
Holter Recordings at Initial Assessment for Long QT Syndrome: Relationship to Genotype Status and Cardiac Events


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.2.1. Patient Information
2.2.2. ECG Analysis
2.2.3. Holter Recordings and Analyses
2.2.4. Statistical Analyses
3. Results
3.1. Study Population
3.2. ECG Findings
3.3. Genotype Status
3.4. Symptomatic Status
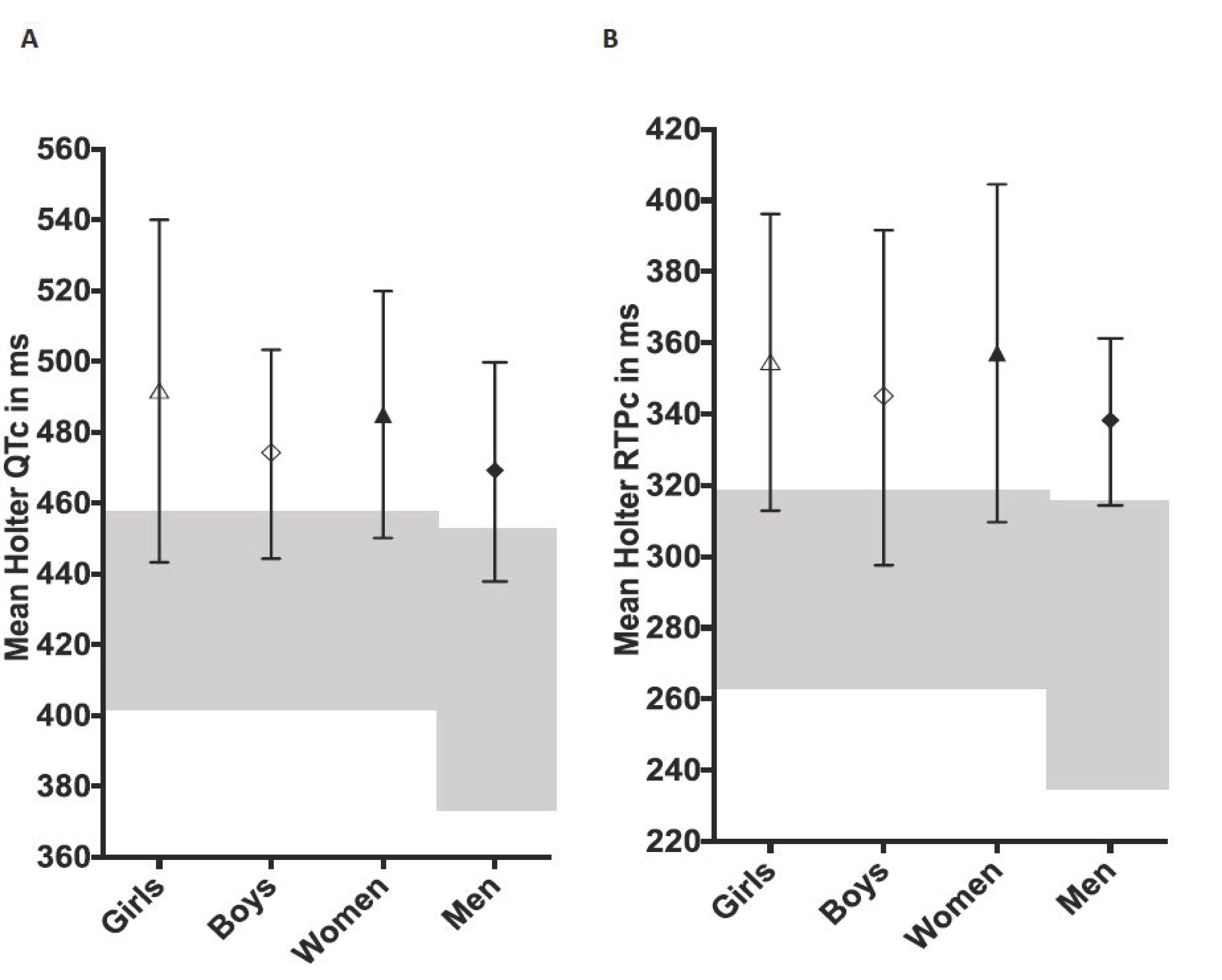
3.5. Diagnosis of LQTS Using Holter mQTc and mRTPc
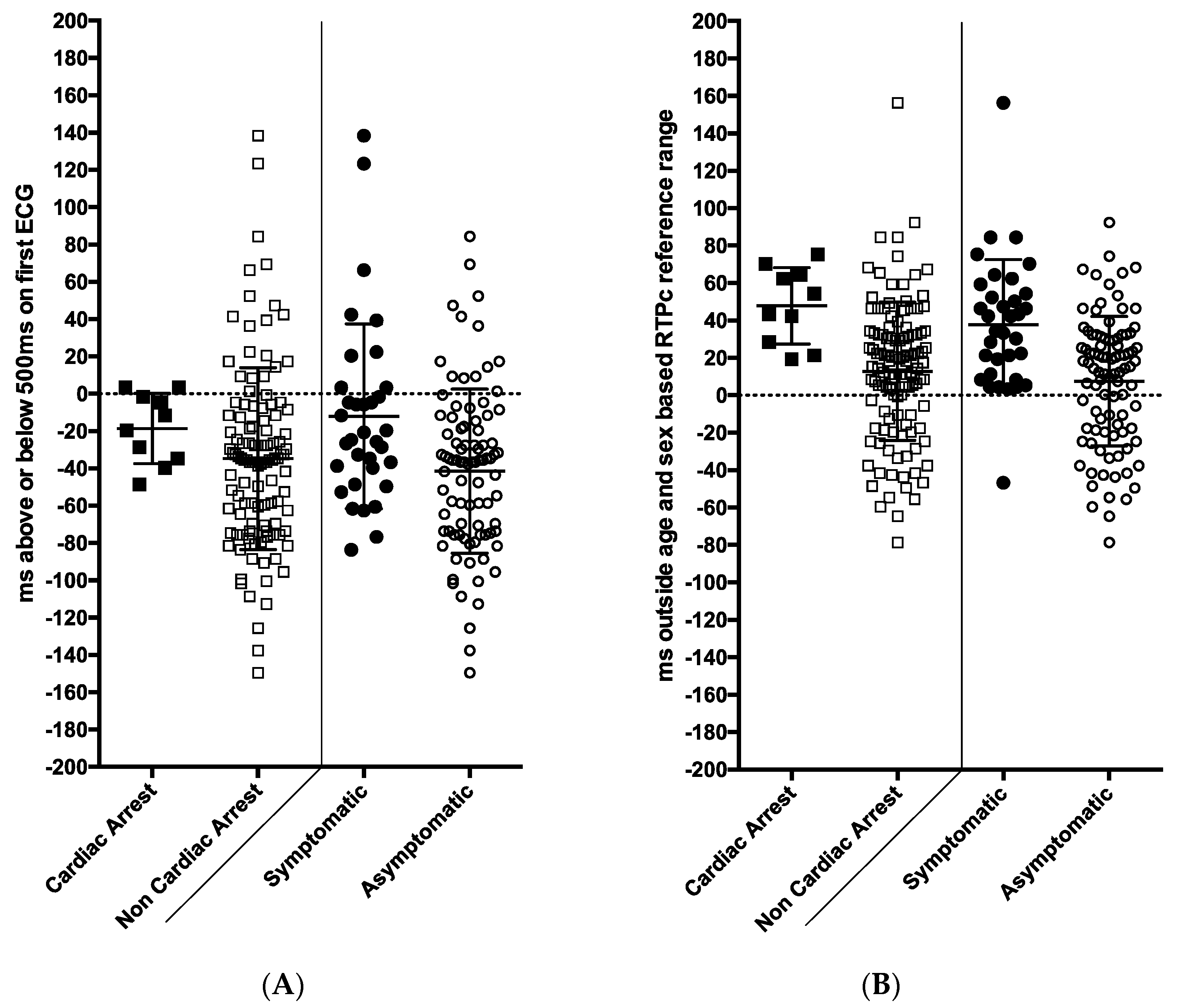
3.6. Predicting Risk of Syncope and Cardiac Arrest Using Holter Measurements and the Initial 12 Lead ECG
3.7. Comparison of Holter Measurements with 12-Lead ECG Measurements
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Priori, S.G.; Schwartz, P.J.; Napolitano, C.; Bloise, R.; Ronchetti, E.; Grillo, M.; Vicentini, A.; Spazzolini, C.; Nastoli, J.; Bottelli, G.; et al. Risk stratification in the long-QT syndrome. N. Engl. J. Med. 2003, 348, 1866–1874. [Google Scholar] [CrossRef] [PubMed]
- Vincent, G.M.; Timothy, K.W.; Leppert, M.; Keating, M. The spectrum of symptoms and QT intervals in carriers of the gene for the long-QT syndrome. N. Engl. J. Med. 1992, 327, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, E.S.; Priori, S.G.; Napolitano, C.; Schwartz, P.J.; Iyengar, S.; Elston, R.C.; Schnell, A.H.; Gorodeski, E.Z.; Rammohan, G.; Bahhur, N.O.; et al. Electrocardiographic prediction of abnormal genotype in congenital long QT syndrome: Experience in 101 related family members. J. Cardiovasc. Electrophysiol. 2001, 12, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.A.; Gula, L.J.; Klein, G.J.; Yee, R.; Skanes, A.C.; Krahn, A.D. Utility of treadmill testing in identification and genotype prediction in long-QT syndrome. Circ. Arrhythm. Electrophysiol. 2010, 3, 120–125. [Google Scholar] [CrossRef]
- Viskin, S.; Rosovski, U.; Sands, A.J.; Chen, E.; Kistler, P.M.; Kalman, J.M.; Rodriguez Chavez, L.; Iturralde Torres, P.; Cruz, F.F.; Centurion, O.A.; et al. Inaccurate electrocardiographic interpretation of long QT: The majority of physicians cannot recognize a long QT when they see one. Heart Rhythm 2005, 2, 569–574. [Google Scholar] [CrossRef]
- Eggeling, T.; Osterhues, H.H.; Hoeher, M.; Gabrielsen, F.G.; Weismueller, P.; Hombach, V. Value of Holter monitoring in patients with the long QT syndrome. Cardiology 1992, 81, 107–114. [Google Scholar] [CrossRef]
- Mauriello, D.A.; Johnson, J.N.; Ackerman, M.J. Holter monitoring in the evaluation of congenital long QT syndrome. Pacing Clin. Electrophysiol. 2011, 34, 1100–1104. [Google Scholar] [CrossRef]
- Halamek, J.; Couderc, J.P.; Jurak, P.; Vondra, V.; Zareba, W.; Viscor, I.; Leinveber, P. Measure of the QT-RR dynamic coupling in patients with the long QT syndrome. Ann. Noninvasive Electrocardiol. 2012, 17, 323–330. [Google Scholar] [CrossRef]
- Page, A.; Aktas, M.K.; Soyata, T.; Zareba, W.; Couderc, J.P. “QT clock” to improve detection of QT prolongation in long QT syndrome patients. Heart Rhythm 2016, 13, 190–198. [Google Scholar] [CrossRef]
- Waddell-Smith, K.E.; Chaptynova, A.A.; Li, J.; Crawford, J.R.; Hinds, H.; Skinner, J.R. Normative Heart-Rate Corrected Values for Repolarisation Length From Holter Recordings in Children and Adults. Heart Lung Circ. 2020, 29, 1469–1475. [Google Scholar] [CrossRef]
- Earle, N.; Crawford, J.; Smith, W.; Hayes, I.; Shelling, A.; Hood, M.; Stiles, M.; Maxwell, F.; Heaven, D.; Love, D.R.; et al. Community detection of long QT syndrome with a clinical registry: An alternative to ECG screening programs? Heart Rhythm 2013, 10, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Postema, P.G.; De Jong, J.S.; Van der Bilt, I.A.; Wilde, A.A. Accurate electrocardiographic assessment of the QT interval: Teach the tangent. Heart Rhythm 2008, 5, 1015–1018. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, I.; Moss, A.J. Long QT syndrome. J. Am. Coll. Cardiol. 2008, 51, 2291–2300. [Google Scholar] [CrossRef] [PubMed]
- Laguna, P.; Thakor, N.V.; Caminal, P.; Jane, R.; Yoon, H.R.; Bayes de Luna, A.; Marti, V.; Guindo, J. New algorithm for QT interval analysis in 24-hour Holter ECG: Performance and applications. Med. Biol. Eng. Comput. 1990, 28, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Follansbee, C.W.; Beerman, L.; Arora, G. Automated QT analysis on Holter monitors in pediatric patients can differentiate long QT syndrome from controls. Pacing Clin. Electrophysiol. 2018, 41, 50–56. [Google Scholar] [CrossRef]
- Page, A.; McNitt, S.; Xia, X.; Zareba, W.; Couderc, J.P. Population-based beat-to-beat QT analysis from Holter recordings in the long QT syndrome. J. Electrocardiol. 2017, 50, 787–791. [Google Scholar] [CrossRef]
- Arsenos, P.; Gatzoulis, K.A.; Dilaveris, P.; Gialernios, T.; Sideris, S.; Lazaros, G.; Archontakis, S.; Tsiachris, D.; Kartsagoulis, E.; Stefanadis, C. The rate-corrected QT interval calculated from 24-hour Holter recordings may serve as a significant arrhythmia risk stratifier in heart failure patients. Int. J. Cardiol. 2011, 147, 321–323. [Google Scholar] [CrossRef]
- Arsenos, P.; Gatzoulis, K.A.; Dilaveris, P.; Sideris, S.; Tousoulis, D. T wave alternans extracted from 30-minute short resting Holter ECG recordings predicts mortality in heart failure. J. Electrocardiol. 2018, 51, 588–591. [Google Scholar] [CrossRef]
- Arsenos, P.; Gatzoulis, K.A.; Laina, A.; Doundoulakis, I.; Soulaidopoulos, S.; Kordalis, A.; Oikonomou, G.; Triantafyllou, K.; Fragakis, N.; Vasilikos, V.; et al. QT interval extracted from 30-minute short resting Holter ECG recordings predicts mortality in heart failure. J. Electrocardiol. 2022, 72, 109–114. [Google Scholar] [CrossRef]
- Rautaharju, P.M.; Zhou, S.H.; Wong, S.; Calhoun, H.P.; Berenson, G.S.; Prineas, R.; Davignon, A. Sex differences in the evolution of the electrocardiographic QT interval with age. Can. J. Cardiol. 1992, 8, 690–695. [Google Scholar]
- Goldenberg, I.; Mathew, J.; Moss, A.J.; McNitt, S.; Peterson, D.R.; Zareba, W.; Benhorin, J.; Zhang, L.; Vincent, G.M.; Andrews, M.L.; et al. Corrected QT variability in serial electrocardiograms in long QT syndrome: The importance of the maximum corrected QT for risk stratification. J. Am. Coll. Cardiol. 2006, 48, 1047–1052. [Google Scholar] [CrossRef] [PubMed]
- Phan, D.Q.; Silka, M.J.; Lan, Y.T.; Chang, R.K. Comparison of formulas for calculation of the corrected QT interval in infants and young children. J. Pediatrics 2015, 166, 960–964.e2. [Google Scholar] [CrossRef] [PubMed]
- Crotti, L.; Spazzolini, C.; Porretta, A.P.; Dagradi, F.; Taravelli, E.; Petracci, B.; Vicentini, A.; Pedrazzini, M.; La Rovere, M.T.; Vanoli, E.; et al. Vagal reflexes following an exercise stress test: A simple clinical tool for gene-specific risk stratification in the long QT syndrome. J. Am. Coll. Cardiol. 2012, 60, 2515–2524. [Google Scholar] [CrossRef] [PubMed]
- Viskin, S.; Postema, P.G.; Bhuiyan, Z.A.; Rosso, R.; Kalman, J.M.; Vohra, J.K.; Guevara-Valdivia, M.E.; Marquez, M.F.; Kogan, E.; Belhassen, B.; et al. The response of the QT interval to the brief tachycardia provoked by standing: A bedside test for diagnosing long QT syndrome. J. Am. Coll. Cardiol. 2010, 55, 1955–1961. [Google Scholar] [CrossRef] [PubMed]
- Horner, J.M.; Horner, M.M.; Ackerman, M.J. The diagnostic utility of recovery phase QTc during treadmill exercise stress testing in the evaluation of long QT syndrome. Heart Rhythm 2011, 8, 1698–1704. [Google Scholar] [CrossRef]
- Sy, R.W.; van der Werf, C.; Chattha, I.S.; Chockalingam, P.; Adler, A.; Healey, J.S.; Perrin, M.; Gollob, M.H.; Skanes, A.C.; Yee, R.; et al. Derivation and validation of a simple exercise-based algorithm for prediction of genetic testing in relatives of LQTS probands. Circulation 2011, 124, 2187–2194. [Google Scholar] [CrossRef]
- Seethala, S.; Singh, P.; Shusterman, V.; Ribe, M.; Haugaa, K.H.; Němec, J. QT Adaptation and Intrinsic QT Variability in Congenital Long QT Syndrome. J. Am. Heart Assoc. 2015, 4, e002395. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All < 15 Years | All < 15 Years and Female ≥ 15 Years | Female ≥ 15 Years | Male ≥ 15 Years | ||
|---|---|---|---|---|---|
| 28 Family gene-negative subjects | Initial ECG QTc (ms) | 420 (30) | 418 (30) | 413 (31) | 430 (13) |
| Mean Holter mQTc (ms) | 436 (30) | 436 (27) | 435 (12) | 436 (22) | |
| Mean Holter mRTPc (ms) | 291 (26) | 292 (25) | 291 (10) | 285 (15) | |
| 101 Subjects with LQTS * | Initial ECG QTc (ms) | 477 (42) | 481 (43) | 492 (45) | 461 (43) |
| Mean Holter mQTc (ms) | 481 (39) | 482 (38) | 485 (35) | 469 (31) | |
| Mean Holter mRTPc (ms) | 349 (45) | 351 (46) | 357 (47) | 338 (25) | |
| Mean Value (SD) ms | Lower and Upper * Limits (Mean − 2SD and Mean + 2SD) ms | Highest Normative Mean Value Recorded, ms | |
|---|---|---|---|
| mQTc all females and males < 15 years | 424 (15) | 394–454 | 467 |
| mQTc males ≥ 15 years | 408 (19) | 370–446 | 436 |
| mRTPc all females and males < 15 years | 291 (14) | 263–319 | 325 |
| mRTPc males ≥ 15 years | 274 (20) | 234–314 | 303 |
| Sensitivity (%) | Specificity (%) | ||
| LQTS disease status | |||
| First ECG | QTc prolonged QTc > 500 ms | 69 23 | 92 100 |
| Holter mQTc > ULN | 85 | 75 | |
| Holter mRTPc > ULN | 89 | 86 | |
| Holter mRTPc > 30 ms above ULN | 48 | 100 | |
| Risk of Cardiac Symptoms | |||
| First ECG | QTc prolonged QTc > 500 ms | 74 24 | 26 85 |
| Holter mQTc > ULN | 94 | 36 | |
| Holter mQTc > 30 ms above ULN | 47 | 69 | |
| Holter mRTPc > 30 ms above ULN | 74 | 51 | |
| Risk of Cardiac Arrest | |||
| First ECG | QTc prolonged QTc > 500 ms | 80 20 | 46 82 |
| Holter mQTc > ULN | 90 | 29 | |
| Holter mQTc > 30 ms above ULN | 70 | 66 | |
| Holter mRTPc > 30 ms above ULN | 100 | 48 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waddell-Smith, K.E.; Chaptynova, A.A.; Li, J.; Crawford, J.R.; Hinds, H.; Skinner, J.R. Holter Recordings at Initial Assessment for Long QT Syndrome: Relationship to Genotype Status and Cardiac Events. J. Cardiovasc. Dev. Dis. 2022, 9, 164. https://doi.org/10.3390/jcdd9050164
Waddell-Smith KE, Chaptynova AA, Li J, Crawford JR, Hinds H, Skinner JR. Holter Recordings at Initial Assessment for Long QT Syndrome: Relationship to Genotype Status and Cardiac Events. Journal of Cardiovascular Development and Disease. 2022; 9(5):164. https://doi.org/10.3390/jcdd9050164
Chicago/Turabian StyleWaddell-Smith, Kathryn E., Alexandra A. Chaptynova, Jian Li, Jackie R. Crawford, Halina Hinds, and Jonathan R. Skinner. 2022. "Holter Recordings at Initial Assessment for Long QT Syndrome: Relationship to Genotype Status and Cardiac Events" Journal of Cardiovascular Development and Disease 9, no. 5: 164. https://doi.org/10.3390/jcdd9050164
APA StyleWaddell-Smith, K. E., Chaptynova, A. A., Li, J., Crawford, J. R., Hinds, H., & Skinner, J. R. (2022). Holter Recordings at Initial Assessment for Long QT Syndrome: Relationship to Genotype Status and Cardiac Events. Journal of Cardiovascular Development and Disease, 9(5), 164. https://doi.org/10.3390/jcdd9050164