Antifungal Susceptibly Testing by Concentration Gradient Strip Etest Method for Fungal Isolates: A Review



Abstract
1. Introduction
2. Principle of the Concentration Gradient Strip (Etest)
3. Etest as a Routine AFST Method
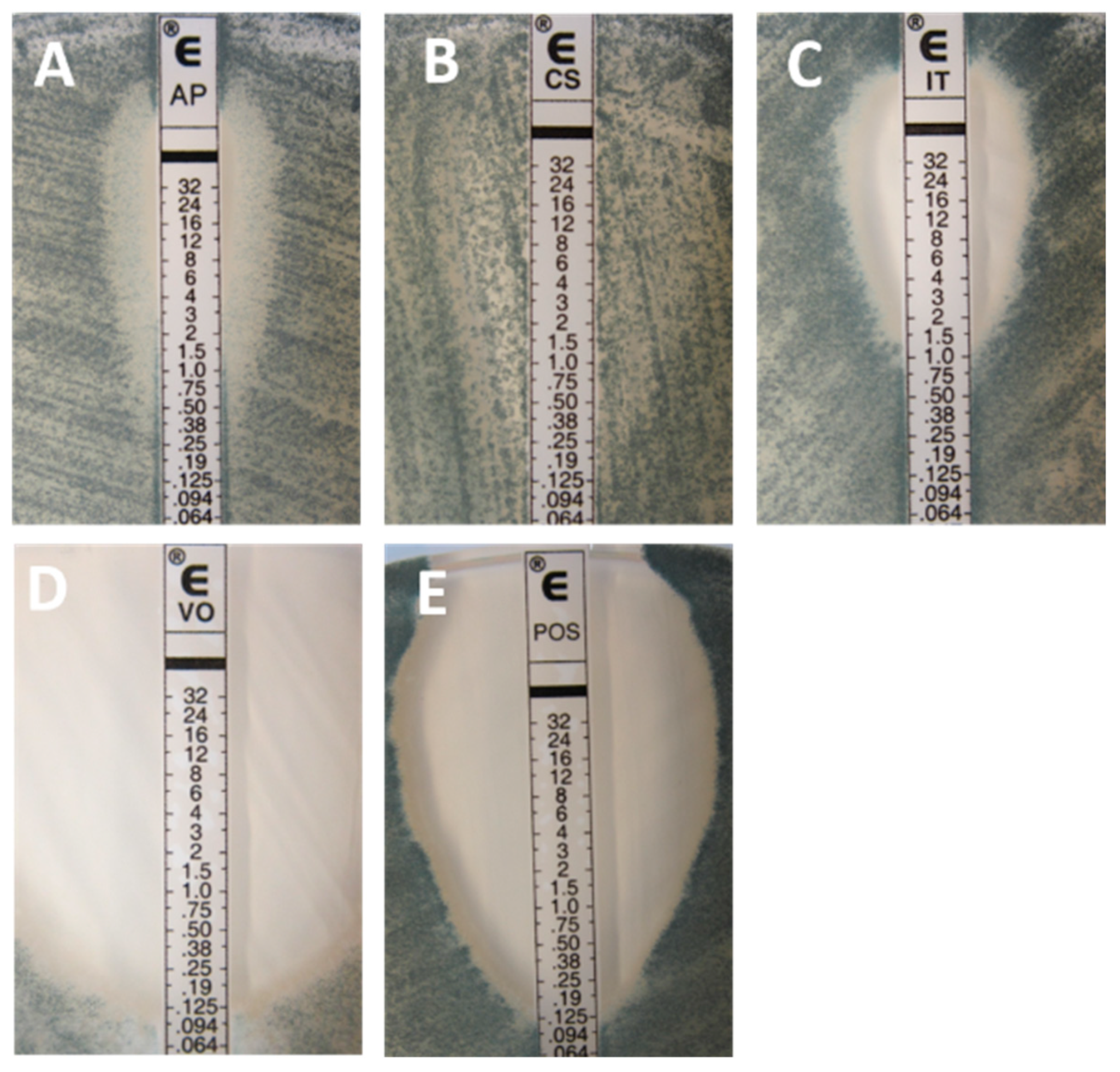
3.1. Inhibition Patterns and Reading Problems
3.2. Interlaboratory Reproducibility
3.3. Correlation with Reference Techniques
3.3.1. Yeasts
Amphotericin B
Flucytosine
The Triazoles
- Fluconazole
- Itraconazole, Posaconazole, and Voriconazole
The Echinocandins
Evaluation of EA According to MIC Ranges
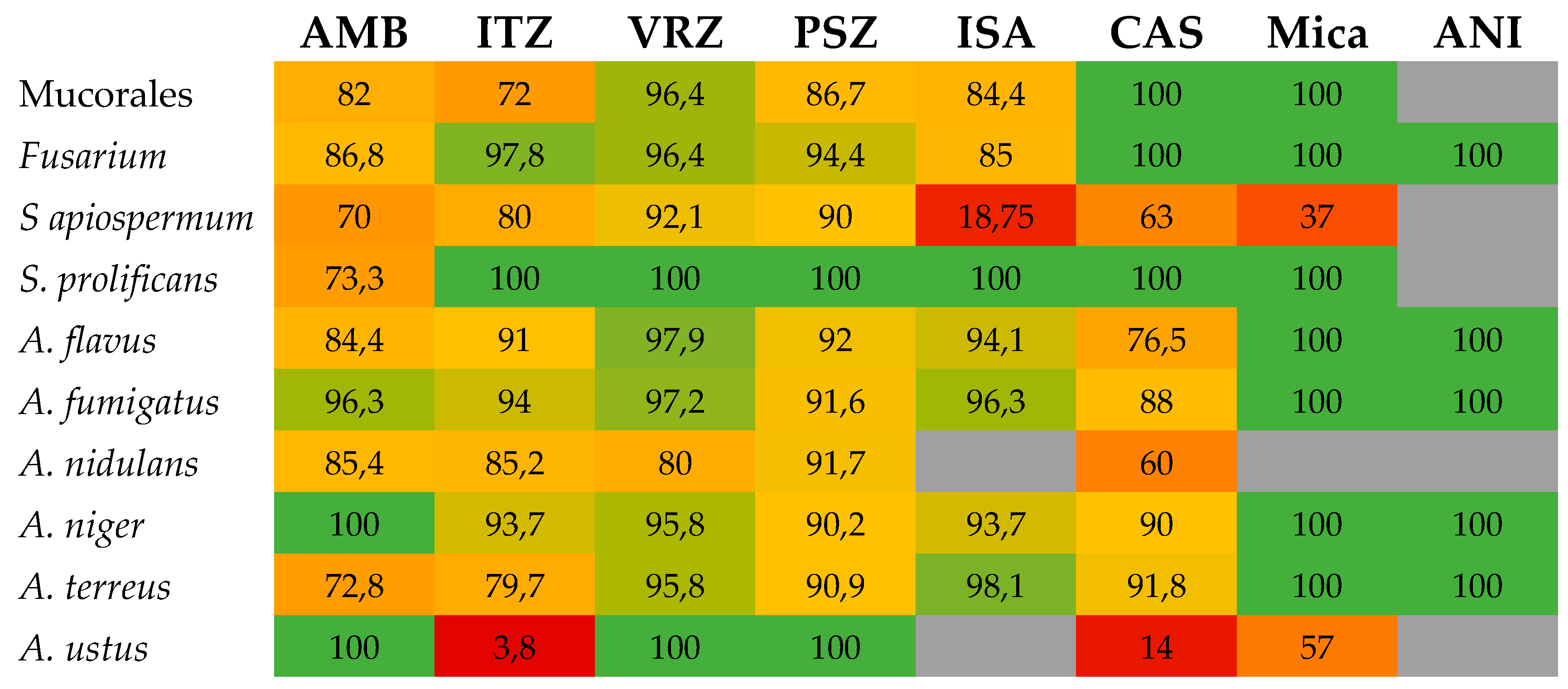
3.3.2. Filamentous Fungi
Aspergillus spp.
Mucorales
Fusarium spp.
Scedosporium
3.4. Ability to Detect Acquired Resistance
3.5. Etest for Direct Antifungal Susceptibility Testing on Blood Samples
3.6. Etest Specific ECVs
4. Etest as an AFST Research Tool
Combination Studies
5. Conclusions and Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Arendrup, M.C.; Bille, J.; Dannaoui, E.; Ruhnke, M.; Heussel, C.P.; Kibbler, C. ECIL-3 classical diagnostic procedures for the diagnosis of invasive fungal diseases in patients with leukaemia. Bone Marrow Transpl. 2012, 47, 1030–1045. [Google Scholar] [CrossRef] [PubMed]
- Cuenca-Estrella, M.; Verweij, P.E.; Arendrup, M.C.; Arikan-Akdagli, S.; Bille, J.; Donnelly, J.P.; Jensen, H.E.; Lass-Florl, C.; Richardson, M.D.; Akova, M.; et al. ESCMID* guideline for the diagnosis and management of Candida diseases 2012: Diagnostic procedures. Clin. Microbiol. Infect. 2012, 18 (Suppl. 7), 9–18. [Google Scholar] [CrossRef]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Florl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24 (Suppl. 1), e1–e38. [Google Scholar] [CrossRef] [PubMed]
- Arendrup, M.C.; Boekhout, T.; Akova, M.; Meis, J.F.; Cornely, O.A.; Lortholary, O.; European Society of Clinical Microbiology and Infectious Diseases Fungal Infection Study Group; European Confederation of Medical Mycology. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of rare invasive yeast infections. Clin. Microbiol. Infect. 2014, 20 (Suppl. 3), 76–98. [Google Scholar] [CrossRef]
- Chowdhary, A.; Meis, J.F.; Guarro, J.; de Hoog, G.S.; Kathuria, S.; Arendrup, M.C.; Arikan-Akdagli, S.; Akova, M.; Boekhout, T.; Caira, M.; et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of systemic phaeohyphomycosis: Diseases caused by black fungi. Clin. Microbiol. Infect. 2014, 20 (Suppl. 3), 47–75. [Google Scholar] [CrossRef]
- Cornely, O.A.; Arikan-Akdagli, S.; Dannaoui, E.; Groll, A.H.; Lagrou, K.; Chakrabarti, A.; Lanternier, F.; Pagano, L.; Skiada, A.; Akova, M.; et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of mucormycosis 2013. Clin. Microbiol. Infect. 2014, 20 (Suppl. 3), 5–26. [Google Scholar] [CrossRef]
- Tortorano, A.M.; Richardson, M.; Roilides, E.; van Diepeningen, A.; Caira, M.; Munoz, P.; Johnson, E.; Meletiadis, J.; Pana, Z.D.; Lackner, M.; et al. ESCMID and ECMM joint guidelines on diagnosis and management of hyalohyphomycosis: Fusarium spp., Scedosporium spp. and others. Clin. Microbiol. Infect. 2014, 20 (Suppl. 3), 27–46. [Google Scholar] [CrossRef] [PubMed]
- Arendrup, M.C.; Meletiadis, J.; Mouton, J.W.; Lagrou, K.; Hamal, P.; Guinea, J.; Subcommittee on Antifungal Susceptibility Testing (AFST) of the ESCMID European Committee for Antimicrobial Susceptibility Testing (EUCAST). Method for the determination of broth dilution minimum inhibitory concentrations of antifungal agents for yeasts. EUCAST Definitive Document E.Def 7.3.1. 2017. Available online: http://www.eucast.org/astoffungi/methodsinantifungalsusceptibilitytesting/susceptibility_testing_of_yeasts/ (accessed on 15 September 2019).
- Clinical and laboratory Standards Institute (CLSI). Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts, Approved Standard, 3rd ed.; CLSI document M27-A3; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008. [Google Scholar]
- Arendrup, M.C.; Meletiadis, J.; Mouton, J.W.; Lagrou, K.; Hamal, P.; Guinea, J.; Subcommittee on Antifungal Susceptibility Testing (AFST) of the ESCMID European Committee for Antimicrobial Susceptibility Testing (EUCAST). Method for the determination of broth dilution minimum inhibitory concentrations of antifungal agents for conidia forming moulds. EUCAST Definitive Document E.Def 9.3.1. 2017. Available online: http://www.eucast.org/astoffungi/methodsinantifungalsusceptibilitytesting/susceptibility_testing_of_moulds/ (accessed on 15 September 2019).
- Clinical and laboratory Standards Institute (CLSI). Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi, 2nd ed.; Approved standard. Document M-38A2; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008. [Google Scholar]
- bioMérieux SA. Etest Antifungal Susceptibility Testing Package Insert; bioMérieux SA: Marcy-l’Etoile, France, 2013. [Google Scholar]
- AB Biodisk. Etest for MIC Determination of Antifungal Agents: Reading Guide for Yeast; AB Biodisk: Solna, Sweden, 2006. [Google Scholar]
- bioMérieux SA. Etest Technical Guide No.10. Antifungal Susceptibility Testing of Moulds; bioMérieux SA: Marcy-l'Étoile, France, 2011. [Google Scholar]
- Arthington-Skaggs, B.A.; Lee-Yang, W.; Ciblak, M.A.; Frade, J.P.; Brandt, M.E.; Hajjeh, R.A.; Harrison, L.H.; Sofair, A.N.; Warnock, D.W. Comparison of visual and spectrophotometric methods of broth microdilution MIC end point determination and evaluation of a sterol quantitation method for in vitro susceptibility testing of fluconazole and itraconazole against trailing and nontrailing Candida isolates. Antimicrob. Agents Chemother. 2002, 46, 2477–2481. [Google Scholar] [PubMed]
- Stevens, D.A.; Espiritu, M.; Parmar, R. Paradoxical effect of caspofungin: Reduced activity against Candida albicans at high drug concentrations. Antimicrob. Agents Chemother. 2004, 48, 3407–3411. [Google Scholar] [CrossRef]
- Wagener, J.; Loiko, V. Recent insights into the paradoxical effect of echinocandins. J. Fungi 2017, 4. [Google Scholar] [CrossRef]
- Khlif, M.; Bogreau, H.; Michel-Nguyen, A.; Ayadi, A.; Ranque, S. Trailing or paradoxical growth of Candida albicans when exposed to caspofungin is not associated with microsatellite genotypes. Antimicrob. Agents Chemother. 2010, 54, 1365–1368. [Google Scholar] [CrossRef] [PubMed]
- Chamilos, G.; Lewis, R.E.; Albert, N.; Kontoyiannis, D.P. Paradoxical effect of echinocandins across Candida species in vitro: Evidence for echinocandin-specific and Candida species-related differences. Antimicrob. Agents Chemother. 2007, 51, 2257–2259. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Zambrano, L.J.; Escribano, P.; Sanchez-Carrillo, C.; Bouza, E.; Guinea, J. Frequency of the paradoxical effect measured using the EUCAST procedure with micafungin, anidulafungin, and caspofungin against Candida species isolates causing candidemia. Antimicrob. Agents Chemother. 2017, 61. [Google Scholar] [CrossRef] [PubMed]
- Rueda, C.; Puig-Asensio, M.; Guinea, J.; Almirante, B.; Cuenca-Estrella, M.; Zaragoza, O.; CANDIPOP Project from GEIH-GEMICOMED (SEIMC) and REIPI. Evaluation of the possible influence of trailing and paradoxical effects on the clinical outcome of patients with candidemia. Clin. Microbiol. Infect. 2017, 23, 49e1–49e8. [Google Scholar] [CrossRef] [PubMed]
- Siopi, M.; Tsala, M.; Siafakas, N.; Zerva, L.; Meletiadis, J. Evaluation of the "dip effect" phenomenon in antifungal susceptibility testing of Candida spp. against echinocandins by use of gradient concentration strips. J. Clin. Microbiol. 2015, 53, 3654–3659. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A. Evaluation of broth microdilution testing parameters and agar diffusion Etest procedure for testing susceptibilities of Aspergillus spp. to caspofungin acetate (MK-0991). J. Clin. Microbiol. 2003, 41, 403–409. [Google Scholar] [CrossRef]
- Dannaoui, E.; Abdul, M.; Arpin, M.; Michel-Nguyen, A.; Piens, M.A.; Favel, A.; Lortholary, O.; Dromer, F. Results obtained with various antifungal susceptibility testing methods do not predict early clinical outcome in patients with cryptococcosis. Antimicrob. Agents Chemother. 2006, 50, 2464–2470. [Google Scholar] [CrossRef]
- Dannaoui, E.; Paugam, A.; Develoux, M.; Chochillon, C.; Matheron, J.; Datry, A.; Bouges-Michel, C.; Bonnal, C.; Dromer, F.; Bretagne, S. Comparison of antifungal MICs for yeasts obtained using the EUCAST method in a reference laboratory and the Etest in nine different hospital laboratories. Clin. Microbiol. Infect. 2010, 16, 863–869. [Google Scholar] [CrossRef]
- Warnock, D.W.; Johnson, E.M.; Rogers, T.R. Multi-centre evaluation of the Etest method for antifungal drug susceptibility testing of Candida spp. and Cryptococcus neoformans. BSAC Working Party on Antifungal Chemotherapy. J. Antimicrob. Chemother. 1998, 42, 321–331. [Google Scholar] [CrossRef][Green Version]
- Espinel-Ingroff, A.; Pfaller, M.; Erwin, M.E.; Jones, R.N. Interlaboratory evaluation of Etest method for testing antifungal susceptibilities of pathogenic yeasts to five antifungal agents by using Casitone agar and solidified RPMI 1640 medium with 2% glucose. J. Clin. Microbiol. 1996, 34, 848–852. [Google Scholar]
- Pfaller, M.A.; Messer, S.A.; Bolmstrom, A.; Odds, F.C.; Rex, J.H. Multisite reproducibility of the Etest MIC method for antifungal susceptibility testing of yeast isolates. J. Clin. Microbiol. 1996, 34, 1691–1693. [Google Scholar] [PubMed]
- Ranque, S.; Lachaud, L.; Gari-Toussaint, M.; Michel-Nguyen, A.; Mallie, M.; Gaudart, J.; Bertout, S. Interlaboratory reproducibility of Etest amphotericin B and caspofungin yeast susceptibility testing and comparison with the CLSI method. J. Clin. Microbiol. 2012, 50, 2305–2309. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Messer, S.A.; Bolmstrom, A. Evaluation of Etest for determining in vitro susceptibility of yeast isolates to amphotericin B. Diagn. Microbiol. Infect. Dis. 1998, 32, 223–227. [Google Scholar] [CrossRef]
- Wanger, A.; Mills, K.; Nelson, P.W.; Rex, J.H. Comparison of Etest and National Committee for Clinical Laboratory Standards broth macrodilution method for antifungal susceptibility testing: Enhanced ability to detect amphotericin B-resistant Candida isolates. Antimicrob. Agents Chemother. 1995, 39, 2520–2522. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, F.E.; Dias, A.L.; Melhem, M.S.; Szeszs, M.W.; Auler, M.E.; Ruiz, L.S.; Goncalves da Silva, E.; Gandra, R.F.; Paula, C.R. Antifungal susceptibility of bloodstream yeasts isolated at a public children's hospital in Brazil: Comparison of the Etest and the AFST-EUCAST microdilution method. Can. J. Microbiol. 2007, 53, 1300–1306. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Chiu, M.; Nelson, P.W.; Lancaster, M.; Pfaller, M.A.; Rex, J.H. Lot-to-lot variability of antibiotic medium 3 used for testing susceptibility of Candida isolates to amphotericin B. J. Clin. Microbiol. 1997, 35, 270–272. [Google Scholar] [PubMed]
- Alexander, B.D.; Byrne, T.C.; Smith, K.L.; Hanson, K.E.; Anstrom, K.J.; Perfect, J.R.; Reller, L.B. Comparative evaluation of Etest and sensititre yeastone panels against the Clinical and Laboratory Standards Institute M27-A2 reference broth microdilution method for testing Candida susceptibility to seven antifungal agents. J. Clin. Microbiol. 2007, 45, 698–706. [Google Scholar] [CrossRef]
- Chryssanthou, E. Trends in antifungal susceptibility among Swedish Candida species bloodstream isolates from 1994 to 1998: Comparison of the E-test and the Sensititre YeastOne Colorimetric Antifungal Panel with the NCCLS M27-A reference method. J. Clin. Microbiol. 2001, 39, 4181–4183. [Google Scholar] [CrossRef]
- Shin, J.H.; Kim, M.N.; Jang, S.J.; Ju, M.Y.; Kim, S.H.; Shin, M.G.; Suh, S.P.; Ryang, D.W. Detection of amphotericin B resistance in Candida haemulonii and closely related species by use of the Etest, Vitek-2 Yeast susceptibility system, and CLSI and EUCAST broth microdilution methods. J. Clin. Microbiol. 2012, 50, 1852–1855. [Google Scholar] [CrossRef]
- Maxwell, M.J.; Messer, S.A.; Hollis, R.J.; Diekema, D.J.; Pfaller, M.A. Evaluation of Etest method for determining voriconazole and amphotericin B MICs for 162 clinical isolates of Cryptococcus neoformans. J. Clin. Microbiol. 2003, 41, 97–99. [Google Scholar] [CrossRef]
- Metin, D.Y.; Hilmioglu-Polat, S.; Samlioglu, P.; Doganay-Oflazoglu, B.; Inci, R.; Tumbay, E. Evaluation of antifungal susceptibility testing with microdilution and Etest methods of Candida blood isolates. Mycopathologia 2011, 172, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Mahabeer, Y.; Chang, C.C.; Naidu, D.; Dorasamy, A.; Lewin, S.; Ndung'u, T.; Moosa, M.Y.; French, M.; Mlisana, K.; Coovadia, Y. Comparison of Etests and Vitek 2 (R) to broth microdilution for the susceptibility testing of Cryptococcus neoformans. Diagn. Microbiol. Infect. Dis. 2014, 80, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Espinel-Ingroff, A. Etest for antifungal susceptibility testing of yeasts. Diagn. Microbiol. Infect. Dis. 1994, 19, 217–220. [Google Scholar] [CrossRef]
- Sewell, D.L.; Pfaller, M.A.; Barry, A.L. Comparison of broth macrodilution, broth microdilution, and E test antifungal susceptibility tests for fluconazole. J. Clin. Microbiol. 1994, 32, 2099–2102. [Google Scholar] [PubMed]
- Pfaller, M.A.; Messer, S.A.; Karlsson, A.; Bolmstrom, A. Evaluation of the Etest method for determining fluconazole susceptibilities of 402 clinical yeast isolates by using three different agar media. J. Clin. Microbiol. 1998, 36, 2586–2589. [Google Scholar]
- Maxwell, M.J.; Messer, S.A.; Hollis, R.J.; Boyken, L.; Tendolkar, S.; Diekema, D.J.; Pfaller, M.A. Evaluation of Etest method for determining fluconazole and voriconazole MICs for 279 clinical isolates of Candida species infrequently isolated from blood. J. Clin. Microbiol. 2003, 41, 1087–1090. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A. Comparison of three commercial assays and a modified disk diffusion assay with two broth microdilution reference assays for testing zygomycetes, Aspergillus spp., Candida spp., and Cryptococcus neoformans with posaconazole and amphotericin B. J. Clin. Microbiol. 2006, 44, 3616–3622. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Messer, S.A.; Mills, K.; Bolmstrom, A.; Jones, R.N. Evaluation of Etest method for determining posaconazole MICs for 314 clinical isolates of Candida species. J. Clin. Microbiol. 2001, 39, 3952–3954. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Messer, S.A.; Houston, A.; Mills, K.; Bolmstrom, A.; Jones, R.N. Evaluation of the Etest method for determining voriconazole susceptibilities of 312 clinical isolates of Candida species by using three different agar media. J. Clin. Microbiol. 2000, 38, 3715–3717. [Google Scholar]
- Espinel-Ingroff, A.; Canton, E.; Pelaez, T.; Peman, J. Comparison of micafungin MICs as determined by the Clinical and Laboratory Standards Institute broth microdilution method (M27-A3 document) and Etest for Candida spp. isolates. Diagn. Microbiol. Infect. Dis. 2011, 70, 54–59. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A.; Canton, E.; Peman, J.; Martin-Mazuelo, E. Comparison of anidulafungin MICs determined by the clinical and laboratory standards institute broth microdilution method (M27-A3 document) and Etest for Candida species isolates. Antimicrob. Agents Chemother. 2010, 54, 1347–1350. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Castanheira, M.; Diekema, D.J.; Messer, S.A.; Moet, G.J.; Jones, R.N. Comparison of European Committee on Antimicrobial Susceptibility Testing (EUCAST) and Etest methods with the CLSI broth microdilution method for echinocandin susceptibility testing of Candida species. J. Clin. Microbiol. 2010, 48, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Messer, S.A.; Mills, K.; Bolmstrom, A.; Jones, R.N. Evaluation of Etest method for determining caspofungin (MK-0991) susceptibilities of 726 clinical isolates of Candida species. J. Clin. Microbiol. 2001, 39, 4387–4389. [Google Scholar] [CrossRef]
- Bougnoux, M.E.; Dannaoui, E.; Accoceberry, I.; Angoulvant, A.; Bailly, E.; Botterel, F.; Chevrier, S.; Chouaki, T.; Cornet, M.; Dalle, F.; et al. Multicenter comparison of the Etest and EUCAST methods for antifungal susceptibility testing of Candida isolates to micafungin. Antimicrob. Agents Chemother. 2016, 60, 5088–5091. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Zambrano, L.J.; Escribano, P.; Rueda, C.; Zaragoza, O.; Bouza, E.; Guinea, J. Comparison between the EUCAST procedure and the Etest for determination of the susceptibility of Candida species isolates to micafungin. Antimicrob. Agents Chemother. 2013, 57, 5767–5770. [Google Scholar] [CrossRef] [PubMed]
- Fleck, R.; Dietz, A.; Hof, H. In Vitro susceptibility of Candida species to five antifungal agents in a German university hospital assessed by the reference broth microdilution method and Etest. J. Antimicrob. Chemother. 2007, 59, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Chryssanthou, E.; Cuenca-Estrella, M. Comparison of the Antifungal Susceptibility Testing Subcommittee of the European Committee on Antibiotic Susceptibility Testing proposed standard and the E-test with the NCCLS broth microdilution method for voriconazole and caspofungin susceptibility testing of yeast species. J. Clin. Microbiol. 2002, 40, 3841–3844. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vandenbossche, I.; Vaneechoutte, M.; Vandevenne, M.; De Baere, T.; Verschraegen, G. Susceptibility testing of fluconazole by the NCCLS broth macrodilution method, E-test, and disk diffusion for application in the routine laboratory. J. Clin. Microbiol. 2002, 40, 918–921. [Google Scholar] [CrossRef]
- Araujo, R.; Espinel-Ingroff, A. Comparison of assessment of oxygen consumption, Etest, and CLSI M38-A2 broth microdilution methods for evaluation of the susceptibility of Aspergillus fumigatus to posaconazole. Antimicrob. Agents Chemother. 2009, 53, 4921–4923. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Verweij, P.; Nielsen, H.V. Evaluation of MIC strip isavuconazole test for susceptibility testing of wild-type and non-wild-type Aspergillus fumigatus isolates. Antimicrob. Agents Chemother. 2017, 61, e01659-01616. [Google Scholar] [CrossRef]
- Arikan, S.; Sancak, B.; Alp, S.; Hascelik, G.; McNicholas, P. Comparative in vitro activities of posaconazole, voriconazole, itraconazole, and amphotericin B against Aspergillus and Rhizopus, and synergy testing for Rhizopus. Med. Mycol. 2008, 46, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Escribano, P.; Pelaez, T.; Recio, S.; Bouza, E.; Guinea, J. Characterization of clinical strains of Aspergillus terreus complex: Molecular identification and antifungal susceptibility to azoles and amphotericin B. Clin. Microbiol. Infect. 2012, 18, E24–E26. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A. Comparison of the E-test with the NCCLS M38-P method for antifungal susceptibility testing of common and emerging pathogenic filamentous fungi. J. Clin. Microbiol. 2001, 39, 1360–1367. [Google Scholar] [PubMed]
- Espinel-Ingroff, A.; Rezusta, A. E-Test method for testing susceptibilities of Aspergillus spp. to the new triazoles voriconazole and posaconazole and to established antifungal agents: Comparison with NCCLS broth microdilution method. J. Clin. Microbiol. 2002, 40, 2101–2107. [Google Scholar] [PubMed]
- Fuller, J.; Schofield, A.; Jiwa, S.; Sand, C.; Jansen, B.; Rennie, R. Caspofungin Etest endpoint for Aspergillus isolates shows poor agreement with the reference minimum effective concentration. J. Clin. Microbiol. 2010, 48, 479–482. [Google Scholar] [PubMed]
- Guinea, J.; Pelaez, T.; Recio, S.; Torres-Narbona, M.; Bouza, E. In Vitro antifungal activities of isavuconazole (BAL4815), voriconazole, and fluconazole against 1007 isolates of zygomycete, Candida, Aspergillus, Fusarium, and Scedosporium species. Antimicrob. Agents Chemother. 2008, 52, 1396–1400. [Google Scholar] [CrossRef]
- Howard, S.J.; Harrison, E.; Bowyer, P.; Varga, J.; Denning, D.W. Cryptic species and azole resistance in the Aspergillus niger complex. Antimicrob. Agents Chemother. 2011, 55, 4802–4809. [Google Scholar] [CrossRef]
- Kondori, N.; Svensson, E.; Mattsby-Baltzer, I. In Vitro susceptibility of filamentous fungi to itraconazole, voriconazole and posaconazole by Clinical and Laboratory Standards Institute reference method and E-test. Mycoses 2011, 54, e318–e322. [Google Scholar] [CrossRef]
- Lamoth, F.; Alexander, B.D. Comparing Etest and broth microdilution for antifungal susceptibility testing of the most-relevant pathogenic molds. J. Clin. Microbiol. 2015, 53, 3176–3181. [Google Scholar] [CrossRef]
- Martin-Mazuelos, E.; Peman, J.; Valverde, A.; Chaves, M.; Serrano, M.C.; Canton, E. Comparison of the Sensititre YeastOne colorimetric antifungal panel and Etest with the NCCLS M38-A method to determine the activity of amphotericin B and itraconazole against clinical isolates of Aspergillus spp. J. Antimicrob. Chemother. 2003, 52, 365–370. [Google Scholar] [CrossRef]
- Martos, A.I.; Romero, A.; Gonzalez, M.T.; Gonzalez, A.; Serrano, C.; Castro, C.; Peman, J.; Canton, E.; Martin-Mazuelos, E. Evaluation of the Etest method for susceptibility testing of Aspergillus spp. and Fusarium spp. to three echinocandins. Med. Mycol. 2010, 48, 858–861. [Google Scholar] [CrossRef] [PubMed]
- Meletiadis, J.; Mouton, J.W.; Meis, J.F.; Bouman, B.A.; Verweij, P.E. Comparison of the Etest and the sensititre colorimetric methods with the NCCLS proposed standard for antifungal susceptibility testing of Aspergillus species. J. Clin. Microbiol. 2002, 40, 2876–2885. [Google Scholar] [CrossRef] [PubMed]
- Messer, S.A.; Diekema, D.J.; Hollis, R.J.; Boyken, L.B.; Tendolkar, S.; Kroeger, J.; Pfaller, M.A. Evaluation of disk diffusion and Etest compared to broth microdilution for antifungal susceptibility testing of posaconazole against clinical isolates of filamentous fungi. J. Clin. Microbiol. 2007, 45, 1322–1324. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ozkutuk, A.; Ergon, C.; Metin, D.Y.; Yucesoy, M.; Polat, S.H. Comparison of disk diffusion, E-test and broth microdilution test in determination of susceptibility of Aspergillus species to amphotericin B, itraconazole and voriconazole. J. Chemother. 2008, 20, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Messer, S.A.; Boyken, L.; Hollis, R.J.; Diekema, D.J. In Vitro susceptibility testing of filamentous fungi: Comparison of Etest and reference M38-A microdilution methods for determining posaconazole MICs. Diagn. Microbiol. Infect. Dis. 2003, 45, 241–244. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Messer, S.A.; Mills, K.; Bolmstrom, A. In Vitro susceptibility testing of filamentous fungi: Comparison of Etest and reference microdilution methods for determining itraconazole MICs. J. Clin. Microbiol. 2000, 38, 3359–3361. [Google Scholar] [CrossRef]
- Pinto, E.; Lago, M.; Branco, L.; Vale-Silva, L.A.; Pinheiro, M.D. Evaluation of Etest performed in Mueller-Hinton agar supplemented with glucose for antifungal susceptibility testing of clinical isolates of filamentous fungi. Mycopathologia 2014, 177, 157–166. [Google Scholar] [CrossRef]
- Serrano, M.C.; Morilla, D.; Valverde, A.; Chavez, M.; Espinel-Ingroff, A.; Claro, R.; Ramirez, M.; Mazuelos, E.M. Comparison of Etest with modified broth microdilution method for testing susceptibility of Aspergillus spp. to voriconazole. J. Clin. Microbiol. 2003, 41, 5270–5272. [Google Scholar] [CrossRef]
- Szekely, A.; Johnson, E.M.; Warnock, D.W. Comparison of E-test and broth microdilution methods for antifungal drug susceptibility testing of molds. J. Clin. Microbiol. 1999, 37, 1480–1483. [Google Scholar]
- Verweij, P.E.; Te Dorsthorst, D.T.; Rijs, A.J.; De Vries-Hospers, H.G.; Meis, J.F. Nationwide survey of in vitro activities of itraconazole and voriconazole against clinical Aspergillus fumigatus isolates cultured between 1945 and 1998. J. Clin. Microbiol. 2002, 40, 2648–2650. [Google Scholar] [CrossRef]
- Imbert, S.; Normand, A.C.; Ranque, S.; Costa, J.M.; Guitard, J.; Accoceberry, I.; Bonnal, C.; Fekkar, A.; Bourgeois, N.; Houze, S.; et al. Species identification and in vitro antifungal susceptibility of Aspergillus terreus species complex clinical isolates from a french multicenter study. Antimicrob. Agents Chemother. 2018, 62, e02315-17. [Google Scholar] [CrossRef] [PubMed]
- Al-Hatmi, A.M.; Normand, A.C.; Ranque, S.; Piarroux, R.; de Hoog, G.S.; Meletiadis, J.; Meis, J.F. Comparative evaluation of Etest, EUCAST, and CLSI methods for amphotericin B, voriconazole, and posaconazole against clinically relevant Fusarium species. Antimicrob. Agents Chemother. 2017, 61, e01671-16. [Google Scholar] [CrossRef] [PubMed]
- Debourgogne, A.; de Hoog, S.; Lozniewski, A.; Machouart, M. Amphotericin B and voriconazole susceptibility profiles for the Fusarium solani species complex: Comparison between the E-test and CLSI M38-A2 microdilution methodology. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 615–618. [Google Scholar] [CrossRef]
- Drogari-Apiranthitou, M.; Mantopoulou, F.D.; Skiada, A.; Kanioura, L.; Grammatikou, M.; Vrioni, G.; Mitroussia-Ziouva, A.; Tsakris, A.; Petrikkos, G. In Vitro antifungal susceptibility of filamentous fungi causing rare infections: Synergy testing of amphotericin B, posaconazole and anidulafungin in pairs. J. Antimicrob. Chemother. 2012, 67, 1937–1940. [Google Scholar] [CrossRef]
- Tortorano, A.M.; Prigitano, A.; Esposto, M.C.; Arsic Arsenijevic, V.; Kolarovic, J.; Ivanovic, D.; Paripovic, L.; Klingspor, L.; Nordoy, I.; Hamal, P.; et al. European Confederation of Medical Mycology (ECMM) epidemiological survey on invasive infections due to Fusarium species in Europe. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1623–1630. [Google Scholar] [CrossRef] [PubMed]
- Martin-Vicente, A.; Guarro, J.; Gonzalez, G.M.; Lass-Florl, C.; Lackner, M.; Capilla, J. Voriconazole MICs are predictive for the outcome of experimental disseminated scedosporiosis. J. Antimicrob. Chemother. 2017, 72, 1118–1122. [Google Scholar] [CrossRef] [PubMed]
- Caramalho, R.; Maurer, E.; Binder, U.; Araujo, R.; Dolatabadi, S.; Lass-Florl, C.; Lackner, M. Etest cannot be recommended for in vitro susceptibility testing of mucorales. Antimicrob. Agents Chemother. 2015, 59, 3663–3665. [Google Scholar] [CrossRef]
- Chowdhary, A.; Kathuria, S.; Singh, P.K.; Sharma, B.; Dolatabadi, S.; Hagen, F.; Meis, J.F. Molecular characterization and in vitro antifungal susceptibility of 80 clinical isolates of mucormycetes in Delhi, India. Mycoses 2014, 57 (Suppl. 3), 97–107. [Google Scholar] [CrossRef]
- Torres-Narbona, M.; Guinea, J.; Martinez-Alarcon, J.; Pelaez, T.; Bouza, E. In Vitro activities of amphotericin B, caspofungin, itraconazole, posaconazole, and voriconazole against 45 clinical isolates of zygomycetes: Comparison of CLSI M38-A, Sensititre YeastOne, and the Etest. Antimicrob. Agents Chemother. 2007, 51, 1126–1129. [Google Scholar] [CrossRef][Green Version]
- Pfaller, J.B.; Messer, S.A.; Hollis, R.J.; Diekema, D.J.; Pfaller, M.A. In Vitro susceptibility testing of Aspergillus spp.: Comparison of Etest and reference microdilution methods for determining voriconazole and itraconazole MICs. J. Clin. Microbiol. 2003, 41, 1126–1129. [Google Scholar] [CrossRef]
- Al-Hatmi, A.M.S.; Curfs-Breuker, I.; de Hoog, G.S.; Meis, J.F.; Verweij, P.E. Antifungal Susceptibility Testing of Fusarium: A Practical Approach. J. Fungi 2017, 3, 19. [Google Scholar] [CrossRef] [PubMed]
- Espinel-Ingroff, A.; Arendrup, M.; Canton, E.; Cordoba, S.; Dannaoui, E.; Garcia-Rodriguez, J.; Gonzalez, G.M.; Govender, N.P.; Martin-Mazuelos, E.; Lackner, M.; et al. Multicenter study of method-dependent epidemiological cutoff values for detection of resistance in Candida spp. and Aspergillus spp. to amphotericin B and echinocandins for the Etest agar diffusion method. Antimicrob. Agents Chemother. 2017, 61, e01792-16. [Google Scholar] [CrossRef] [PubMed]
- Favel, A.; Peyron, F.; De Meo, M.; Michel-Nguyen, A.; Carriere, J.; Chastin, C.; Regli, P. Amphotericin B susceptibility testing of Candida lusitaniae isolates by flow cytofluorometry: Comparison with the Etest and the NCCLS broth macrodilution method. J. Antimicrob. Chemother. 1999, 43, 227–232. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Law, D.; Moore, C.B.; Denning, D.W. Amphotericin B resistance testing of Candida spp.: A comparison of methods. J. Antimicrob. Chemother. 1997, 40, 109–112. [Google Scholar] [CrossRef]
- Lozano-Chiu, M.; Paetznick, V.L.; Ghannoum, M.A.; Rex, J.H. Detection of resistance to amphotericin B among Cryptococcus neoformans clinical isolates: Performances of three different media assessed by using E-test and National Committee for Clinical Laboratory Standards M27-A methodologies. J. Clin. Microbiol. 1998, 36, 2817–2822. [Google Scholar]
- Peyron, F.; Favel, A.; Michel-Nguyen, A.; Gilly, M.; Regli, P.; Bolmstrom, A. Improved detection of amphotericin B-resistant isolates of Candida lusitaniae by Etest. J. Clin. Microbiol. 2001, 39, 339–342. [Google Scholar] [CrossRef]
- Barchiesi, F.; Spreghini, E.; Sanguinetti, M.; Giannini, D.; Manso, E.; Castelli, P.; Girmenia, C. Effects of amphotericin B on Aspergillus flavus clinical isolates with variable susceptibilities to the polyene in an experimental model of systemic aspergillosis. J. Antimicrob. Chemother. 2013, 68, 2587–2591. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Garcia-Effron, G.; Buzina, W.; Mortensen, K.L.; Reiter, N.; Lundin, C.; Jensen, H.E.; Lass-Florl, C.; Perlin, D.S.; Bruun, B. Breakthrough Aspergillus fumigatus and Candida albicans double infection during caspofungin treatment: Laboratory characteristics and implication for susceptibility testing. Antimicrob. Agents Chemother. 2009, 53, 1185–1193. [Google Scholar] [CrossRef]
- Baixench, M.T.; Aoun, N.; Desnos-Ollivier, M.; Garcia-Hermoso, D.; Bretagne, S.; Ramires, S.; Piketty, C.; Dannaoui, E. Acquired resistance to echinocandins in Candida albicans: Case report and review. J. Antimicrob. Chemother. 2007, 59, 1076–1083. [Google Scholar] [CrossRef]
- Bourgeois, N.; Laurens, C.; Bertout, S.; Balard, Y.; Krasteva, D.; Rispail, P.; Lachaud, L. Assessment of caspofungin susceptibility of Candida glabrata by the Etest(R), CLSI, and EUCAST methods, and detection of FKS1 and FKS2 mutations. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1247–1252. [Google Scholar] [CrossRef]
- Desnos-Ollivier, M.; Dromer, F.; Dannaoui, E. Detection of caspofungin resistance in Candida spp. by Etest. J. Clin. Microbiol. 2008, 46, 2389–2392. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Prigent, G.; Ait-Ammar, N.; Levesque, E.; Fekkar, A.; Costa, J.M.; El Anbassi, S.; Foulet, F.; Duvoux, C.; Merle, J.C.; Dannaoui, E.; et al. Echinocandin resistance in Candida species isolates from liver transplant recipients. Antimicrob. Agents Chemother. 2017, 61, e01229-16. [Google Scholar] [CrossRef] [PubMed]
- Burgel, P.R.; Baixench, M.T.; Amsellem, M.; Audureau, E.; Chapron, J.; Kanaan, R.; Honore, I.; Dupouy-Camet, J.; Dusser, D.; Klaassen, C.H.; et al. High prevalence of azole-resistant Aspergillus fumigatus in adults with cystic fibrosis exposed to itraconazole. Antimicrob. Agents Chemother. 2012, 56, 869–874. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A.; Turnidge, J.; Alastruey-Izquierdo, A.; Botterel, F.; Canton, E.; Castro, C.; Chen, Y.C.; Chen, Y.; Chryssanthou, E.; Dannaoui, E.; et al. Method-dependent epidemiological cutoff values for detection of triazole resistance in Candida and Aspergillus species for the sensititre YeastOne colorimetric broth and Etest agar diffusion methods. Antimicrob. Agents Chemother. 2019, 63, e01651-18. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A.; Turnidge, J.; Alastruey-Izquierdo, A.; Dannaoui, E.; Garcia-Effron, G.; Guinea, J.; Kidd, S.; Pelaez, T.; Sanguinetti, M.; Meletiadis, J.; et al. Posaconazole MIC distributions for Aspergillus fumigatus species complex by four methods: Impact of cyp51A mutations on estimation of epidemiological cutoff values. Antimicrob. Agents Chemother. 2018, 62, e01916-17. [Google Scholar] [CrossRef]
- Idelevich, E.A.; Gross, U.; Becker, K.; Bader, O. Comparative evaluation of different gradient diffusion tests for detection of azole resistance in Aspergillus fumigatus. Diagn. Microbiol. Infect. Dis. 2018, 91, 52–54. [Google Scholar] [CrossRef]
- Bordallo-Cardona, M.A.; Marcos-Zambrano, L.J.; Sanchez-Carrillo, C.; Bouza, E.; Munoz, P.; Escribano, P.; Guinea, J. Resistance to echinocandins in Candida can be detected by performing the Etest directly on blood culture samples. Antimicrob. Agents Chemother. 2018, 62, e00162-18. [Google Scholar] [CrossRef]
- Chang, H.C.; Chang, J.J.; Chan, S.H.; Huang, A.H.; Wu, T.L.; Lin, M.C.; Chang, T.C. Evaluation of Etest for direct antifungal susceptibility testing of yeasts in positive blood cultures. J. Clin. Microbiol. 2001, 39, 1328–1333. [Google Scholar] [CrossRef]
- Escribano, P.; Marcos-Zambrano, L.J.; Gomez, A.; Sanchez, C.; Martinez-Jimenez, M.C.; Bouza, E.; Guinea, J. The Etest performed directly on blood culture bottles is a reliable tool for detection of fluconazole-resistant Candida albicans isolates. Antimicrob. Agents Chemother. 2017, 61, e00400-17. [Google Scholar] [CrossRef]
- Guinea, J.; Recio, S.; Escribano, P.; Torres-Narbona, M.; Pelaez, T.; Sanchez-Carrillo, C.; Rodriguez-Creixems, M.; Bouza, E. Rapid antifungal susceptibility determination for yeast isolates by use of Etest performed directly on blood samples from patients with fungemia. J. Clin. Microbiol. 2010, 48, 2205–2212. [Google Scholar] [CrossRef]
- Jabeen, K.; Kumar, H.; Farooqi, J.; Mehboob, R.; Brandt, M.E.; Zafar, A. Agreement of direct antifungal susceptibility testing from positive blood culture bottles with the conventional method for Candida species. J. Clin. Microbiol. 2016, 54, 343–348. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Salse, M.; Gangneux, J.P.; Cassaing, S.; Delhaes, L.; Fekkar, A.; Dupont, D.; Botterel, F.; Costa, D.; Bourgeois, N.; Bouteille, B.; et al. Multicentre study to determine the Etest epidemiological cut-off values of antifungal drugs in Candida spp. and Aspergillus fumigatus species complex. Clin. Microbiol. Infect. 2019. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.N.; Lo, H.J.; Wu, C.C.; Ko, H.C.; Chang, T.P.; Yang, Y.L. Loss of heterozygosity of FCY2 leading to the development of flucytosine resistance in Candida tropicalis. Antimicrob. Agents Chemother. 2011, 55, 2506–2514. [Google Scholar] [CrossRef] [PubMed]
- Vasicek, E.M.; Berkow, E.L.; Bruno, V.M.; Mitchell, A.P.; Wiederhold, N.P.; Barker, K.S.; Rogers, P.D. Disruption of the transcriptional regulator Cas5 results in enhanced killing of Candida albicans by Fluconazole. Antimicrob. Agents Chemother. 2014, 58, 6807–6818. [Google Scholar] [CrossRef]
- Vasicek, E.M.; Berkow, E.L.; Flowers, S.A.; Barker, K.S.; Rogers, P.D. UPC2 is universally essential for azole antifungal resistance in Candida albicans. Eukaryot. Cell 2014, 13, 933–946. [Google Scholar] [CrossRef]
- Lewis, R.E.; Diekema, D.J.; Messer, S.A.; Pfaller, M.A.; Klepser, M.E. Comparison of Etest, chequerboard dilution and time-kill studies for the detection of synergy or antagonism between antifungal agents tested against Candida species. J. Antimicrob. Chemother. 2002, 49, 345–351. [Google Scholar] [CrossRef]
- Canton, E.; Peman, J.; Gobernado, M.; Viudes, A.; Espinel-Ingroff, A. Synergistic activities of fluconazole and voriconazole with terbinafine against four Candida species determined by checkerboard, time-kill, and Etest methods. Antimicrob. Agents Chemother. 2005, 49, 1593–1596. [Google Scholar] [CrossRef]
- Dannaoui, E.; Schwarz, P.; Lortholary, O. In Vitro interactions between antifungals and immunosuppressive drugs against zygomycetes. Antimicrob. Agents Chemother. 2009, 53, 3549–3551. [Google Scholar] [CrossRef]
- Kiraz, N.; Dag, I.; Yamac, M.; Kiremitci, A.; Kasifoglu, N.; Akgun, Y. Antifungal activity of caspofungin in combination with amphotericin B against Candida glabrata: Comparison of disk diffusion, Etest, and time-kill methods. Antimicrob. Agents Chemother. 2009, 53, 788–790. [Google Scholar] [CrossRef]
- Kiraz, N.; Dag, I.; Yamac, M.; Kiremitci, A.; Kasifoglu, N.; Oz, Y. Synergistic activities of three triazoles with caspofungin against Candida glabrata isolates determined by time-kill, Etest, and disk diffusion methods. Antimicrob. Agents Chemother. 2010, 54, 2244–2247. [Google Scholar] [CrossRef]
- Li, Y.; Wan, Z.; Liu, W.; Li, R. Synergistic activity of chloroquine with fluconazole against fluconazole-resistant isolates of Candida species. Antimicrob. Agents Chemother. 2015, 59, 1365–1369. [Google Scholar] [CrossRef] [PubMed]
- Pankey, G.; Ashcraft, D.; Kahn, H.; Ismail, A. Time-kill assay and Etest evaluation for synergy with polymyxin B and fluconazole against Candida glabrata. Antimicrob. Agents Chemother. 2014, 58, 5795–5800. [Google Scholar] [CrossRef] [PubMed]
- Planche, V.; Ducroz, S.; Alanio, A.; Bougnoux, M.E.; Lortholary, O.; Dannaoui, E. In Vitro combination of anidulafungin and voriconazole against intrinsically azole-susceptible and -resistant Aspergillus spp. Antimicrob. Agents Chemother. 2012, 56, 4500–4503. [Google Scholar] [CrossRef] [PubMed]
- Raffetin, A.; Courbin, V.; Jullien, V.; Dannaoui, E. In Vitro combination of isavuconazole with echinocandins against azole-susceptible and -resistant Aspergillus spp. Antimicrob. Agents Chemother. 2018, 62, e01382-17. [Google Scholar] [CrossRef]
- Ben-Ami, R.; Lewis, R.E.; Kontoyiannis, D.P. In Vitro interactions among echinocandins against Aspergillus fumigatus: Lack of concordance among methods. Med. Mycol. 2011, 49, 285–288. [Google Scholar] [CrossRef][Green Version]
- Cowen, L.E.; Lindquist, S. Hsp90 potentiates the rapid evolution of new traits: Drug resistance in diverse fungi. Science 2005, 309, 2185–2189. [Google Scholar] [CrossRef]
- Cowen, L.E.; Singh, S.D.; Kohler, J.R.; Collins, C.; Zaas, A.K.; Schell, W.A.; Aziz, H.; Mylonakis, E.; Perfect, J.R.; Whitesell, L.; et al. Harnessing Hsp90 function as a powerful, broadly effective therapeutic strategy for fungal infectious disease. Proc. Natl. Acad. Sci. USA 2009, 106, 2818–2823. [Google Scholar] [CrossRef]
- Dannaoui, E.; Lortholary, O.; Dromer, F. In Vitro evaluation of double and triple combinations of antifungal drugs against Aspergillus fumigatus and Aspergillus terreus. Antimicrob. Agents Chemother. 2004, 48, 970–978. [Google Scholar] [CrossRef]
- Kontoyiannis, D.P.; Lewis, R.E.; Sagar, N.; May, G.; Prince, R.A.; Rolston, K.V. Itraconazole-amphotericin B antagonism in Aspergillus fumigatus: An E- test-based strategy. Antimicrob. Agents Chemother. 2000, 44, 2915–2918. [Google Scholar] [CrossRef]
- Lafleur, M.D.; Sun, L.; Lister, I.; Keating, J.; Nantel, A.; Long, L.; Ghannoum, M.; North, J.; Lee, R.E.; Coleman, K.; et al. Potentiation of azole antifungals by 2-adamantanamine. Antimicrob. Agents Chemother. 2013, 57, 3585–3592. [Google Scholar] [CrossRef]
- Vitale, R.G.; Afeltra, J.; Dannaoui, E. Antifungal combinations. Methods Mol. Med. 2005, 118, 143–152. [Google Scholar] [PubMed]
- White, R.L.; Burgess, D.S.; Manduru, M.; Bosso, J.A. Comparison of three different in vitro methods of detecting synergy: Time-kill, checkerboard, and E test. Antimicrob. Agents Chemother. 1996, 40, 1914–1918. [Google Scholar] [CrossRef] [PubMed]
- Adams, E.K.; Ashcraft, D.S.; Pankey, G.A. In Vitro synergistic activity of caspofungin plus polymyxin B against fluconazole-resistant Candida glabrata. Am. J. Med. Sci. 2016, 351, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Denardi, L.B.; Keller, J.T.; de Azevedo, M.I.; Oliveira, V.; Piasentin, F.B.; Severo, C.B.; Santurio, J.M.; Alves, S.H. Comparison between Etest and broth microdilution methods for testing itraconazole-resistant Aspergillus fumigatus susceptibility to antifungal combinations. Mycopathologia 2018, 183, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, P.; Janbon, G.; Dromer, F.; Lortholary, O.; Dannaoui, E. Combination of amphotericin B with flucytosine is active in vitro against flucytosine-resistant isolates of Cryptococcus neoformans. Antimicrob. Agents Chemother. 2007, 51, 383–385. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Species | CLSI and Etest | EUCAST and Etest | ||||||
|---|---|---|---|---|---|---|---|---|
| No. Isol | EA% | Comments | EA % AM3 | Ref | No. Isol | EA% | Ref | |
| C. albicans | 53 | 96 | 48 h macro Etest | 98 | [31] | 345 d | 81 | [25] |
| 266 | 98 | 48 h micro Etest | [30] | 54 | 15 | [32] | ||
| 94 | 99 | 48 h micro | [34] | |||||
| 123 | 97 | 48 h macro Etest | [35] | |||||
| 181 | 84/88 | micro Etest 24/48 h | [38] | |||||
| C. glabrata | 9 | 100 | 48 h macro Etest | 100 | [31] | 104 d | 69 | [25] |
| 102 | 100 | 48 h micro Etest | [30] | 11 | 44 | [32] | ||
| 38 | 100 | 48 h micro | [34] | |||||
| 38 | 77/86 | micro Etest 24/48 h | [38] | |||||
| C. krusei | 28 | 96 | 48 h micro Etest | [30] | ||||
| 5 | 100 | 48 h micro | [34] | |||||
| C. parapsilosis | 10 | 100 | 48 h Macro/Etest | 90 | [31] | 68 d | 65 | [25] |
| 142 | 100 | 48 h micro Etest | [30] | 38 | 2,7 | [32] | ||
| 31 | 100 | 48 h Micro | [34] | |||||
| 47 | 85/85 | micro Etest 24/48 h | [38] | |||||
| C. tropicalis | 79 | 99 | 48 h micro Etest | [30] | 54 d | 61 | [25] | |
| 34 | 100 | 48 h micro | [34] | 33 | 22 | [32] | ||
| 13 | 92 | 48 h macro Etest | 85 | [31] | ||||
| 48 | 80/89 | micro Etest 24/48 h | [38] | |||||
| C. lusitaniae | 19 a | 89 | 48 h micro Etest | [30] | ||||
| 8 | 100 | 48 h micro | [34] | |||||
| C. auris | 20 | 100 | 24 h micro Etest b | [36] | 20 | 100 | [36] | |
| C. neoformans | 162 | 99 | micro Etest 72 h | [37] | 26 d | 73 | [25] | |
| 85 | 83 | micro Etest 48–72 h | [39] | |||||
| Species | CLSI and Etest | EUCAST and Etest | |||||
|---|---|---|---|---|---|---|---|
| No. Isol | EA% | Comments | Ref. | No. Isol | EA% | Ref | |
| C. albicans | 28 | 93/100 a | macro 24/48 h Etest | [40] | 166 | 96 | [25] |
| 94 | 93 | 48 h micro | [34] | 54 | 72 | [32] | |
| 123 | 89 b | 48 h macro Etest | [35] | ||||
| C. glabrata | 6 | 100/83 | macro 24/48 h Etest | [40] | 46 | 100 | [25] |
| 38 | 100 | 48 h micro | [34] | 11 | 78 | [32] | |
| C. krusei | 7 | 86/100 | macro 24/48 h Etest | [40] | |||
| 5 | 100 | 48 h micro | [34] | ||||
| C. parapsilosis | 7 | 86/100 | macro 24/48 h Etest | [40] | 26 | 92 | [25] |
| 31 | 100 | 48 h micro | [34] | 38 | 82 | [32] | |
| C. tropicalis | 14 | 93/100 | macro 24/48 h Etest | [40] | 25 | 100 | [25] |
| 34 | 94 | 48 h micro | [34] | 33 | 62 | [32] | |
| C. lusitaniae | 6 | 83/100 | macro 24/48 h Etest | [40] | |||
| 8 | 100 | 48 h micro | [34] | ||||
| C. neoformans | 10 | 70/60 | macro 24/48 h Etest | [40] | 20 | 35 | [25] |
| Species/Agent | CLSI and Etest | EUCAST and Etest | |||||||
|---|---|---|---|---|---|---|---|---|---|
| No. Isol | EA% | Comments | EA % M-H Agar | EA % Casitone | Ref | No. Isol | EA % | Ref | |
| Fluconazole | |||||||||
| C. albicans | 28 | 82/75 a | macro Etest 24/48 h | [40] | 354 | 67 | [25] | ||
| 122 | 93/79 | macro Etest 24/48 h | [41] | 54 | 91 | [32] | |||
| 208 | 97/96 | micro Etest 24/48 h | [38] | ||||||
| 23 | 96 | macro Etest 48 h | [31] | ||||||
| 161 | 90 | micro Etest 48 h | 50 | 95 | [42] | ||||
| 123 | 85 | 48 h macro Etest | [35] | ||||||
| 94 | 98 | 48 h micro | [34] | ||||||
| C. glabrata | 12 | 92 | macro Etest 48 h | [31] | 110 | 73 | [25] | ||
| 41 | 100 | micro Etest 48 h | 28 | 95 | [42] | 11 | 82 | [32] | |
| 6 | 100/83 a | macro Etest 24/48 h | [40] | ||||||
| 34 | 77/75 | micro Etest 24/48 h | [38] | ||||||
| 41 | 37/34 | macro Etest 24/48 h | [41] | ||||||
| 38 | 82 | 48 h micro | [34] | ||||||
| C. guilliermondii | 53 b | 91 | micro Etest 48 h | [43] | |||||
| 7 | 100/100 a | macro Etest 24/48 h | [40] | ||||||
| C. krusei | 32 | 100 | micro Etest 48 h | 90 | 97 | [42] | |||
| 118 | 97 | micro Etest 48 h | [43] | ||||||
| 5 | 40 | 48 h micro | [34] | ||||||
| C. parapsilosis | 7 | 100/100 a | macro Etest 24/48 h | [40] | 69 | 78 | [25] | ||
| 12 | 100 | macro Etest 48 h | [31] | 38 | 82 | [32] | |||
| 29 | 100 | micro Etest 48 h | 17 | 100 | [42] | ||||
| 54 | 89/98 | micro Etest 24/48 h | [38] | ||||||
| 31 | 87 | 48 h micro | [34] | ||||||
| C. tropicalis | 14 | 100/93 a | macro Etest 24/48 h | [40] | 54 | 85 | [25] | ||
| 13 | 93 | macro Etest 48 h | [31] | 33 | 58 | [32] | |||
| 35 | 91 | micro Etest 48 h | 91 | 100 | [42] | ||||
| 34 | 100 | 48 h micro | [34] | ||||||
| 52 | 96/85 | micro Etest 24/48 h | [38] | ||||||
| 45 | 56/67 | macro; 24/48 h Etest | [41] | ||||||
| C. lusitaniae | 31 | 97 | micro Etest 48 h | 45 | 100 | [42] | |||
| 8 | 100 | 48 h micro | [34] | ||||||
| 56 | 100 | micro Etest 48 h | [43] | ||||||
| 6 | 83/83 a | macro Etest 24/48 h | [40] | ||||||
| C. neoformans | 40 | 97 | micro Etest 48 h | 87 | 93 | [42] | 30 | 77 | [25] |
| 97 | 95 c | micro Etest 48–72 h | [39] | ||||||
| 10 | 90/83 a | macro Etest 48/72 h | [40] | ||||||
| Itraconazole | |||||||||
| C. albicans | 94 | 97 | 48 h micro | [34] | 109 | 73 | [25] | ||
| 123 | 72 | 48 h macro Etest | [39] | 54 | 72 | [32] | |||
| 205 | 96/95 | micro Etest 24/48 h | [38] | ||||||
| C. glabrata | 38 | 89 | 48 h micro | [34] | 31 | 68 | [25] | ||
| 34 | 75/77 | micro Etest 24/48 h | [38] | 11 | 55 | [32] | |||
| C. krusei | 5 | 80 | 48 h micro | [34] | |||||
| C. lusitaniae | 8 | 100 | 48 h micro | [34] | |||||
| C. parapsilosis | 31 | 100 | 48h micro | [34] | 13 | 92 | [25] | ||
| 52 | 95/95 | micro Etest 24/48 h | [38] | 38 | 95 | [32] | |||
| C. tropicalis | 34 | 94 | 48 h micro | [34] | 14 | 50 | [25] | ||
| 46 | 85/85 | micro Etest 24/48 h | [38] | 33 | 73 | [32] | |||
| C. neoformans | NA | NA | 11 | 72 | [25] | ||||
| Posaconazole | |||||||||
| C. albicans | 25 | 92/92 | micro Etest 24/48 h | [44] | |||||
| 174 | 98 | micro Etest at 48 h | [45] | ||||||
| 94 | 100 | 48 h micro | [34] | ||||||
| C. dubliniensis | 10 | 92/92 | micro Etest at 24/48 h | [44] | |||||
| C. glabrata | 57 | 93 | micro Etest at 48 h | [45] | |||||
| 10 | 100/90 | micro Etest at 24/48 h | [44] | ||||||
| 38 | 95 | 48 h micro | [34] | ||||||
| C. krusei | 5 | 100 | micro Etest at 48 h | [45] | |||||
| 10 | 100/100 | micro Etest at 24/48 h | [44] | ||||||
| 5 | 100 | 48 h micro | [34] | ||||||
| C. lusitaniae | 10 | 70/90 | micro Etest at 24/48 h | [44] | |||||
| 8 | 100 | ||||||||
| C. parapsilosis | 39 | 85 | micro Etest at 48 h | [45] | |||||
| 10 | 60/90 | microm Etest at 24/48 h | [44] | ||||||
| 31 | 100 | 48 h micro | [34] | ||||||
| C. tropicalis | 31 | 97 | micro Etest at 48 h | [45] | |||||
| 10 | 70/100 | micro Etest at 24/48 h | [44] | ||||||
| 34 | 100 | 48 h micro | [34] | ||||||
| C. guilliermondii | 6 | 88 | micro Etest at 48 h | [45] | |||||
| 10 | 80/100 | micro Etest at 24/48 h | [44] | ||||||
| C. neoformans | 15 | 93 | micro Etest at 72 h | [44] | |||||
| Voriconazole | |||||||||
| C. albicans | 174 | 99 d | micro Etest 48 h | [46] | 308 | 88 | [25] | ||
| 94 | 93 | 48 h micro | [34] | 54 | 87 | [32] | |||
| 212 | 99/96 | micro Etest 24/48 h | [38] | ||||||
| C. glabrata | 55 | 91 d | micro Etest 48 h | [46] | 98 | 82 | [25] | ||
| 38 | 89 | 48 h micro | [34] | 11 | 60 | [32] | |||
| 44 | 93/100 | micro Etest 24/48 h | [38] | ||||||
| C. krusei | 5 | 100 d | micro Etest 48 h | [46] | |||||
| 5 | 100 | 48 h micro | [34] | ||||||
| 118 | 99 | micro Etest 48 h | [43] | ||||||
| C. lusitaniae | 8 | 100 | 48 h micro | [34] | |||||
| 56 | 100 | micro Etest 48 h | [43] | ||||||
| C. parapsilosis | 39 | 100 d | micro Etest 48 h | [46] | 59 | 86 | [25] | ||
| 31 | 97 | 48 h micro | [34] | 38 | 95 | [32] | |||
| 55 | 96/100 | micro Etest 24/48 h | [38] | ||||||
| C. tropicalis | 31 | 100 d | micro Etest 48 h | [46] | 48 | 81 | [25] | ||
| 34 | 85 | 48 h micro | [34] | 33 | 73 | [32] | |||
| 54 | 100/91 | micro Etest 24/48 h | [38] | ||||||
| C. guilliermondii | 6 | 100 d | micro Etest 48 h | [46] | |||||
| 53 b | 79 | micro Etest 48 h | [43] | ||||||
| C. neoformans | 93 | 91 c | micro Etest 48–72 h | [39] | 22 | 86 | [25] | ||
| 162 | 94 | micro Etest 72 h | [37] | ||||||
| Species/Agent | CLSI and Etest | EUCAST and Etest | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. Isol | EA% | Comments | EA% AM3 | EA% Casitone | Ref CLSI | No. Isol | EA% | Comments | Ref | |
| Caspofungin | ||||||||||
| C. albicans | 486 | 95 | Micro/Etest 48h | 88 | 85 | [50] | 120 | 80 | [25] | |
| 94 | 89 | 48 h Micro | [34] | |||||||
| 32 | 94 | Micro/Etest 24h | [49] | |||||||
| C. glabrata | 96 | 99 | Micro/Etest 48h | 100 | 100 | [50] | 45 | 67 | [25] | |
| 38 | 90 | 48 h Micro | [34] | |||||||
| 34 | 94 | Micro/Etest 24h | [49] | |||||||
| C. krusei | 11 | 100 | Micro/Etest 48h | 100 | 80 | [50] | ||||
| 5 | 100 | 48 h Micro | [34] | |||||||
| 11 | 91 | Micro/Etest 24h | [49] | |||||||
| C. lusitaniae | 8 | 100 | 48 h Micro | [34] | ||||||
| C. parapsilosis | 47 | 79 | Micro/Etest 48h | 49 | 77 | [50] | 29 | 90 | [25] | |
| 31 | 100 | 48 h Micro | [34] | |||||||
| 25 | 100 | Micro/Etest 24h | [49] | |||||||
| C. tropicalis | 51 | 86 | Micro/Etest 48h | 23 | 40 | [50] | 20 | 60 | [25] | |
| 34 | 88 | 48 h Micro | [34] | |||||||
| 12 | 100 | Micro/Etest 24h | [49] | |||||||
| C. guilliermondii | 33 | 100 | Micro/Etest 48h | 100 | 83 | [50] | ||||
| 19 | 84 | Micro/Etest 24h | [49] | |||||||
| C. neoformans | 4 | 100 | [25] | |||||||
| Micafungin | ||||||||||
| C. albicans | 125 | 97 | Micro/Etest 24h | [47] | 31 | 93/90 | 24/48 h | [52] | ||
| 32 | 100 | Micro/Etest 24h | [49] | 159 | 100 | [51] | ||||
| C. glabrata | 52 | 100 | Micro/Etest 24h | [47] | 40 | 89/90 | 24/48 h | [52] | ||
| 34 | 94 | Micro/Etest 24h | [49] | 152 | 99 | [51] | ||||
| C. krusei | 39 | 95 | Micro/Etest 24h | [47] | 10 | 80/80 | 24/48 h | [52] | ||
| 11 | 100 | Micro/Etest 24h | [49] | 127 | 98 | [51] | ||||
| C. parapsilosis | 31 | 87 | Micro/Etest 24h | [47] | 27 | 75/93 | 24/48 h | [52] | ||
| 25 | 100 | Micro/Etest 24h | [49] | 152 | 97 | [51] | ||||
| C. tropicalis | 39 | 90 | Micro/Etest 24h | [47] | 28 | 93/89 | 24/48 h | [52] | ||
| 12 | 100 | Micro/Etest 24h | [49] | 152 | 99 | [51] | ||||
| C. guilliermondii | 11 | 91 | Micro/Etest 24h | [47] | ||||||
| 19 | 79 | Micro/Etest 24h | [49] | |||||||
| C. kefyr | 136 | 98 | [51] | |||||||
| Anidulafungin | ||||||||||
| C. albicans | 33 | 91 | Micro/Etest 24h | [48] | ||||||
| 32 | 78 | Micro/Etest 24h | [49] | |||||||
| C. glabrata | 13 | 69 | Micro/Etest 24h | [48] | ||||||
| 34 | 91 | Micro/Etest 24h | [49] | |||||||
| C. krusei | 12 | 75 | Micro/Etest 24h | [48] | ||||||
| 11 | 100 | Micro/Etest 24h | [49] | |||||||
| C. parapsilosis | 57 | 74 | Micro/Etest 24h | [48] | ||||||
| 25 | 100 | Micro/Etest 24h | [49] | |||||||
| C. tropicalis | 15 | 100 | Micro/Etest 24h | [48] | ||||||
| 12 | 100 | Micro/Etest 24h | [49] | |||||||
| C. guilliermondii | 9 | 78 | Micro/Etest 24h | [48] | ||||||
| 19 | 95 | Micro/Etest 24h | [49] | |||||||
| Organisms | Number of Isolates | ATF | Reference Technique | Endpoint Used for Comparison | Essential Agreement (EA) with Reference Technique a | Comments | Reference |
|---|---|---|---|---|---|---|---|
| Aspergillus | 123 | AMB | CLSI | +/−2 dil | 75%–100% | Lowest EA for A. flavus, A. fumigatus, and A. nidulans. Higher EA for Etest at 24h | [60] |
| Aspergillus | 126 | AMB | CLSI | +/−2 dil | 96% | Higher MICs for Etest | [44] |
| Aspergillus | 154 | AMB | CLSI | +/−2 dil | 16%–100% | 16% for A. terreus, 97-100% for other species | [66] |
| Aspergillus | 40 | AMB | CLSI | +/−2 dil | 60%–100% | 50-100% at +/− 1dil | [76] |
| Aspergillus | 63 | AMB | CLSI | +/−2 dil | 88.5% | Higher EA for Etest at 24h | [67] |
| Aspergillus | 25 | AMB | CLSI | +/−2 dil | 89.2% | Higher EA for Etest at 24h. higher MICs for Etest | [69] |
| Aspergillus | 107 | AMB | CLSI | +/−2 dil | 91.7% | Higher EA for Etest at 24h | [61] |
| Aspergillus | 32 | AMB | CLSI | +/−2 dil | 81% | Higher EA for Etest at 24h | [71] |
| Aspergillus | 48 | AMB | CLSI | +/−2 dil | 100% | EA at +/− 1 dil: 72% for A. fumigatus and 62% for A. niger -Etest in MHG | [74] |
| Aspergillus | 87 | AMB | CLSI | ND | ND | Only A. terreus. Lower MICs for Etest | [59] |
| Aspergillus | 79 | AMB | EUCAST | +/−2 dil | 79.7% | Only A. terreus, CA 88.7% | [78] |
| Aspergillus | 123 | ITZ | CLSI | +/−2 dil | 83.3%–100% | higher MICs by Etest. Lowest EA for A. nidulans | [60] |
| Aspergillus | 29 | ITZ | CLSI | +/−1 dil | 75.8% | Higher MIC by Etest | [65] |
| Aspergillus | 24 | ITZ | CLSI | +/−2 dil | 100% | / | [73] |
| Aspergillus | 40 | ITZ | CLSI | +/−2 dil | 90%–100% | 40-100% at +/− 1dil | [76] |
| Aspergillus | 63 | ITZ | CLSI | +/−2 dil | 67.2% | Higher EA for Etest at 24h. Higher MIC by Etest | [67] |
| Aspergillus | 25 | ITZ | CLSI | +/−2 dil | 72.5% | Higher EA for Etest at 24h. Higher MIC by Etest | [69] |
| Aspergillus | 376 | ITZ | CLSI | +/−2 dil | 95.8% | Higher MIC by Etest | [87] |
| Aspergillus | 107 | ITZ | CLSI | +/−2 dil | 91.8% | Higher EA for Etest at 24h | [61] |
| Aspergillus | 170 | ITZ | CLSI | +/−1 dil | 93.5% | / | [77] |
| Aspergillus | 32 | ITZ | CLSI | +/−2 dil | 75% | / | [71] |
| Aspergillus | 50 | ITZ | mEUCAST | ND | ND | Only A. niger. Lower MIC by Etest | [64] |
| Aspergillus | 79 | ITZ | EUCAST | +/−2 dil | 73.4% | Only A. terreus, higher MIC by Etest. CA 98.7% | [78] |
| Aspergillus | 29 | VRZ | CLSI | +/−1 dil | 100% | / | [65] |
| Aspergillus | 154 | VRZ | CLSI | +/−2 dil | 95%–100% | Lower MIC by Etest | [66] |
| Aspergillus | 376 | VRZ | CLSI | +/−2 dil | 97.6% | Lower MIC by Etest | [87] |
| Aspergillus | 77 | VRZ | mCLSI | +/−2 dil | 93.5% | Higher EA for Etest at 24 h. Higher MIC by Etest | [75] |
| Aspergillus | 107 | VRZ | CLSI | +/−2 dil | 96.3% | / | [61] |
| Aspergillus | 32 | VRZ | CLSI | +/−2 dil | 85% | / | [71] |
| Aspergillus | 48 | VRZ | CLSI | +/−2 dil | 92%–100% | at +/− 1 dil 36% for A. fumigatus and 8% for A. niger -Etest in MHG | [74] |
| Aspergillus | 79 | VRZ | EUCAST | +/−2 dil | 93.7% | Only A. terreus, CA 100% | [78] |
| Aspergillus | 126 | PSZ | CLSI | +/−2 dil | 97% | / | [44] |
| Aspergillus | 29 | PSZ | CLSI | +/−1 dil | 93% | / | [65] |
| Aspergillus | 154 | PSZ | CLSI | +/−2 dil | 64%–100% | / | [66] |
| Aspergillus | 55 | PSZ | CLSI | +/−2 dil | 82%–88% | 82% for A. fumigatus, 88% for other species. Lower MIC by Etest | [72] |
| Aspergillus | 50 | PSZ | CLSI | +/−2 dil | 90%–92% | CA 84–88% | [56] |
| Aspergillus | 107 | PSZ | CLSI | +/−2 dil | 95.3% | / | [61] |
| Aspergillus | 48 | PSZ | CLSI | +/−2 dil | 100% | at +/− 1 dil 72% for A. fumigatus and 85% for A. niger -Etest in MHG | [74] |
| Aspergillus | 82 | PSZ | CLSI | ND | ND | Lower MIC by Etest | [58] |
| Aspergillus | 140 | PSZ | CLSI | ND | ND | CA 99.3% | [70] |
| Aspergillus | 79 | PSZ | EUCAST | +/−2 dil | 96.2% | Only A. terreus, CA 77.2% | [78] |
| Aspergillus | 702 | ISA | CLSI | +/−2 dil | 96.7% | Lower MIC by Etest | [63] |
| Aspergillus | 79 | ISA | EUCAST | +/−2 dil | 89%–90% | Only A. fumigatus. Lower MIC by Etest | [57] |
| Aspergillus | 79 | ISA | EUCAST | +/−2 dil | 97.5% | Only A. terreus, CA 97.4% | [78] |
| Aspergillus | 154 | CAS | CLSI | +/−2 dil | 14%–100% | 14% for A. ustus, 80–100% for other species | [66] |
| Aspergillus | 67 | CAS | CLSI | +/−2 dil | 79%–83.5% | Higher EA for Etest at 24h | [68] |
| Aspergillus | 169 | CAS | CLSI | +/−2 dil | 38%–80% | / | [23] |
| Aspergillus | 272 | CAS | CLSI | +/−2 dil | 61% | 26% at +/− 1 dil | [62] |
| Aspergillus | 48 | CAS | CLSI | +/−2 dil | 100% | at +/− 1 dil 76% for A. fumigatus and 62% for A. niger -Etest in MHG | [74] |
| Aspergillus | 79 | CAS | EUCAST | +/−2 dil | 96.2% | Only A. terreus | [78] |
| Aspergillus | 154 | Mica | CLSI | +/−2 dil | 57%–100% | 57% for A. ustus, 100% for other species | [66] |
| Aspergillus | 67 | Mica | CLSI | +/−2 dil | 100% | / | [68] |
| Aspergillus | 79 | Mica | EUCAST | +/−2 dil | 100% | Only A. terreus | [78] |
| Aspergillus | 67 | ANI | CLSI | +/−2 dil | 100% | / | [68] |
| Aspergillus | 48 | ANI | CLSI | +/−2 dil | 100% | All MIC values < 0.03 µg/mL | [74] |
| Aspergillus | 79 | ANI | EUCAST | +/−2 dil | 100% | Only A. terreus | [78] |
| Organisms | Number of Isolates | ATF | Reference Technique | Endpoint Used for Comparison | Essential Agreement (EA) with Reference Technique | Comments | Reference |
|---|---|---|---|---|---|---|---|
| Mucorales | 131 | AMB | EUCAST | +/− 2 dil | 73% | / | [84] |
| Mucorales | 92 | AMB | CLSI | +/− 1 dil | 96.5% | / | [44] |
| Mucorales | 80 | AMB | CLSI | ND | ND | CA 87% | [85] |
| Mucorales | 14 | AMB | EUCAST | +/− 2 dil | 78.6% | 50% at +/− 1 dil | [81] |
| Mucorales | 35 | AMB | CLSI | +/− 2 dil | 91% | / | [66] |
| Mucorales | 45 | AMB | CLSI | +/− 2 dil | 70.5% | EA depends on incubation time | [86] |
| Mucorales | 10 | AMB | CLSI | +/− 2 dil | 90% | 90% at +/− 1dil | [76] |
| Mucorales | 21 | ITZ | CLSI | +/− 1 dil | 80% | / | [65] |
| Mucorales | 6 | ITZ | CLSI | +/− 2 dil | 83% | / | [73] |
| Mucorales | 45 | ITZ | CLSI | +/− 2 dil | 70.5% | EA depends on incubation time | [86] |
| Mucorales | 10 | ITZ | CLSI | +/− 2 dil | 50% | 20% at +/− 1dil | [76] |
| Mucorales | 21 | VRZ | CLSI | +/− 1 dil | 90% | / | [65] |
| Mucorales | 35 | VRZ | CLSI | +/− 2 dil | 100% | / | [66] |
| Mucorales | 131 | PSZ | EUCAST | +/− 2 dil | 77% | / | [84] |
| Mucorales | 21 | PSZ | CLSI | +/− 1 dil | 80% | / | [65] |
| Mucorales | 92 | PSZ | CLSI | +/− 1 dil | 95.7% | / | [44] |
| Mucorales | 80 | PSZ | CLSI | ND | ND | CA 67% | [85] |
| Mucorales | 14 | PSZ | EUCAST | +/− 2 dil | 100% | 78.6% at +/− 1 dil | [81] |
| Mucorales | 35 | PSZ | CLSI | +/− 2 dil | 94% | / | [66] |
| Mucorales | 45 | PSZ | CLSI | +/− 2 dil | 88.6% | EA depends on incubation time | [86] |
| Mucorales | 45 | ISA | CLSI | +/− 2 dil | 84.4% | 71.1% at +/− 1 dil | [63] |
| Mucorales | 35 | CAS | CLSI | +/− 2 dil | 100% | / | [66] |
| Mucorales | 35 | Mica | CLSI | +/− 2 dil | 100% | / | [66] |
| Organisms | Number of Isolates | ATF | Reference Technique | Endpoint Used for Comparison | Essential Agreement (EA) with Reference Technique | Comments | Reference |
|---|---|---|---|---|---|---|---|
| Fusarium | 20 | AMB | EUCAST | +/−2 dil | 95% | 80% at +/− 1 dil, CA 100% | [79] |
| Fusarium | 20 | AMB | CLSI | +/−2 dil | 90% | 60% at +/− 1 dil, CA 85% | [79] |
| Fusarium | 7 | AMB | EUCAST | +/−2 dil | 100% | 85.7% at +/− 1 dil | [81] |
| Fusarium | 34 | AMB | CLSI | +/−2 dil | 94% | / | [66] |
| Fusarium | 54 | AMB | EUCAST | +/−2 dil | 96% | / | [82] |
| Fusarium | 10 | AMB | CLSI | +/−2 dil | 70% | 10% at +/− 1 dil | [76] |
| Fusarium | 48 | AMB | CLSI | +/−2 dil | 72.9% | 54.2% at +/− 1 dil | [80] |
| Fusarium | 10 | AMB | CLSI | +/−2 dil | 40–70% | EA depends on incubation time | [60] |
| Fusarium | 7 | AMB | CLSI | +/−2 dil | 100% | Etest in MHG | [74] |
| Fusarium | 13 | ITZ | CLSI | +/−2 dil | 100% | / | [73] |
| Fusarium | 54 | ITZ | EUCAST | +/−2 dil | 100% | / | [82] |
| Fusarium | 10 | ITZ | CLSI | +/−2 dil | 90% | 90% at +/− 1 dil | [76] |
| Fusarium | 10 | ITZ | CLSI | +/−2 dil | 100% | / | [60] |
| Fusarium | 5 | ITZ | CLSI | +/− 1 dil | 80% | / | [65] |
| Fusarium | 20 | VRZ | EUCAST | +/−2 dil | 95% | 75% at +/− 1 dil, CA 95% | [79] |
| Fusarium | 20 | VRZ | CLSI | +/−2 dil | 95% | 80% at +/− 1 dil, CA 95% | [79] |
| Fusarium | 34 | VRZ | CLSI | +/−2 dil | 100% | / | [66] |
| Fusarium | 54 | VRZ | EUCAST | +/−2 dil | 100% | / | [82] |
| Fusarium | 48 | VRZ | CLSI | +/−2 dil | 91.7% | 62.5% at +/− 1 dil | [80] |
| Fusarium | 5 | VRZ | CLSI | +/− 1 dil | 80% | / | [65] |
| Fusarium | 7 | VRZ | CLSI | +/−2 dil | 100% | Etest in MHG | [74] |
| Fusarium | 20 | PSZ | EUCAST | +/−2 dil | 100% | 45% at +/− 1 dil, CA 90% | [79] |
| Fusarium | 20 | PSZ | CLSI | +/−2 dil | 85% | 70% at +/− 1 dil, CA 90% | [79] |
| Fusarium | 7 | PSZ | EUCAST | +/−2 dil | 100% | 100% at +/− 1 dil | [81] |
| Fusarium | 34 | PSZ | CLSI | +/−2 dil | 100% | / | [66] |
| Fusarium | 54 | PSZ | EUCAST | +/−2 dil | 96% | / | [82] |
| Fusarium | 5 | PSZ | CLSI | +/− 1 dil | 60% | / | [65] |
| Fusarium | 7 | PSZ | CLSI | +/−2 dil | 100% | Etest in MHG | [74] |
| Fusarium | 20 | ISA | CLSI | +/−2 dil | 85% | 65% at +/− 1 dil | [63] |
| Fusarium | 34 | CAS | CLSI | +/−2 dil | 100% | / | [66] |
| Fusarium | 10 | CAS | CLSI | +/−2 dil | 100% | All isolates R | [68] |
| Fusarium | 7 | CAS | CLSI | +/−2 dil | 100% | Etest in MHG, all isolates R | [74] |
| Fusarium | 34 | Mica | CLSI | +/−2 dil | 100% | / | [66] |
| Fusarium | 10 | Mica | CLSI | +/−2 dil | 100% | All isolates R | [68] |
| Fusarium | 10 | ANI | CLSI | +/−2 dil | 100% | All isolates R | [68] |
| Fusarium | 7 | ANI | CLSI | +/−2 dil | 100% | Etest in MHG, all isolates R | [74] |
| Organisms | Number of Isolates | ATF | Reference Technique | Endpoint Used for Comparison | Essential Agreement (EA) with Reference Technique | Comments | Reference |
|---|---|---|---|---|---|---|---|
| Scedosporium | 10 | AMB | CLSI | +/−2 dil | 100% | / | [60] |
| Scedosporium | 15 | AMB | CLSI | +/−2 dil | 20% Sa / 20% Sp | 20% Sa / 20% Sp at +/− 1 dil | [76] |
| Scedosporium | 25 | AMB | CLSI | +/−2 dil | 80% Sa / 100% Sp | / | [66] |
| Scedosporium | 10 | ITZ | CLSI | +/−2 dil | 100% | / | [60] |
| Scedosporium | 15 | ITZ | CLSI | +/−2 dil | 60% Sa / 100% Sp | 50% Sa / 100% Sp at +/− 1 dil | [76] |
| Scedosporium | 5 | ITZ | CLSI | +/−2 dil | 100% | / | [73] |
| Scedosporium | 25 | VRZ | CLSI | +/−2 dil | 90% Sa / 100% Sp | / | [66] |
| Scedosporium | 31 | VRZ | CLSI | +/−2 dil | 93.5% | 87.1% at +/− 1 dil; CA 93.6% | [83] |
| Scedosporium | 25 | PSZ | CLSI | +/−2 dil | 90% Sa / 100% Sp | / | [66] |
| Scedosporium | 22 | ISA | CLSI | +/−2 dil | 18.7% Sa / 100% Sp | 6.25% Sa / 100% Sp at +/− 1 dil | [63] |
| Scedosporium | 25 | CAS | CLSI | +/−2 dil | 63% Sa / 100% Sp | / | [66] |
| Scedosporium | 25 | Mica | CLSI | +/−2 dil | 37% Sa / 100% Sp | / | [66] |
| Species | ECV (µg/ml) for | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amphotericin B | Fluconazole | Itraconazole | Voriconazole | Posaconazole | |||||||||||
| Etest | CLSI | EUCAST | Etest | CLSI | EUCAST | Etest | CLSI | EUCAST | Etest | CLSI | EUCAST | Etest | CLSI | EUCAST | |
| C. albicans | 1 a | 2 a | 1 c | 1 b | 0.5 e | 1 c | 0.25 e | NA | 0.064 c | 0.03 e | 0.03 e | 0.125 c | 0.12 e | 0.06 e | NA |
| C. glabrata | 2 a | 2 a | 1 c | 64 e | 8 e | 32 c | 8 e | 4 e | 2.0 c | 2 e | 0.25 e | 1.0 c | NA | 1 e | NA |
| C. krusei | 4 a | 2 a | 1 c | NA | 32 e | 128 c | 2 e | 1 e | 1.0 c | 2 e | 0.5 e | 1.0 c | NA | 0.5 e | NA |
| C. parapsilosis | 2 a | 2 a | 1 c | 4 e | 1 e | 2 c | NA | NA | 0.125 c | 0.25 e | 0.03 e | 0.125 c | 0.12 e | 0.25 e | NA |
| C. tropicalis | 2 a | 2 a | 1 c | 4 e | 1 e | 2 c | 0.5 e | 0.5 e | 0.125 c | 0.5 e | 0.12 e | 0.125 c | 0.12 e | 0.12 e | NA |
| C. dubliniensis | 0.5 a,d | NA | NA | NA | 0.5 e | NA | NA | NA | 0.064 c | NA | 0.03 e | NA | NA | 0.25 e | NA |
| C. kefyr | 2 b | NA | NA | 1 b | NA | NA | NA | NA | NA | 0.03 b | NA | NA | NA | NA | NA |
| C. lusitaniae | 1 b | NA | NA | 1 b | 1 e | NA | NA | 0.5 e | 0.125 c | 0.03 b | 0.06 e | 0.064 c | NA | 0.06 e | NA |
| C. guilliermondii | 1 b | NA | NA | 4 b | 8 e | 16 c | NA | NA | 2.0 c | 0.125 b | 0.12 e | 0.25 c | NA | 0.5 e | NA |
| A. fumigatus | 2 a | 2 a | 1 a | NA | NA | NA | 2 e | 1 e | 1.0 c | 0.5 e | 1 e | 1.0 c | 0.25 e | 0.25 e | NA |
| A. flavus | 8 a | 4 a | 4 a | NA | NA | NA | 1 e | 1 e | 1.0 c | 0.5 e | 2 e | 2.0 c | 0.5 e | 0.5 e | NA |
| A. niger | 2 a | 2 a | 1 a | NA | NA | NA | 4 e | 4 e | 4.0 c | 1 e | 2 e | 2.0 c | 0.5 e | 2 e | NA |
| A. terreus | 16 a | 4 a | 4 a | NA | NA | NA | NA | 2 e | 0.5 c | NA | 2 e | 2.0 c | 0.25 e | 1 e | NA |
| A. nidulans | NA | NA | NA | NA | NA | NA | NA | NA | 1 c | NA | NA | NA | NA | NA | NA |
| Species | ECV (µg/mL) for | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Caspofungin | Micafungin | Anidulafungin | |||||||
| Etest | CLSI | EUCAST | Etest | CLSI | EUCAST | Etest | CLSI | EUCAST | |
| C. albicans | 0.5 a | NA | NA | 0.03 a | 0.03 a | 0.015 c | 0.016 a | 0.12 a | 0.03 c |
| C. glabrata | 1 a | NA | NA | 0.03 a | 0.03 a | 0.03 c | 0.03 a | 0.12 a | 0.06 c |
| C. krusei | 1 a | NA | NA | 0.25 a | 0.25 a | 0.25 c | 0.06 a | 0.25 a | 0.06 c |
| C. parapsilosis | 4 a | NA | NA | 2 a | 4 a | 2 c | 8 a,d | 8 a | 4 c |
| C. tropicalis | 1 a,d | NA | NA | 0.12 a,d | 0.06 a | 0.06 c | 0.03 a | 0.06 a | 0.06 c |
| C. kefyr | 0,25 b | NA | NA | 0.25 b | NA | NA | NA | NA | NA |
| C. lusitaniae | 1 b | NA | NA | NA | NA | NA | NA | NA | NA |
| C. guilliermondii | 2 b | NA | NA | NA | NA | NA | NA | NA | NA |
| A. fumigatus | 0.125 d | NA | NA | 0.016 b,d | NA | NA | NA | NA | NA |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dannaoui, E.; Espinel-Ingroff, A. Antifungal Susceptibly Testing by Concentration Gradient Strip Etest Method for Fungal Isolates: A Review. J. Fungi 2019, 5, 108. https://doi.org/10.3390/jof5040108
Dannaoui E, Espinel-Ingroff A. Antifungal Susceptibly Testing by Concentration Gradient Strip Etest Method for Fungal Isolates: A Review. Journal of Fungi. 2019; 5(4):108. https://doi.org/10.3390/jof5040108
Chicago/Turabian StyleDannaoui, Eric, and Ana Espinel-Ingroff. 2019. "Antifungal Susceptibly Testing by Concentration Gradient Strip Etest Method for Fungal Isolates: A Review" Journal of Fungi 5, no. 4: 108. https://doi.org/10.3390/jof5040108
APA StyleDannaoui, E., & Espinel-Ingroff, A. (2019). Antifungal Susceptibly Testing by Concentration Gradient Strip Etest Method for Fungal Isolates: A Review. Journal of Fungi, 5(4), 108. https://doi.org/10.3390/jof5040108