Comparison of Two Commercial Colorimetric Broth Microdilution Tests for Candida Susceptibility Testing: Sensititre YeastOne versus MICRONAUT-AM

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Intralaboratory Reproducibility
3.2. Essential Agreement
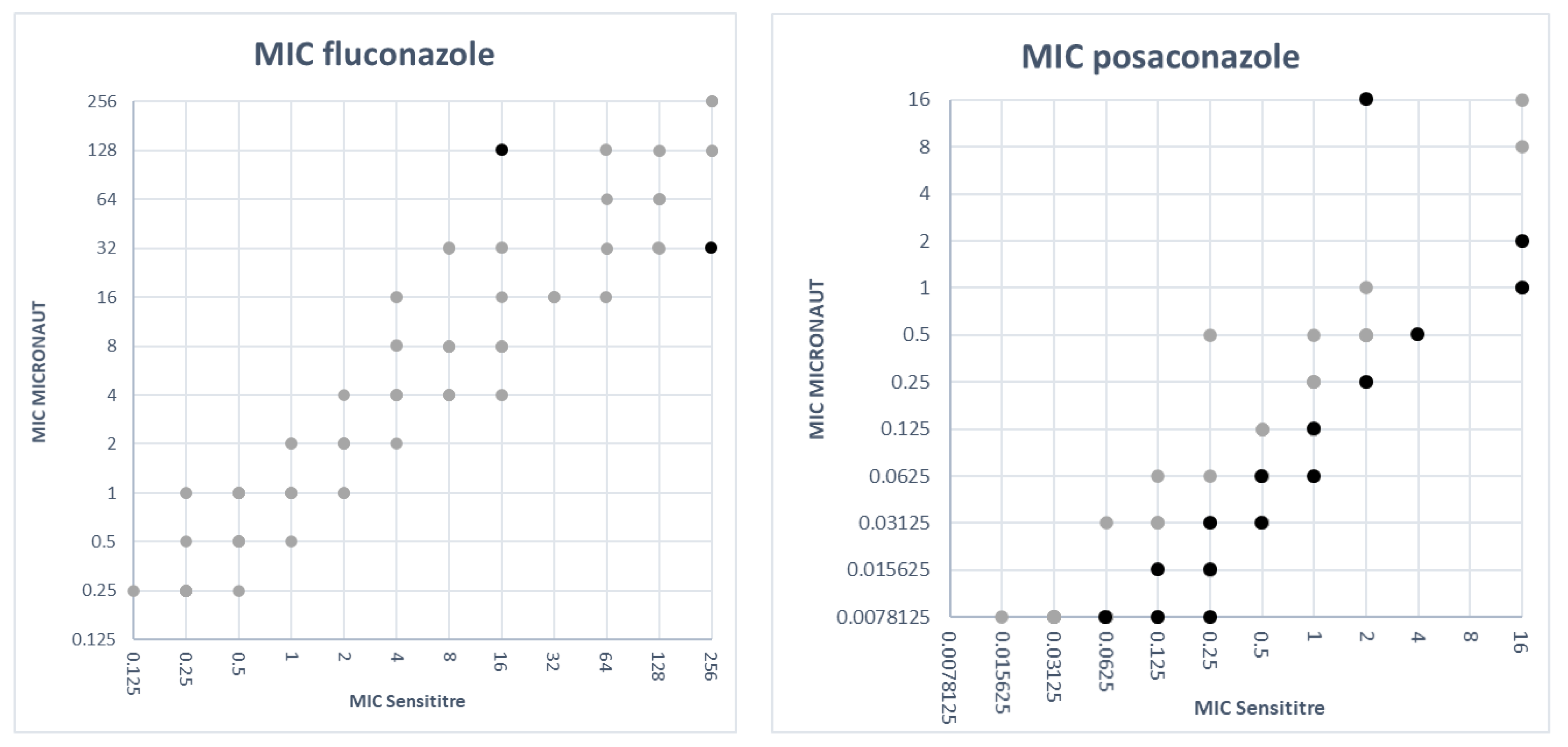
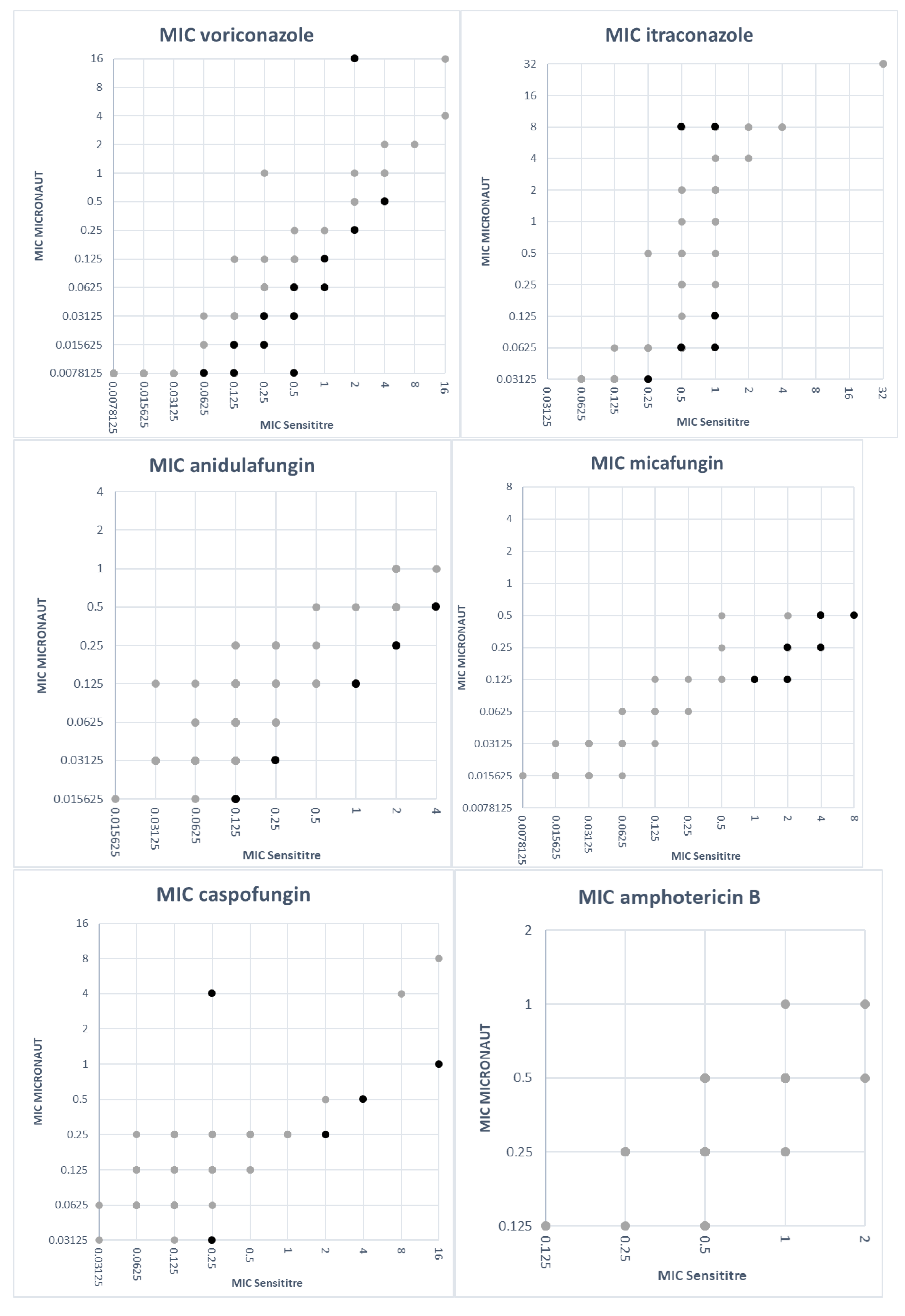
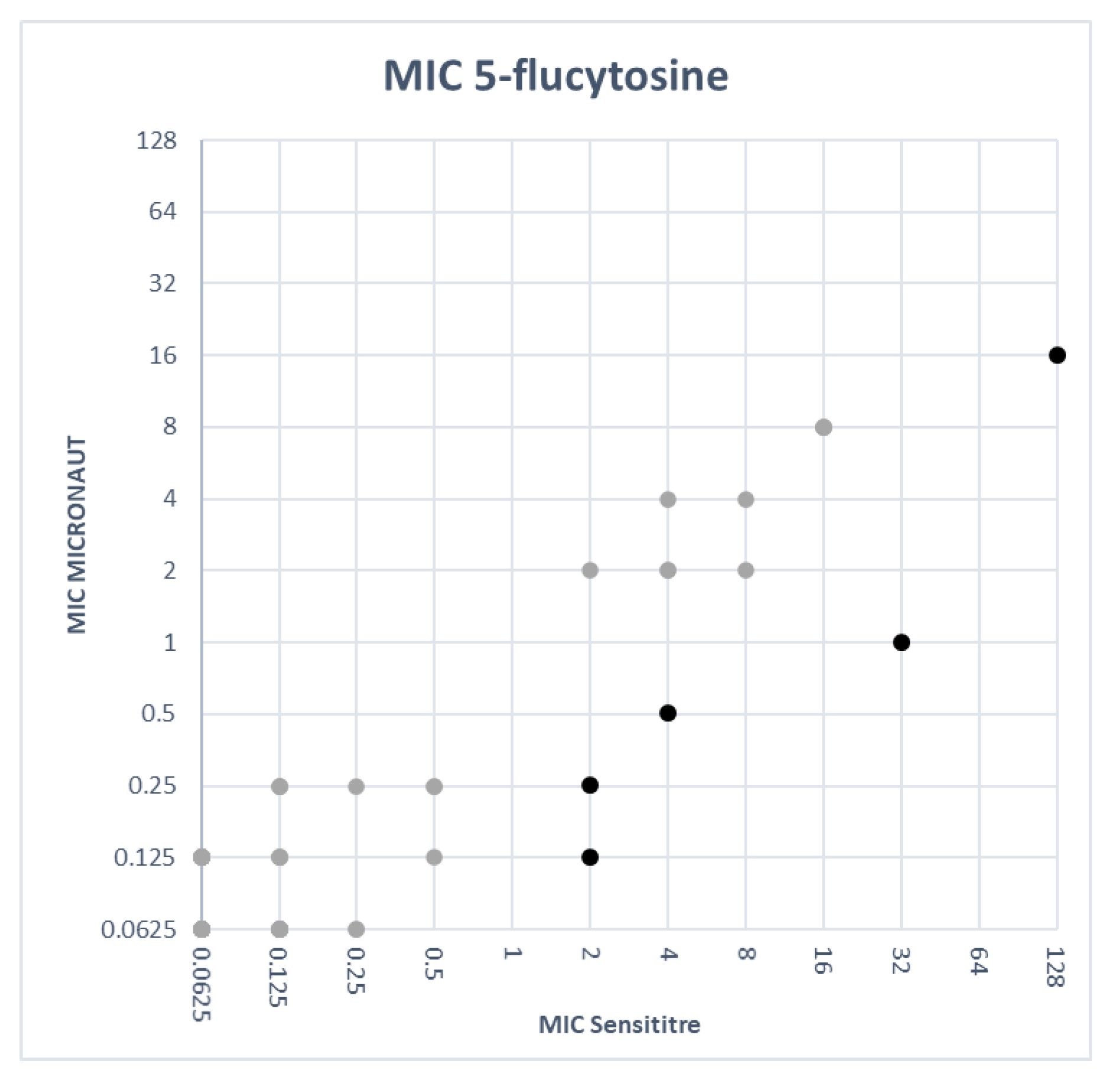
3.3. Comparison of MIC Values
3.4. Categorical Agreement
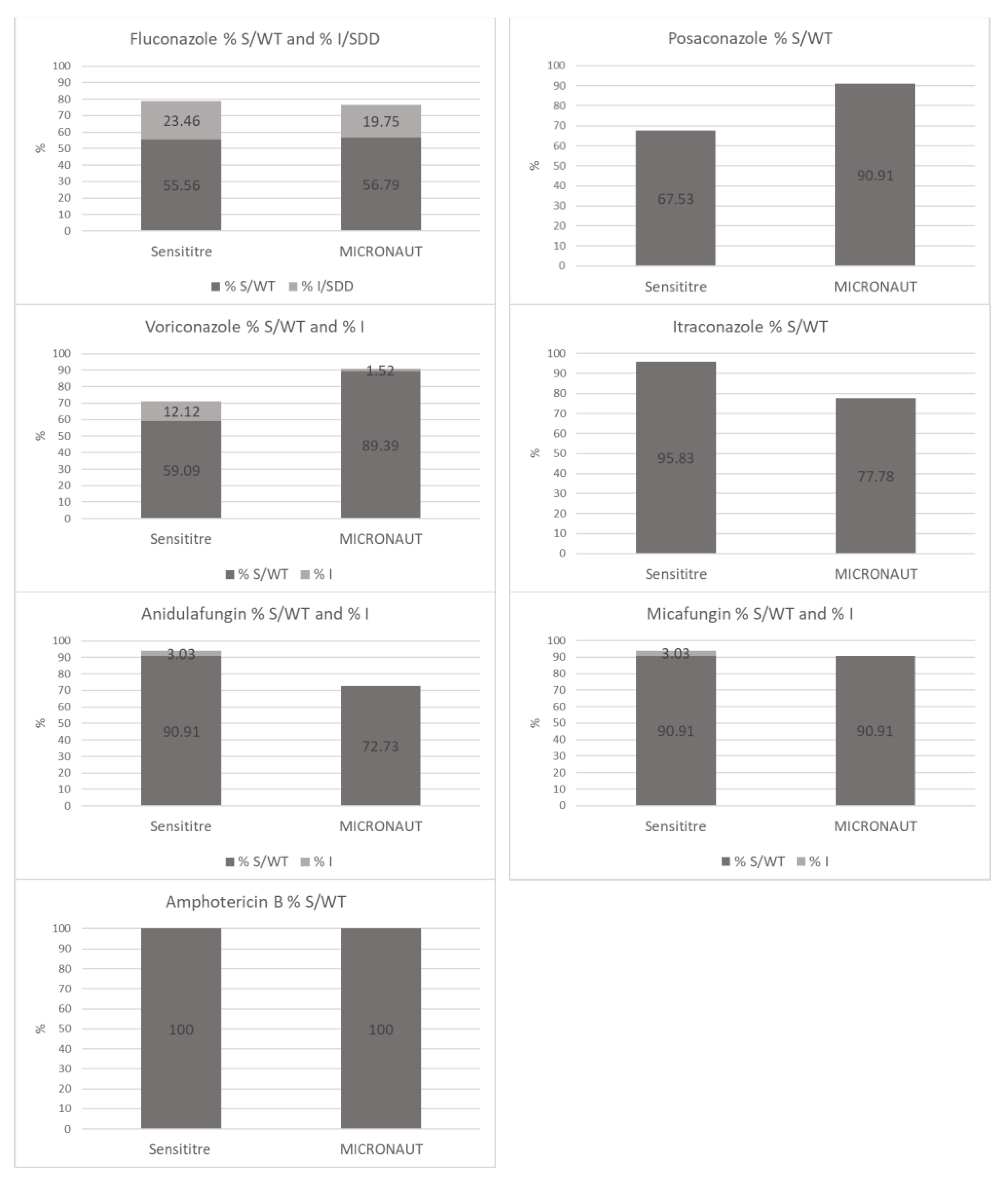
3.5. Comparison of Susceptibility Ratios
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References and Notes
- OPATHY Consortium; Gabaldón, T. Recent Trends in Molecular Diagnostics of Yeast Infections: From PCR to NGS. FEMS Microbiol. Rev. 2019, 43, 517–547. [Google Scholar] [CrossRef] [PubMed]
- Zomorodian, K.; Bandegani, A.; Mirhendi, H.; Pakshir, K.; Alinejhad, N.; Poostforoush Fard, A. In Vitro Susceptibility and Trailing Growth Effect of Clinical Isolates of Candida Species to Azole Drugs. Jundishapur J. Microbiol. 2016, 9, e28666. [Google Scholar] [CrossRef] [PubMed]
- Kucukates, E.; Gultekin, N.; Alisan, Z.; Hondur, N.; Ozturk, R. Identification of Candida Species and Susceptibility Testing with Sensititre YeastOne Microdilution Panel to 9 Antifungal Agents. Saudi Med. J. 2016, 37, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Canton, E.; Peman, J.; Iniguez, C.; Hervas, D.; Lopez-Hontangas, J.L.; Pina-Vaz, C.; Camarena, J.J.; Campos-Herrero, I.; Garcia-Garcia, I.; Garcia-Tapia, A.M.; et al. Epidemiological Cutoff Values for Fluconazole, Itraconazole, Posaconazole, and Voriconazole for Six Candida Species as Determined by the Colorimetric Sensititre YeastOne Method. J. Clin. Microbiol. 2013, 51, 2691–2695. [Google Scholar] [CrossRef]
- Sanguinetti, M.; Posteraro, B. Susceptibility Testing of Fungi to Antifungal Drugs. J. Fungi 2018, 4, 110. [Google Scholar] [CrossRef] [PubMed]
- Ksiezopolska, E.; Gabaldón, T. Evolutionary Emergence of Drug Resistance in Candida Opportunistic Pathogens. Genes 2018, 9, 461. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, E.; Hammarström, H.; Ataollahy, N.; Kondori, N. Species Distribution and Antifungal Drug Susceptibilities of Yeasts Isolated from the Blood Samples of Patients with Candidemia. Sci. Rep. 2019, 9, 3838. [Google Scholar] [CrossRef] [PubMed]
- Alexander, B.D.; Byrne, T.C.; Smith, K.L.; Hanson, K.E.; Anstrom, K.J.; Perfect, J.R.; Reller, L.B. Comparative Evaluation of Etest and Sensititre YeastOne Panels against the Clinical and Laboratory Standards Institute M27-A2 Reference Broth Microdilution Method for Testing Candida Susceptibility to Seven Antifungal Agents. J. Clin. Microbiol. 2007, 45, 698–706. [Google Scholar] [CrossRef]
- Binder, U.; Aigner, M.; Risslegger, B.; Hörtnagl, C.; Lass-Flörl, C.; Lackner, M. Minimal Inhibitory Concentration (MIC)-Phenomena in Candida Albicans and Their Impact on the Diagnosis of Antifungal Resistance. J. Fungi 2019, 5, 83. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Castanheira, M.; Messer, S.A.; Rhomberg, P.R.; Jones, R.N. Comparison of EUCAST and CLSI Broth Microdilution Methods for the Susceptibility Testing of 10 Systemically Active Antifungal Agents When Tested against Candida spp. Diagn. Microbiol. Infect. Dis. 2014, 79, 198–204. [Google Scholar] [CrossRef]
- Aigner, M.; Erbeznik, T.; Gschwentner, M.; Lass-Flörl, C. Etest and Sensititre YeastOne Susceptibility Testing of Echinocandins against Candida Species from a Single Center in Austria. Antimicrob. Agents Chemother. 2017, 61, e00512-17. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A.; Turnidge, J.; Alastruey-Izquierdo, A.; Botterel, F.; Canton, E.; Castro, C.; Chen, Y.-C.; Chen, Y.; Chryssanthou, E.; Dannaoui, E.; et al. Method-Dependent Epidemiological Cutoff Values for Detection of Triazole Resistance in Candida and Aspergillus Species for the Sensititre YeastOne Colorimetric Broth and Etest Agar Diffusion Methods. Antimicrob. Agents Chemother. 2018, 63, e01651-18. [Google Scholar] [CrossRef]
- Linares, M.J.; Charriel, G.; Solis, F.; Casal, M. Comparison of Two Microdilution Methods for Testing Susceptibility of Candida Spp. to Voriconazole. J. Clin. Microbiol. 2004, 42, 899–902. [Google Scholar] [CrossRef] [PubMed]
- Thermo Fisher ScientificTM. SENSITITRE® YEASTONE® For in Vitro Diagnostic Use. MCS Diagnostics. 2012. Available online: https://docplayer.net/21149741-Sensititre-yeastone-for-in-vitro-diagnostic-use.html (accessed on 18 January 2021).
- MERLIN a Bruker Company. ©MERLIN Diagnostika GmbH. MICRONAUT-AM. 2018. Provided by the Manufacturer.
- MERLIN a Bruker Company. ©MERLIN Diagnostika GmbH. Certificate of Quality. MICRONAUT-AM Antifungal Agents MIC. Catalognumber: E1-831-040. LOT: 190409831A. Expiry Date: 9 April 2021. Date of Release: 26 April 2019. Provided by the Manufacturer.
- SensititreTM YeastOneTM YO10 AST Plate. Available online: https://www.thermofisher.com/order/catalog/product/YO10 (accessed on 18 January 2021).
- Rampersad, S.N. Multiple Applications of Alamar Blue as an Indicator of Metabolic Function and Cellular Health in Cell Viability Bioassays. Sensors 2012, 12, 12347–12360. [Google Scholar] [CrossRef] [PubMed]
- Yajko, D.M.; Madej, J.J.; Lancaster, M.V.; Sanders, C.A.; Cawthon, V.L.; Gee, B.; Babst, A.; Hadley, W.K. Colorimetric Method for Determining MICs of Antimicrobial Agents for Mycobacterium Tuberculosis. J. Clin. Microbiol. 1995, 33, 2324–2327. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Messer, S.A.; Hollis, R.J.; Espinel-Ingroff, A.; Ghannoum, M.A.; Plavan, H.; Killian, S.B.; Knapp, C.C. Multisite Reproducibility of MIC Results by the Sensititre® YeaStone Colorimetric Antifungal Susceptibility Panel. Diagn. Microbiol. Infect. Dis. 1998, 31, 543–547. [Google Scholar] [CrossRef]
- Clark, R.B.; Lewinski, M.A.; Loeffelholz, M.J.; Tibbetts, R.J. Cumitech 31A: Verification and Validation of Procedures in the Clinical Microbiology Laboratory; American Society for Microbiology: Washington, DC, USA, 2009; ISBN 978-1-55581-530-1. [Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts, 4th ed.; CLSI standard M27 (ISBN 1-56238-826-6 [Print]; ISBN 1-56238-827-4 [Electronic]); Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2017. [Google Scholar]
- Arendrup, M.C.; Meletiadis, J.; Mouton, J.W.; Lagrou, K.; Hamal, P.; Guinea, J. Subcommittee on Antifungal Susceptibility Testing (AFST) of the ESCMID European Committee for Antimicrobial Susceptibility Testing (EUCAST). EUCAST DEFINITIVE DOCUMENT E.DEF 7.3.2. Method for the Determination of Broth Dilution Minimum Inhibitory Concentrations of Antifungal Agents for Yeasts; 2020; p. 21. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Files/EUCAST_E_Def_7.3.2_Yeast_testing_definitive_revised_2020.pdf (accessed on 26 January 2021).
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antifungal Susceptibility Testing of Yeasts, 1st ed.; CLSI supplement M60 (ISBN 1-56238-828-2 [Print]; ISBN 1-56238-829-0 [Electronic]); Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2017. [Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Epidemiological Cutoff Values for Antifungal Susceptibility Testing, 3rd ed.; CLSI supplement M59 (ISBN 978-1-68440-080-5 [Print]; ISBN 978-1-68440-081-2 [Electronic]); Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020. [Google Scholar]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs for Antifungal Agents, Version 10.0, 2020. Available online: http://www.eucast.org/astoffungi/clinicalbreakpointsforantifungals/ (accessed on 26 January 2021).
- The European Committee on Antimicrobial Susceptibility Testing. Overview of Antifungal ECOFFs and Clinical Breakpoints for Yeasts, Moulds and Dermatophytes Using the EUCAST E.Def 7.3, E.Def 9.3 and E.Def 11.0 Procedures. Version 2, 2020. Available online: http://www.eucast.org (accessed on 26 January 2021).
- Espinel-Ingroff, A.; Pfaller, M.; Messer, S.A.; Knapp, C.C.; Killian, S.; Norris, H.A.; Ghannoum, M.A. Multicenter Comparison of the Sensititre YeastOne Colorimetric Antifungal Panel with the National Committee for Clinical Laboratory Standards M27-A Reference Method for Testing Clinical Isolates of Common and Emerging Candida spp., Cryptococcus spp., and Other Yeasts and Yeast-Like Organisms. J. Clin. Microbiol. 1999, 37, 591–595. [Google Scholar] [CrossRef]
- Cuenca-Estrella, M.; Gomez-Lopez, A.; Mellado, E.; Rodriguez-Tudela, J.L. Correlation between the Procedure for Antifungal Susceptibility Testing for Candida spp. of the European Committee on Antibiotic Susceptibility Testing (EUCAST) and Four Commercial Techniques. Clin. Microbiol. Infect. 2005, 11, 486–492. [Google Scholar] [CrossRef][Green Version]
- Pfaller, M.A.; Espinel-Ingroff, A.; Jones, R.N. Clinical Evaluation of the Sensititre YeastOne Colorimetric Antifungal Plate for Antifungal Susceptibility Testing of the New Triazoles Voriconazole, Posaconazole, and Ravuconazole. J. Clin. Microbiol. 2004, 42, 4577–4580. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mellinghoff, S.C.; Cornely, O.A.; Jung, N. Essentials in Candida Bloodstream Infection. Infection 2018, 46, 897–899. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antifungal Agent | Species | CLSI MIC CBP (mg/L) | CLSI ECV (mg/L) | EUCAST MIC CBP (mg/L) | EUCAST ECV (mg/L) |
|---|---|---|---|---|---|
| Fluconazole | C. glabrata | SDD ≤ 32, R ≥ 64 | - | S ≤ 0.001, R > 16 | - |
| C. albicans | S ≤ 2, SDD 4, R ≥ 8 | - | S ≤ 2, R > 4 | - | |
| C. parapsilosis | S ≤ 2, SDD 4, R ≥ 8 | - | S ≤ 2, R > 4 | - | |
| C. tropicalis | S ≤ 2, SDD 4, R ≥ 8 | - | S ≤ 2, R > 4 | - | |
| C. lusitaniae | - | 1 | - | - | |
| C. dubliniensis | - | 0.5 | S ≤ 2, R > 4 | - | |
| C. guilliermondii | - | 8 | IE | 16 | |
| C. kefyr | - | 1 | - | [1] | |
| Non-species related | - | - | S ≤ 2, R > 4 | - | |
| Posaconazole | C. glabrata | - | 1 | IE | 1 |
| C. albicans | - | 0.06 | S ≤ 0.06, R > 0.06 | - | |
| C. parapsilosis | - | 0.25 | S ≤ 0.06, R > 0.06 | - | |
| C. tropicalis | - | 0.12 | S ≤ 0.06, R > 0.06 | - | |
| C. lusitaniae | - | 0.06 | - | - | |
| C. dubliniensis | - | 0.12 | S ≤ 0.06, R > 0.06 | - | |
| C. krusei | - | 0.5 | IE | 0.5 | |
| C. guilliermondii | - | 0.5 | IE | 0.25 | |
| Non-species related | - | - | IE | - | |
| Voriconazole | C. glabrata | - | 0.25 | IE | 1 |
| C. albicans | S ≤ 0.12, I 0.25–0.5, R ≥ 1 | - | S ≤ 0.06, R > 0.25 | - | |
| C. parapsilosis | S ≤ 0.12, I 0.25–0.5, R ≥ 1 | - | S ≤ 0.125, R > 0.25 | - | |
| C. tropicalis | S ≤ 0.12, I 0.25–0.5, R ≥ 1 | - | S ≤ 0.125, R > 0.25 | - | |
| C. lusitaniae | - | - | - | - | |
| C. dubliniensis | - | - | S ≤ 0.06, R > 0.25 | - | |
| C. krusei | S ≤ 0.5, I 1, R ≥ 2 | - | IE | 1 | |
| C. guilliermondii | - | - | IE | - | |
| Non-species related | - | - | IE | - | |
| Itraconazole | C. glabrata | - | 4 | IE | 2 |
| C. albicans | - | - | S ≤ 0.06, R > 0.06 | - | |
| C. parapsilosis | - | 0.5 | S ≤ 0.125, R > 0.125 | - | |
| C. tropicalis | - | 0.5 | S ≤ 0.125, R > 0.125 | - | |
| C. lusitaniae | - | 1 | - | 0.125 | |
| C. dubliniensis | - | 0.25 | S ≤ 0.06, R > 0.06 | - | |
| C. krusei | - | 1 | IE | 1 | |
| C. guilliermondii | - | 2 | IE | 2 | |
| Non-species related | - | - | IE | - | |
| Anidulafungin | C. glabrata | S ≤ 0.12, I 0.25, R ≥ 0.5 | - | S ≤ 0.06, R > 0.06 | - |
| C. albicans | S ≤ 0.25, I 0.5, R ≥ 1 | - | S ≤ 0.03, R > 0.03 | - | |
| C. parapsilosis | S ≤ 2, I 4, R ≥ 8 | - | S ≤ 4, R > 4 | - | |
| C. tropicalis | S ≤ 0.25, I 0.5, R ≥ 1 | - | S ≤ 0.06, R > 0.06 | - | |
| C. lusitaniae | - | 1 | - | - | |
| C. dubliniensis | - | 0.12 | - | - | |
| C. krusei | S ≤ 0.25, I 0.5, R ≥ 1 | - | S ≤ 0.06, R > 0.06 | - | |
| C. guilliermondii | S ≤ 2, I 4, R ≥ 8 | - | IE | - | |
| Non-species related | - | - | IE | - | |
| Micafungin | C. glabrata | S ≤ 0.06, I 0.12, R ≥ 0.25 | - | S ≤ 0.03, R > 0.03 | - |
| C. albicans | S ≤ 0.25, I 0.5, R ≥ 1 | - | S ≤ 0.016, R > 0.016 | - | |
| C. parapsilosis | S ≤ 2, I 4, R ≥ 8 | - | S ≤ 2, R > 2 | - | |
| C. tropicalis | S ≤ 0.25, I 0.5, R ≥ 1 | - | IE | 0.06 | |
| C. lusitaniae | - | 0.5 | - | - | |
| C. dubliniensis | - | 0.12 | - | - | |
| C. krusei | S ≤ 0.25, I 0.5, R ≥ 1 | - | IE | 0.25 | |
| C. guilliermondii | S ≤ 2, I 4, R ≥ 8 | - | IE | - | |
| Non-species related | - | - | IE | - | |
| Caspofungin | C. glabrata | S ≤ 0.12, I 0.25, R ≥ 0.5 | - | † | † |
| C. albicans | S ≤ 0.25, I 0.5, R ≥ 1 | - | † | † | |
| C. parapsilosis | S ≤ 2, I 4, R ≥ 8 | - | † | † | |
| C. tropicalis | S ≤ 0.25, I 0.5, R ≥ 1 | - | † | † | |
| C. lusitaniae | - | 1 | † | † | |
| C. dubliniensis | - | - | † | † | |
| C. krusei | S ≤ 0.25, I 0.5, R ≥ 1 | - | † | † | |
| C. guilliermondii | S ≤ 2, I 4, R ≥ 8 | - | † | † | |
| Non-species related | - | - | † | † | |
| Amphotericin B | C. glabrata | - | 2 | S ≤ 1, R > 1 | - |
| C. albicans | - | 2 | S ≤ 1, R > 1 | - | |
| C. parapsilosis | - | 1 | S ≤ 1, R > 1 | - | |
| C. tropicalis | - | 2 | S ≤ 1, R > 1 | - | |
| C. lusitaniae | - | 2 | - | [0.5] | |
| C. dubliniensis | - | 0.5 | S ≤ 1, R > 1 | - | |
| C. krusei | - | 2 | S ≤ 1, R > 1 | - | |
| C. guilliermondii | - | 2 | IE | [0.5] | |
| C. kefyr | - | 2 | [1] | ||
| Non-species related | - | - | IE | - |
| QC Strain | Antifungal Agent | Sensititre Modal MIC (mg/L) | MICRONAUT Modal MIC (mg/L) | Sensititre Percentage of MICs within Mode ± 1 Dilution | MICRONAUT Percentage of MICs within Mode ± 1 Dilution |
|---|---|---|---|---|---|
| Fluconazole | 1 | 1 | 100% | 100% | |
| Posaconazole | 0.06 | ≤0.008 | 100% | 100% | |
| Voriconazole | 0.015 | ≤0.008 | 100% | 100% | |
| Itraconazole | 0.12 | ≤0.03 | 100% | 100% | |
| ATCC 22019 | Anidulafungin | 1 | 0.25 | 100% | 100% |
| C. parapsilosis | Micafungin | 1 | 0.12 | 100% | 100% |
| Caspofungin | 0.5 | 0.12–0.25 | 100% | 100% | |
| Amphotericin B | 0.5 | 0.25 | 100% | 100% | |
| 5-Flucytosine | 0.5 | ≤0.06 | 100% | 100% | |
| Fluconazole | 32–64 | 32 | 100% | 100% | |
| Posaconazole | 0.25 | 0.03 | 100% | 100% | |
| Voriconazole | 0.25 | 0.03 | 100% | 100% | |
| Itraconazole | 0.25 | ≤0.03 | 100% | 100% | |
| ATCC 6258 | Anidulafungin | 0.12 | 0.03 | 100% | 100% |
| C. krusei | Micafungin | 0.12–0.25 | 0.06 | 100% | 100% |
| Caspofungin | 0.5 | 0.25 | 100% | 100% | |
| Amphotericin B | 1 | 0.5 | 100% | 100% | |
| 5-Flucytosine | 16 | 8 | 100% | 75% |
| Antifungal Agent | EA (%) | CA (%) | Number and Percentage CA Discrepancies | ||
|---|---|---|---|---|---|
| mD | MD | VMD | |||
| Fluconazole | 98.0 | 95.1 | 3 (3.7%) | 0 | 1 (1.2%) |
| Posaconazole | 38.3 | 74.0 | 0 | 1 (1.3%) | 19 (24.7%) |
| Voriconazole | 64.6 | 66.7 | 9 (13.6%) | 0 | 13 (19.7%) |
| Itraconazole | 72.7 | 81.9 | 0 | 13 (18.1%) | 0 |
| Anidulafungin | 89.9 | 75.8 | 2 (3.0%) | 14 (21.2%) | 0 |
| Micafungin | 84.8 | 93.9 | 2 (3.0%) | 2 (3.0%) | 0 |
| Caspofungin | 94.9 | - | - | - | - |
| Amphotericin B | 100 | 100 | 0 | 0 | 0 |
| 5-Flucytosine | 94.9 | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Philips, S.; Van Hoecke, F.; De Laere, E.; Vervaeke, S.; De Smedt, R.; Boelens, J.; De Geyter, D.; Piérard, D.; Lagrou, K. Comparison of Two Commercial Colorimetric Broth Microdilution Tests for Candida Susceptibility Testing: Sensititre YeastOne versus MICRONAUT-AM. J. Fungi 2021, 7, 356. https://doi.org/10.3390/jof7050356
Philips S, Van Hoecke F, De Laere E, Vervaeke S, De Smedt R, Boelens J, De Geyter D, Piérard D, Lagrou K. Comparison of Two Commercial Colorimetric Broth Microdilution Tests for Candida Susceptibility Testing: Sensititre YeastOne versus MICRONAUT-AM. Journal of Fungi. 2021; 7(5):356. https://doi.org/10.3390/jof7050356
Chicago/Turabian StylePhilips, Sophie, Frederik Van Hoecke, Emmanuel De Laere, Steven Vervaeke, Roos De Smedt, Jerina Boelens, Deborah De Geyter, Denis Piérard, and Katrien Lagrou. 2021. "Comparison of Two Commercial Colorimetric Broth Microdilution Tests for Candida Susceptibility Testing: Sensititre YeastOne versus MICRONAUT-AM" Journal of Fungi 7, no. 5: 356. https://doi.org/10.3390/jof7050356
APA StylePhilips, S., Van Hoecke, F., De Laere, E., Vervaeke, S., De Smedt, R., Boelens, J., De Geyter, D., Piérard, D., & Lagrou, K. (2021). Comparison of Two Commercial Colorimetric Broth Microdilution Tests for Candida Susceptibility Testing: Sensititre YeastOne versus MICRONAUT-AM. Journal of Fungi, 7(5), 356. https://doi.org/10.3390/jof7050356