Underlying Conditions and Clinical Spectrum of Chronic Pulmonary Aspergillosis (CPA): An Experience from a Tertiary Care Hospital in Karachi, Pakistan


Abstract
1. Introduction
2. Material and Methods
2.1. Study Design and Settings
2.2. Statistical Analysis
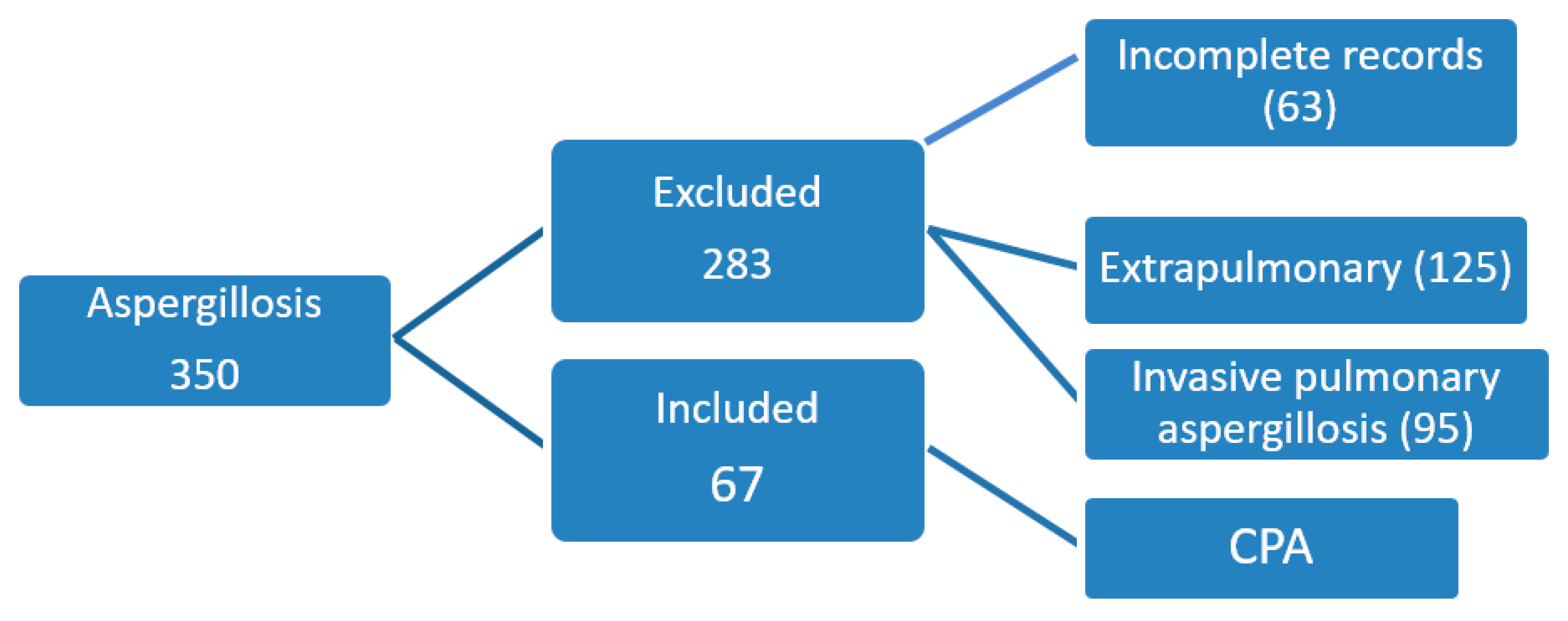
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Denning, D.W.; Pleuvry, A.; Cole, D.C. Global burden of chronic pulmonary aspergillosis as a sequel to pulmonary tuberculosis. Bull. World Health Organ. 2011, 89, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Denning, D.W.; Chakrabarti, A. Estimation of the burden of chronic and allergic pulmonary aspergillosis in India. PLoS ONE 2014, 9, e114745. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C. European Society for Clinical Microbiology and Infectious Diseases and European Respiratory Society. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management. Eur. Respir. J. 2016, 47, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.L.; Denning, D.W. Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma. Eur. Respir. J. 2011, 37, 65–872. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Riniotis, K.; Dobrashian, R.; Sambatakou, H. Chronic cavitary and fibrosing pulmonary and pleural aspergillosis: Case series, proposed nomenclature change, and review. Clin. Infect. Dis. 2003, 37, S265–S280. [Google Scholar] [CrossRef]
- Tashiro, T.; Izumikawa, K.; Tashiro, M.; Takazono, T.; Morinaga, Y.; Yamamoto, K.; Imamura, Y.; Miyazaki, T.; Seki, M.; Kakeya, H.; et al. Diagnostic significance of Aspergillus species isolated from respiratory samples in an adult pneumology ward. Med. Mycol. 2011, 49, 581–587. [Google Scholar] [CrossRef]
- Shahid, M.; Malik, A.; Bhargava, R. Prevalence of aspergillosis in chronic lung diseases. Indian J. Med. Microbiol. 2001, 19, 201–205. [Google Scholar]
- British Thoracic and Tuberculosis Association. Aspergilloma and residual tuberculous cavities—The results of a resurvey. Tubercle 1970, 51, 227–245. [Google Scholar] [CrossRef]
- Page, I.D.; Byanyima, R.; Hosmane, S.; Onyachi, N.; Opira, C.; Richardson, M.; Sawyer, R.; Sharman, A.; Denning, D.W. Chronic pulmonary aspergillosis commonly complicates treated pulmonary tuberculosis with residual cavitation. Eur. Resp. J. 2019, 53, 1801184. [Google Scholar] [CrossRef]
- Sehgal, I.S.; Dhooria, S.; Choudhary, H.; Aggarwal, A.N.; Garg, M.; Chakrabarti, A.; Agarwal, R. Efficiency of A fumigatus-specific IgG and galactomannan testing in the diagnosis of simple aspergilloma. Mycoses 2019, 62, 1108–1115. [Google Scholar] [CrossRef]
- Beltrán Rodríguez, N.; San Juan-Galán, J.L.; Fernández Andreu, C.M.; María Yera, D.; Barrios Pita, M.; Perurena Lancha, M.R.; Velar Martínez, R.E.; Illnait Zaragozí, M.T.; Martínez Machín, G.F. Chronic Pulmonary Aspergillosis in Patients with Underlying Respiratory Disorders in Cuba—A Pilot Study. J. Fungi 2019, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Jabeen, K.; Farooqi, J.; Mirza, S.; Denning, D.W.; Zafar, A. Serious fungal infections in Pakistan. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Setianingrum, F.; Rautemaa-Richardson, R.; Shah, R.; Denning, D.W. Clinical outcome of chronic pulmonary aspergillosis patients managed surgically. In Proceedings of the 9th Trends in Medical Mycology Conference, Nice, France, 11–14 October 2019. J. Fungi 2019, 5, 95. [Google Scholar] [CrossRef]
- Denning, D.W.; Page, I.D.; Chakaya, J.; Jabeen, K.; Jude, C.M.; Cornet, M.; Alastruey-Izquierdo, A.; Bongomin, F.; Bowyer, P.; Chakrabarti, A.; et al. Case definition of chronic pulmonary aspergillosis in resource-constrained settings. Emerg. Infect. Dis. 2018, 24. [Google Scholar] [CrossRef]
- Kosmidis, C.; Denning, D.W. The clinical spectrum of pulmonary aspergillosis. Thorax 2015, 70, 270–277. [Google Scholar] [CrossRef]
- Tamura, A.; Suzuki, J.; Fukami, T.; Matsui, H.; Akagawa, S.; Ohta, K.; Hebisawa, A.; Takahashi, F. Chronic pulmonary aspergillosis as a sequel to lobectomy for lung cancer. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 650–656. [Google Scholar] [CrossRef]
- Hayes, G.E.; Novak-Frazer, L. Chronic Pulmonary Aspergillosis—Where Are We? And Where Are We Going? J. Fungi 2016, 2, 18. [Google Scholar] [CrossRef]
- Dooley, K.E.; Chaisson, R.E. Tuberculosis and diabetes mellitus: Convergence of two epidemics. Lancet Infect. Dis. 2009, 9, 737–746. [Google Scholar] [CrossRef]
- Jiménez-Corona, M.E.; Cruz-Hervert, L.P.; García-García, L.; Ferreyra-Reyes, L.; Delgado-Sánchez, G.; Bobadilla-Del-Valle, M.; Canizales-Quintero, S.; Ferreira-Guerrero, E.; Báez-Saldaña, R.; Téllez-Vázquez, N.; et al. Association of diabetes and tuberculosis: Impact on treatment and post-treatment outcomes. Thorax 2013, 68, 214–220. [Google Scholar] [CrossRef]
- Baker, M.A.; Harries, A.D.; Jeon, C.Y.; Hart, J.E.; Kapur, A.; Lönnroth, K.; Ottmani, S.E.; Goonesekera, S.D.; Murray, M.B. The impact of diabetes on tuberculosis treatment outcomes: A systematic review. The impact of diabetes on tuberculosis treatment outcomes: A systematic review. BMC. Med. 2011, 9, 81. [Google Scholar] [CrossRef]
- Uffredi, M.L.; Mangiapan, G.; Cadranel, J.; Kac, G. Significance of Aspergillus fumigatus isolation from respiratory specimens of nongranulocytopenic patients. Eur. J. Clin. Microbiol. Infect. Dis. 2003, 22, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Kurashima, A.; Kamei, K.; Oritsu, M.; Ando, T.; Yamamoto, T.; Niki, Y. Efficacy and safety of short- and long-term treatment of itraconazole on chronic necrotizing pulmonary aspergillosis in multicenter study. J. Infect. Chemother. 2012, 18, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Vishwanath, G.; Aggarwal, A.N.; Garg, M.; Gupta, D.; Chakrabarti, A. Itraconazole in chronic cavitary pulmonary aspergillosis: A randomised controlled trial and systematic review of literature. Mycoses 2013, 56, 559–570. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total n = 67 | Percentage |
|---|---|---|
| Age (Mean) | 45.9 ± 15 years | |
| Gender | ||
| Male | 44 | 65.7% |
| Female | 23 | 34.3% |
| Smoking status | ||
| Ex-smoker | 21 | 31.3% |
| Non-Smoker | 46 | 68.7% |
| Current smoker | 0 | - |
| Clinical Symptoms | ||
| Cough | 55 | 82.0% |
| Hemoptysis | 40 | 59.7% |
| Weight loss | 34 | 50.7% |
| Dyspnea | 24 | 35.8% |
| Fever | 22 | 32.8% |
| Anorexia | 7 | 10.4% |
| Chest pain | 9 | 13.4% |
| Associated Condition | n = 33 | 49.3% |
| DM | 19 | 28.4% |
| CLD | 2 | 3.0% |
| CRF | 2 | 3.0% |
| Malignancy | 3 | 4.5% |
| Inhaled steroid | 14 | 20.9% |
| Oral steroid | 11 | 16.4% |
| Underlying Lung Condition | ||
| Previous TB | 58 | 86.6% |
| ABPA bronchiectasis | 8 | 11.9% |
| Post-pneumonia bronchiectasis | 6 | 8.9% |
| COPD | 7 | 10.4% |
| Previous CTS surgery | 5 | 7.4% |
| Active TB | 2 | 2.9% |
| ILD | 2 | 2.9% |
| Sarcoidosis | 1 | 1.4% |
| Granulomatous polyangiitis | 1 | 1.4% |
| Diagnostic criteria | ||
| Clinical + Radiographic+ Histopathology | 28 | 41.7% |
| Clinical + Radiographic + Microbiology | 35 | 49.2% |
| Clinical + Radiographic+ Histopathology + Microbiology | 6 | 8.9% |
| n = Number | Percentage (%) | |
|---|---|---|
| Types of CPA | ||
| Simple aspergilloma | 33 | 49.2% |
| CCPA | 30 | 44.7% |
| CFPA | 3 | 4.4% |
| SAIA | 1 | 1.4% |
| Aspergillus species | n =39 | |
| A. fumigatus A. flavus A. niger A. terreus | 13 17 12 7 | 33.3% 43.5% 30.7% 17.9% |
| Two or more Aspergillus species A flavus + A. niger + A. terreus A. flavus + A. niger A. flavus + A. niger + A. fumigatus | 8/39 3 4 1 | 20.5% 20.0% 40.0% 10.0% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iqbal, N.; Irfan, M.; Mushtaq, A.; Jabeen, K. Underlying Conditions and Clinical Spectrum of Chronic Pulmonary Aspergillosis (CPA): An Experience from a Tertiary Care Hospital in Karachi, Pakistan. J. Fungi 2020, 6, 41. https://doi.org/10.3390/jof6020041
Iqbal N, Irfan M, Mushtaq A, Jabeen K. Underlying Conditions and Clinical Spectrum of Chronic Pulmonary Aspergillosis (CPA): An Experience from a Tertiary Care Hospital in Karachi, Pakistan. Journal of Fungi. 2020; 6(2):41. https://doi.org/10.3390/jof6020041
Chicago/Turabian StyleIqbal, Nousheen, Muhammad Irfan, Ammar Mushtaq, and Kauser Jabeen. 2020. "Underlying Conditions and Clinical Spectrum of Chronic Pulmonary Aspergillosis (CPA): An Experience from a Tertiary Care Hospital in Karachi, Pakistan" Journal of Fungi 6, no. 2: 41. https://doi.org/10.3390/jof6020041
APA StyleIqbal, N., Irfan, M., Mushtaq, A., & Jabeen, K. (2020). Underlying Conditions and Clinical Spectrum of Chronic Pulmonary Aspergillosis (CPA): An Experience from a Tertiary Care Hospital in Karachi, Pakistan. Journal of Fungi, 6(2), 41. https://doi.org/10.3390/jof6020041