
Performance, Correlation and Kinetic Profile of Circulating Serum Fungal Biomarkers of Invasive Aspergillosis in High-Risk Patients with Hematologic Malignancies

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Clinical Samples and Biomarker Testing
2.3. Data Analysis
3. Results
3.1. Patients’ Characteristics and IA Episodes
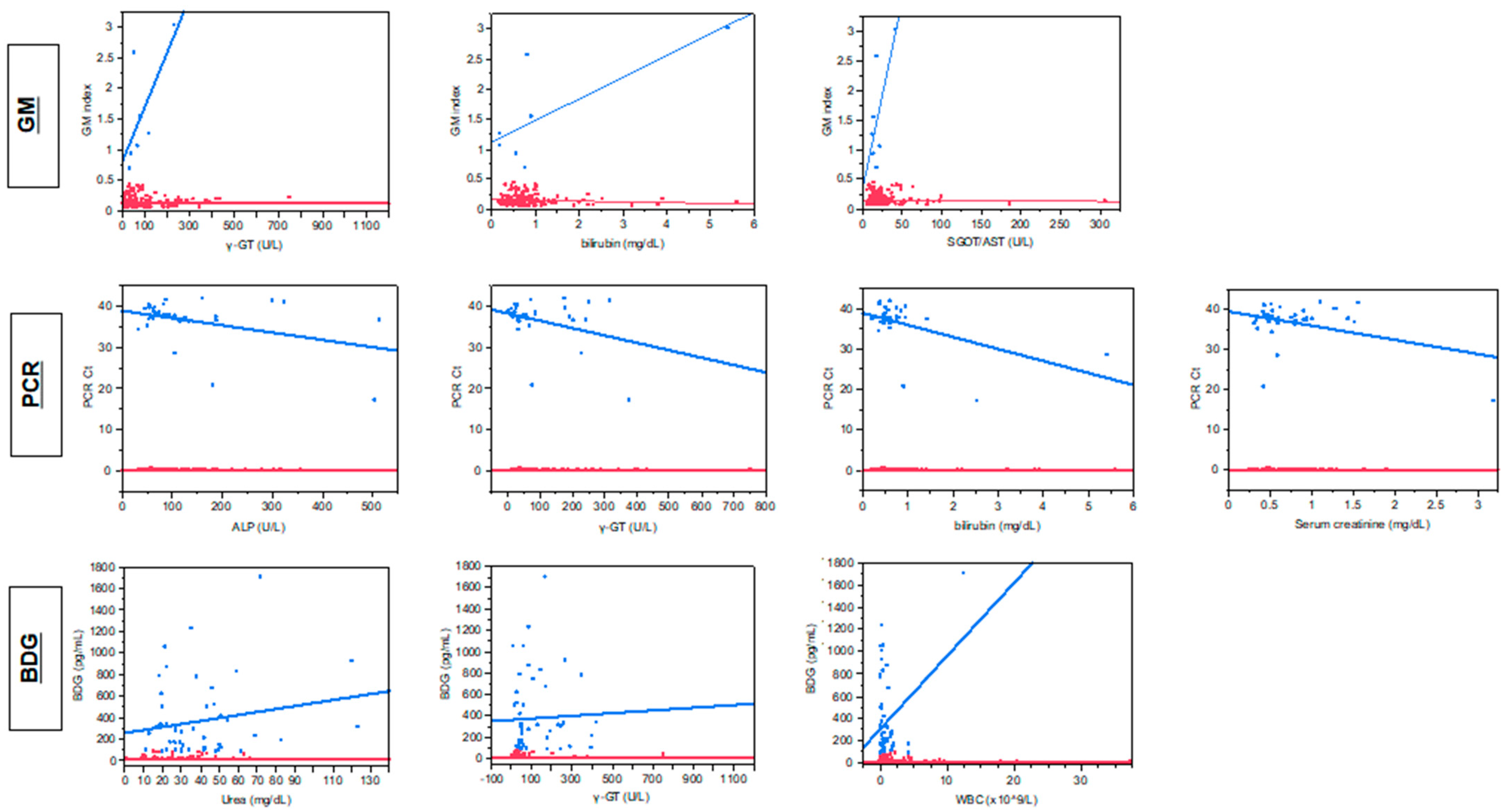
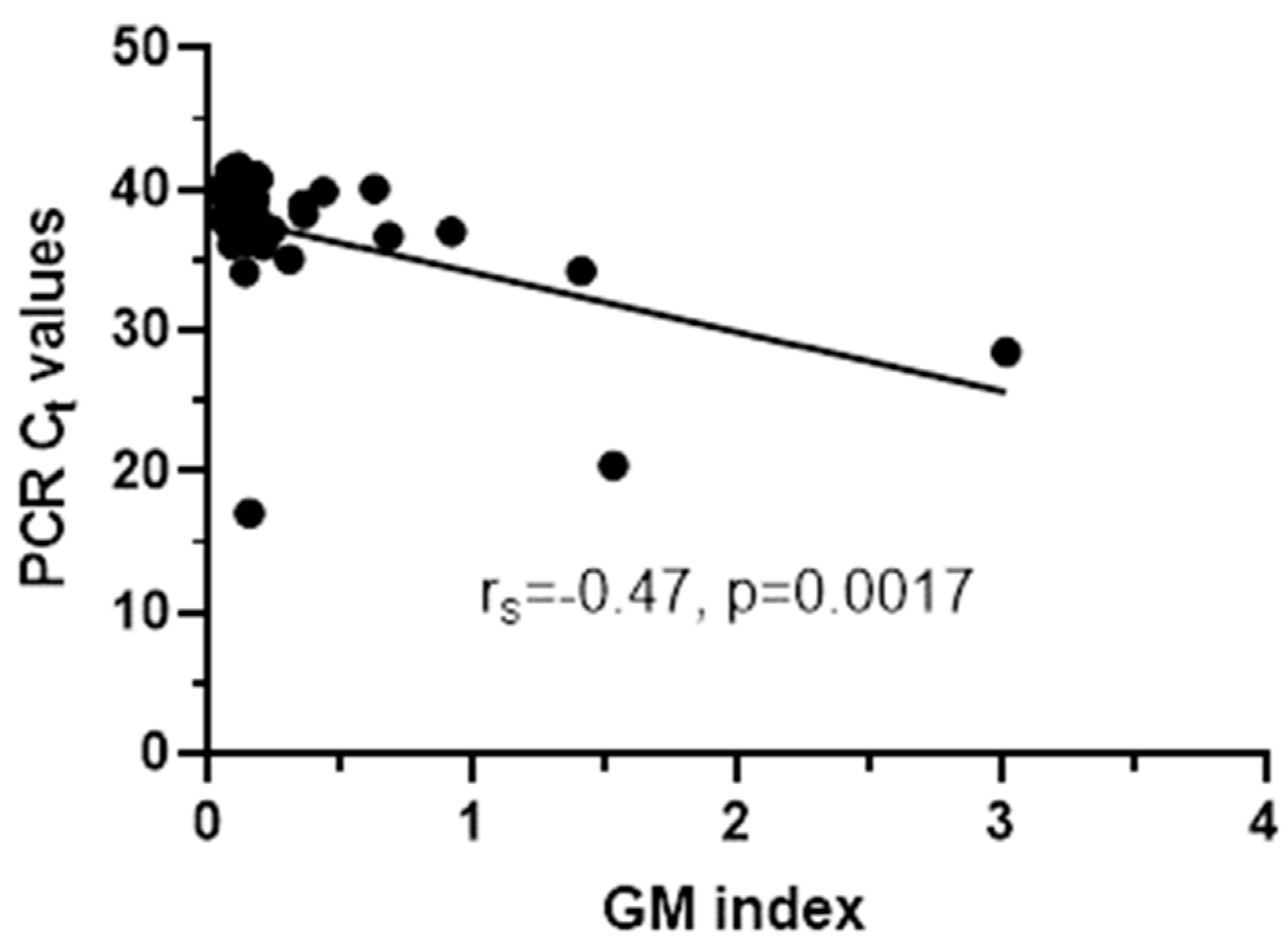
3.2. Correlation between Fungal Biomarkers and Various Parameters
3.3. Biomarkers per Sample
3.4. Biomarkers per Patient
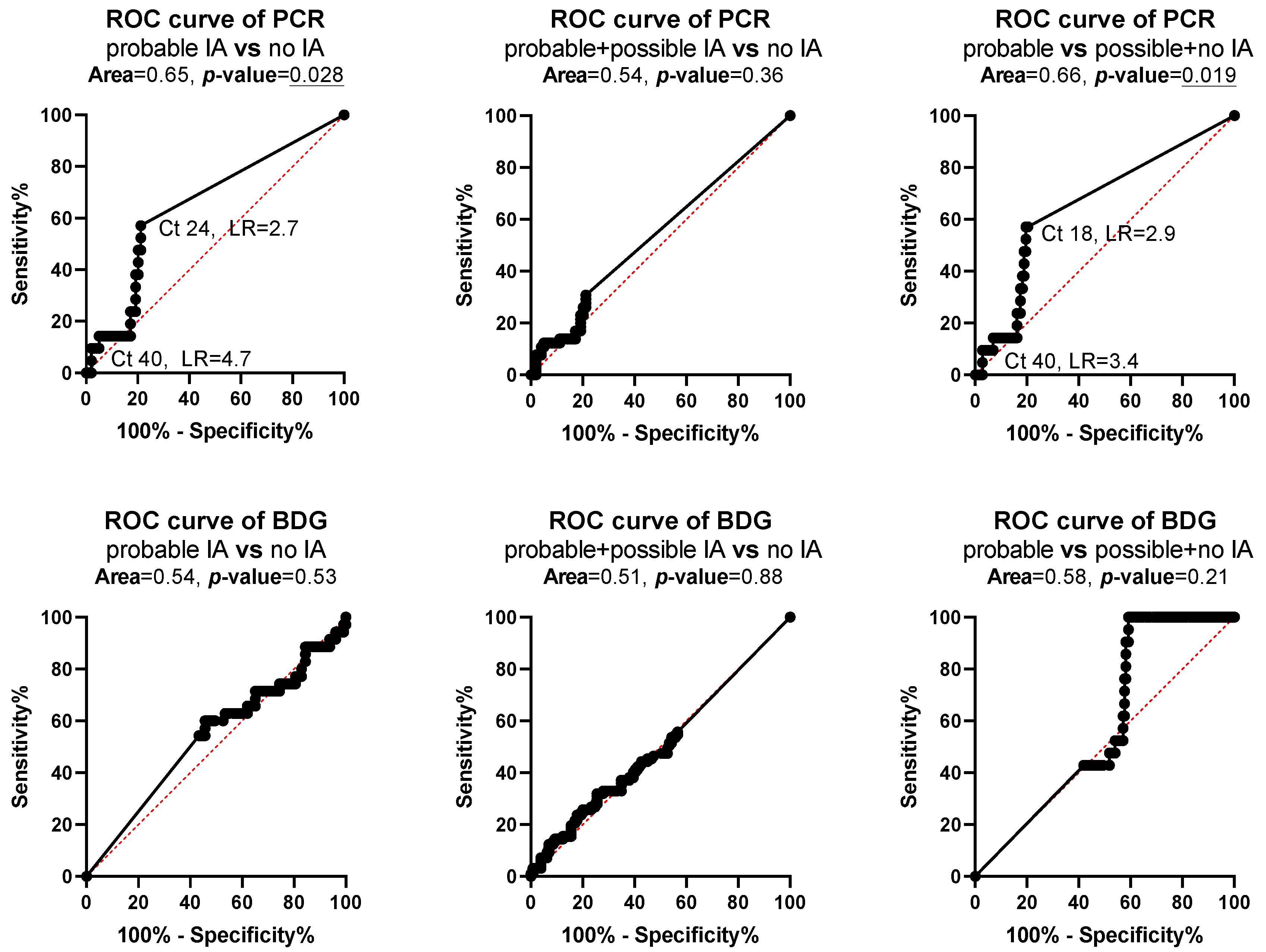
3.5. Agreement between Biomarkers and Diagnostic Performance
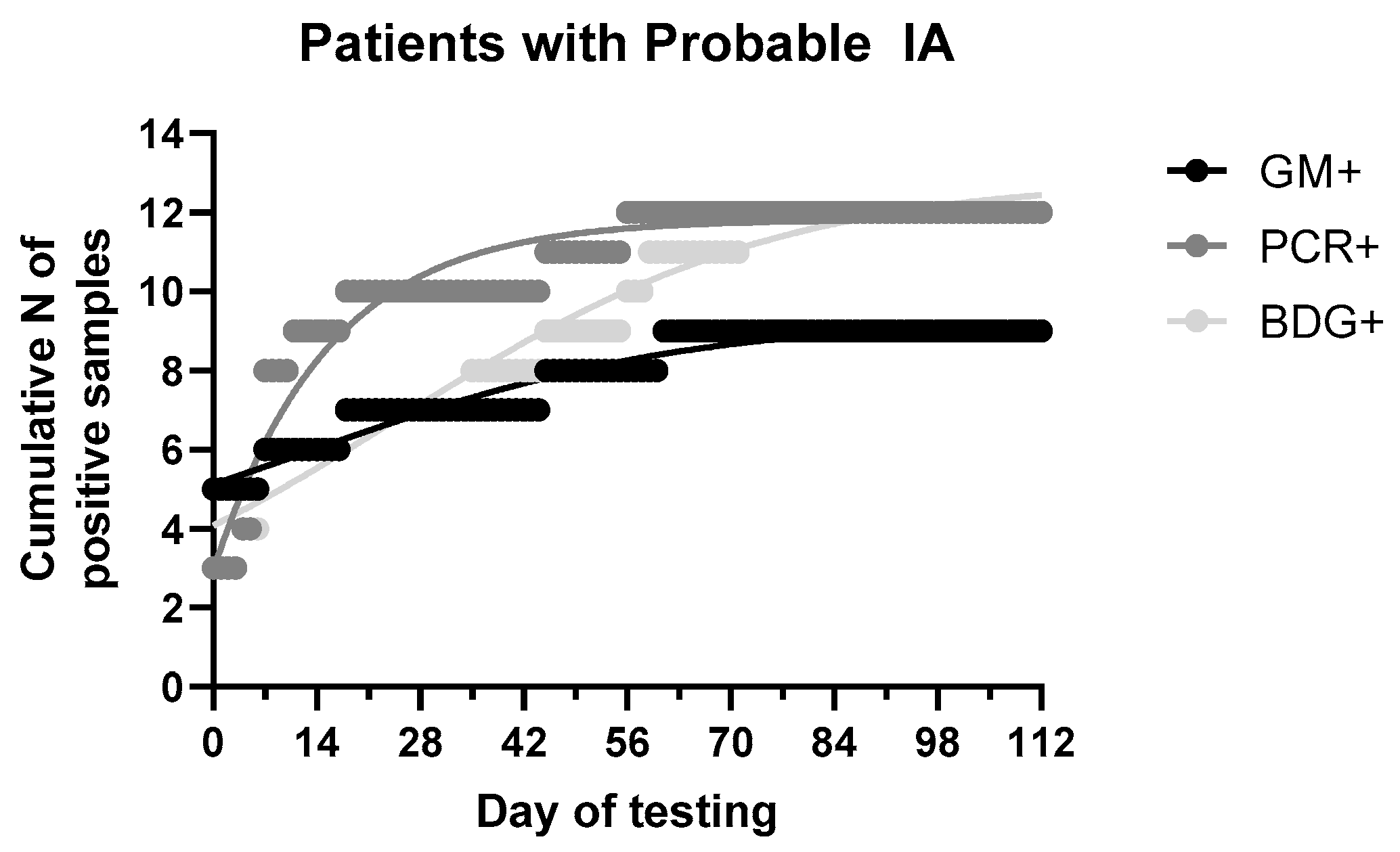
3.6. Time-To-Positivity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jenks, J.D.; Hoenigl, M. Treatment of aspergillosis. J. Fungi 2018, 4, 98. [Google Scholar] [CrossRef]
- Lamoth, F.; Calandra, T. Early diagnosis of invasive mould infections and disease. J. Antimicrob. Chemother. 2017, 72, i19–i28. [Google Scholar] [CrossRef]
- Girmenia, C.; Guerrisi, P.; Frustaci, A.M.; Fama, A.; Finolezzi, E.; Perrone, S.; Gentile, G.; Collerone, F.; Brocchieri, S.; Guerrisi, V. New category of probable invasive pulmonary aspergillosis in haematological patients. Clin. Microbiol. Infect. 2012, 18, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, A.; Porcher, R.; Sulahian, A.; De Bazelaire, C.; Chagnon, K.; Raffoux, E.; Vekhoff, A.; Cornet, M.; Isnard, F.; Brethon, B.; et al. The strategy for the diagnosis of invasive pulmonary aspergillosis should depend on both the underlying condition and the leukocyte count of patients with hematologic malignancies. Blood 2012, 119, 1831–1837. [Google Scholar] [CrossRef] [PubMed]
- Milito, M.A.; Kontoyiannis, D.P.; Lewis, R.E.; Liu, P.; Mawlawi, O.R.; Truong, M.T.; Marom, E.M. Influence of host immunosuppression on CT findings in invasive pulmonary aspergillosis. Med. Mycol. 2010, 48, 817–823. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef]
- Mercier, T.; Guldentops, E.; Lagrou, K.; Maertens, J. Galactomannan, a Surrogate Marker for Outcome in Invasive Aspergillosis: Finally Coming of Age. Front. Microbiol. 2018, 9, 661. [Google Scholar] [CrossRef]
- Neofytos, D.; Railkar, R.; Mullane, K.M.; Fredricks, D.N.; Granwehr, B.; Marr, K.A.; Almyroudis, N.G.; Kontoyiannis, D.P.; Maertens, J.; Fox, R.; et al. Correlation between circulating fungal biomarkers and clinical outcome in invasive aspergillosis. PLoS ONE 2015, 10. [Google Scholar] [CrossRef]
- Hammarström, H.; Stjärne Aspelund, A.; Christensson, B.; Heußel, C.P.; Isaksson, J.; Kondori, N.; Larsson, L.; Markowicz, P.; Richter, J.; Wennerås, C.; et al. Prospective evaluation of a combination of fungal biomarkers for the diagnosis of invasive fungal disease in high-risk haematology patients. Mycoses 2018, 61, 623–632. [Google Scholar] [CrossRef]
- Morton, C.O.; Loeffler, J.; De Luca, A.; Frost, S.; Kenny, C.; Duval, S.; Romani, L.; Rogers, T.R. Dynamics of extracellular release of Aspergillus fumigatus DNA and galactomannan during growth in blood and serum. J. Med. Microbiol. 2010, 59, 408–413. [Google Scholar] [CrossRef]
- Mennink-Kersten, M.A.; Ruegebrink, D.; Wasei, N.; Melchers, W.J.; Verweij, P.E. In vitro release by Aspergillus fumigatus of galactofuranose antigens, 1,3-beta-D-glucan, and DNA, surrogate markers used for diagnosis of invasive aspergillosis. J. Clin. Microbiol. 2006, 44, 1711–1718. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Winston, D.J.; Limaye, A.P.; Pelletier, S.; Safdar, N.; Morris, M.I.; Meneses, K.; Busuttil, R.W.; Wagener, M.M.; Wheat, L.J. Performance characteristics of galactomannan and β-d-glucan in high-risk liver transplant recipients. Transplantation 2015, 99, 2543–2550. [Google Scholar] [CrossRef]
- Stanzani, M.; Lewis, R.E.; Fiacchini, M.; Ricci, P.; Tumietto, F.; Viale, P.; Ambretti, S.; Baccarani, M.; Cavo, M.; Vianelli, N. A Risk Prediction Score for Invasive Mold Disease in Patients with Hematological Malignancies. PLoS ONE 2013, 8, e75531. [Google Scholar] [CrossRef] [PubMed]
- Herbrecht, R.; Bories, P.; Moulin, J.C.; Ledoux, M.P.; Letscher-Bru, V. Risk stratification for invasive aspergillosis in immunocompromised patients. Ann. N. Y. Acad. Sci. 2012, 1272, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Pagano, L.; Akova, M.; Dimopoulos, G.; Herbrecht, R.; Drgona, L.; Blijlevens, N. Risk assessment and prognostic factors for mould-related diseases in immunocompromised patients. J. Antimicrob. Chemother. 2011, 66, i5–i14. [Google Scholar] [CrossRef]
- Bio-Rad. PLATELIATM ASPERGILLUS Ag; Bio-Rad: Hercules, CA, USA, 2013. [Google Scholar]
- Associates of Cape Cod. FUNGITELL® ASSAY Instructions for Use; Associates of Cape Cod: East Falmouth, MA, USA, 2020. [Google Scholar]
- White, P.L.; Mengoli, C.; Bretagne, S.; Cuenca-Estrella, M.; Finnstrom, N.; Klingspor, L.; Melchers, W.J.G.; McCulloch, E.; Barnes, R.A.; Donnelly, J.P.; et al. Evaluation of Aspergillus PCR protocols for testing serum specimens. J. Clin. Microbiol. 2011, 49, 3842–3848. [Google Scholar] [CrossRef]
- White, P.L.; Barton, R.; Guiver, M.; Linton, C.J.; Wilson, S.; Smith, M.; Gomez, B.L.; Carr, M.J.; Kimmitt, P.T.; Seaton, S.; et al. A consensus on fungal polymerase chain reaction diagnosis? A United Kingdom-Ireland evaluation of polymerase chain reaction methods for detection of systemic fungal infections. J. Mol. Diagn 2006, 8, 376–384. [Google Scholar] [CrossRef]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) C. Clin. Infect. Dis. 2008, 46, 1813–1821. [Google Scholar] [CrossRef]
- Pfeiffer, C.D.; Fine, J.P.; Safdar, N. Diagnosis of invasive aspergillosis using a galactomannan assay: A meta-analysis. Clin. Infect. Dis. 2006, 42, 1417–1427. [Google Scholar] [CrossRef]
- Haidar, G.; Falcione, B.A.; Nguyen, M.H. Diagnostic modalities for invasive mould infections among hematopoietic stem cell transplant and solid organ recipients: Performance characteristics and practical roles in the clinic. J. Fungi 2015, 1, 252–276. [Google Scholar] [CrossRef] [PubMed]
- Karageorgopoulos, D.E.; Vouloumanou, E.K.; Ntziora, F.; Michalopoulos, A.; Rafailidis, P.I.; Falagas, M.E. β-D-glucan assay for the diagnosis of invasive fungal infections: A meta-analysis. Clin. Infect. Dis. 2011, 52, 750–770. [Google Scholar] [CrossRef]
- Prattes, J.; Schilcher, G.; Krause, R. Reliability of serum 1,3-beta- d -glucan assay in patients undergoing renal replacement therapy: A review of the literature. Mycoses 2015, 58, 4–9. [Google Scholar] [CrossRef]
- Albert, O.; Toubas, D.; Strady, C.; Cousson, J.; Delmas, C.; Vernet, V.; Villena, I. Reactivity of (1→3)-β-d-glucan assay in bacterial bloodstream infections. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 1453–1460. [Google Scholar] [CrossRef]
- Racil, Z.; Kocmanova, I.; Lengerova, M.; Weinbergerova, B.; Buresova, L.; Toskova, M.; Winterova, J.; Timilsina, S.; Rodriguez, I.; Mayer, J. Difficulties in using 1,3-β-D-glucan as the screening test for the early diagnosis of invasive fungal infections in patients with haematological malignancies - High frequency of false-positive results and their analysis. J. Med. Microbiol. 2010, 59, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Arvanitis, M.; Ziakas, P.D.; Zacharioudakis, I.M.; Zervou, F.N.; Caliendo, A.M.; Mylonakis, E. PCR in Diagnosis of Invasive Aspergillosis: A Meta-Analysis of Diagnostic Performance. J. Clin. Microbiol. 2014, 52, 3731–3742. [Google Scholar] [CrossRef] [PubMed]
- Ullmann, A.J.J.; Aguado, J.M.M.; Arikan-Akdagli, S.; Denning, D.W.W.; Groll, A.H.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.E.; Munoz, P.; Verweij, P.E.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24, e1–e38. [Google Scholar] [CrossRef] [PubMed]
- Patterson, T.F.; Thompson, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- White, P.L.; Wingard, J.R.; Bretagne, S.; Löffler, J.; Patterson, T.F.; Slavin, M.A.; Barnes, R.A.; Pappas, P.G.; Donnelly, J.P. Aspergillus Polymerase Chain Reaction: Systematic Review of Evidence for Clinical Use in Comparison with Antigen Testing. Clin. Infect. Dis. 2015, 61, 1293–1303. [Google Scholar] [CrossRef] [PubMed]
- Boch, T.; Spiess, B.; Cornely, O.A.; Vehreschild, J.J.; Rath, P.M.; Steinmann, J.; Heinz, W.J.; Hahn, J.; Krause, S.W.; Kiehl, M.G.; et al. Diagnosis of invasive fungal infections in haematological patients by combined use of galactomannan, 1,3-β-D-glucan, Aspergillus PCR, multifungal DNA-microarray, and Aspergillus azole resistance PCRs in blood and bronchoalveolar lavage samples: Results of a prospective multicentre study. Clin. Microbiol. Infect. 2016, 22, 862–868. [Google Scholar] [CrossRef]
- Aguado, J.M.; Vazquez, L.; Fernandez-Ruiz, M.; Villaescusa, T.; Ruiz-Camps, I.; Barba, P.; Silva, J.T.; Batlle, M.; Solano, C.; Gallardo, D.; et al. Serum galactomannan versus a combination of galactomannan and polymerase chain reaction-based aspergillus DNA detection for early therapy of invasive aspergillosis in high-risk hematological patients: A randomized controlled trial. Clin. Infect. Dis. 2015, 60, 405–414. [Google Scholar] [CrossRef]
- Bennett, J.E.; Friedman, M.M.; Dupont, B. Receptor-Mediated Clearance of Aspergillus Galactomannan. J. Infect. Dis. 2016, 155, 1005–1010. [Google Scholar] [CrossRef]
- Halder, L.D.; Abdelfatah, M.A.; Jo, E.A.H.; Jacobsen, I.D.; Westermann, M.; Beyersdorf, N.; Lorkowski, S.; Zipfel, P.F.; Skerka, C. Factor H binds to extracellular DNA traps released from human blood monocytes in response to Candida albicans. Front. Immunol. 2017, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Toth, C.A.; Thomoas, P. Special article liver endocytosis and kupffer cells. Hepatology 1992, 16, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Duettmann, W.; Koidl, C.; Troppan, K.; Seeber, K.; Buzina, W.; Wölfler, A.; Wagner, J.; Krause, R.; Hoenigl, M. Serum and urine galactomannan testing for screening in patients with hematological malignancies. Med. Mycol. 2014, 52, 647–652. [Google Scholar] [CrossRef][Green Version]
- Dufresne, S.F.; Datta, K.; Li, X.; Dadachova, E.; Staab, J.F.; Patterson, T.F.; Feldmesser, M.; Marr, K.A. Detection of urinary excreted fungal galactomannan-like antigens for diagnosis of invasive aspergillosis. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- Raggam, R.B.; Fischbach, L.M.L.; Prattes, J.; Duettmann, W.; Eigl, S.; Reischies, F.; Wölfler, A.; Rabensteiner, J.; Prueller, F.; Krause, R.; et al. Detection of (1→3)-β-D-glucan in same-day urine and serum samples obtained from patients with haematological malignancies. Mycoses 2015, 58, 394–398. [Google Scholar] [CrossRef]
- Koc, E.; Reis, K.A.; Ebinc, F.A.; Pasaoglu, H.; Demirtas, C.; Omeroglu, S.; Derici, U.B.; Guz, G.; Erten, Y.; Bali, M.; et al. Protective effect of beta-glucan on contrast induced-nephropathy and a comparison of beta-glucan with nebivolol and N-acetylcysteine in rats. Clin. Exp. Nephrol. 2011, 15, 658–665. [Google Scholar] [CrossRef]
- Rice, P.J.; Lockhart, B.E.; Barker, L.A.; Adams, E.L.; Ensley, H.E.; Williams, D.L. Pharmacokinetics of fungal (1-3)-β-D-glucans following intravenous administration in rats. Int. Immunopharmacol. 2004, 4, 1209–1215. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Classification | (No of Samples/Patients) | No of Samples/Patients Positive for Indicated Assay | ||||||
|---|---|---|---|---|---|---|---|---|
| GM | BDG | PCR | GM + BDG | GM + PCR | BDG + PCR | GM + BDG + PCR | ||
| Probable IA | Samples (n = 20) | 9 (45%) | 11 (55%) | 11 (55%) | 5 (25%) | 5 (25%) | 7 (35%) | 3 (15%) |
| Patients (n = 8) | 7 (88%) | 5 (62%) | 5 (62%) | 4 (50%) | 4 (50%) | 4 (50%) | 3 (38%) | |
| Possible IA | Samples (n = 43) | 2 (5%) | 20 (46%) | 8 (19%) | 1 (2%) | 1 (2%) | 2 (5%) | 1 (2%) |
| Patients (n = 24) | 2 (8%) | 11 (46%) | 8 (33%) | 1 (4%) | 1 (4%) | 2 (8%) | 1 (4%) | |
| No evidence for IA | Samples (n = 93) | 0 (0%) | 37 (40%) | 20 (22%) | 0 (0%) | 0 (0%) | 13 (14%) | 0 (0%) |
| Patients (n = 51) | 0 (0%) | 18 (35%) | 14 (27%) | 0 (0%) | 0 (0%) | 11 (22%) | 0 (0%) | |
| Total | Samples (n = 156) | 11 (7%) | 68 (44%) | 39 (25%) | 6 (4%) | 6 (4%) | 22 (14%) | 4 (3%) |
| Patients (n = 83) | 9 (11%) | 34 (41%) | 27 (32%) | 5 (6%) | 5 (6%) | 17 (20%) | 4 (5%) | |
| Fungal Biomarkers | Probable IA vs. no IA | Probable+Possible IA vs. no IA | Probable IA vs. Possible+no IA |
|---|---|---|---|
| GM | 45%/100%/100%/64% | 17%/100%/100%/64% | 45%/98%/82%/92% |
| PCR | 55%/78%/35%/89% | 30%/78%/49%/62% | 55%/79%/28%/92% |
| BDG | 55%/60%/23%/86% | 49%/60%/46%/64% | 55%/58%/16%/90% |
| PCR/BDG | 75%/53%/25%/91% | 65%/53%/48%/69% | 75%/48%/18%/93% |
| PCR/GM | 80%/78%/44%/95% | 40%/78%/56%/66% | 80%/79%/36%/96% |
| BDG/GM | 80%/60%/30%/93% | 59%/60%/50%/68% | 80%/57%/22%/95% |
| PCR/BDG/GM | 90%/53%/29%/96% | 71%/53%/51%/73% | 90%/48%/20%/97% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siopi, M.; Karakatsanis, S.; Roumpakis, C.; Korantanis, K.; Eldeik, E.; Sambatakou, H.; Sipsas, N.V.; Tsirigotis, P.; Pagoni, M.; Meletiadis, J. Performance, Correlation and Kinetic Profile of Circulating Serum Fungal Biomarkers of Invasive Aspergillosis in High-Risk Patients with Hematologic Malignancies. J. Fungi 2021, 7, 211. https://doi.org/10.3390/jof7030211
Siopi M, Karakatsanis S, Roumpakis C, Korantanis K, Eldeik E, Sambatakou H, Sipsas NV, Tsirigotis P, Pagoni M, Meletiadis J. Performance, Correlation and Kinetic Profile of Circulating Serum Fungal Biomarkers of Invasive Aspergillosis in High-Risk Patients with Hematologic Malignancies. Journal of Fungi. 2021; 7(3):211. https://doi.org/10.3390/jof7030211
Chicago/Turabian StyleSiopi, Maria, Stamatis Karakatsanis, Christoforos Roumpakis, Konstantinos Korantanis, Elina Eldeik, Helen Sambatakou, Nikolaos V. Sipsas, Panagiotis Tsirigotis, Maria Pagoni, and Joseph Meletiadis. 2021. "Performance, Correlation and Kinetic Profile of Circulating Serum Fungal Biomarkers of Invasive Aspergillosis in High-Risk Patients with Hematologic Malignancies" Journal of Fungi 7, no. 3: 211. https://doi.org/10.3390/jof7030211
APA StyleSiopi, M., Karakatsanis, S., Roumpakis, C., Korantanis, K., Eldeik, E., Sambatakou, H., Sipsas, N. V., Tsirigotis, P., Pagoni, M., & Meletiadis, J. (2021). Performance, Correlation and Kinetic Profile of Circulating Serum Fungal Biomarkers of Invasive Aspergillosis in High-Risk Patients with Hematologic Malignancies. Journal of Fungi, 7(3), 211. https://doi.org/10.3390/jof7030211