
Prognostic Scores and Azole-Resistant Aspergillus fumigatus in Invasive Aspergillosis from an Indian Respiratory Medicine ICU (ICU Patients with IA Suspicion)

Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population and Study Settings
2.2. Galactomannan Antigen
2.3. ICU Scoring Systems
2.4. Antifungal Susceptibility Testing
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and Mortality Rate
3.2. Galactomannan Antigen Testing
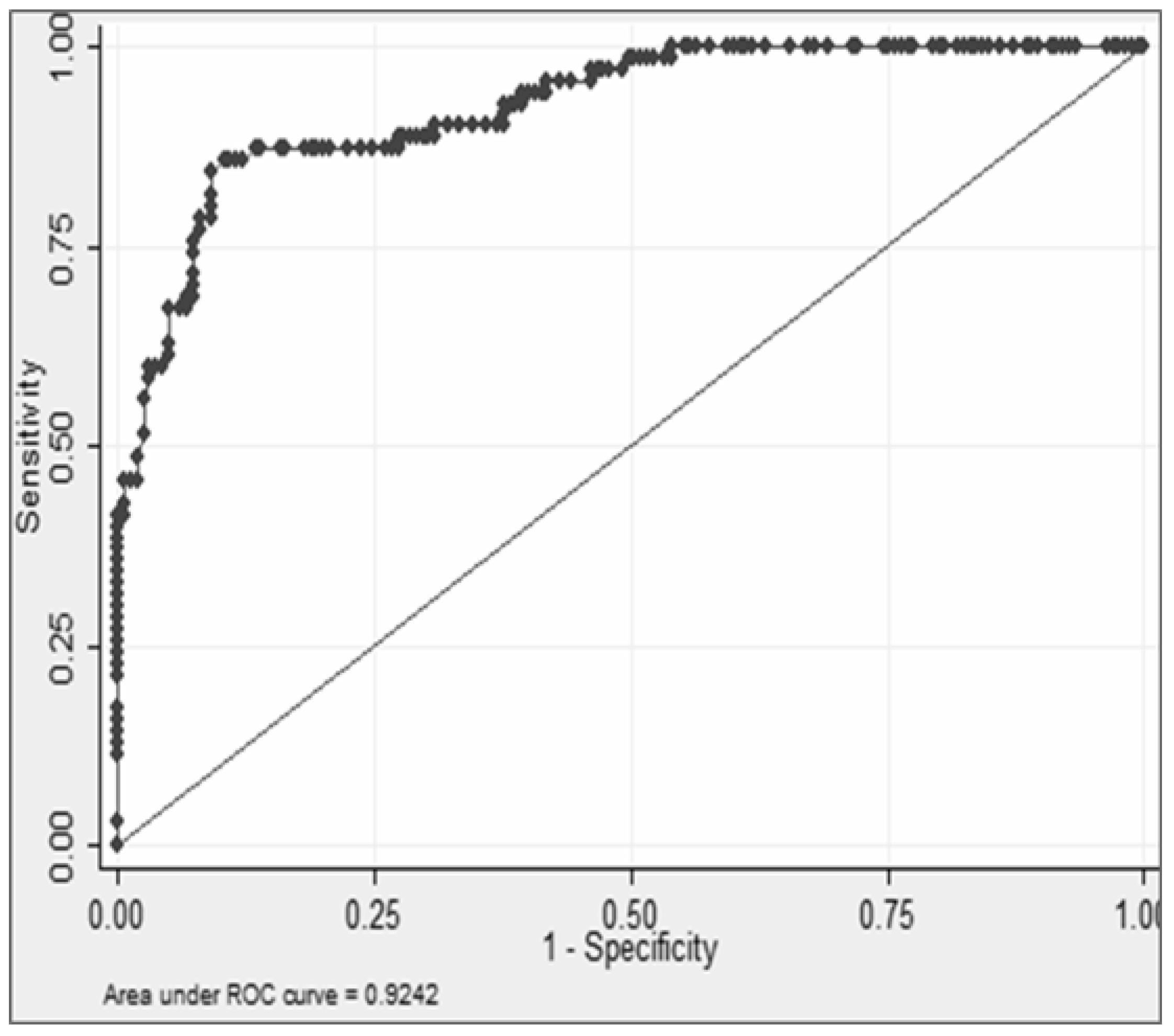
3.3. Performance of the ICU Scoring Systems and Significant GM Cut-Off for Mortality
3.4. Antifungal Susceptibility Testing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Taccone, F.S.; Van den Abeele, A.-M.; Bulpa, P.; Misset, B.; Meersseman, W.; Cardoso, T.; Paiva, J.-A.; Blasco-Navalpotro, M.; De Laere, E.; Dimopoulos, G.; et al. Epidemiology of invasive aspergillosis in critically ill patients: Clinical presentation, underlying conditions, and outcomes. Crit. Care 2015, 19, 7. [Google Scholar] [CrossRef] [PubMed]
- Barberan, J.; Sanz, F.; Hernandez, J.-L.; Merlos, S.; Malmierca, E.; Garcia-Perez, F.-J.; Sanchez-Haya, E.; Segarra, M.; de la Llana, F.G.; Granizo, J.-J.; et al. Clinical features of invasive pulmonary aspergillosis vs. colonization in COPD patients distributed by GOLD stage. J. Infect. 2012, 65, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Baddley, J.W. Clinical risk factors for invasive aspergillosis. Med. Mycol. 2011, 49, S7–S12. [Google Scholar] [CrossRef]
- Vandewoude, K.; Blot, S.; Benoit, D.; Colardyn, F.; Vogelaers, D. Invasive aspergillosis in critically ill patients: Attributable mortality and excesses in length of ICU stay and ventilator dependence. J. Hosp. Infect. 2004, 56, 269–276. [Google Scholar] [CrossRef]
- Vandewoude, K.; Blot, S.; Benoit, D.; Depuydt, P.; Vogelaers, D.; Colardyn, F. Invasive aspergillosis in critically ill patients: Analysis of risk factors for acquisition and mortality. Acta Clin. Belg. 2004, 59, 251–257. [Google Scholar] [CrossRef]
- Meersseman, W.; Vandecasteele, S.J.; Wilmer, A.; Verbeken, E.; Peetermans, W.E.; Van Wijngaerden, E. Invasive aspergillosis in critically ill patients without malignancy. Am. J. Respir. Crit. Care Med. 2004, 170, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Gursel, G.; Demirtas, S. Value of APACHE II, SOFA and CPIS scores in predicting prognosis in patients with ventilator-associated pneumonia. Respiration 2006, 73, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.J.; Anaissie, E.J.; Denning, D.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Segal, B.H.; Steinbach, W.J.; Stevens, D.A.; et al. Treatment of aspergillosis: Clinical practice guidelines of the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 46, 327–360. [Google Scholar] [CrossRef]
- Verweij, P.E.; Ananda-Rajah, M.; Andes, D.; Arendrup, M.C.; Brüggemann, R.J.; Chowdhary, A.; Cornely, O.; Groll, A.H.; Izumikawa, K.; Jan Kullberg, B.; et al. International expert opinion on the management of infection caused by azole-resistant Aspergillus fumigatus. Drug Resist. Updates 2015, 21, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Blot, S.I.; Taccone, F.S.; Van den Abeele, A.-M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am. J. Respir. Crit. Care Med. 2012, 186, 56–64. [Google Scholar] [CrossRef]
- Wayne, P.; Clinical and Laboratory Standards Institute. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi; CLSI Document M38-A2; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008. [Google Scholar]
- Arendrup, M.C.; Guinea, J.; Cuenca-Estrella, M.; Meletiadis, J.; Mouton, J.W.; Lagrou, K.; Howard, S.J.; Subcommittee on Antifungal Susceptibility Testing (AFST) of the ESCMID European Committee for Antimicrobial Susceptibility Testing (EUCAST). Method for the Determination of Broth Dilution Minimum Inhibitory Concentrations of Antifungal Agents for Conidia Forming Moulds; EUCAST Definitive Document E. DEF 7.3; Subcommittee on Antifungal Susceptibility Testing (AFST) of the ESCMID European Committee for Antimicrobial Susceptibility Testing (EUCAST): Amsterdam, The Netherlands, 2015. [Google Scholar]
- CLSI. Epidemiological Cutoff Values for Antifungal Susceptibility Testing, 2nd ed.; CLSI Supplement M59; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- Arendrup, M.C.; Cuenca-Estrella, M.; Lass-Flörl, C.; Hope, W.W.; European Committee on Antimicrobial Susceptibility Testing Subcommittee on Antifungal Susceptibility Testing (EUCAST-AFST). EUCAST technical note on Aspergillus and amphotericin B, itraconazole, and posaconazole. Clin. Microbiol. Infect. 2012, 18, E248–E250. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing. Antifungal agents—Breakpoint Tables for Interpretation of MICs, Version 8.1. 2017. Available online: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Clinical_breakpoints/Antifungal_breakpoints_v_8.1_March_2017.pdf (accessed on 11 October 2021).
- Rodriguez-Tudela, J.L.; Alcazar-Fuoli, L.; Mellado, E.; Alastruey-Izquierdo, A.; Monzon, A.; Cuenca-Estrella, M. Epidemiological cutoffs and cross-resistance to azole drugs in Aspergillus fumigatus. Antimicrob. Agents Chemother. 2008, 52, 2468–2472. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, H.; Li, R.; Bu, D.; Wan, Z. Mutations in the cyp51A gene and susceptibility to itraconazole in Aspergillus fumigatus serially isolated from a patient with lung aspergilloma. J. Antimicrob. Chemother. 2005, 55, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Hanley, J.A.; McNeil, B.J. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 1983, 148, 839–843. [Google Scholar] [CrossRef]
- Martin, S.J.; Yost, R.J. Infectious diseases in the critically ill patients. J. Pharm. Pract. 2011, 24, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Bajwa, S.J.; Kulshrestha, A. Fungal infections in intensive care unit: Challenges in diagnosis and management. Ann. Med. Health Sci. Res. 2013, 3, 238–244. [Google Scholar] [CrossRef]
- Bassetti, M.; Righi, E.; De Pascale, G.; De Gaudio, R.; Giarratano, A.; Mazzei, T.; Morace, G.; Petrosillo, N.; Stefani, S.; Antonelli, M. How to manage aspergillosis in non-neutropenic intensive care unit patients. Crit. Care 2014, 18, 458. [Google Scholar] [CrossRef] [PubMed]
- Burghi, G.; Lemiale, V.; Seguin, A.; Lambert, J.; Lacroix, C.; Canet, E.; Moreau, A.-S.; Ribaud, P.; Schnell, D.; Mariotte, E.; et al. Outcomes of mechanically ventilated hematology patients with invasive pulmonary aspergillosis. Intensive Care Med. 2011, 37, 1605–1612. [Google Scholar] [CrossRef]
- Lortholary, O.; Gangneux, J.-P.; Sitbon, K.; Lebeau, B.; de Monbrison, F.; Le Strat, Y.; Coignard, B.; Dromer, F.; Bretagne, S. Epidemiological trends in invasive aspergillosis in France: The SAIF network (2005–2007). Clin. Microbiol. Infect. 2011, 17, 1882–1889. [Google Scholar] [CrossRef] [PubMed]
- Teering, S.; Verreth, A.; Peeters, A.; van Regenmortel, N.; de Laet, I.; Schoonheydt, K.; Dits, H.; van de Vyvere, M.; Libeer, C.; Meersseman, W.; et al. Prognostic value of serum galactomannan in mixed ICU patients: A retrospective observational study. Anaesthesiol. Intensive Ther. 2014, 47, 145–154. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Chang, S.; Ding, L.; Li, F.; Zhan, Q. Value of consecutive galactomannan determinations for the diagnosis and prognosis of invasive pulmonary aspergillosis in critically ill chronic obstructive pulmonary disease. Med. Mycol. 2011, 49, 345–351. [Google Scholar] [CrossRef]
- Vandewoude, K.H.; Vogelaers, D.; Blot, S.I. Aspergillosis in the ICU—The new 21st century problem? Med. Mycol. 2006, 44, S71–S76. [Google Scholar] [CrossRef]
- Moreno, R.; Jordan, B.; Metnitz, P. The changing prognostic determinants in the critically ill patient. In 2007 Yearbook of Intensive care and Emergency Medicine; Vincent, J.L., Ed.; Springer: Heidelberg, Germany, 2007; pp. 899–907. [Google Scholar]
- Vincent, J.L.; Moreno, R. Clinical review: Scoring systems in the critically ill. Crit. Care 2010, 14, 207. [Google Scholar] [CrossRef]
- Kopterides, P.; Liberopoulos, P.; Ilias, I.; Anthi, A.; Pragkastis, D.; Tsangaris, I.; Tsaknis, G.; Armaganidis, A.; Dimopoulou, I. General prognostic scores in outcome prediction for cancer patients admitted to the intensive care unit. Am. J. Crit. Care 2011, 20, 56–66. [Google Scholar] [CrossRef][Green Version]
- Saleh, A.; Ahmed, M.A.; Sultan, I.; Abdel-Lateif, A. Comparison of the mortality prediction of different ICU scoring systems (APACHE II and III, SAPS II, and SOFA) in a single-center ICU subpopulation with acute respiratory distress syndrome. Egypt. J. Chest. Dis. Tuberc. 2015, 64, 843–848. [Google Scholar] [CrossRef]
- Xiao, K.; Guo, C.; Su, L.; Yan, P.; Li, X.; Xie, L. Prognostic value of different scoring models in patients with multiple organ dysfunction syndrome associated with acute COPD exacerbation. J. Thorac. Dis. 2015, 7, 329–336. [Google Scholar] [PubMed]
- Howard, S.J.; Arendrup, M.C. Acquired antifungal drug resistance in Aspergillus fumigatus: Epidemiology and detection. Med. Mycol. 2011, 49, S90–S95. [Google Scholar] [CrossRef] [PubMed]
- Howard, S.J.; Cerar, D.; Anderson, M.J.; Albarrag, A.; Fisher, M.; Pasqualotto, A.C.; Laverdiere, M.; Arendrup, M.C.; Perlin, D.; Denning, D.W. Frequency and evolution of azole resistance in Aspergillus fumigatus associated with treatment failure. Emerg. Infect. Dis. 2009, 15, 1068–1076. [Google Scholar] [CrossRef] [PubMed]
- Snelders, E.; Van Der Lee, H.A.L.; Kuijpers, J.; Rijs, A.J.M.M.; Varga, J.; Samson, R.A.; Mellado, E.; Donders, A.R.T.; Melchers, W.; Verweij, P.E. Emergence of azole resistance in Aspergillus fumigatus and spread of a single resistance mechanism. PLoS Med. 2008, 5, e219. [Google Scholar] [CrossRef]
- Moore, C.; Sayers, N.; Mosquera, J.; Slaven, J.; Denning, D. Antifungal drug resistance in Aspergillus. J. Infect. 2000, 41, 203–220. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Rubio, R.; Gonzalez-Jimenez, I.; Lucio, J.; Mellado, E. Aspergillus fumigatus cross-resistance between clinical and demethylase inhibitor azole drugs. Appl. Environ. Microbiol. 2021, 87, e02539-20. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Sharma, C.; Kathuria, S.; Hagen, F.; Meis, J. Prevalence and mechanism of triazole resistance in Aspergillus fumigatus in a referral chest hospital in Delhi, India and an update of the situation in Asia. Front. Microbiol. 2015, 6, 428. [Google Scholar] [CrossRef]
- Chowdhary, A.; Kathuria, S.; Randhawa, H.S.; Gaur, S.N.; Klaassen, C.H.; Meis, J. Isolation of multiple-triazole-resistant Aspergillus fumigatus strains carrying the TR/L98H mutations in the cyp51A gene in India. J. Antimicrob. Chemother. 2012, 67, 362–366. [Google Scholar] [CrossRef]
- Chowdhary, A.; Kathuria, S.; Xu, J.; Sharma, C.; Sundar, G.; Singh, P.K.; Gaur, S.N.; Hagen, F.; Klaassen, C.H.; Meis, J.F. Clonal expansion and emergence of environmental multiple-triazole-resistant Aspergillus fumigatus strains carrying the TR34/L98H mutations in the cyp51A gene in India. PLoS ONE 2012, 7, e52871. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Sharma, C.; Kathuria, S.; Hagen, F.; Meis, J.F. Azole-resistant Aspergillus fumigatus with the environmental TR46/Y121F/T289A mutation in India. J. Antimicrob. Chemother. 2014, 69, 555–571. [Google Scholar] [CrossRef] [PubMed]
- Dabas, Y.; Xess, I.; Bakshi, S.; Mahapatra, M.; Seth, R. Emergence of azole-resistant Aspergillus fumigatus from immunocompromised hosts in India. Antimicrob. Agents Chemother. 2018, 62, e02264-17. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Messer, S.A.; Boyken, L.; Rice, C.; Tendolkar, S.; Hollis, R.J.; Diekema, D. In Vitro Survey of Triazole Cross-Resistance among More than 700 Clinical Isolates of Aspergillus Species. J. Clin. Microbiol. 2008, 46, 2568–2572. [Google Scholar] [CrossRef] [PubMed]
- Baddley, J.W.; Marr, K.A.; Andes, D.R.; Walsh, T.J.; Kauffman, C.A.; Kontoyiannis, D.P.; Ito, J.I.; Balajee, S.A.; Pappas, P.G.; Moser, S.A. Patterns of Susceptibility of Aspergillus Isolates Recovered from Patients Enrolled in the Transplant-Associated Infection Surveillance Network. J. Clin. Microbiol. 2009, 47, 3271–3275. [Google Scholar] [CrossRef]
- Shi, J.-Y.; Xu, Y.-C.; Shi, Y.; Lü, H.-X.; Liu, Y.; Zhao, W.-S.; Chen, D.-M.; Xi, L.-Y.; Zhou, X.; Wang, H.; et al. In vitro susceptibility testing of Aspergillus spp. against voriconazole, itraconazole, posaconazole, amphotericin B and caspofungin. Chin. Med. J. 2010, 123, 2706–2709. [Google Scholar] [PubMed]
- Ahmad, S.; Joseph, L.; Hagen, F.; Meis, J.; Khan, Z. Concomitant occurrence of itraconazole-resistant and -susceptible strains of Aspergillus fumigatus in routine cultures. J. Antimicrob. Chemother. 2015, 70, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, M.; Izumikawa, K.; Minematsu, A.; Hirano, K.; Iwanaga, N.; Ide, S.; Mihara, T.; Hosogaya, N.; Takazono, T.; Morinaga, Y.; et al. Antifungal susceptibilities of Aspergillus fumigatus clinical isolates obtained in Nagasaki, Japan. Antimicrob. Agents Chemother. 2012, 56, 584–587. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total | Mortality in Invasive Aspergillosis (IA) CI: 0.23–0.35 | p-Value | Unadjusted OR (95% CI) | |
|---|---|---|---|---|---|
| Survivor (n = 165; 70.2%) | Non-Survivors (n = 70; 29.7%) | ||||
| Age (years) | 50.6 ± 15.8 (48.2–53.1) | 50.7 ± 16.9 (46.7–54.8) | 0.97 | ||
| 0–12 | 6 | 2 (33.3) | 4 (66.6) | 0.23 | |
| 12–18 | 16 | 12 (75) | 4 (25) | 0.16 (0.02–1.29) | |
| 19–60 | 161 | 113 (70.1) | 48 (29.8) | 0.21 (0.03–1.19) | |
| >60 | 52 | 38 (73) | 14 (26.9) | 0.18 (0.03–1.11) | |
| Male | 149 | 103 (69.1) | 46 (30.8) | 0.63 | 1.15 (0.64–2.07) |
| Seasonal variation | |||||
| Summer | 66 | 39 (59) | 27 (40.9) | 0.07 | 2.15 (1.03–4.49) |
| Autumn | 36 | 24 (66.6) | 12 (33.3) | 1.55 (0.64–3.76) | |
| Hematological malignancy | 27 | 12 (44.4) | 15 (55.5) | 0.002 | 3.47 (1.53–7.88) |
| CGD/TB | 216 | 151 (69.9) | 65 (30) | 0.73 | 1.2 (0.41–3.48) |
| COPD | 41 | 13 (31.7) | 28 (68.2) | 0.00 | 7.79 (3.71–16.35) |
| ARF | 15 | 9 (60) | 6 (40) | 0.37 | 1.62 (0.55–4.75) |
| Metastatic cancer | 3 | 2 (66.6) | 1 (33.3) | 0.89 | 1.18 (0.1–13.24) |
| Diabetes | 14 | 6 (42.8) | 8 (57.1) | 0.02 | 3.41 (1.13–10.25) |
| Corticosteroid administration < 7 days | 47 | 25 (53.1) | 22 (46.8) | 0.004 | 2.56 (1.32–4.96) |
| Corticosteroid administration ≥ 21 days | 16 | 6 (37.5) | 10 (62.5) | 0.003 | 4.41 (1.53–12.68) |
| Variables | Total (n = 235) | Mortality in Invasive Aspergillosis (IA) CI: 0.23–0.35 | p-Value | Unadjusted Odds Ratio (95% CI) | |
|---|---|---|---|---|---|
| Survivor (n = 165; 70.2%) | Non-Survivors (n = 70; 29.7%) | ||||
| Mechanical ventilation | 95 | 63 (66.3) | 32 (33.6) | 0.28 | 1.36 (0.77–2.4) |
| Thrombocytopenia | 85 | 58 (68.2) | 27 (31.7) | 0.61 | 1.15 (0.65–2.06) |
| Vasopressors | 18 | 12 (66.6) | 6 (33.3) | 0.73 | 1.19 (0.42–3.32) |
| Pneumonia | 80 | 55 (68.7) | 25 (31.25) | 0.58 | 1.11 (0.61–1.99) |
| Sepsis | 19 | 12 (63.1) | 7 (36.8) | 0.48 | 1.41 (0.53–3.76) |
| Temperature | 0.26 | ||||
| 38–39.3 °C | 130 | 86 (66.1) | 44 (33.8) | 1.65 (0.9–3.04) | |
| ≥39.4 °C | 16 | 11 (68.7) | 5 (31.2) | 1.47 (0.45–4.71 | |
| Prolonged treatments | 0.003 F | ||||
| Steroids | 26 | 10 (38.4) | 16 (61.5) | 3.76 (1.55–9.13) | |
| HAART | 3 | 2 (66.6) | 1 (33.3) | 1.17 (0.01–13.41) | |
| Duration in ICU | 0.88 | ||||
| >4–7 days | 69 | 46 (66.6) | 23 (33.3) | 1.31 (0.5–3.41) | |
| >7–14 days | 104 | 75 (72.1) | 29 (27.8) | 1.01 (0.4–2.54) | |
| >14 days | 33 | 23 (69.7) | 10 (30.3) | 1.14 (0.37–3.43) | |
| Neutropenia | 35 | 22 (62.8) | 13 (37.1) | 0.302 | 1.48 (0.69–3.14) |
| Malnourishment | 10 | 4 (40) | 6 (60) | 0.03 | 3.77 (1.03–13.81) |
| Mechanical ventilation | 192 | 61 (66.3) | 31 (33.7) | 0.29 | 1.35 (0.76–2.39) |
| Dialysis | 13 | 6 (46.1) | 7 (53.8) | 0.05 | 2.94 (0.95–9.1) |
| Antibiotics administered | |||||
| Cefoperazone-sulbactam | 113 | 80 (70.8) | 33 (29.2) | 0.85 | 0.94 (0.54–1.65) |
| Amikacin | 153 | 114 (74.5) | 39 (25.4) | 0.04 | 0.56 (0.31–1) |
| Piperacillin-tazobactam | 74 | 42 (56.7) | 32 (43.2) | 0.002 | 2.46 (1.37–4.43) |
| Vancomycin | 90 | 66 (73.3) | 24 (26.6) | 0.41 | 0.78 (0.43–1.4) |
| Linezolid | 71 | 49 (69) | 22 (30.9) | 0.79 | 1.08 (0.59–1.98) |
| Metrogyl | 62 | 52 (83.8) | 10 (16.1) | 0.00 | 0.36 (0.17–0.76) |
| Meropenam | 107 | 75 (70) | 32 (29.9) | 0.97 | 1.01 (0.57–1.77) |
| Levofloxacin | 91 | 65 (71.4) | 26 (28.5) | 0.74 | 0.9 (0.51–1.61) |
| Other β lactam drugs | 26 | 21 (80.7) | 5 (19.21) | 0.21 | 0.52 (0.19–1.46) |
| Radiological findings | 0.86 | ||||
| Pleural effusion | 10 | 6 (60) | 4 (40) | 1.47 (0.39–5.16) | |
| Consolidation | 10 | 6 (60) | 4 (40) | 1.47 (0.39–5.6) | |
| Aspergillus culture positivity | 34 | 7 (20.59) | 27 (79.41) | 0.00 | 14.17 (5.77–34.75) |
| Galactomannan cut-off for mortality (≥1.04) | 64 | 12 (18.75) | 52 (81.25) | 0.00 | 36.83 (16.62–81.59) |
| Survival within 30 Days | Total (n = 235) | AspICU Criteria for Invasive Aspergillosis (IA) | p-Value | OR (95% CI) | |||
|---|---|---|---|---|---|---|---|
| Proven + Putative (n = 22; 9.36%) (mean ± SD: 2.46 ± 1.75; median: 1.64) | No IA (n = 201; 85.5%) (mean ± SD: 0.83 ± 0.5; median: 0.7) | Colonization (n = 12; 5.1%) (mean ± SD: 4.83 ± 1.65; median: 5.79) | Unadjusted | Adjusted | |||
| Survivor n (%); Median | 165 | 6 (3.6); 1.47 | 158 (95.7); 0.57 | 1 (0.6); 1.09 | 0.00 | ||
| Non-survivor n (%); Median | 70 | 16 (22.8); 2.09 | 43 (61.4); 1.48 | 11 (15.7); 6 | 14.17 (6.7–34.75) | 1.34 × 1017 | |
| Variable | Total (n = 235) | Mortality in Invasive Aspergillosis (IA) CI: 0.23–0.35 | p-Value | OR (95% CI) | ||
|---|---|---|---|---|---|---|
| Survivor n = 165 | Non-Survivors n = 70 | Unadjusted | Adjusted | |||
| APACHE II score Mean ± SD; median (95% CI) | 235 15.81 ± 4.25; 16 (15.23–16.36) | 165 15.35 ± 4.23; 15 (14.7–16) | 70 16.88 ± 4.14; 17 (15.89–17.87) | 0.011 | 1.08 (1.01–1.16) | 1.13 (0.99–1.29) |
| SAPS II score Mean ± SD; median (95% CI) | 216 35.82 ± 7.68; 35 (34.79–36.58) | 153 35 ± 7.6; 35 (33.8–36.2) | 63 37.6 ± 7.5 (35.7–39.5) | 0.022 | 1.04 (1–1.08) | 0.98 (0.90–1.06) |
| SOFA score Mean ± SD; median (95% CI) | 235 6.71 ± 1.49; 7 (6.51–6.9) | 165 6.52 ± 1.47; 7 (6.3–6.75) | 70 7.14 ± 1.45; 7 (6.76–7.49) | 0.003 | 1.32 (1.09–1.06) | 0.91 (0.90–1.06) |
| GM values Mean ± SD; median (95% CI) | 235 1.19 ± 1.25; 0.79 (1.03–1.35) | 165 0.68 ± 0.34; 0.606 (0.63–0.73) | 70 2.37 ± 1.73; 1.64 (1.96–2.79) | 0.000 | 44.61 (15.71–126.69) | 56.57 (17.25–185.44) |
| ICU Mortality Scores | ROC Curve | Hosmer–Lemeshow Goodness-of-Fit | Predicted Mortality, % | Standardized Mortality Ratio (95% CI) | ||
|---|---|---|---|---|---|---|
| AUC, (SE) | 95% CI | χ2 | p | |||
| APACHE II | 0.595 (0.03) | (0.518–0.672) | 11.04 | 0.92 | 24.63 | 1.20 (0.94–1.51) |
| SAPS II | 0.602 (0.04) | 0.518–0.686) | 38.69 | 0.13 | 20.07 | 1.46 (1.13–1.86) |
| SOFA | 0.610 (0.03) | (0.534–0.685) | 9.49 | 0.14 | 14.89 | 2.00 (1.57–2.51) |
| GM values | 0.924 (0.01) | (0.888–0.960) | 154.21 | 0.52 | 29.78 | 1 (0.78–1.51) |
| Antifungal | CLSI (%) (n, 34) | EUCAST (%) (n, 34) | Concordance | ICC * (95% CI) | ||
|---|---|---|---|---|---|---|
| Susceptible | Non-Susceptible | Wild-Type | Non Wild-Type | |||
| Itraconazole | 25 (73.52%) | 9 (26.47%) | 24 (70.58%) | 10 (29.41%) | 99 | 0.97 (0.93–0.99) |
| Voriconazole | 33 (97.05%) | 1 (2.94%) | 33 (97.05%) | 1 (2.94%) | 94 | 0.96 (0.91–0.98) |
| Posaconazole | 33 (97.05%) | 1 (2.94%) | 31 (91.17%) | 3 (8.82%) | 91 | 0.91 (0.69–0.97) |
| Amphotericin B | 29 (95.29%) | 5 (14.70%) | 29 (95.29%) | 5 (14.70%) | 98 | 0.97 (0.76–0.99) |
| Caspofungin | 34 (100%) | 0 | 33 (97.05%) | 1 (2.94%) | 90 | 0.94 (0.88–0.97) |
| Micafungin | 34 (100%) | 0 | 34 (100%) | 0 | 100 | 1 |
| GenBank Accession Number | Sex, Age (Years) | Underlying Disease | Clinical Specimen | AspICU Criterion | Delta (∆) GM (∆GM = GM1day 0-GM2 day 7) | Type of Mutation | Itr MIC (µg/mL) | Vor MIC (µg/mL) | Pos MIC (µg/mL) | Resistant Antifungal | Antifungal Treatment | 30-Day Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MF148156 | M, 45 | COPD, TB | Sputum | Putative | −0.46 | G54R (hotspot) | 8 | 4 | 0.03 | ITR, VOR | AMB | Died |
| MF148157 | M, 49 | COPD, TB | Sputum | Putative | 0.29 | G54R (hotspot) | 4 | 0.06 | 0.03 | ITR | AMB | Died |
| MF148158 | M, 48 | TB | BAL, pleural fluid | Putative | −0.35 | G54R (hotspot) | 8 | 0.06 | 0.03 | ITR | AMB | Died |
| MF148159 | M, 67 | COPD, TB | ETA | Putative | −0.965 | P216L (defined) | 16 | 0.06 | 1 | ITR, POS | AMB+ VOR | Died |
| MF148160 | F, 59 | COPD, TB | BAL | Putative | 0.829 | P216L (defined) | 8 | 0.03 | 0.03 | ITR | VOR | Survived |
| MF148161 | M, 45 | TB | Sputum | Colonizer | −2.08 | G54R (hotspot) | 16 | 0.06 | 0.03 | ITR | AMB | Died |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dabas, Y.; Mohan, A.; Xess, I. Prognostic Scores and Azole-Resistant Aspergillus fumigatus in Invasive Aspergillosis from an Indian Respiratory Medicine ICU (ICU Patients with IA Suspicion). J. Fungi 2021, 7, 991. https://doi.org/10.3390/jof7110991
Dabas Y, Mohan A, Xess I. Prognostic Scores and Azole-Resistant Aspergillus fumigatus in Invasive Aspergillosis from an Indian Respiratory Medicine ICU (ICU Patients with IA Suspicion). Journal of Fungi. 2021; 7(11):991. https://doi.org/10.3390/jof7110991
Chicago/Turabian StyleDabas, Yubhisha, Anant Mohan, and Immaculata Xess. 2021. "Prognostic Scores and Azole-Resistant Aspergillus fumigatus in Invasive Aspergillosis from an Indian Respiratory Medicine ICU (ICU Patients with IA Suspicion)" Journal of Fungi 7, no. 11: 991. https://doi.org/10.3390/jof7110991
APA StyleDabas, Y., Mohan, A., & Xess, I. (2021). Prognostic Scores and Azole-Resistant Aspergillus fumigatus in Invasive Aspergillosis from an Indian Respiratory Medicine ICU (ICU Patients with IA Suspicion). Journal of Fungi, 7(11), 991. https://doi.org/10.3390/jof7110991