
Pediatric Myocarditis: What Have We Learnt So Far?




Abstract
:1. Introduction
2. Definition of Myocarditis and Diagnostic Criteria
3. Epidemiology
4. Causes
4.1. Viral Myocarditis
4.2. Infectious Non-Viral Causes
4.3. Noninfectious Etiology
5. Pathogenesis
5.1. Viral Myocarditis
5.2. Autoimmune Pathway
6. Signs and Symptoms
6.1. Heart Failure
6.2. Arrhythmias
6.3. Chest Pain and Angina-Like Presentation
6.4. Sudden Death
7. Diagnosis in the Clinical Setting
7.1. Electrocardiography
7.2. Echocardiography
7.3. Laboratory Findings and Biomarkers
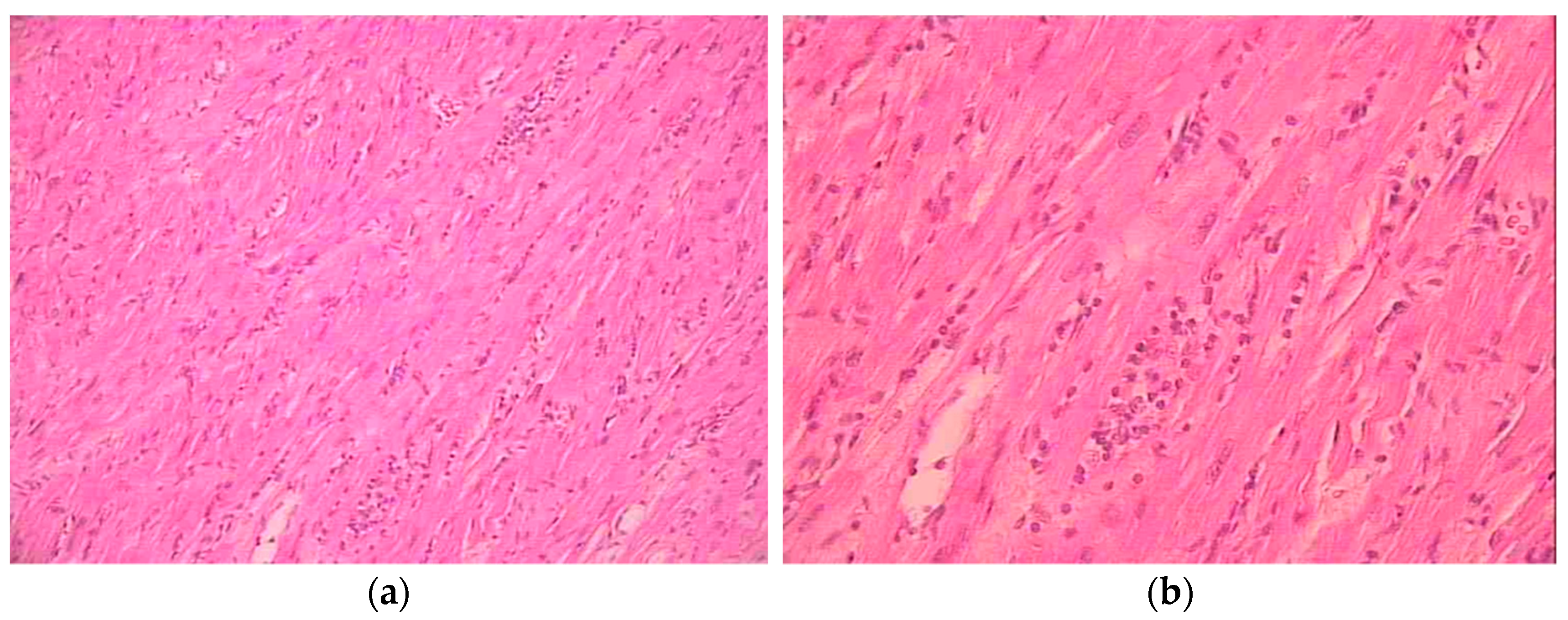
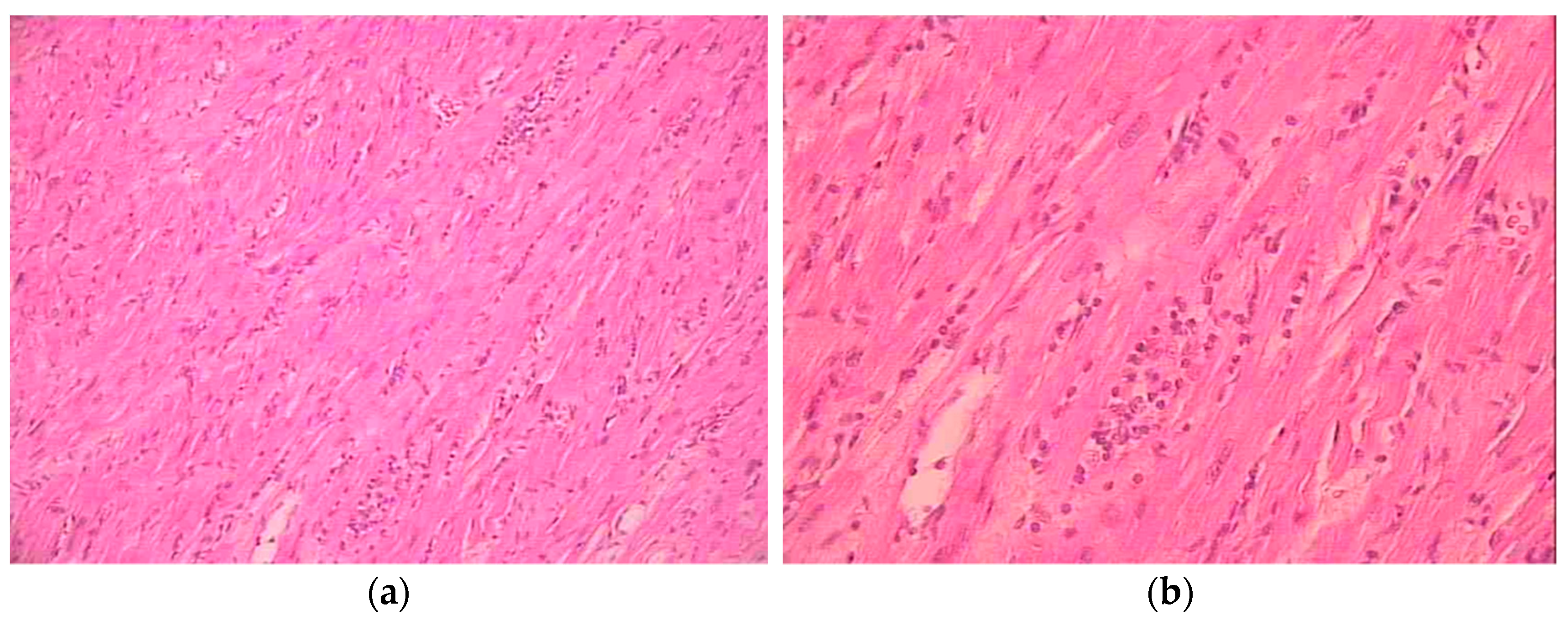
7.4. Endomyocardial Biopsy (EMB)
Giant Cell Myocarditis (GCM)
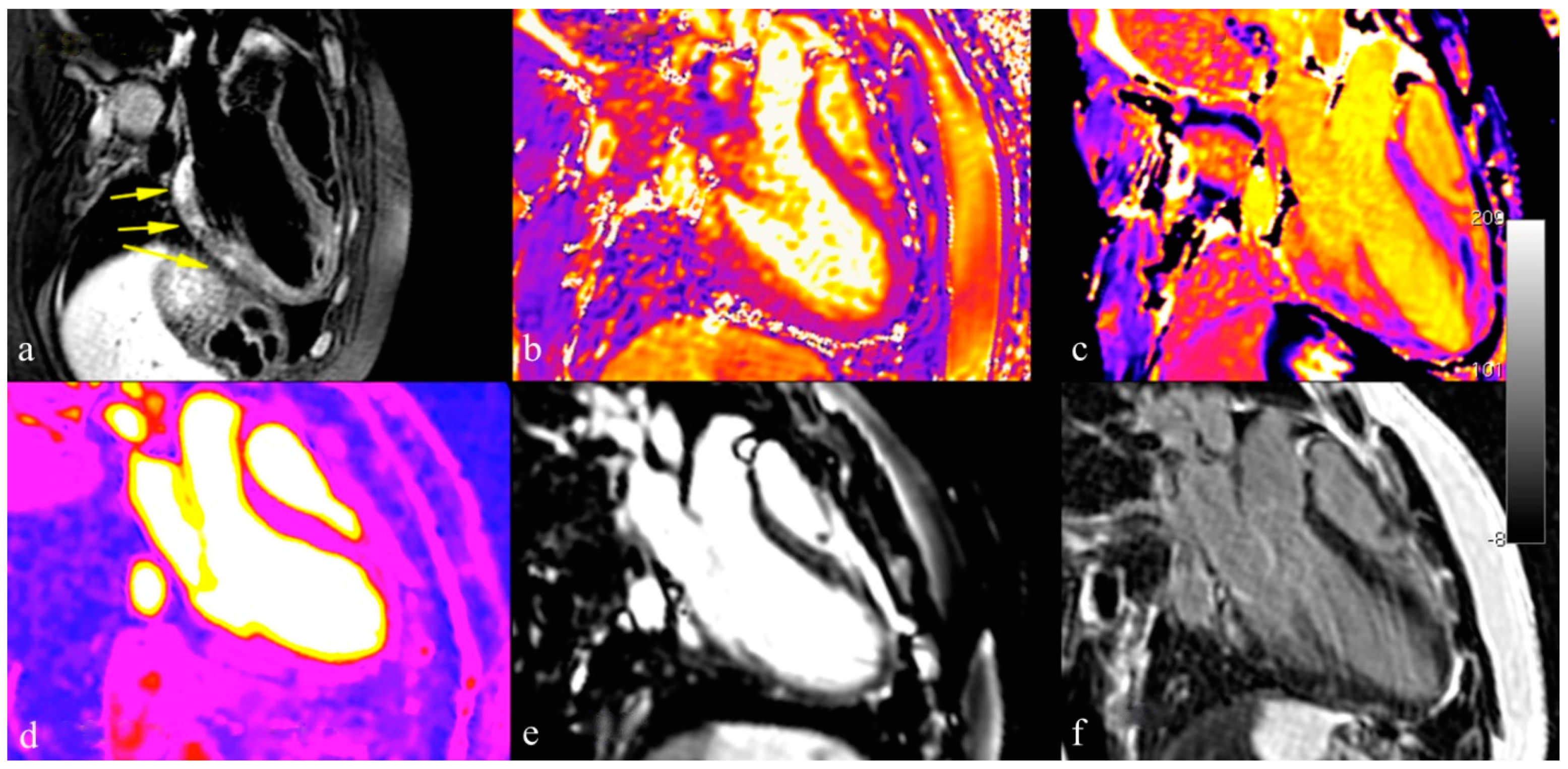
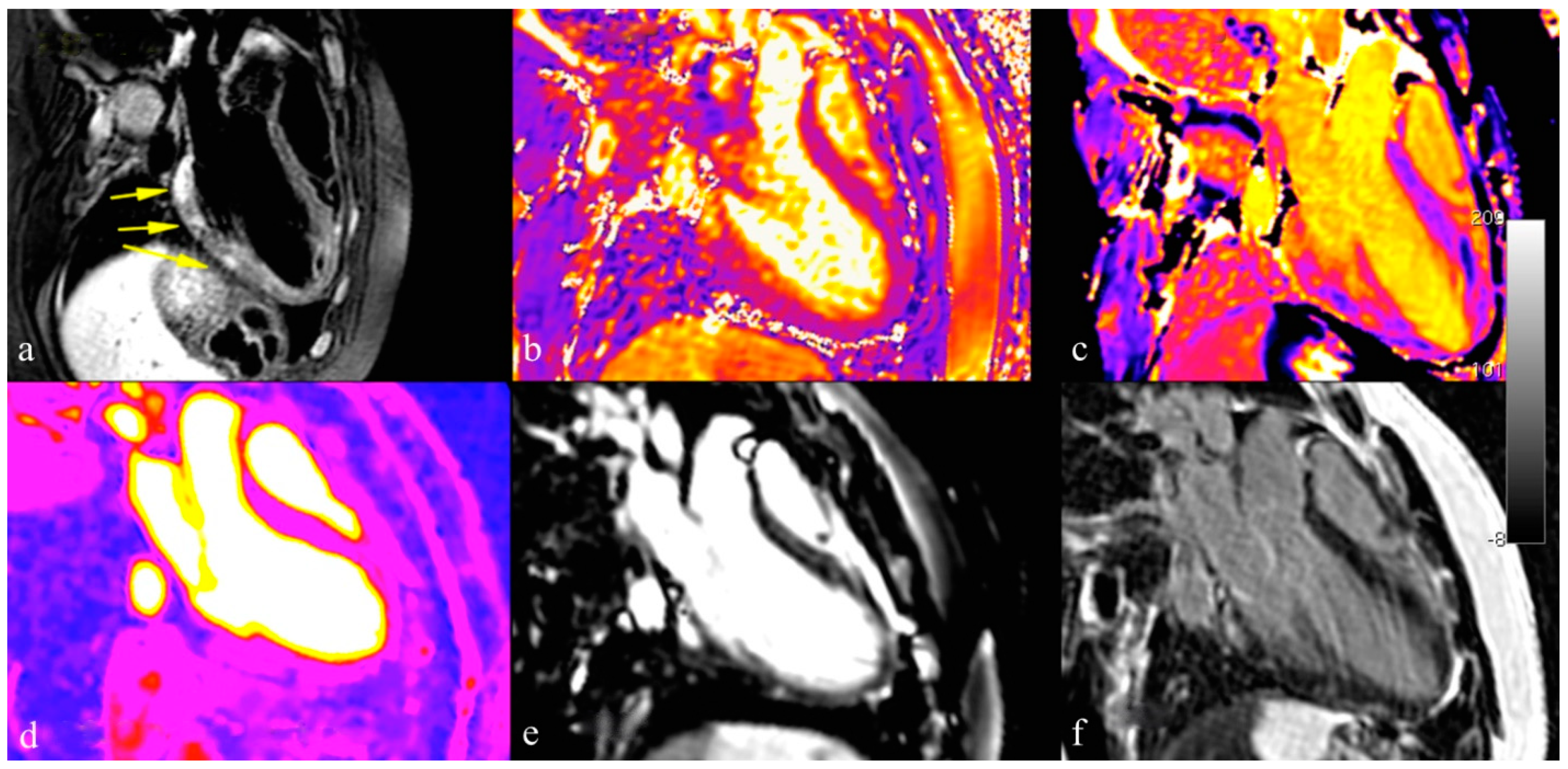
7.5. Cardiovascular Magnetic Resonance (CMR)
- (1)
- Regional high T2 intensity signal or high T2 intensity signal ratio suggestive for myocardial edema;
- (2)
- Increased early gadolinium enhancement (EGE) ratio, suggestive for hyperemia and/or capillary leak;
- (3)
- Presence of late gadolinium enhancement (LGE) of non-ischemic pattern, a sign of non-ischemic necrosis.
8. Therapy
8.1. Symptoms-Based Therapy
8.2. Circulatory Support
8.3. Immunosuppressive Therapy (IT)
8.4. Intravenous Immunoglobulin (IVIG)
8.5. Antivirals
9. Follow-Up
10. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef] [PubMed]
- Law, Y.M.; Lal, A.K.; Chen, S.; Čiháková, D.; Cooper, L.T., Jr.; Deshpande, S.; Godown, J.; Grosse-Wortmann, L.; Robinson, J.D.; Towbin, J.A. Diagnosis and Management of Myocarditis in Children: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e123–e135. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.P.; Malipiero, G.; Marcolongo, R.; Iliceto, S. Myocarditis: A Clinical Overview. Curr. Cardiol. Rep. 2017, 19, 63. [Google Scholar] [CrossRef] [PubMed]
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef]
- Richardson, P.; McKenna, R.W.; Bristow, M.; Maisch, B.; Mautner, B.; O'Connell, J.; Olsen, E.; Thiene, G.; Goodwin, J.; Gyarfas, I.; et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of Cardiomyopathies. Circulation 1996, 93, 841–842. [Google Scholar] [CrossRef]
- Aretz, H.T.; Billingham, M.E.; Edwards, W.D.; Factor, S.M.; Fallon, J.T.; Fenoglio, J.J. Jr.; Olsen, E.G.; Schoen, F.J. Myocarditis. A histopathologic definition and classification. Am. J. Cardiovasc. Pathol. 1987, 1, 3–14. [Google Scholar]
- Gagliardi, M.G.; Bevilacqua, M.; Di Renzi, P.; Picardo, S.; Passariello, R.; Marcelletti, C. Usefulness of magnetic resonance imaging for diagnosis of acute myocarditis in infants and children, and comparison with endomyocardial biopsy. Am. J. Cardiol. 1991, 68, 1089–1091. [Google Scholar] [CrossRef]
- Gagliardi, M.G.; Polletta, B.; Di Renzi, P. MRI for the diagnosis and follow-up of myocarditis. Circulation 1999, 99, 458–459. [Google Scholar] [CrossRef]
- Friedrich, M.G.; Sechtem, U.; Schulz-Menger, J.; Holmvang, G.; Alakija, P.; Cooper, L.T.; White, J.A.; Abdel-Aty, H.; Gutberlet, M.; Prasad, S.; et al. Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J. Am. Coll. Cardiol. 2009, 53, 1475–1487. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef]
- Cornicelli, M.D.; Rigsby, C.K.; Rychlik, K.; Pahl, E.; Robinson, J.D. Diagnostic performance of cardiovascular magnetic resonance native T1 and T2 mapping in pediatric patients with acute myocarditis. J. Cardiovasc. Magn. Reson. 2019, 21, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagliardi, M.G.; Bevilacqua, M.; Squitieri, C.; Boldrini, R.; Di Julio, D.P.; Marcelletti, C. Dilated cardiomyopathy caused by acute myocarditis in pediatric patients: Evolution of myocardial damage in a group of potential heart transplant candidates. J. Heart Lung Transpl. 1993, 12, S224–S229. [Google Scholar]
- Caforio, A.L.P.; Marcolongo, R.; Jahns, R.; Fu, M.; Felix, S.B.; Iliceto, S. Immune-mediated and autoimmune myocarditis: Clinical presentation, diagnosis and management. Heart Fail. Rev. 2013, 18, 715–732. [Google Scholar] [CrossRef] [PubMed]
- Vasudeva, R.; Bhatt, P.; Lilje, C.; Desai, P.; Amponsah, J.; Umscheid, J.; Parmar, N.; Bhatt, N.; Adupa, R.; Pagad, S.; et al. Trends in Acute Myocarditis Related Pediatric Hospitalizations in the United States, 2007–2016. Am. J. Cardiol. 2021, 149, 95–102. [Google Scholar] [CrossRef]
- Arola, A.; Pikkarainen, E.; Sipilä, J.O.T.; Pykäri, J.; Rautava, P.; Kytö, V. Occurrence and Features of Childhood Myocarditis: A Nationwide Study in Finland. J. Am. Heart Assoc. 2017, 6, e005306. [Google Scholar] [CrossRef] [Green Version]
- Butts, R.J.; Boyle, G.J.; Deshpande, S.R.; Gambetta, K.; Knecht, K.R.; Prada-Ruiz, C.A.; Richmond, M.E.; West, S.C.; Lal, A.K. Characteristics of Clinically Diagnosed Pediatric Myocarditis in a Contemporary Multi-Center Cohort. Pediatr. Cardiol. 2017, 38, 1175–1182. [Google Scholar] [CrossRef]
- Longson, M.; Cole, F.M.; Davies, D. Isolation of a Coxsackie virus group B, type 5, from the heart of a fatal case of myocarditis in an adult. J. Clin. Pathol. 1969, 22, 654–658. [Google Scholar] [CrossRef] [Green Version]
- Bowles, N.E.; Ni, J.; Kearney, D.L.; Pauschinger, M.; Schultheiss, H.P.; McCarthy, R.; Hare, J.; Bricker, J.T.; Bowles, K.R.; Towbin, J.A. Detection of viruses in myocardial tissues by polymerase chain reaction: Evidence of adenovirus as a common cause of myocarditis in children and adults. J. Am. Coll. Cardiol. 2003, 42, 466–472. [Google Scholar] [CrossRef] [Green Version]
- Gagliardi, M.G.; Fierabracci, A.; Pilati, M.; Chinali, M.; Bassano, C.; Saura, F.; Giovannoni, I.; Francalanci, P. The impact of specific viruses on clinical outcome in children presenting with acute heart failure. Int. J. Mol. Sci. 2016, 17, 486. [Google Scholar] [CrossRef]
- Foerster, S.R.; Canter, C.E. Contemporary etiology, outcomes, and therapy in pediatric myocarditis. Prog. Pediatr. Cardiol. 2011, 31, 123–128. [Google Scholar] [CrossRef]
- Sanna, G.; Serrau, G.; Bassareo, P.P.; Neroni, P.; Fanos, V.; Marcialis, M.A. Children’s heart and COVID-19: Up-to-date evidence in the form of a systematic review. Eur. J. Pediatr. 2020, 179, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Santonja, C.; Santos-Briz, A.; Palmedo, G.; Kutzner, H.; Requena, L. Detection of human parvovirus B19 DNA in 22% of 1815 cutaneous biopsies of a wide variety of dermatological conditions suggests viral persistence after primary infection and casts doubts on its pathogenic significance. Br. J. Dermatol. 2017, 177, 1060–1065. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.P.; Calabrese, F.; Angelini, A.; Tona, F.; Vinci, A.; Bottaro, S.; Ramondo, A.; Carturan, E.; Iliceto, S.; Thiene, G.; et al. A prospective study of biopsy-proven myocarditis: Prognostic relevance of clinical and aetiopathogenetic features at diagnosis. Eur. Heart J. 2007, 28, 1326–1333. [Google Scholar] [CrossRef] [Green Version]
- Dionne, A.; Sperotto, F.; Chamberlain, S.; Baker, A.L.; Powell, A.J.; Prakash, A.; Castellanos, D.A.; Saleeb, S.F.; De Ferranti, S.D.; Newburger, J.W.; et al. Association of Myocarditis with BNT162b2 Messenger RNA COVID-19 Vaccine in a Case Series of Children. JAMA Cardiol. 2021, 6, 1446–1450. [Google Scholar] [CrossRef] [PubMed]
- Kohli, U.; Desai, L.; Chowdhury, D.; Harahsheh, A.S.; Yonts, A.B.; Ansong, A.; Sabati, A.; Nguyen, H.H.; Hussain, T.; Khan, D.; et al. mRNA Coronavirus Disease 2019 Vaccine-Associated Myopericarditis in Adolescents: A Survey Study. J. Pediatr. 2022, 243, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Witberg, G.; Barda, N.; Hoss, S.; Richter, I.; Wiessman, M.; Aviv, Y.; Grinberg, T.; Auster, O.; Dagan, N.; Balicer, R.D.; et al. Myocarditis after COVID-19 Vaccination in a Large Health Care Organization. N. Engl. J. Med. 2021, 385, 2132–2139. [Google Scholar] [CrossRef] [PubMed]
- Matsumori, A.; Wang, H.; Abelmann, W.H.; Crumpacker, C.S. Treatment of viral myocarditis with ribavirin in an animal preparation. Circulation 1985, 71, 834–839. [Google Scholar] [CrossRef] [Green Version]
- Sato, Y.; Matsumori, A. Treatment of coxsackievirus B3 myocarditis by immunoactive peptide in an animal model. Clin. Immunol. Immunopathol. 1992, 65, 65–69. [Google Scholar] [CrossRef]
- Huang, C.H.; Vallejo, J.G.; Kollias, G.; Mann, D.L. Role of the Innate Immune System in Acute Viral Myocarditis. Basic Res. Cardiol. 2009, 104, 228. [Google Scholar] [CrossRef]
- Heymans, S.; Eriksson, U.; Lehtonen, J.; Cooper, L.T. The Quest for New Approaches in Myocarditis and Inflammatory Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 68, 2348–2364. [Google Scholar] [CrossRef]
- Liu, P.; Aitken, K.; Kong, Y.Y.; Opavsky, M.A.; Martino, T.; Dawood, F.; Wen, W.H.; Kozeiradzki, I.; Bachmaier, K.; Straus, D.; et al. The tyrosine kinase p56lck is essential in coxsackievirus B3-mediated heart disease. Nat. Med. 2000, 6, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Anzai, A.; Mindur, J.E.; Halle, L.; Sano, S.; Choi, J.L.; He, S.; McAlpine, C.S.; Chan, C.T.; Kahles, F.; Valet, C.; et al. Self-reactive CD4 + IL-3 + T cells amplify autoimmune inflammation in myocarditis by inciting monocyte chemotaxis. J. Exp. Med. 2019, 216, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Rose, N.R. Myocarditis: Infection versus autoimmunity. J. Clin. Immunol. 2009, 29, 730–737. [Google Scholar] [CrossRef]
- Klingel, K.; Hohenadl, C.; Canu, A.; Albrecht, M.; Seemann, M.; Mall, G.; Kandolf, R. Ongoing enterovirus-induced myocarditis is associated with persistent heart muscle infection: Quantitative analysis of virus replication, tissue damage, and inflammation. Proc. Natl. Acad. Sci. USA 1992, 89, 314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caforio, A.L.P.; Iliceto, S. Genetically determined myocarditis: Clinical presentation and immunological characteristics. Curr. Opin. Cardiol. 2008, 23, 219–226. [Google Scholar] [CrossRef]
- Campuzano, O.; Fernández-Falgueras, A.; Sarquella-Brugada, G.; Sanchez, O.; Cesar, S.; Mademont, I.; Allegue, C.; Mates, J.; Pérez-Serra, A.; Coll, M.; et al. A Genetically Vulnerable Myocardium May Predispose to Myocarditis. J. Am. Coll. Cardiol. 2015, 66, 2913–2914. [Google Scholar] [CrossRef] [Green Version]
- Rose, N.R.; Bona, C. Defining criteria for autoimmune diseases (Witebsky’s postulates revisited). Immunol. Today 1993, 14, 426–430. [Google Scholar] [CrossRef]
- Mahon, N.G.; Madden, B.P.; Caforio, A.L.P.; Elliott, P.M.; Haven, A.J.; Keogh, B.E.; Davies, M.J.; McKenna, W.J. Immunohistologic evidence of myocardial disease in apparently healthy relatives of patients with dilated cardiomyopathy. J. Am. Coll. Cardiol. 2002, 39, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Kindermann, I.; Kindermann, M.; Kandolf, R.; Klingel, K.; Bültmann, B.; Müller, T.; Lindinger, A.; Böhm, M. Predictors of outcome in patients with suspected myocarditis. Circulation 2008, 118, 639–648. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.; Keeling, P.J.; Zachara, E.; Mestroni, L.; Camerini, F.; Mann, J.M.; Bottazzo, G.F.; McKenna, W.J. Evidence from family studies for autoimmunity in dilated cardiomyopathy. Lancet 1994, 344, 773–777. [Google Scholar] [CrossRef]
- Caforio, A.L.P.; Marcolongo, R.; Basso, C.; Iliceto, S. Clinical presentation and diagnosis of myocarditis. Heart 2015, 101, 1332–1344. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.P.; Angelini, A.; Blank, M.; Shani, A.; Kivity, S.; Goddard, G.; Doria, A.; Schiavo, A.; Testolina, M.; Bottaro, S.; et al. Passive transfer of affinity-purified anti-heart autoantibodies (AHA) from sera of patients with myocarditis induces experimental myocarditis in mice. Int. J. Cardiol. 2015, 179, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Schulze, K.; Becker, B.F.; Schultheiss, H.P. Antibodies to the ADP/ATP carrier, an autoantigen in myocarditis and dilated cardiomyopathy, penetrate into myocardial cells and disturb energy metabolism in vivo. Circ. Res. 1989, 64, 179–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caforio, A.L.; Goldman, J.H.; Haven, A.J.; Baig, K.M.; Libera, L.D.; McKenna, W.J. Circulating cardiac-specific autoantibodies as markers of autoimmunity in clinical and biopsy-proven myocarditis. The Myocarditis Treatment Trial Investigators. Eur. Heart J. 1997, 18, 270–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagliardi, M.G.; Bevilacqua, M.; Bassano, C.; Leonardi, B.; Boldrini, R.; Camassei, F.D.; Fierabracci, A.; Ugazio, A.G.; Bottazzo, G.F. Long term follow up of children with myocarditis treated by immunosuppression and of children with dilated cardiomyopathy. Heart 2004, 90, 1167–1171. [Google Scholar] [CrossRef] [PubMed]
- Seidel, F.; Opgen-Rhein, B.; Rentzsch, A.; Boehne, M.; Wannenmacher, B.; Boecker, D.; Reineker, K.; Grafmann, M.; Wiegand, G.; Hecht, T.; et al. Clinical characteristics and outcome of biopsy-proven myocarditis in children—Results of the German prospective multicentre registry “MYKKE”. Int. J. Cardiol. 2022, 357, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Messroghli, D.R.; Pickardt, T.; Fischer, M.; Opgen-Rhein, B.; Papakostas, K.; Böcker, D.; Jakob, A.; Khalil, M.; Mueller, G.C.; Schmidt, F.; et al. Toward evidence-based diagnosis of myocarditis in children and adolescents: Rationale, design, and first baseline data of MYKKE, a multicenter registry and study platform. Am. Heart J. 2017, 187, 133–144. [Google Scholar] [CrossRef]
- Durani, Y.; Egan, M.; Baffa, J.; Selbst, S.M.; Nager, A.L. Pediatric myocarditis: Presenting clinical characteristics. Am. J. Emerg. Med. 2009, 27, 942–947. [Google Scholar] [CrossRef]
- Suthar, D.; Dodd, D.A.; Godown, J. Identifying Non-Invasive Tools to Distinguish Acute Myocarditis from Dilated Cardiomyopathy in Children. Pediatr. Cardiol. 2018, 39, 1134–1138. [Google Scholar] [CrossRef]
- Fairweather, D.L.; Cooper, L.T.; Blauwet, L.A. Sex and Gender Differences in Myocarditis and Dilated Cardiomyopathy. Curr. Probl. Cardiol. 2013, 38, 7–46. [Google Scholar] [CrossRef] [Green Version]
- Kociol, R.D.; Cooper, L.T.; Fang, J.C.; Moslehi, J.J.; Pang, P.S.; Sabe, M.A.; Shah, R.V.; Sims, D.B.; Thiene, G.; Vardeny, O. Recognition and Initial Management of Fulminant Myocarditis: A Scientific Statement from the American Heart Association. Circulation 2020, 141, E69–E92. [Google Scholar] [CrossRef] [PubMed]
- Casadonte, J.R.; Mazwi, M.L.; Gambetta, K.E.; Palac, H.L.; McBride, M.E.; Eltayeb, O.M.; Monge, M.C.; Backer, C.L.; Costello, J.M. Risk Factors for Cardiac Arrest or Mechanical Circulatory Support in Children with Fulminant Myocarditis. Pediatr. Cardiol. 2017, 38, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, R.; Sumitomo, N.; Komori, A.; Abe, Y.; Nakamura, T.; Fukuhara, J.; Matsumura, M.; Miyashita, M.; Kanamaru, H.; Ayusawa, M.; et al. The follow-up evaluation of electrocardiogram and arrhythmias in children with fulminant myocarditis. Circ. J. 2011, 75, 932–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canter, C.E.; Simpson, K.P. Diagnosis and treatment of myocarditis in children in the current era. Circulation 2014, 129, 115–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jindal, A.; Singhi, S. Acute chest pain. Indian J. Pediatr. 2011, 78, 1262–1267. [Google Scholar] [CrossRef]
- Angelini, A.; Calzolari, V.; Calabrese, F.; Boffa, G.M.; Maddalena, F.; Chioin, R.; Thiene, G. Myocarditis mimicking acute myocardial infarction: Role of endomyocardial biopsy in the differential diagnosis. Heart 2000, 84, 245–250. [Google Scholar] [CrossRef] [Green Version]
- Maron, B.J.; Doerer, J.J.; Haas, T.S.; Tierney, D.M.; Mueller, F.O. Sudden deaths in young competitive athletes: Analysis of 1866 deaths in the United States, 1980–2006. Circulation 2009, 119, 1085–1092. [Google Scholar] [CrossRef]
- Harris, K.M.; Mackey-Bojack, S.; Bennett, M.; Nwaudo, D.; Duncanson, E.; Maron, B.J. Sudden Unexpected Death Due to Myocarditis in Young People, Including Athletes. Am. J. Cardiol. 2021, 143, 131–134. [Google Scholar] [CrossRef]
- Jhamnani, S.; Fuisz, A.; Lindsay, J. The spectrum of electrocardiographic manifestations of acute myocarditis: An expanded understanding. J. Electrocardiol. 2014, 47, 941–947. [Google Scholar] [CrossRef]
- Skouri, H.N.; Dec, G.W.; Friedrich, M.G.; Cooper, L.T. Noninvasive imaging in myocarditis. J. Am. Coll. Cardiol. 2006, 48, 2085–2093. [Google Scholar] [CrossRef] [Green Version]
- Khoo, N.S.; Smallhorn, J.F.; Atallah, J.; Kaneko, S.; MacKie, A.S.; Paterson, I. Altered left ventricular tissue velocities, deformation and twist in children and young adults with acute myocarditis and normal ejection fraction. J. Am. Soc. Echocardiogr. 2012, 25, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Wisotzkey, B.L.; Soriano, B.D.; Albers, E.L.; Ferguson, M.; Buddhe, S. Diagnostic role of strain imaging in atypical myocarditis by echocardiography and cardiac MRI. Pediatr. Radiol. 2018, 48, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Gursu, H.A.; Cetin, I.I.; Azak, E.; Kibar, A.E.; Surucu, M.; Orgun, A.; Pamuk, U. The assessment of treatment outcomes in patients with acute viral myocarditis by speckle tracking and tissue Doppler methods. Echocardiography 2019, 36, 1666–1674. [Google Scholar] [CrossRef] [PubMed]
- Lauer, B.; Niederau, C.; Kühl, U.; Schannwell, M.; Pauschinger, M.; Strauer, B.E.; Schultheiss, H.P. Cardiac troponin T in patients with clinically suspected myocarditis. J. Am. Coll. Cardiol. 1997, 30, 1354–1359. [Google Scholar] [CrossRef] [Green Version]
- Januzzi, J.L.; Camargo, C.A.; Anwaruddin, S.; Baggish, A.L.; Chen, A.A.; Krauser, D.G.; Tung, R.; Cameron, R.; Nagurney, J.T.; Chae, C.U.; et al. The N-terminal Pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. Am. J. Cardiol. 2005, 95, 948–954. [Google Scholar] [CrossRef]
- Katzmann, J.L.; Schlattmann, P.; Rigopoulos, A.G.; Noutsias, E.; Bigalke, B.; Pauschinger, M.; Tschope, C.; Sedding, D.; Schulze, P.C.; Noutsias, M. Meta-analysis on the immunohistological detection of inflammatory cardiomyopathy in endomyocardial biopsies. Heart Fail. Rev. 2020, 25, 277–294. [Google Scholar] [CrossRef]
- Kandolf, R.; Ameis, D.; Kirschner, P.; Canu, A.; Hofschneider, P.H. In situ detection of enteroviral genomes in myocardial cells by nucleic acid hybridization: An approach to the diagnosis of viral heart disease. Proc. Natl. Acad. Sci. USA 1987, 84, 6272–6276. [Google Scholar] [CrossRef] [Green Version]
- Martin, A.B.; Webber, S.; Fricker, F.J.; Jaffe, R.; Demmler, G.; Kearney, D.; Zhang, Y.H.; Bodurtha, J.; Gelb, B.; Ni, J.; et al. Acute myocarditis. Rapid diagnosis by PCR in children. Circulation 1994, 90, 330–339. [Google Scholar] [CrossRef] [Green Version]
- Pophal, S.G.; Sigfusson, G.; Booth, K.L.; Bacanu, S.A.; Webber, S.A.; Ettedgui, J.A.; Neches, W.H.; Park, S.C. Complications of endomyocardial biopsy in children. J. Am. Coll. Cardiol. 1999, 34, 2105–2110. [Google Scholar] [CrossRef] [Green Version]
- Mills, K.I.; Vincent, J.A.; Zuckerman, W.A.; Hoffman, T.M.; Canter, C.E.; Marshall, A.C.; Blume, E.D.; Bergersen, L.; Daly, K.P. Is Endomyocardial Biopsy a Safe and Useful Procedure in Children with Suspected Cardiomyopathy? Pediatr. Cardiol. 2016, 37, 1200–1210. [Google Scholar] [CrossRef]
- Brighenti, M.; Donti, A.; Giulia Gagliardi, M.; Maschietto, N.; Marini, D.; Lombardi, M.; Vairo, U.; Agnoletti, G.; Milanesi, O.; Pongiglione, G.; et al. Endomyocardial biopsy safety and clinical yield in pediatric myocarditis: An Italian perspective. Catheter. Cardiovasc. Interv. 2016, 87, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, G.M. Myocarditis of giant-cell type in an infant. Am. J. Clin. Pathol. 1955, 25, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T.; Berry, G.J.; Shabetai, R. Idiopathic giant-cell myocarditis—natural history and treatment. Multicenter Giant Cell Myocarditis Study Group Investigators. N. Engl. J. Med. 1997, 336, 1860–1866. [Google Scholar] [CrossRef]
- Kittleson, M.M.; Minhas, K.M.; Irizarry, R.A.; Ye, S.Q.; Edness, G.; Breton, E.; Conte, J.V.; Tomaselli, G.; Garcia, J.G.N.; Hare, J.M. Gene expression in giant cell myocarditis: Altered expression of immune response genes. Int. J. Cardiol. 2005, 102, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Rosenstein, E.D.; Zucker, M.J.; Kramer, N. Giant cell myocarditis: Most fatal of autoimmune diseases. Semin. Arthritis Rheum. 2000, 30, 1–16. [Google Scholar] [CrossRef]
- Xu, J.; Brooks, E.G. Giant Cell Myocarditis: A Brief Review. Arch. Pathol. Lab. Med. 2016, 140, 1429–1434. [Google Scholar] [CrossRef] [Green Version]
- Hang, W.; Chen, C.; Seubert, J.M.; Wang, D.W. Fulminant myocarditis: A comprehensive review from etiology to treatments and outcomes. Signal Transduct. Target Ther. 2020, 5, 287. [Google Scholar] [CrossRef]
- Brailovsky, Y.; Masoumi, A.; Bijou, R.; Oliveros, E.; Sayer, G.; Takeda, K.; Uriel, N. Fulminant Giant Cell Myocarditis Requiring Bridge with Mechanical Circulatory Support to Heart Transplantation. JACC Case Rep. 2022, 4, 265–270. [Google Scholar] [CrossRef]
- Friedrich, M.G. Cardiovascular Magnetic Resonance for Myocardial Inflammation: Lake Louise Versus Mapping? Circ. Cardiovasc. Imaging 2018, 11, e008010. [Google Scholar] [CrossRef] [Green Version]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [CrossRef] [Green Version]
- Radunski, U.K.; Lund, G.K.; Stehning, C.; Schnackenburg, B.; Bohnen, S.; Adam, G.; Blankenberg, S.; Muellerleile, K. CMR in patients with severe myocarditis: Diagnostic value of quantitative tissue markers including extracellular volume imaging. JACC Cardiovasc. Imaging 2014, 7, 667–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, J.A.; Lee, Y.J.; Salerno, M. Diagnostic performance of extracellular volume, native T1, and T2 mapping versus Lake Louise criteria by cardiac magnetic resonance for detection of acute myocarditis a meta-analysis. Circ. Cardiovasc. Imaging 2018, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luetkens, J.A.; Faron, A.; Isaak, A.; Dabir, D.; Kuetting, D.; Feisst, A.; Schmeel, F.C.; Sprinkart, A.M.; Thomas, D. Comparison of Original and 2018 Lake Louise Criteria for Diagnosis of Acute Myocarditis: Results of a Validation Cohort. Radiol. Cardiothorac. Imaging 2019, 1, e190010. [Google Scholar] [CrossRef]
- Pitak, B.; Opgen-Rhein, B.; Schubert, S.; Reineker, K.; Wiegand, G.; Boecker, D.; Rentzsch, A.; Ruf, B.; Özcan, S.; Wannenmacher, B.; et al. Cardiovascular magnetic resonance in children with suspected myocarditis: Current practice and applicability of adult protocols. Cardiol. Young 2022, 1–9. [Google Scholar] [CrossRef]
- Pennington, D.G.; Swartz, M.T. Circulatory support in infants and children. Ann. Thorac. Surg. 1993, 55, 233–237. [Google Scholar] [CrossRef]
- Ghelani, S.J.; Spaeder, M.C.; Pastor, W.; Spurney, C.F.; Klugman, D. Demographics, trends, and outcomes in pediatric acute myocarditis in the United States, 2006 to 2011. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 622–627. [Google Scholar] [CrossRef] [Green Version]
- Dimas, V.V.; Morray, B.H.; Kim, D.W.; Almond, C.S.; Shahanavaz, S.; Tume, S.C.; Peng, L.F.; McElhinney, D.B.; Justino, H. A multicenter study of the impella device for mechanical support of the systemic circulation in pediatric and adolescent patients. Catheter. Cardiovasc. Interv. 2017, 90, 124–129. [Google Scholar] [CrossRef]
- Miera, O.; Germann, M.; Cho, M.Y.; Photiadis, J.; Walter, E.M.D.; Hetzer, R.; Berger, F.; Schmitt, K.R.L. Bridge to recovery in children on ventricular assist devices-protocol, predictors of recovery, and long-term follow-up. J. Heart Lung Transplant. 2018, 37, 1459–1466. [Google Scholar] [CrossRef]
- de By, T.M.M.H.; Schweiger, M.; Waheed, H.; Berger, F.; Hübler, M.; Özbaran, M.; Maruszewski, B.; Napoleone, C.P.; Loforte, A.; Meyns, B.; et al. The European Registry for Patients with Mechanical Circulatory Support (EUROMACS): First EUROMACS Paediatric (Paedi-EUROMACS) report. Eur. J. Cardiothorac. Surg. 2018, 54, 800–808. [Google Scholar] [CrossRef]
- Foerster, S.R.; Canter, C.E.; Cinar, A.; Sleeper, L.A.; Webber, S.A.; Pahl, E.; Kantor, P.F.; Alvarez, J.A.; Colan, S.D.; Jefferies, J.L.; et al. Ventricular remodeling and survival are more favorable for myocarditis than for idiopathic dilated cardiomyopathy in childhood: An outcomes study from the Pediatric Cardiomyopathy Registry. Circ. Heart Fail. 2010, 3, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Gajarski, R.J.; Towbin, J.A. Recent advances in the etiology, diagnosis, and treatment of myocarditis and cardiomyopathies in children. Curr. Opin. Pediatr. 1995, 7, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.W.; O’Connell, J.B.; Herskowitz, A.; Rose, N.R.; McManus, B.M.; Billingham, M.E.; Moon, T.E. A clinical trial of immunosuppressive therapy for myocarditis. The Myocarditis Treatment Trial Investigators. N. Engl. J. Med. 1995, 333, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Hufnagel, G.; Pankuweit, S.; Richter, A.; Schönian, U.; Maisch, B. The European Study of Epidemiology and Treatment of Cardiac Inflammatory Diseases (ESETCID). First epidemiological results. Herz 2000, 25, 279–285. [Google Scholar] [CrossRef]
- Chan, K.Y.; Iwahara, M.; Benson, L.N.; Wilson, G.J.; Freedom, R.M. Immunosuppressive therapy in the management of acute myocarditis in children: A clinical trial. J. Am. Coll. Cardiol. 1991, 17, 458–460. [Google Scholar] [CrossRef]
- Marcolongo, R.; Rizzo, S.; Cerutti, A.; Reffo, E.; Castaldi, B.; Baritussio, A.; Basso, C.; Di Salvo, G.; Caforio, A.L.P. The multiple faces of autoimmune/immune-mediated myocarditis in children: A biopsy-proven case series treated with immunosuppressive therapy. ESC Heart Fail. 2021, 8, 1604. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Li, X.; Li, D. Immunosuppressive Treatment for Myocarditis in the Pediatric Population: A Meta-Analysis. Front. Pediatr. 2019, 7, 430. [Google Scholar] [CrossRef] [PubMed]
- Drucker, N.A.; Colan, S.D.; Lewis, A.B.; Beiser, A.S.; Wessel, D.L.; Takahashi, M.; Baker, A.L.; Perez-Atayde, A.R.; Newburger, J.W. Gamma-globulin treatment of acute myocarditis in the pediatric population. Circulation 1994, 89, 252–257. [Google Scholar] [CrossRef] [Green Version]
- Basta, M.; Branch, D.R. 7th International Immunoglobulin Conference: Mechanisms of Action. Clin. Exp. Immunol. 2014, 178, 87. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.S.; Tseng, Y.H.; Chen, M.Y.; Chung, C.M.; Tsai, M.H.; Wang, P.C.; Chang, J.J.; Chen, T.H.; Lin, Y.S. In-hospital and post-discharge outcomes of pediatric acute myocarditis underwent after high-dose steroid or intravenous immunoglobulin therapy. BMC Cardiovasc. Disord. 2019, 19, 10. [Google Scholar] [CrossRef]
- Ettedgui, J.A.; Ladusans, E.; Bamford, M. Complete heart block as a complication of varicella. Int. J. Cardiol. 1987, 14, 362–365. [Google Scholar] [CrossRef]
- Shabtai, M.; Luft, B.; Waltzer, W.C.; Anaise, D.; Rapaport, F.T. Massive cytomegalovirus pneumonia and myocarditis in a renal transplant recipient: Successful treatment with DHPG. Transplant. Proc. 1988, 20, 562–563. [Google Scholar] [PubMed]
- Dasgupta, S.; Iannucci, G.; Mao, C.; Clabby, M.; Oster, M.E. Myocarditis in the pediatric population: A review. Congenit. Heart Dis. 2019, 14, 868–877. [Google Scholar] [CrossRef] [PubMed]
- Nardi, P.; Pellegrino, A.; Scafuri, A.; Olevano, C.; Bassano, C.; Zeitani, J.; Chiariello, L. Survival and durability of mitral valve repair surgery for degenerative mitral valve disease. J. Card. Surg. 2011, 26, 360–366. [Google Scholar] [CrossRef]
- Gentili, F.; Cafiero, G.; Perrone, M.A.; Bianco, M.; Salvati, A.; Giordano, U.; Kikina, S.S.; Guccione, P.; De Zorzi, A.; Galletti, L.; et al. The Effects of Physical Inactivity and Exercise at Home in Young Patients with Congenital Heart Disease during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10065. [Google Scholar] [CrossRef] [PubMed]
- Ferrero, P.; Piazza, I. Myocarditis in the pediatric population: CMR image appraisal of myocardial inflammation. Int. J. Cardiol. 2021, 329, 249–250. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, M.G.; Crea, F.; Polletta, B.; Bassano, C.; La Vigna, G.; Ballerini, L.; Ragonese, P. Coronary microvascular endothelial dysfunction in transplanted children. Eur. Heart J. 2001, 22, 254–260. [Google Scholar] [CrossRef]
- Leonardi, B.; Secinaro, A.; Calvieri, C.; Perrone, M.A.; Gimigliano, F.; Muscogiuri, G.; Carotti, A.; Drago, F. The role of 3D imaging in the follow-up of patients with repaired tetralogy of Fallot. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1698–1709. [Google Scholar] [CrossRef]
- Leonardi, B.; Gentili, F.; Perrone, M.A.; Sollazzo, F.; Cocomello, L.; Kikina, S.S.; Wald, R.M.; Palmieri, V.; Secinaro, A.; Gagliardi, M.G.; et al. Cardiopulmonary Exercise Testing in Repaired Tetralogy of Fallot: Multiparametric Overview and Correlation with Cardiac Magnetic Resonance and Physical Activity Level. J. Cardiovasc. Dev. Dis. 2022, 9, 26. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Diagnosis | Histological Findings |
|---|---|
| Myocarditis | Presence of inflammatory infiltrate of the myocardium AND necrosis and/or degeneration of adjacent myocytes of non-ischemic pattern (BOTH are requirements for the diagnosis) |
| Borderline Myocarditis | Too scarce inflammatory infiltrate OR presence of inflammatory infiltrate of the myocardium WITHOUT NECROSIS of the myocytes. |
| No Myocarditis | Absence of the above-mentioned histological features |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomiato, E.; Perrone, M.A.; Palmieri, R.; Gagliardi, M.G. Pediatric Myocarditis: What Have We Learnt So Far? J. Cardiovasc. Dev. Dis. 2022, 9, 143. https://doi.org/10.3390/jcdd9050143
Pomiato E, Perrone MA, Palmieri R, Gagliardi MG. Pediatric Myocarditis: What Have We Learnt So Far? Journal of Cardiovascular Development and Disease. 2022; 9(5):143. https://doi.org/10.3390/jcdd9050143
Chicago/Turabian StylePomiato, Elettra, Marco Alfonso Perrone, Rosalinda Palmieri, and Maria Giulia Gagliardi. 2022. "Pediatric Myocarditis: What Have We Learnt So Far?" Journal of Cardiovascular Development and Disease 9, no. 5: 143. https://doi.org/10.3390/jcdd9050143
APA StylePomiato, E., Perrone, M. A., Palmieri, R., & Gagliardi, M. G. (2022). Pediatric Myocarditis: What Have We Learnt So Far? Journal of Cardiovascular Development and Disease, 9(5), 143. https://doi.org/10.3390/jcdd9050143