-analysis of Randomized Controlled Trials. Acad. Emerg. Med. 2018, 25, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Gacto-Sanchez, P. Surgical treatment and management of the severely burn patient: Review and update. Med. Intensiv. 2017, 41, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Vigani, A.; Culler, C.A. Systemic and Local Management of Burn Wounds. Vet. Clin. N. Am. Small Anim. Pract. 2017, 47, 1149–1163. [Google Scholar] [CrossRef]
- Rowley-Conwy, G. Management of burns in intensive and acute care. Nurs. Stand. 2013, 27, 63–64. [Google Scholar] [CrossRef]
- Spronk, I.; Legemate, C.; Oen, I.; Van Loey, N.; Polinder, S.; Van Baar, M. Health related quality of life in adults after burn injuries: A systematic review. PLoS ONE 2018, 13, e0197507. [Google Scholar] [CrossRef]
- Kool, M.B.; Geenen, R.; Egberts, M.R.; Wanders, H.; Van Loey, N.E. Patients’ perspectives on quality of life after burn. Burns 2017, 43, 747–756. [Google Scholar] [CrossRef]
- Shahrokhi, S.; Arno, A.; Jeschke, M.G. The use of dermal substitutes in burn surgery: Acute phase. Wound Repair Regen. 2014, 22, 14–22. [Google Scholar] [CrossRef]
- van der Veen, V.C.; van der Wal, M.B.; van Leeuwen, M.C.; Ulrich, M.M.; Middelkoop, E. Biological background of dermal substitutes. Burns 2010, 36, 305–321. [Google Scholar] [CrossRef]
- Uccioli, L.; Meloni, M.; Izzo, V.; Giurato, L. Use of Nevelia Dermal-Epidermal Regenerative Template in the Management of Ischemic Diabetic Foot Postsurgical Wounds. Int. J. Low. Extrem. Wounds 2020, 19, 282–288. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, B.; Orlandi, F.; D’Autilio, M.F.L.M.; Scioli, M.G.; Orlandi, A.; Cervelli, V.; Gentile, P. Long-term follow-up comparison of two different bi-layer dermal substitutes in tissue regeneration: Clinical outcomes and histological findings. Int. Wound J. 2018, 15, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Yiğitbaş, H. Our experience with dermal substitute Nevelia® in the treatment of severely burned patients. Turk. J. Trauma Emerg. Surg. 2019, 25, 520–526. [Google Scholar] [CrossRef]
- Ferrer, C.; Colom, F.; Fraseés, S.; Mulet, E.; Abad, J.L.; Alioó, J.L. Detection and Identification of Fungal Pathogens by PCR and by ITS2 and 5.8S Ribosomal DNA Typing in Ocular Infections. J. Clin. Microbiol. 2001, 39, 2873–2879. [Google Scholar] [CrossRef] [PubMed]
- Lipový, B.; Brychta, P.; Řihová, H.; Hanslianová, M.; Loskotová, A.; Jarkovský, J.; Kaloudová, Y.; Suchánek, I. Prevalence of infectious complications in burn patients requiring intensive care: Data from a pan-European study. Epidemiol. Mikrobiol. Imunol. 2016, 65, 25–32. [Google Scholar] [PubMed]
- Ceniceros, A.; Pértega, S.; Galeiras, R.; Mourelo, M.; Lopez, E.; Broullon, J.; Sousa, L.; Freire, D.; Pértega-Díaz, S. Predicting mortality in burn patients with bacteraemia. Infection 2015, 44, 215–222. [Google Scholar] [CrossRef]
- Egozi, D.; Hussein, K.; Filson, S.; Mashiach, T.; Ullmann, Y.; Raz-Pasteur, A. Bloodstream infection as a predictor for mortality in severe burn patients: An 11-year study. Epidemiol. Infect. 2013, 142, 2172–2179. [Google Scholar] [CrossRef]
- Church, D.; Elsayed, S.; Reid, O.; Winston, B.; Lindsay, R. Burn Wound Infections. Clin. Microbiol. Rev. 2006, 19, 403–434. [Google Scholar] [CrossRef]
- Lachiewicz, A.M.; Hauck, C.G.; Weber, D.J.; Cairns, A.B.; Van Duin, D. Bacterial Infections After Burn Injuries: Impact of Multidrug Resistance. Clin. Infect. Dis. 2017, 65, 2130–2136. [Google Scholar] [CrossRef]
- Horvath, E.E.; Murray, C.K.; Vaughan, G.M.; Chung, K.K.; Hospenthal, D.R.; Wade, C.E.; Holcomb, J.B.; Wolf, S.; Mason, A.D.; Cancio, L.C. Fungal Wound Infection (Not Colonization) Is Independently Associated with Mortality in Burn Patients. Ann. Surg. 2007, 245, 978–985. [Google Scholar] [CrossRef]
- Becker, W.K.; Cioffi, W.G.; McManus, A.T.; Kim, S.H.; McManus, W.F.; Mason, A.D.; Pruitt, B.A. Fungal Burn Wound Infection. Arch. Surg. 1991, 126, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Mousa, A.H. Fungal infection of burn wounds in patients with open and occlusive treatment methods. East. Mediterr. Health J. 1999, 5, 333–336. [Google Scholar]
- Murray, C.K.; Loo, F.L.; Hospenthal, D.R.; Cancio, L.C.; Jones, J.A.; Kim, S.H.; Holcomb, J.B.; Wade, C.E.; Wolf, S. Incidence of systemic fungal infection and related mortality following severe burns. Burns 2008, 34, 1108–1112. [Google Scholar] [CrossRef]
- Howard, P.; Cancio, L.; McManus, A.; Goodwin, C.; Kim, S.; Pruitt, B. What’s new in burn-associated infections? Curr. Surg. 1999, 56, 397–405. [Google Scholar] [CrossRef]
- Schofield, C.M.; Murray, C.K.; Horvath, E.E.; Cancio, L.C.; Kim, S.H.; Wolf, S.; Hospenthal, D.R. Correlation of culture with histopathology in fungal burn wound colonization and infection. Burns 2007, 33, 341–346. [Google Scholar] [CrossRef]
- Schaal, J.; Leclerc, T.; Soler, C.; Donat, N.; Cirrode, A.; Jault, P.; Bargues, L. Epidemiology of filamentous fungal infections in burned patients: A French retrospective study. Burns 2015, 41, 853–863. [Google Scholar] [CrossRef]
- Katz, T.; Wasiak, J.; Cleland, H.; Padiglione, A. Incidence of non-candidal fungal infections in severe burn injury: An Australian perspective. Burns 2014, 40, 881–886. [Google Scholar] [CrossRef]
- Capoor, M.R.; Gupta, S.; Sarabahi, S.; Mishra, A.; Tiwari, V.K.; Aggarwal, P. Epidemiological and clinico-mycological profile of fungal wound infection from largest burn centre in Asia. Mycoses 2011, 55, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Rosanova, M.T.; Brizuela, M.; Villasboas, M.; Guarracino, F.; Alvarez, V.; Santos, P.; Finquelievich, J. Fusarium spp infections in a pediatric burn unit: Nine years of experience. Braz. J. Infect. Dis. 2016, 20, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Douglas, A.P.; Chen, S.C.-A.; Slavin, M.A. Emerging infections caused by non- Aspergillus filamentous fungi. Clin. Microbiol. Infect. 2016, 22, 670–680. [Google Scholar] [CrossRef] [PubMed]
- Chouaki, T.; Lavarde, V.; Lachaud, L.; Raccurt, C.P.; Hennequin, C. Invasive Infections Due toTrichodermaSpecies: Report of 2 Cases, Findings of In Vitro Susceptibility Testing, and Review of the Literature. Clin. Infect. Dis. 2002, 35, 1360–1367. [Google Scholar] [CrossRef] [PubMed]
- Kredics, L.; Antal, Z.; Dóczi, I.; Manczinger, L.; Kevei, F.; Nagy, E. Clinical importance of the genus Trichoderma. Acta Microbiol. Immunol. Hung. 2003, 50, 105–117. [Google Scholar] [CrossRef]
- Trabelsi, S.; Hariga, D.; Khaled, S. First case of Trichoderma longibrachiatum infection in a renal transplant recipient in Tunisia and review of the literature. Tunis Med. 2010, 88, 52–57. [Google Scholar]
- Chen, S.C.-A.; Blyth, C.C.; Sorrell, T.C.; Slavin, M. Pneumonia and Lung Infections due to Emerging and Unusual Fungal Pathogens. Semin. Respir. Crit. Care Med. 2011, 32, 703–716. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.; Groll, A.; Hiemenz, J.; Fleming, R.; Roilides, E.; Anaissie, E. Infections due to emerging and uncommon medically important fungal pathogens. Clin. Microbiol. Infect. 2004, 10, 48–66. [Google Scholar] [CrossRef]
- Sandoval-Denis, M.; Sutton, D.A.; Cano-Lira, J.F.; Gené, J.; Fothergill, A.W.; Wiederhold, N.P.; Guarro, J. Phylogeny of the Clinically Relevant Species of the Emerging Fungus Trichoderma and Their Antifungal Susceptibilities. J. Clin. Microbiol. 2014, 52, 2112–2125. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, H.; Kusne, S.; Sutton, D.A.; Manez, R.; Carrau, R.; Nichols, K.A.L.; Skedros, D.; Todo, S.; Rinaldi, M.G.; Nichols, L.; et al. Acute invasive sinusitis due to Trichoderma longibrachiatum in a liver and small bowel transplant recipient. Clin. Infect. Dis. 1998, 26, 487–489. [Google Scholar] [CrossRef] [PubMed]
- Kerr, C.M.; Perfect, J.R.; Craven, P.C.; Jorgensen, J.H.; Drutz, D.J.; Shelburne, J.D.; Gallis, H.A.; Gutman, R.A. Fungal Peritonitis in Patients on Continuous Ambulatory Peritoneal Dialysis. Ann. Intern. Med. 1983, 99, 334–337. [Google Scholar] [CrossRef]
- Piens, M.A.; Celard, M.; de Monbrison, F.; Grando, J.; Vandenesch, F.; Mottolese, C.; Picot, S. Trichoderma infection of cerebro-spinal fluid shunt device in a non immunocompromised patient. J. Mycol. Med. 2004, 14, 49–51. [Google Scholar]
- Ranque, S.; Garcia-Hermoso, D.; Michel-Nguyen, A.; Dumon, H. Isolation of Trichoderma atroviride from a liver transplant. J. Mycol. Méd. 2008, 18, 234–236. [Google Scholar] [CrossRef]
- Seguin, P.; Degeilh, B.; Grulois, I.; Gacouin, A.; Maugendre, S.; Dufour, T.; Dupont, B.; Camus, C. Successful treatment of a brain abscess due toTrichoderma longibrachiatum after surgical resection. Eur. J. Clin. Microbiol. Infect. Dis. 1995, 14, 445–448. [Google Scholar] [CrossRef]
- Tascini, C.; Cardinali, G.; Barletta, V.; Di Paolo, A.; Leonildi, A.; Zucchelli, G.; Corte, L.; Colabella, C.; Roscini, L.; Consorte, A.; et al. First Case of Trichoderma longibrachiatum CIED (Cardiac Implantable Electronic Device)-Associated Endocarditis in a Non-immunocompromised Host: Biofilm Removal and Diagnostic Problems in the Light of the Current Literature. Mycopathologia 2015, 181, 297–303. [Google Scholar] [CrossRef]
- Struck, M.; Gille, J. Fungal infections in burns: A comprehensive review. Ann. Burn. Fire Disasters 2013, 26, 147–153. [Google Scholar]
- Kyriopoulos, E.; Kyriakopoulos, A.; Karonidis, A.; Gravvanis, A.; Gamatsi, I.; Tsironis, C.; Tsoutsos, D. Burn injuries and soft tissue traumas complicated by mucormycosis infection: A report of six cases and review of the literature. Ann. Burn. Fire Disasters 2015, 28, 280–287. [Google Scholar]
- Gonzalez, S.R.; Wolter, K.G.; Yuen, J.C. Infectious Complications Associated with the Use of Integra: A Systematic Review of the Literature. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2869. [Google Scholar] [CrossRef]
- Peck, M.D.; Kessler, M.; Meyer, A.A.; Morris, P.A.B. A Trial of the Effectiveness of Artificial Dermis in the Treatment of Patients with Burns Greater Than 45% Total Body Surface Area. J. Trauma Acute Care Surg. 2002, 52, 971–978. [Google Scholar] [CrossRef]
- Munster, A.M.; Smith-Meek, M.; Shalom, A. Acellular allograft dermal matrix: Immediate or delayed epidermal coverage? Burns 2001, 27, 150–153. [Google Scholar] [CrossRef]
- Branski, L.K.; Herndon, D.N.; Pereira, C.; Mlcak, R.P.; Celis, M.M.; Lee, J.O.; Sanford, A.P.; Norbury, W.B.; Zhang, X.-J.; Jeschke, M.G. Longitudinal assessment of Integra in primary burn management: A randomized pediatric clinical trial. Crit. Care Med. 2007, 35, 2615–2623. [Google Scholar] [CrossRef]
- Bloemen, M.C.T.; Van Der Wal, M.B.A.; Verhaegen, P.D.H.M.; Nieuwenhuis, M.; Van Baar, M.E.; Van Zuijlen, P.P.M.; Middelkoop, E. Clinical effectiveness of dermal substitution in burns by topical negative pressure: A multicenter randomized controlled trial. Wound Repair Regen. 2012, 20, 797–805. [Google Scholar] [CrossRef]
- Lagus, H.; Sarlomo-Rikala, M.; Böhling, T.; Vuola, J. Prospective study on burns treated with Integra®, a cellulose sponge and split thickness skin graft: Comparative clinical and histological study—Randomized controlled trial. Burns 2013, 39, 1577–1587. [Google Scholar] [CrossRef]
- Bootun, R. Effects of immunosuppressive therapy on wound healing. Int. Wound J. 2012, 10, 98–104. [Google Scholar] [CrossRef]
- Zhang, H.; Qu, W.; Nazzal, M.; Ortiz, J. Burn patients with history of kidney transplant experience increased incidence of wound infection. Burns 2020, 46, 609–615. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lipový, B.; Raška, F.; Kocmanová, I.; Hanslianová, M.; Hladík, M.; Holoubek, J.; Bezdíček, M.; Macháček, C. Trichoderma longibrachiatum and Aspergillus fischeri Infection as a Cause of Skin Graft Failure in a Patient with Critical Burns after Liver Transplantation. J. Fungi 2021, 7, 487. https://doi.org/10.3390/jof7060487
Lipový B, Raška F, Kocmanová I, Hanslianová M, Hladík M, Holoubek J, Bezdíček M, Macháček C. Trichoderma longibrachiatum and Aspergillus fischeri Infection as a Cause of Skin Graft Failure in a Patient with Critical Burns after Liver Transplantation. Journal of Fungi. 2021; 7(6):487. https://doi.org/10.3390/jof7060487
Chicago/Turabian StyleLipový, Břetislav, Filip Raška, Iva Kocmanová, Markéta Hanslianová, Martin Hladík, Jakub Holoubek, Matěj Bezdíček, and Ctirad Macháček. 2021. "Trichoderma longibrachiatum and Aspergillus fischeri Infection as a Cause of Skin Graft Failure in a Patient with Critical Burns after Liver Transplantation" Journal of Fungi 7, no. 6: 487. https://doi.org/10.3390/jof7060487
APA StyleLipový, B., Raška, F., Kocmanová, I., Hanslianová, M., Hladík, M., Holoubek, J., Bezdíček, M., & Macháček, C. (2021). Trichoderma longibrachiatum and Aspergillus fischeri Infection as a Cause of Skin Graft Failure in a Patient with Critical Burns after Liver Transplantation. Journal of Fungi, 7(6), 487. https://doi.org/10.3390/jof7060487