
Evaluation of Serum Biomarkers for Improved Diagnosis of Candidemia

 , , ,
, , ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Institutional Setting and Patient Cohort
2.2. Invasive Candidiasis (CAGTA) IgG VirClia Monotest
2.3. Wako β-D-Glucan Test
2.4. CandId Real-Time PCR
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taieb, F.; Méchaï, F.; Lefort, A.; Lanternier, F.; Bougnoux, M.E.; Lortholary, O. Management of candidemia and invasive candidiasis. Rev. Med. Interne 2011, 32, 173–180. [Google Scholar] [CrossRef]
- Koehler, P.; Stecher, M.; Cornely, O.A.; Koehler, D.; Vehreschild, M.J.G.T.; Bohlius, J.; Wisplinghoff, H.; Vehreschild, J.J. Morbidity and mortality of candidaemia in Europe: An epidemiologic meta-analysis. Clin. Microbiol. Infect. 2019, 25, 1200–1212. [Google Scholar] [CrossRef]
- Giacobbe, D.R.; Marelli, C.; Mora, S.; Guastavino, S.; Russo, C.; Brucci, G.; Limongelli, A.; Vena, A.; Mikulska, M.; Tayefi, M.; et al. Early diagnosis of candidemia with explainable machine learning on automatically extracted laboratory and microbiological data: Results of the AUTO-CAND project. Ann. Med. 2023, 55, 2285454. [Google Scholar] [CrossRef] [PubMed]
- Antinori, S.; Milazzo, L.; Sollima, S.; Galli, M.; Corbellino, M. Candidemia and invasive candidiasis in adults: A narrative review. Eur. J. Intern. Med. 2016, 34, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Parra-Sánchez, M.; Zakariya-Yousef Breval, I.; Castro Méndez, C.; García-Rey, S.; Loza Vazquez, A.; Úbeda Iglesias, A.; Macías Guerrero, D.; Romero Mejías, A.; León Gil, C.; Martín-Mazuelos, E.; et al. Candida albicans Germ-Tube Antibody: Evaluation of a New Automatic Assay for Diagnosing Invasive Candidiasis in ICU Patients. Mycopathologia 2017, 182, 645–652. [Google Scholar] [CrossRef]
- Eades, C.P.; Bakri, A.R.B.A.; Lau, J.C.Y.; Moore, C.B.; Novak-Frazer, L.; Richardson, M.D.; Rautemaa-Richardson, R. Comparison of β-1-3-D-Glucan and Candida Mannan Biomarker Assays with Serological Tests for the Diagnosis of Candidemia. J. Fungi 2023, 9, 813. [Google Scholar] [CrossRef] [PubMed]
- Mikulska, M.; Balletto, E.; Castagnola, E.; Mularoni, A. Beta-D-Glucan in Patients with Haematological Malignancies. J. Fungi 2021, 7, 1046. [Google Scholar] [CrossRef]
- Finkelman, M.A. Specificity Influences in (1→3)-β-d-Glucan-Supported Diagnosis of Invasive Fungal Disease. J. Fungi 2020, 7, 14. [Google Scholar] [CrossRef]
- Azim, A.; Ahmed, A. Diagnosis and management of invasive fungal diseases in non-neutropenic ICU patients, with focus on candidiasis and aspergillosis: A comprehensive review. Front. Cell. Infect. Microbiol. 2024, 14, 1256158. [Google Scholar] [CrossRef]
- Wang, K.; Luo, Y.; Zhang, W.; Xie, S.; Yan, P.; Liu, Y.; Li, Y.; Ma, X.; Xiao, K.; Fu, H.; et al. Diagnostic value of Candida mannan antigen and anti-mannan IgG and IgM antibodies for Candida infection. Mycoses 2020, 63, 181–188. [Google Scholar] [CrossRef]
- Martínez-Jiménez, M.C.; Muñoz, P.; Guinea, J.; Valerio, M.; Alonso, R.; Escribano, P.; Bouza, E. Potential role of Candida albicans germ tube antibody in the diagnosis of deep-seated candidemia. Med. Mycol. 2014, 52, 270–275. [Google Scholar] [CrossRef]
- Clancy, C.J.; Nguyen, M.H. Non-Culture Diagnostics for Invasive Candidiasis: Promise and Unintended Consequences. J. Fungi 2018, 4, 27. [Google Scholar] [CrossRef] [PubMed]
- Barantsevich, N.; Barantsevich, E. Diagnosis and Treatment of Invasive Candidiasis. Antibiotics 2022, 11, 718. [Google Scholar] [CrossRef]
- Wei, S.; Wu, T.; Wu, Y.; Ming, D.; Zhu, X. Diagnostic accuracy of Candida albicans germ tube antibody for invasive candidiasis: Systematic review and meta-analysis. Diagn. Microbiol. Infect. Dis. 2019, 93, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Pini, P.; Colombari, B.; Marchi, E.; Castagnoli, A.; Venturelli, C.; Sarti, M.; Blasi, E. Performance of Candida albicans germ tube antibodies (CAGTA) and its association with (1 → 3)-β-D-glucan (BDG) for diagnosis of invasive candidiasis (IC). Diagn. Microbiol. Infect. Dis. 2019, 93, 39–43. [Google Scholar] [CrossRef]
- León, C.; Ruiz-Santana, S.; Saavedra, P.; Castro, C.; Loza, A.; Zakariya, I.; Úbeda, A.; Parra, M.; Macías, D.; Tomás, J.I.; et al. Contribution of Candida biomarkers and DNA detection for the diagnosis of invasive candidiasis in ICU patients with severe abdominal conditions. Crit. Care 2016, 20, 149. [Google Scholar] [CrossRef] [PubMed]
- Arendrup, M.C.; Arikan-Akdagli, S.; Jørgensen, K.M.; Barac, A.; Steinmann, J.; Toscano, C.; Arsenijevic, V.A.; Sartor, A.; Lass-Flörl, C.; Hamprecht, A.; et al. European candidaemia is characterised by notable differential epidemiology and susceptibility pattern: Results from the ECMM Candida III study. J. Infect. 2023, 87, 428–437. [Google Scholar] [CrossRef]
- Karageorgopoulos, D.E.; Vouloumanou, E.K.; Ntziora, F.; Michalopoulos, A.; Rafailidis, P.I.; Falagas, M.E. β-D-glucan assay for the diagnosis of invasive fungal infections: A meta-analysis. Clin. Infect. Dis. 2011, 52, 750–770. [Google Scholar] [CrossRef]
- Clancy, C.J.; Nguyen, M.H. Diagnosing Invasive Candidiasis. J. Clin. Microbiol. 2018, 56, e01909-17. [Google Scholar] [CrossRef]
- Morjaria, S.; Frame, J.; Franco-Garcia, A.; Geyer, A.; Kamboj, M.; Babady, N.E. Clinical Performance of (1,3) Beta-D Glucan for the Diagnosis of Pneumocystis Pneumonia (PCP) in Cancer Patients Tested with PCP Polymerase Chain Reaction. Clin. Infect. Dis. 2019, 69, 1303–1309. [Google Scholar] [CrossRef]
- Friedrich, R.; Rappold, E.; Bogdan, C.; Held, J. Comparative Analysis of the Wako β-Glucan Test and the Fungitell Assay for Diagnosis of Candidemia and Pneumocystis jirovecii Pneumonia. J. Clin. Microbiol. 2018, 56, e00464-18. [Google Scholar] [CrossRef]
- Dichtl, K.; Seybold, U.; Wagener, J. Serological biomarkers of candidemia: A retrospective evaluation of three assays. Infection 2019, 47, 217–224. [Google Scholar] [CrossRef]
- De Carolis, E.; Marchionni, F.; Torelli, R.; Angela, M.G.; Pagano, L.; Murri, R.; De Pascale, G.; De Angelis, G.; Sanguinetti, M.; Posteraro, B. Comparative performance evaluation of Wako β-glucan test and Fungitell assay for the diagnosis of invasive fungal diseases. PLoS ONE 2020, 15, e0236095. [Google Scholar] [CrossRef] [PubMed]
- Monday, L.M.; Parraga Acosta, T.; Alangaden, G. T2Candida for the Diagnosis and Management of Invasive Candida Infections. J. Fungi 2021, 7, 178. [Google Scholar] [CrossRef] [PubMed]
- Camp, I.; Spettel, K.; Willinger, B. Molecular Methods for the Diagnosis of Invasive Candidiasis. J. Fungi 2020, 6, 101. [Google Scholar] [CrossRef] [PubMed]
- Price, J.S.; Fallon, M.; Posso, R.; Backx, M.; White, P.L. An Evaluation of the OLM CandID Real-Time PCR to Aid in the Diagnosis of Invasive Candidiasis When Testing Serum Samples. J. Fungi 2022, 8, 935. [Google Scholar] [CrossRef]
- Deckers, C.; Bélik, F.; Khourssaji, M.; Plum, P.E.; Ausselet, N.; Bulpa, P.; Sonet, A.; Bihin, B.; Huang, T.D.; Denis, O.; et al. A decade of candidaemia: A comprehensive analysis of prognosis and risk factors at a Belgian tertiary hospital. Diagn. Microbiol. Infect. Dis. 2024, 110, 116493. [Google Scholar] [CrossRef]
- Sullivan, D.J.; Westerneng, T.J.; Haynes, K.A.; Bennett, D.E.; Coleman, D.C. Candida dubliniensis sp. nov.: Phenotypic and molecular characterization of a novel species associated with oral candidosis in HIV-infected individuals. Microbiology 1995, 141 Pt 7, 1507–1521. [Google Scholar] [CrossRef]

{kind=link}
| Positive BD 1 (n = 35) | Negative BD 1 (n = 20) | |
|---|---|---|
| Demographics | ||
| Age (median years, range) Gender (male/female) | 69 (21–90) | 68 (23–90) |
| 21/14 | 14/6 | |
| Hospitalization Units 2 | ||
| ICU 3 (%) Onco-Hematology (%) Digestive Surgery (%) Internal Medicine (%) Urology (%) Geriatrics (%) Others (%) | 14 (40%) | 1 (5%) |
| 5 (14%) | 4 (20%) | |
| 4 (11%) | 1 (5%) | |
| 4 (11%) | 9 (45%) | |
| 3 (9%) | - | |
| 3 (9%) | 4 (20%) | |
| 2 (6%) | 1 (5%) | |
| Hospital admission reasons | ||
| Surgery (%) Severe bacterial infection (%) Febrile neutropenia (%) Gastrointestinal obstruction (%) Neoplastic recurrence (%) Viral infection (%) Others (%) | 12 (34%) | 5 (25%) |
| 8 (23%) | 5 (25%) | |
| 4 (11%) | 1 (5%) | |
| 4 (11%) | - | |
| 3 (9%) | 1 (5%) | |
| 2 (6%) | 4 (20%) | |
| 2 (6%) | 4 (20%) | |
| Antifungal exposure 4 | 3 (9%) | - |
| One-month mortality | 15 (43%) | 3 (15%) |
| Probable deep-seated candidiasis | 12 (34%) | - |
| Candida spp distribution 5 | ||
| Candida albicans Candida glabrata 6 Candida tropicalis Candida krusei Candida guillermondii Candida dubliniensis | 18 (51%) | - |
| 9 (26%) | - | |
| 5 (14%) | - | |
| 1 (3%) | - | |
| 1 (3%) | - | |
| 1 (3%) | - |
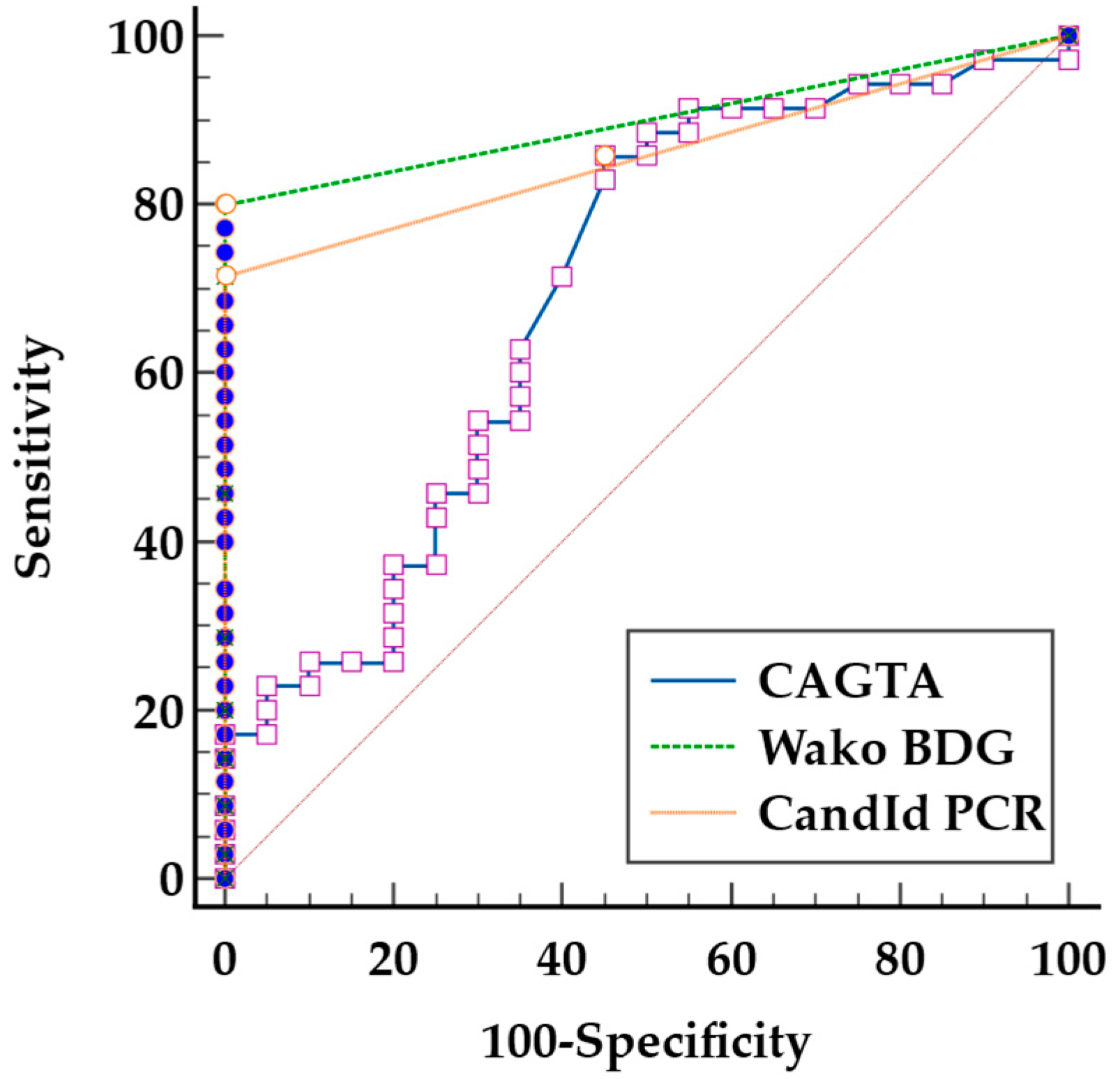
| Biomarker | Sens 1 (%) (95% CI 4) | Spec 2 (%) (95% CI) | AUC 3 (95% CI) |
|---|---|---|---|
| CAGTA 5 | 46 (29–63) | 75 (51–91) | 0.6 (0.4–0.7) |
| BDG 6 | 74 (57–87) | 100 (83–100) | 0.9 (0.7–0.9) |
| PCR 7 | 71 (54–85) | 100 (83–100) | 0.9 (0.7–0.9) |
| CAGTA and/or BDG | 86 (70–95) | 75 (51–91) | 0.8 (0.7–0.9) |
| CAGTA and/orPCR | 83 (66–93) | 75 (51–91) | 0.8 (0.7–0.9) |
| BDG and/orPCR | 91 (77–98) | 100 (83–100) | 0.9 (0.8–1) |
| CAGTA and/or BDG and/or PCR | 94 (81–99) | 75 (51–91) | 0.8 (0.7–0.9) |
| Candida spp. Candidemia | CAGTA 1 | Wako BDG 2 | CandId PCR 3 |
|---|---|---|---|
| Candida albicans (n = 18) | 10 (55%) | 14 (78%) | 15 (83%) |
| Candida glabrata (n = 9) | 4 (44%) | 8 (89%) | 4 (44%) |
| Candida tropicalis (n = 5) | 2 (40%) | 3 (60%) | 4 (80%) |
| Candida krusei (n = 1) | 0 (0%) | 0 (0%) | 1 (100%) |
| Candida guillermondii (n = 1) | 0 (0%) | 0 (0%) | 0 (0%) |
| Candida dubliniensis (n = 1) | 0 (0%) | 1 (100%) | 1 (100%) 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinet-Poleur, A.; Deckers, C.; Saad Albichr, I.; Bogaerts, P.; Honoré, P.M.; Bulpa, P.; Ausselet, N.; Foret, F.; Kidd, F.; Huang, T.-D.; et al. Evaluation of Serum Biomarkers for Improved Diagnosis of Candidemia. J. Fungi 2025, 11, 224. https://doi.org/10.3390/jof11030224
Kinet-Poleur A, Deckers C, Saad Albichr I, Bogaerts P, Honoré PM, Bulpa P, Ausselet N, Foret F, Kidd F, Huang T-D, et al. Evaluation of Serum Biomarkers for Improved Diagnosis of Candidemia. Journal of Fungi. 2025; 11(3):224. https://doi.org/10.3390/jof11030224
Chicago/Turabian StyleKinet-Poleur, Amélie, Corentin Deckers, Imane Saad Albichr, Pierre Bogaerts, Patrick M. Honoré, Pierre Bulpa, Nathalie Ausselet, Frederic Foret, François Kidd, Te-Din Huang, and et al. 2025. "Evaluation of Serum Biomarkers for Improved Diagnosis of Candidemia" Journal of Fungi 11, no. 3: 224. https://doi.org/10.3390/jof11030224
APA StyleKinet-Poleur, A., Deckers, C., Saad Albichr, I., Bogaerts, P., Honoré, P. M., Bulpa, P., Ausselet, N., Foret, F., Kidd, F., Huang, T.-D., & Montesinos, I. (2025). Evaluation of Serum Biomarkers for Improved Diagnosis of Candidemia. Journal of Fungi, 11(3), 224. https://doi.org/10.3390/jof11030224