
A Reference Laboratory Surveillance on Fungal Isolates from Patients with Haematological Malignancy in Japan

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Methods
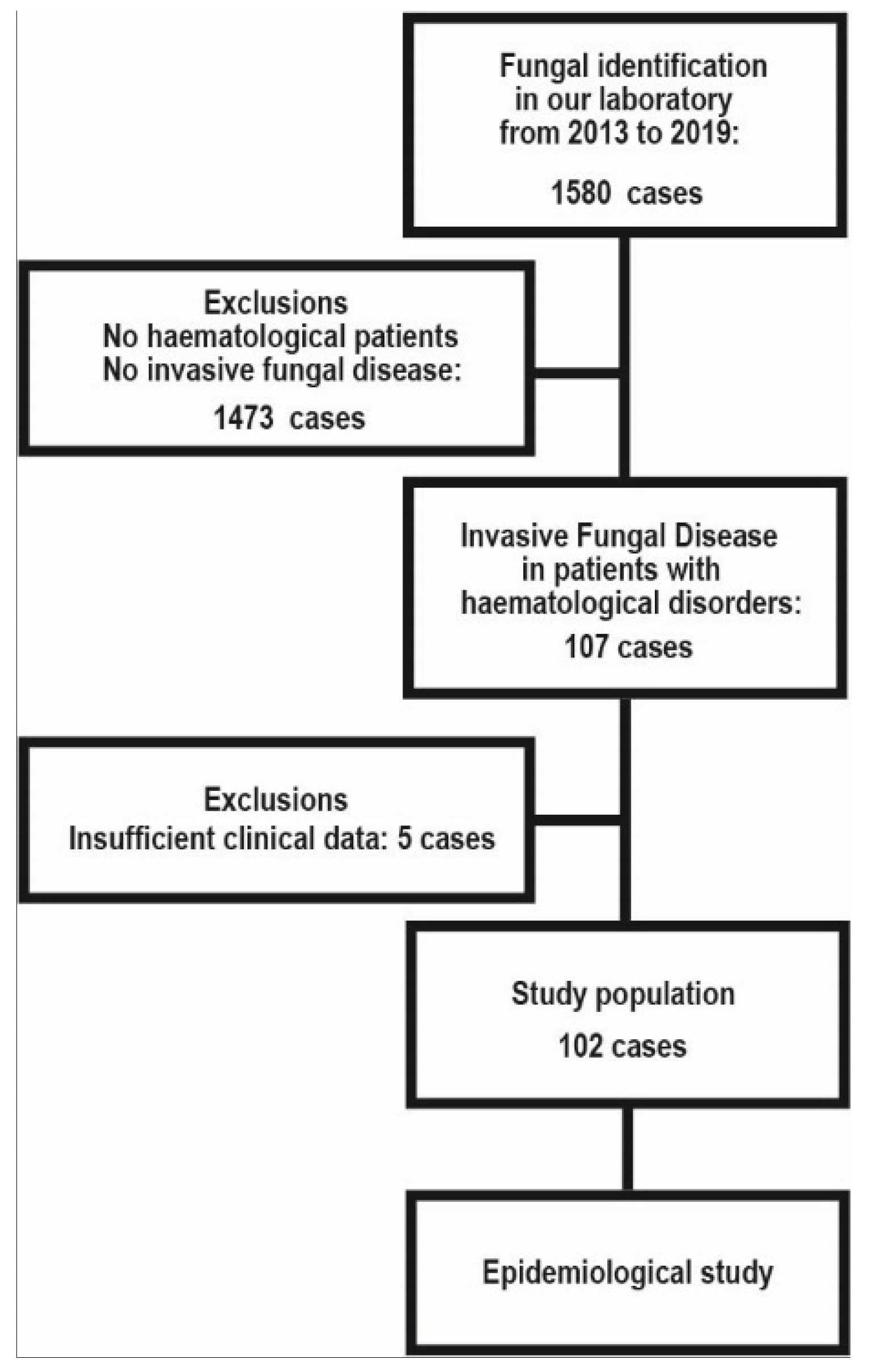
2.1. Epidemiological Study of IFD in Patients with Haematological Disorders in Japan
2.2. Fungal Identification
3. Results
3.1. Characteristics of IFD Cases
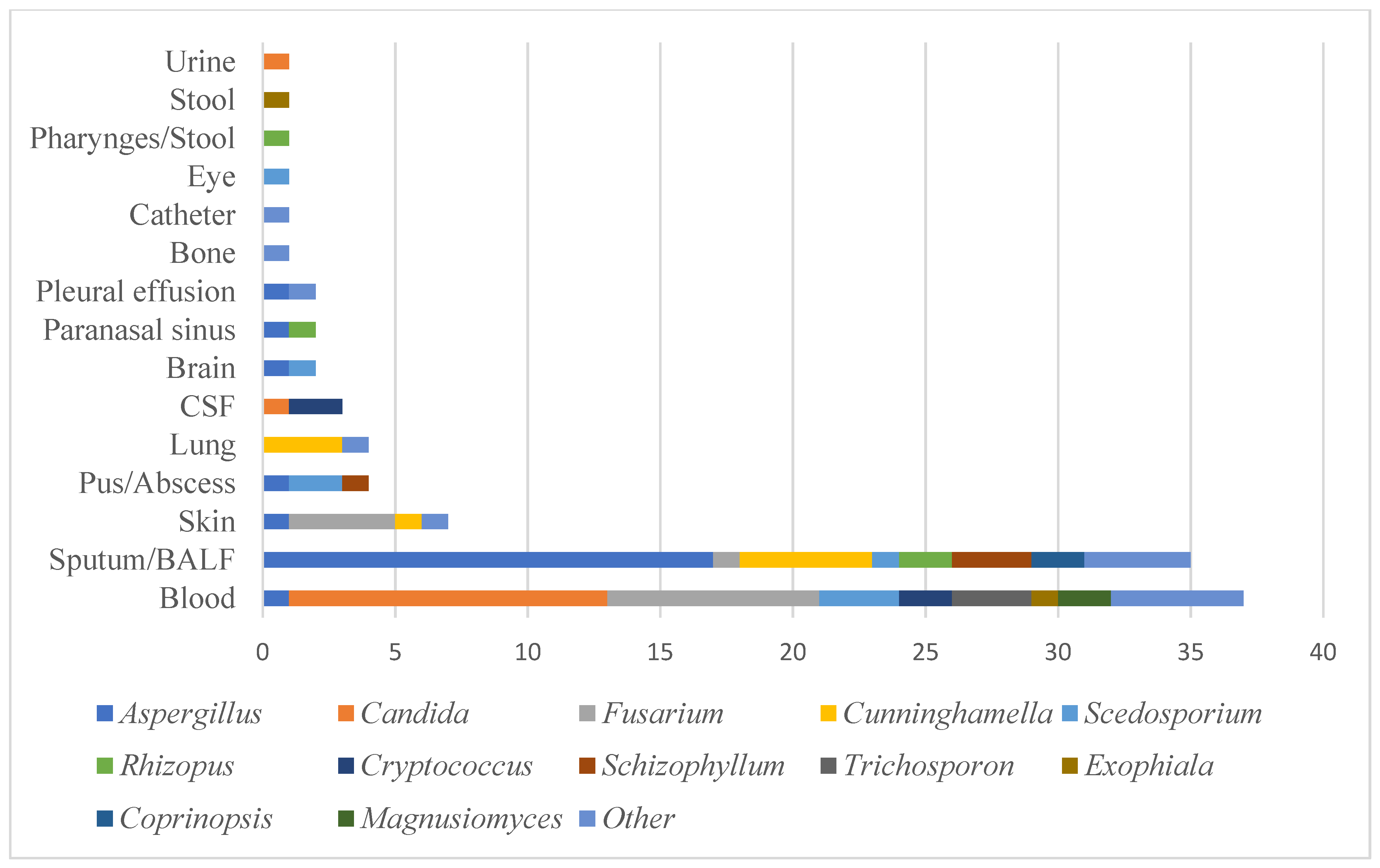
3.2. Causative Species of IFD
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cornely, O.A.; Gachot, B.; Akan, H.; Bassetti, M.; Uzun, O.; Kibbler, C.; Marchetti, O.; De Burghgraeve, P.; Ramadan, S.; Pylkkanen, L.; et al. Epidemiology and Outcome of Fungemia in a Cancer Cohort of the Infectious Diseases Group (IDG) of the European Organization for Research and Treatment of Cancer (EORTC 65031). Clin. Infect. Dis. 2015, 61, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Barreto, J.N.; Beach, C.L.; Wolf, R.C.; Merten, J.A.; Tosh, P.K.; Wilson, J.W.; Hogan, W.J.; Litzow, M.R. The incidence of invasive fungal infections in neutropenic patients with acute leukemia and myelodysplastic syndromes receiving primary antifungal prophylaxis with voriconazole. Am. J. Hematol. 2013, 88, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Prentice, H.G.; Kibbler, C.C.; Prentice, A.G. Towards a targeted, risk-based, antifungal strategy in neutropenic patients. Br. J. Haematol. 2000, 110, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-K.; Cho, S.-Y.; Yoon, S.-S.; Moon, J.-H.; Kim, S.-H.; Lee, J.-H.; Kim, J.S.; Cheong, J.-W.; Jang, J.-H.; Seo, B.-J.; et al. Epidemiology and Risk Factors for Invasive Fungal Diseases among Allogeneic Hematopoietic Stem Cell Transplant Recipients in Korea: Results of “RISK” Study. Biol. Blood Marrow Transplant. 2017, 23, 1773–1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kontoyiannis, D.P.; Marr, K.A.; Park, B.J.; Alexander, B.D.; Anaissie, E.J.; Walsh, T.J.; Ito, J.; Andes, D.R.; Baddley, J.W.; Brown, J.M.; et al. Prospective Surveillance for Invasive Fungal Infections in Hematopoietic Stem Cell Transplant Recipients, 2001–2006: Overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin. Infect. Dis. 2010, 50, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Montesinos, P.; Rodríguez-Veiga, R.; Boluda, B.; Martínez-Cuadrón, D.; Cano, I.; Lancharro, A.; Sanz, J.; Arilla, M.J.; López-Chuliá, F.; Navarro, I.; et al. Incidence and risk factors of post-engraftment invasive fungal disease in adult allogeneic hematopoietic stem cell transplant recipients receiving oral azoles prophylaxis. Bone Marrow Transplant. 2015, 50, 1465–1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, P.; Jiang, E.-L.; Yang, D.-L.; Yan, Z.-S.; Huang, Y.; Wei, J.-L.; Wang, M.; Ma, Q.-L.; Liu, Q.-G.; Zou, D.-H.; et al. Risk factors and prognosis of invasive fungal infections in allogeneic stem cell transplantation recipients: A single-institution experience. Transpl. Infect. Dis. 2010, 12, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.A.; Girmenia, C.; Brüggemann, R.J.; Duarte, R.F.; Kibbler, C.C.; Ljungman, P.; Racil, Z.; Ribaud, P.; Slavin, M.; Cornely, O.A.; et al. European guidelines for primary antifungal prophylaxis in adult haematology patients: Summary of the updated recommendations from the European Conference on Infections in Leukaemia. J. Antimicrob. Chemother. 2018, 73, 3221–3230. [Google Scholar] [CrossRef]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.E.; Verweij, P.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24, e1–e38. [Google Scholar] [CrossRef] [Green Version]
- Hino, Y.; Muraosa, Y.; Oguchi, M.; Yahiro, M.; Yarita, K.; Watanabe, A.; Sakaida, E.; Yokote, K.; Kamei, K. Drain outlets in patient rooms as sources for invasive fusariosis: An analysis of patients with haematological disorders. J. Hosp. Infect. 2020, 105, 518–526. [Google Scholar] [CrossRef]
- Muraosa, Y.; Oguchi, M.; Yahiro, M.; Watanabe, A.; Yaguchi, T.; Kamei, K. Epidemiological Study of Fusarium Species Causing Invasive and Superficial Fusariosis in Japan. Med. Mycol. J. 2017, 58, E5–E13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin. Infect. Dis. 2008, 46, 1813–1821. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, K.; Humber, R.A.; Geiser, D.M.; Kang, S.; Park, B.; Robert, V.A.R.G.; Crous, P.W.; Johnston, P.R.; Aoki, T.; Rooney, A.P.; et al. Phylogenetic diversity of insecticolous fusaria inferred from multilocus DNA sequence data and their molecular identification via FUSARIUM-ID and Fusarium MLST. Mycologia 2012, 104, 427–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miceli, M.H.; Churay, T.; Braun, T.; Kauffman, C.A.; Couriel, D.R. Risk Factors and Outcomes of Invasive Fungal Infections in Allogeneic Hematopoietic Cell Transplant Recipients. Mycopathologia 2017, 182, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Guarro, J. Fusariosis, a complex infection caused by a high diversity of fungal species refractory to treatment. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 1491–1500. [Google Scholar] [CrossRef] [PubMed]
- Nucci, M.; Garnica, M.; Gloria, A.B.; Lehugeur, D.S.; Dias, V.C.; Palma, L.C.; Cappellano, P.; Fertrin, K.Y.; Carlesse, F.; Simoes, B.; et al. Invasive fungal diseases in haematopoietic cell transplant recipients and in patients with acute myeloid leukaemia or myelodysplasia in Brazil. Clin. Microbiol. Infect. 2013, 19, 745–751. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | No. (%) |
|---|---|
| Gender | |
| Male | 67 (65.7) |
| Female | 35 (34.3) |
| Age yrs, median (range) | 57.5 (0–84) |
| Underlying diseases | |
| Acute myeloid leukemia (AML) | 35 (34.3) |
| Acute lymphoblastic leukemia (ALL) | 18 (17.6) |
| Malignant lymphoma (ML) | 12 (11.8) |
| Myelodysplastic syndrome (MDS) | 11 (10.8) |
| Adult T-cell leukemia-lymphoma (ATL) | 5 (4.9) |
| Multiple myeloma (MM) | 5 (4.9) |
| Chronic granulomatous disease (CGD) | 4 (3.9) |
| Chronic active EBV infection (CAEBV) | 2 (1.9) |
| Chronic myeloid leukemia (CML) | 2 (1.9) |
| Idiopathic thrombocytopenic purpura (ITP) | 2 (1.9) |
| Primary myelofibrosis (PMF) | 2 (1.9) |
| Waldenstrom Macroglobulinemia (WM) | 2 (1.9) |
| Aplastic anemia (AA) | 1 (1.0) |
| Hemophagocytic lymphohistiocytosis (HLH) | 1 (1.0) |
| Underlying Diseases | Non-HSCT | Allogeneic HSCT | Autologous SCT |
|---|---|---|---|
| AML | 24 | 11 | 0 |
| ALL | 7 | 11 | 0 |
| ML | 10 | 2 | 0 |
| MDS | 5 | 6 | 0 |
| ATL | 3 | 2 | 0 |
| MM | 0 | 1 | 4 |
| CGD | 1 | 3 | 0 |
| CAEBV | 1 | 1 | 0 |
| CML | 1 | 1 | 0 |
| ITP | 2 | 0 | 0 |
| PMF | 0 | 2 | 0 |
| WM | 1 | 1 | 0 |
| AA | 0 | 1 | 0 |
| HLH | 0 | 1 | 0 |
| Total | 55 | 43 | 4 |
| Genus | Non-HSCT | HSCT | Total |
|---|---|---|---|
| Aspergillus | 12 | 11 | 23 |
| Candida | 9 | 5 | 14 |
| Fusarium | 6 | 7 | 13 |
| Cunninghamella | 5 | 4 | 9 |
| Scedosporium | 6 | 2 | 8 |
| Rhizopus | 1 | 3 | 4 |
| Schizophyllum | 2 | 2 | 4 |
| Cryptococcus | 3 | 1 | 4 |
| Trichosporon | 1 | 2 | 3 |
| Exophiala | 1 | 1 | 2 |
| Coprinopsis | 1 | 1 | 2 |
| Magnusiomyces | 2 | 2 | |
| Scopulariopsis | 1 | 1 | |
| Prototheca | 1 | 1 | |
| Peroneutypa | 1 | 1 | |
| Paecilomyces | 1 | 1 | |
| Mucor | 1 | 1 | |
| Trametes | 1 | 1 | |
| Microsphaeropsis | 1 | 1 | |
| Lomentospora | 1 | 1 | |
| Isaria | 1 | 1 | |
| Apiotrichum | 1 | 1 | |
| Acremonium | 1 | 1 | |
| Rhodotorula | 1 | 1 | |
| Ochroconis | 1 | 1 | |
| Gymnoascus | 1 | 1 |
| Species | No. |
|---|---|
| Aspergillus | |
| Aspergillus fumigatus | 10 |
| Aspergillus flavus | 2 |
| Aspergillus terreus | 2 |
| Aspergillus viridinutans | 2 |
| Aspergillus udagawae | 2 |
| Aspergillus creber | 1 |
| Aspergillus niger | 1 |
| Aspergillus siamensis | 1 |
| Aspergillus tubingensis | 1 |
| Aspergillus unguis | 1 |
| Candida | |
| Candida fermentati | 4 |
| Candida glabrata | 2 |
| Candida palmioleophila | 2 |
| Candida parapsilosis | 2 |
| Candida guilliermondii | 2 |
| Candida albicans | 1 |
| Candida orthopsilosis | 1 |
| Fusarium | |
| Fusarium petroliphilum | 5 |
| Fusarium keratoplasticum | 2 |
| Fusarium solani sensu stricto | 2 |
| Fusarium fujikuroi | 1 |
| Fusarium equiseti | 1 |
| Fusarium falciforme | 1 |
| Fusarium solani (species complex) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hino, Y.; Watanabe, A.; Seki, R.; Tsukamoto, S.; Takeda, Y.; Sakaida, E.; Kamei, K. A Reference Laboratory Surveillance on Fungal Isolates from Patients with Haematological Malignancy in Japan. J. Fungi 2021, 7, 806. https://doi.org/10.3390/jof7100806
Hino Y, Watanabe A, Seki R, Tsukamoto S, Takeda Y, Sakaida E, Kamei K. A Reference Laboratory Surveillance on Fungal Isolates from Patients with Haematological Malignancy in Japan. Journal of Fungi. 2021; 7(10):806. https://doi.org/10.3390/jof7100806
Chicago/Turabian StyleHino, Yutaro, Akira Watanabe, Rio Seki, Shokichi Tsukamoto, Yusuke Takeda, Emiko Sakaida, and Katsuhiko Kamei. 2021. "A Reference Laboratory Surveillance on Fungal Isolates from Patients with Haematological Malignancy in Japan" Journal of Fungi 7, no. 10: 806. https://doi.org/10.3390/jof7100806
APA StyleHino, Y., Watanabe, A., Seki, R., Tsukamoto, S., Takeda, Y., Sakaida, E., & Kamei, K. (2021). A Reference Laboratory Surveillance on Fungal Isolates from Patients with Haematological Malignancy in Japan. Journal of Fungi, 7(10), 806. https://doi.org/10.3390/jof7100806