
Higher Levels of Stress-Related Hair Steroid Hormones Are Associated with the Increased SCORE2 Risk Prediction Algorithm in Apparently Healthy Women

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Sociodemographic, Lifestyle and Health-Related Characteristics
2.3. Stress, Anxiety and Sleep Quality Measures
2.4. Anthropometric Parameters, Biochemical Analyses
2.5. Cardiovascular Risk Evaluation
2.6. Hair Steroid Hormone Analysis
2.7. Statistical Analysis
3. Results
3.1. Study Group Characteristics
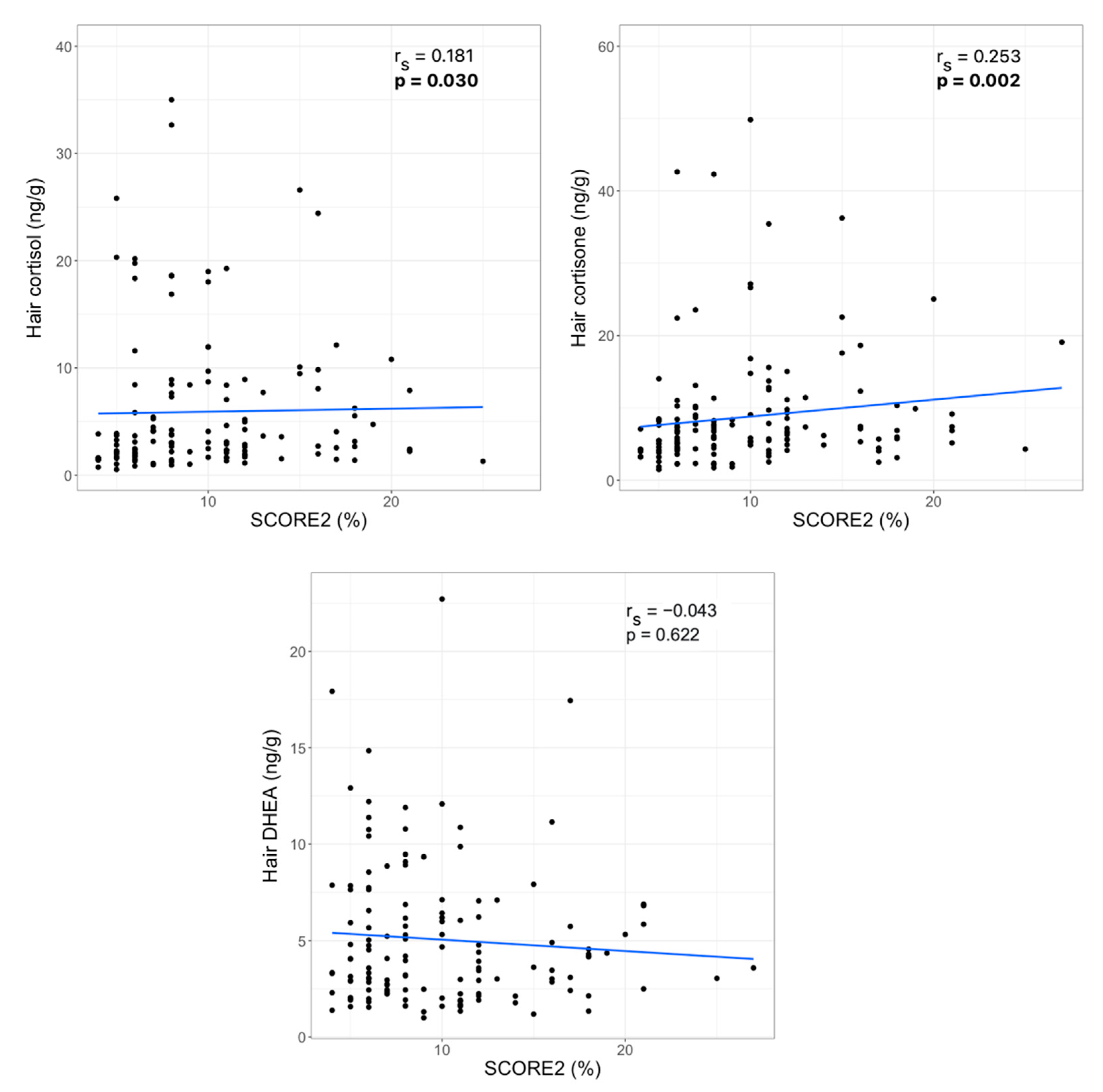
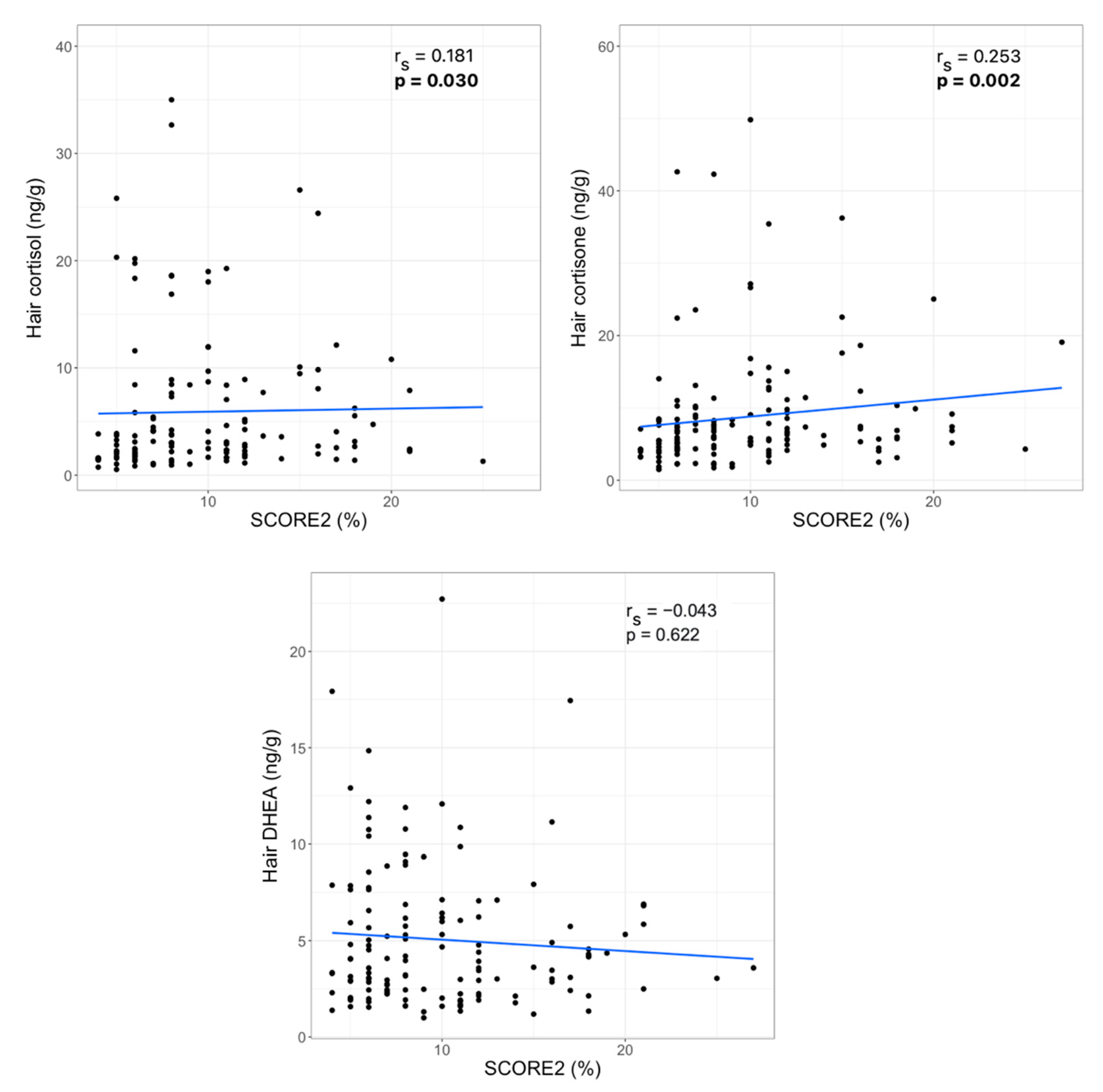
3.2. Hair Steroid Hormones and Cardiovascular Risk Factors
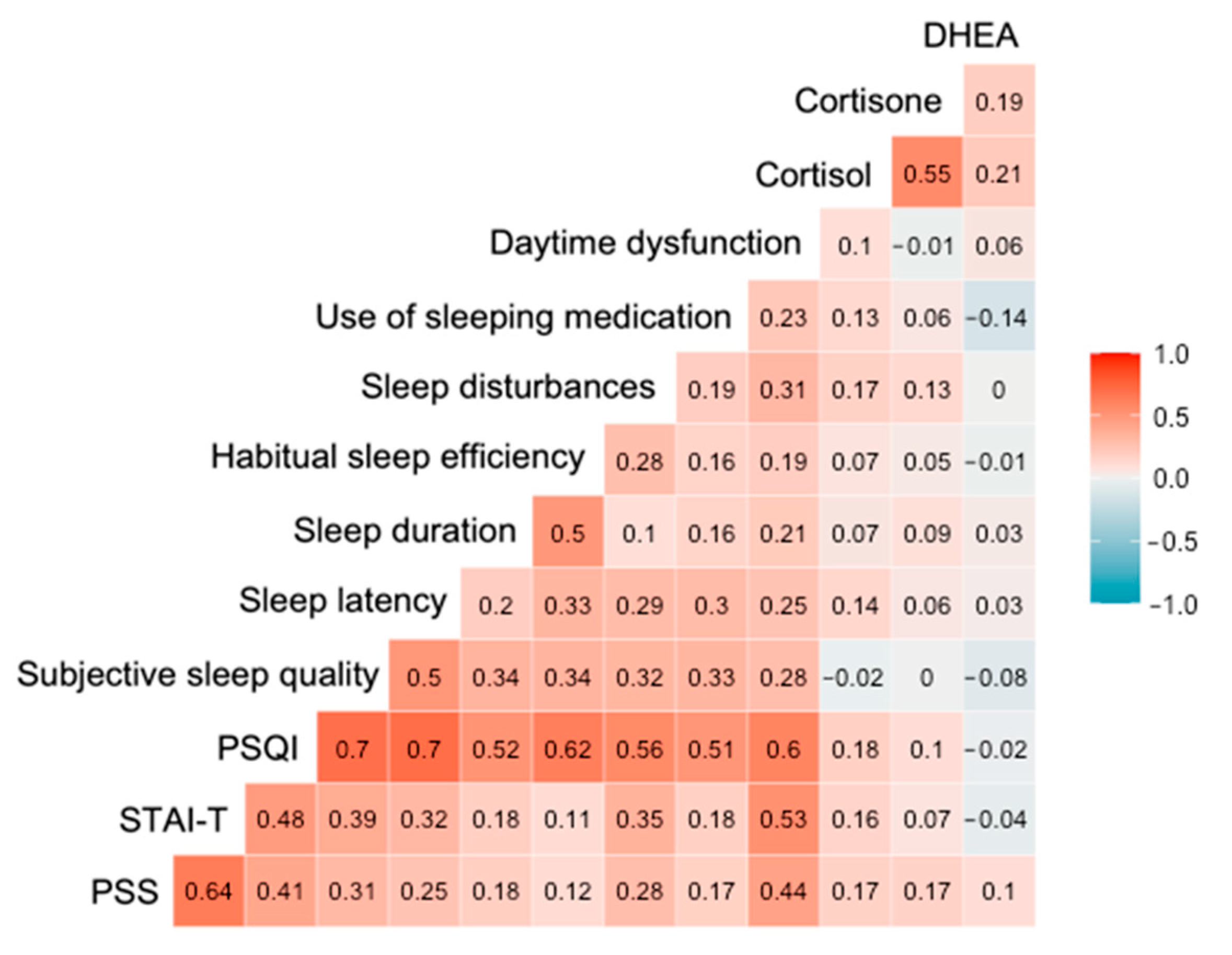
3.3. Hair Steroid Hormones, Self-Reported Stress, Anxiety and Sleep Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jagannathan, R.; Patel, S.A.; Ali, M.K.; Narayan, K.M.V. Global Updates on Cardiovascular Disease Mortality Trends and Attribution of Traditional Risk Factors. Curr. Diab. Rep. 2019, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; MacH, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.; Gwenin, C. Cortisol level dysregulation and its prevalence—Is it nature’s alarm clock? Physiol. Rep. 2021, 8, 1–9. [Google Scholar] [CrossRef]
- Steptoe, A.; Kivimäki, M. Stress and cardiovascular disease. Nat. Rev. Cardiol. 2012, 9, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Rosengren, A.; Hawken, S.; Ôunpuu, S.; Sliwa, K.; Zubaid, M.; Almahmeed, W.A.; Blackett, K.N. Association of psychosocial risk factors with risk of acute myocardial infarction in 11 119 cases and 13 648 controls from 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 953–962. [Google Scholar] [CrossRef]
- Dhaibar, H.A.; Cruz-Topete, D. Predisposition of Women to Cardiovascular Diseases: A Side-Effect of Increased Glucocorticoid Signaling During the COVID-19 Pandemic? Front. Glob. Women’s Health 2021, 2, 1–10. [Google Scholar] [CrossRef]
- Vaccarino, V.; Bremner, J.D. Behavioral, emotional and neurobiological determinants of coronary heart disease risk in women. Neurosci. Biobehav. Rev. 2017, 74, 297–309. [Google Scholar] [CrossRef] [Green Version]
- Geraghty, L.; Figtree, G.A.; Schutte, A.E.; Patel, S.; Woodward, M.; Arnott, C. Cardiovascular Disease in Women: From Pathophysiology to Novel and Emerging Risk Factors. Hear. Lung Circ. 2021, 30, 9–17. [Google Scholar] [CrossRef]
- Gong, I.Y.; Tan, N.S.; Ali, S.H.; Lebovic, G.; Mamdani, M.; Goodman, S.G.; Ko, D.T.; Laupacis, A.; Yan, A.T. Temporal Trends of Women Enrollment in Major Cardiovascular Randomized Clinical Trials. Can. J. Cardiol. 2019, 35, 653–660. [Google Scholar] [CrossRef]
- Dar, T.; Radfar, A.; Abohashem, S.; Pitman, R.K.; Tawakol, A.; Osborne, M.T. Psychosocial Stress and Cardiovascular Disease. Curr. Treat. Options Cardiovasc. Med. 2019, 21, 1–17. [Google Scholar] [CrossRef]
- Nicolaides, N.C.; Kyratzi, E.; Lamprokostopoulou, A.; Chrousos, G.P.; Charmandari, E. Stress, the stress system and the role of glucocorticoids. Neuroimmunomodulation 2014, 22, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Gray, M.J.; Litz, B.T.; Hsu, J.L.; Lombardo, T.W. Psychometric properties of the life events checklist. Assessment 2004, 11, 330–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelsten, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Ostiguy, C.S.; Ellenbogen, M.A.; Linnen, A.M.; Walker, E.F.; Hammen, C.; Hodgins, S. Chronic stress and stressful life events in the offspring of parents with bipolar disorder. J. Affect. Disord. 2009, 114, 74–84. [Google Scholar] [CrossRef] [Green Version]
- Mauss, D.; Jarczok, M.N. The streamlined allostatic load index is associated with perceived stress in life–findings from the MIDUS study. Stress 2021, 24, 404–412. [Google Scholar] [CrossRef]
- Phillips, R.; Kraeuter, A.K.; McDermott, B.; Lupien, S.; Sarnyai, Z. Human nail cortisol as a retrospective biomarker of chronic stress: A systematic review. Psychoneuroendocrinology 2021, 123. [Google Scholar] [CrossRef] [PubMed]
- Russell, E.; Koren, G.; Rieder, M.; Van Uum, S. Hair cortisol as a biological marker of chronic stress: Current status, future directions and unanswered questions. Psychoneuroendocrinology 2012, 37, 589–601. [Google Scholar] [CrossRef] [PubMed]
- Hellhammer, D.H.; Wüst, S.; Kudielka, B.M. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology 2009, 34, 163–171. [Google Scholar] [CrossRef]
- Stalder, T.; Kirschbaum, C. Analysis of cortisol in hair - State of the art and future directions. Brain. Behav. Immun. 2012, 26, 1019–1029. [Google Scholar] [CrossRef]
- Dettenborn, L.; Tietze, A.; Bruckner, F.; Kirschbaum, C. Higher cortisol content in hair among long-term unemployed individuals compared to controls. Psychoneuroendocrinology 2010, 35, 1404–1409. [Google Scholar] [CrossRef]
- Zhang, Y.; Shen, J.; Zhou, Z.; Sang, L.; Zhuang, X.; Chu, M.; Tian, T.; Xiao, J.; Lian, Y. Relationships among shift work, hair cortisol concentration and sleep disorders: A cross-sectional study in China. BMJ Open 2020, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Van Uum, S.H.M.; Sauvé, B.; Fraser, L.A.; Morley-Forster, P.; Paul, T.L.; Koren, G. Elevated content of cortisol in hair of patients with severe chronic pain: A novel biomarker for stress. Stress 2008, 11, 483–488. [Google Scholar] [CrossRef] [PubMed]
- El Mlili, N.; Ahabrach, H.; Cauli, O. Hair cortisol concentration as a biomarker of sleep quality and related disorders. Life 2021, 11, 81. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, L.L.; Acker, D.; du Plessis, S.; Stalder, T.; Suliman, S.; Thorne, M.Y.; Kirschbaum, C.; Seedat, S. Hair cortisol as a biomarker of stress and resilience in South African mixed ancestry females. Psychoneuroendocrinology 2020, 113, 104543. [Google Scholar] [CrossRef] [PubMed]
- Steudte-Schmiedgen, S.; Wichmann, S.; Stalder, T.; Hilbert, K.; Muehlhan, M.; Lueken, U.; Beesdo-Baum, K. Hair cortisol concentrations and cortisol stress reactivity in generalized anxiety disorder, major depression and their comorbidity. J. Psychiatr. Res. 2017, 84, 184–190. [Google Scholar] [CrossRef]
- Coello, K.; Munkholm, K.; Nielsen, F.; Vinberg, M.; Kessing, L.V. Hair cortisol in newly diagnosed bipolar disorder and unaffected first-degree relatives. Psychoneuroendocrinology 2019, 99, 183–190. [Google Scholar] [CrossRef]
- Davison, B.; Singh, G.R.; McFarlane, J. Hair cortisol and cortisone as markers of stress in indigenous and non-indigenous young adults. Stress 2019, 22, 210–220. [Google Scholar] [CrossRef]
- Dutheil, F.; de Saint Vincent, S.; Pereira, B.; Schmidt, J.; Moustafa, F.; Charkhabi, M.; Bouillon-Minois, J.B.; Clinchamps, M. DHEA as a Biomarker of Stress: A Systematic Review and Meta-Analysis. Front. Psychiatry 2021, 12, 1–14. [Google Scholar] [CrossRef]
- Doan, S.N.; DeYoung, G.; Fuller-Rowell, T.E.; Liu, C.; Meyer, J. Investigating relations among stress, sleep and nail cortisol and DHEA. Stress 2018, 21, 188–193. [Google Scholar] [CrossRef]
- Ullmann, E.; Barthel, A.; Petrowski, K.; Stalder, T.; Kirschbaum, C.; Bornstein, S.R. Pilot study of adrenal steroid hormones in hair as an indicator of chronic mental and physical stress. Nat. Sci. Reports 2016, 6, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Kristensen, S.K.; Larsen, S.C.; Olsen, N.J.; Fahrenkrug, J.; Heitmann, B.L. Hair dyeing, hair washing and hair cortisol concentrations among women from the healthy start study. Psychoneuroendocrinology 2017, 77, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Staufenbiel, S.M.; Penninx, B.W.J.H.; de Rijke, Y.B.; van den Akker, E.L.T.; van Rossum, E.F.C. Determinants of hair cortisol and hair cortisone concentrations in adults. Psychoneuroendocrinology 2015, 60, 182–194. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D. Manual for the State-Trait Anxiety Inventory (STAI); Mind Garden, Inc.: Menlo Park, CA, USA, 1968. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Mažeikienė, A.; Bekesiene, S.; Karčiauskaitė, D.; Mazgelytė, E.; Larsson, G.; Petrėnas, T.; Kaminskas, A.; Songailienė, J.; Utkus, A.; Vaičaitienė, R.; et al. The Association between Endogenous Hair Steroid Hormones and Social Environmental Factors in a Group of Conscripts during Basic Military Training. Int. J. Environ. Res. Public Health 2021, 18, 12239. [Google Scholar] [CrossRef] [PubMed]
- Izawa, S.; Miki, K.; Tsuchiya, M.; Yamada, H.; Nagayama, M. Hair and fingernail cortisol and the onset of acute coronary syndrome in the middle-aged and elderly men. Psychoneuroendocrinology 2019, 101, 240–245. [Google Scholar] [CrossRef]
- Faresjö, T.; Strömberg, S.; Jones, M.; Stomby, A.; Karlsson, J.E.; Östgren, C.J.; Faresjö, Å.; Theodorsson, E. Elevated levels of cortisol in hair precede acute myocardial infarction. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Pereg, D.; Gow, R.; Mosseri, M.; Lishner, M.; Rieder, M.; Van Uum, S.; Koren, G. Hair cortisol and the risk for acute myocardial infarction in adult men. Stress 2011, 14, 73–81. [Google Scholar] [CrossRef]
- Manenschijn, L.; Schaap, L.; Van Schoor, N.M.; Van Der Pas, S.; Peeters, G.M.E.E.; Lips, P.; Koper, J.W.; Van Rossum, E.F.C. High long-term cortisol levels, measured in scalp hair, are associated with a history of cardiovascular disease. J. Clin. Endocrinol. Metab. 2013, 98, 2078–2083. [Google Scholar] [CrossRef] [Green Version]
- Bossé, S.; Stalder, T.; D’Antono, B. Childhood Trauma, Perceived Stress, and Hair Cortisol in Adults with and Without Cardiovascular Disease. Psychosom. Med. 2018, 80, 393–402. [Google Scholar] [CrossRef]
- Nafisa, A.; Wattoo, F.H.; Qayyum, M.; Gulfraz, M. The association between chronic stress, hair cortisol, and angiographically documented coronary atherosclerosis, a case-control study. Stress 2021, 1–8. [Google Scholar] [CrossRef]
- Abell, J.G.; Stalder, T.; Ferrie, J.E.; Shipley, M.J.; Kirschbaum, C.; Kivimäki, M.; Kumari, M. Assessing cortisol from hair samples in a large observational cohort: The Whitehall II study. Psychoneuroendocrinology 2016, 73, 148–156. [Google Scholar] [CrossRef] [Green Version]
- Iob, E.; Steptoe, A. Cardiovascular Disease and Hair Cortisol: A Novel Biomarker of Chronic Stress. Curr. Cardiol. Rep. 2019, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanaelst, B.; Michels, N.; De Vriendt, T.; Huybrechts, I.; Vyncke, K.; Sioen, I.; Bammann, K.; Rivet, N.; Raul, J.S.; Molnar, D.; et al. Cortisone in hair of elementary school girls and its relationship with childhood stress. Eur. J. Pediatr. 2013, 172, 843–846. [Google Scholar] [CrossRef] [PubMed]
- van der Valk, E.; Abawi, O.; Mohseni, M.; Abdelmoumen, A.; Wester, V.; van der Voorn, B.; Iyer, A.; van den Akker, E.; Hoeks, S.; van den Berg, S.; et al. Cross-sectional relation of long-term glucocorticoids in hair with anthropometric measurements and their possible determinants: A systematic review and meta-analysis. Obes. Rev. 2021, 1–21. [Google Scholar] [CrossRef]
- Bautista, L.E.; Bajwa, P.K.; Shafer, M.M.; Malecki, K.M.C.; McWilliams, C.A.; Palloni, A. The relationship between chronic stress, hair cortisol and hypertension. Int. J. Cardiol. Hypertens. 2019, 2, 1–6. [Google Scholar] [CrossRef]
- Stalder, T.; Steudte-Schmiedgen, S.; Alexander, N.; Klucken, T.; Vater, A.; Wichmann, S.; Kirschbaum, C.; Miller, R. Stress-related and basic determinants of hair cortisol in humans: A meta-analysis. Psychoneuroendocrinology 2017, 77, 261–274. [Google Scholar] [CrossRef]
- Kuehl, L.K.; Hinkelmann, K.; Muhtz, C.; Dettenborn, L.; Wingenfeld, K.; Spitzer, C.; Kirschbaum, C.; Wiedemann, K.; Otte, C. Hair cortisol and cortisol awakening response are associated with criteria of the metabolic syndrome in opposite directions. Psychoneuroendocrinology 2015, 51, 365–370. [Google Scholar] [CrossRef]
- Stalder, T.; Kirschbaum, C.; Alexander, N.; Bornstein, S.R.; Gao, W.; Miller, R.; Stark, S.; Bosch, J.A.; Fischer, J.E. Cortisol in hair and the metabolic syndrome. J Clin Endocrinol Metab 2013, 98, 2573–2580. [Google Scholar] [CrossRef] [Green Version]
- Savineau, J.P.; Marthan, R.; Dumas De La Roque, E. Role of DHEA in cardiovascular diseases. Biochem. Pharmacol. 2013, 85, 718–726. [Google Scholar] [CrossRef]
- Wang, L.; Szklo, M.; Folsom, A.R.; Cook, N.R.; Gapstur, S.M.; Ouyang, P. Endogenous sex hormones, blood pressure change, and risk of hypertension in postmenopausal women: The Multi-Ethnic Study of Atherosclerosis. Atherosclerosis 2012, 224, 228–234. [Google Scholar] [CrossRef] [Green Version]
- Boxer, R.S.; Kleppinger, A.; Brindisi, J.; Feinn, R.; Burleson, J.A.; Kenny, A.M. Effects of dehydroepiandrosterone (DHEA) on cardiovascular risk factors in older women with frailty characteristics. Age Ageing 2010, 39, 451–458. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; He, Y.O.; Santos, H.; Sathian, B.; Price, J.C.; Diao, J. The effects of dehydroepiandrosterone (DHEA) supplementation on body composition and blood pressure: A meta-analysis of randomized clinical trials. Steroids 2020, 163, 108710. [Google Scholar] [CrossRef] [PubMed]
- Lehrer, H.M.; Dubois, S.K.; Maslowsky, J.; Laudenslager, M.L.; Steinhardt, M.A. Hair cortisol concentration and glycated hemoglobin in African American adults. Psychoneuroendocrinology 2016, 72, 212–218. [Google Scholar] [CrossRef]
- Wei, D.; Liu, X.; Huo, W.; Yu, S.; Li, L.; Wang, C.; Mao, Z. Serum cortisone and glucocorticoid receptor gene (NR3C1) polymorphism in human dysglycemia. Hormones 2020, 19, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Mazgelytė, E.; Karčiauskaitė, D.; Linkevičiūtė, A.; Mažeikienė, A.; Burokienė, N.; Matuzevičienė, R.; Radzevičius, M.; Janiulionienė, A.; Jakaitienė, A.; Dindienė, L.; et al. Association of hair cortisol concentration with prevalence of major cardiovascular risk factors and Allostatic load. Med. Sci. Monit. 2019, 25, 3573–3582. [Google Scholar] [CrossRef]
- Wester, V.L.; Noppe, G.; Savas, M.; van den Akker, E.L.T.; de Rijke, Y.B.; van Rossum, E.F.C. Hair analysis reveals subtle HPA axis suppression associated with use of local corticosteroids: The Lifelines cohort study. Psychoneuroendocrinology 2017, 80, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Vehmeijer, F.O.L.; Santos, S.; De Rijke, Y.B.; Van Den Akker, E.L.T.; Felix, J.F.; Van Rossum, E.F.C.; Jaddoe, V.W.V. Associations of Hair Cortisol Concentrations with Cardiometabolic Risk Factors in Childhood. J. Clin. Endocrinol. Metab. 2021, 106, E3400–E3413. [Google Scholar] [CrossRef] [PubMed]
- Genitsaridi, S.M.; Karampatsou, S.; Papageorgiou, I.; Mantzou, A.; Papathanasiou, C.; Kassari, P.; Paltoglou, G.; Kourkouti, C.; Charmandari, E. Hair Cortisol Concentrations in Overweight and Obese Children and Adolescents. Horm. Res. Paediatr. 2020, 92, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Marais, A.D. Apolipoprotein E in lipoprotein metabolism, health and cardiovascular disease. Pathology 2019, 51, 165–176. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.M.; Tronick, E.Z.; Moore, C.L. Relationship between hair cortisol and perceived chronic stress in a diverse sample. Stress Health 2013, 29, 337–344. [Google Scholar] [CrossRef] [Green Version]
- Qiao, S.; Li, X.; Zilioli, S.; Chen, Z.; Deng, H.; Pan, J.; Guo, W. Hair measurements of cortisol, DHEA, and DHEA to cortisol ratio as biomarkers of chronic stress among people living with HIV in China: Known-group validation. PLoS One 2017, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ling, J.; Xu, D.; Robbins, L.B.; Meyer, J.S. Does hair cortisol really reflect perceived stress? Findings from low-income mother-preschooler dyads. Psychoneuroendocrinology 2020, 111, 104478. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Dai, J.; Li, J. Mediating effects of hair cortisol on the mutual association of job burnout and insomnia: A retrospective exploratory study. J. Psychiatr. Res. 2019, 117, 62–67. [Google Scholar] [CrossRef]
- Greff, M.J.E.; Levine, J.M.; Abuzgaia, A.M.; Elzagallaai, A.A.; Rieder, M.J.; van Uum, S.H.M. Hair cortisol analysis: An update on methodological considerations and clinical applications. Clin. Biochem. 2019, 63, 1–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variable | Median (IQR) or n (%) |
|---|---|
| Age (years) | 55 (7) |
| Education | |
| Lower secondary | 3 (2.1%) |
| Upper secondary | 20 (13.8%) |
| Higher (university or non-university) | 122 (84.1%) |
| Marital status | |
| Married | 107 (73.8%) |
| Single/divorced/widowed | 38 (26.2%) |
| Smoking status | |
| Smoker | 16 (11.0%) |
| Non-smoker | 129 (89.0%) |
| Physical activity 1 | |
| Inactive (Score 2–3) | 87 (60.8%) |
| Active (Score 4–6) | 56 (39.2%) |
| Menopause 2 | |
| Yes | 118 (81.9%) |
| No | 26 (18.1%) |
| Physically traumatic events during the previous 3 months 2 | |
| Yes | 4 (2.8%) |
| No | 140 (97.2%) |
| Psychologically traumatic events during the previous 3 months 2 | |
| Yes | 32 (22.2%) |
| No | 112 (77.8%) |
| Hair washing frequency | |
| ≤1/week | 21 (14.5%) |
| 2–4/week | 95 (65.5%) |
| >5/week | 29 (20.0%) |
| Variable | Mean ± SD, Median (IQR) or n (%) | Range |
|---|---|---|
| PSS | 15.59 ± 5.86 | 0–30 |
| PSS category | ||
| 0–13 (low stress) | 52 (35.9%) | |
| 14–26 (moderate stress) | 88 (60.7%) | |
| 27–30 (high stress) | 5 (3.4%) | |
| PSQI 1 | 5 (5.25) | 1–17 |
| PSQI category 1 | ||
| <5 (good sleeper) | 83 (58.0%) | |
| ≥5 (poor sleeper) | 60 (42.0%) | |
| STAI-T | 40.30 ± 8.87 | 18–67 |
| STAI-T category | ||
| <32 (lower anxiety) | 28 (19.3%) | |
| ≥32 (higher anxiety) | 117 (80.7%) |
| Variable | Mean ± SD or Median (IQR) | Range |
|---|---|---|
| Weight (kg) | 74 (22) | 46–150 |
| Height (cm) | 165.40 ± 5.72 | 149–182 |
| BMI (kg/m2) | 26.81 (8.18) | 17.86–55.77 |
| Waist circumference (cm) | 85 (20) | 62–136 |
| SBP (mmHg) | 127 (21) | 89–180 |
| DBP (mmHg) | 80 ± 9.08 | 59–110 |
| HR (bpm) | 76 (15) | 53–135 |
| Glucose (mmol/L) | 5.39 (0.71) | 4.1–9.21 |
| Total cholesterol (mmol/L) | 5.78 (1.49) | 3.75–10.69 |
| HDL-cholesterol (mmol/L) | 1.64 (0.62) | 0.85–3.2 |
| LDL-cholesterol (mmol/L) | 3.52 (1.32) | 1.6–8.88 |
| Non-HDL-cholesterol (mmol/L) | 4.03 (1.54) | 2.07–9.47 |
| Remnant cholesterol (mmol/L) | 0.53 (0.34) | 0.24–1.84 |
| TAG (mmol/L) | 1.160 (0.74) | 0.52–4.01 |
| Apo B (g/L) 1 | 0.92 (0.37) | 0.093–1.85 |
| Apo A1 (g/L) 1 | 1.56 ± 0.26 | 0.86–2.49 |
| Apo A2 (g/L) 1 | 0.35 (0.065) | 0.22–0.57 |
| Apo E (mg/L) 1 | 44.70 (12.32) | 23.20–79.00 |
| Apo A1/Apo B 1 | 1.62 (0.72) | 0.62–17.31 |
| SCORE2 (%) | 8.00 (6.00) | 4.00–27.00 |
| Hair cortisol (ng/g) 2 | 3.43 (6.75) | 0.53–117.55 |
| Hair cortisone (ng/g) 2 | 6.65 (4.95) | 1.49–73.33 |
| Hair DHEA (ng/g) 3 | 3.97 (4.06) | 0.99–22.72 |
| Variable | Hair Cortisol (ng/g) (Median (IQR)) | p-Value 1 | Hair Cortisone (ng/g) (Median (IQR)) | p-Value 1 | Hair DHEA (ng/g) (Median (IQR)) | p-Value 1 |
|---|---|---|---|---|---|---|
| Menopause | ||||||
| Yes | 3.15 (6.91) | 0.657 | 6.73 (4.88) | 0.342 | 3.60 (3.84) | 0.515 |
| No | 3.62 (5.97) | 5.29 (5.24) | 4.63 (4.55) | |||
| Psychologically traumatic events | ||||||
| Yes | 3.7 (5.28) | 0.586 | 6.89 (4.26) | 0.543 | 4.07 (3.71) | 0.883 |
| No | 3.1 (6.92) | 6.43 (5.05) | 3.93 (4.16) | |||
| Hair washing frequency | ||||||
| ≤1/week | 2.62 (2.51) | 0.134 | 6.76 (5.12) | 0.966 | 5.04 (4.32) | 0.473 |
| 2–4/week | 3.69 (6.36) | 6.61 (4.23) | 3.47 (3.56) | |||
| >5/week | 4.06 (16.04) | 6.07 (5.86) | 4.68 (5.18) | |||
| Smoking status | ||||||
| Smoker | 3.58 (6.96) | 0.849 | 7.26 (5.05) | 0.257 | 4.07 (4.29) | 0.382 |
| Non-smoker | 3.10 (3.50) | 6.24 (3.42) | 3.02 (2.47) | |||
| Physical activity | ||||||
| Inactive | 3.66 (9.74) | 0.333 | 6.69 (5.73) | 0.362 | 3.58 (3.68) | 0.333 |
| Active | 3.58 (4.81) | 6.50 (4.07) | 4.23 (4.73) |
| Variable | Hair Cortisol (ng/g) | Hair Cortisone (ng/g) | Hair DHEA (ng/g) | |||
|---|---|---|---|---|---|---|
| Spearman’s r | p-Value 1 | Spearman’s r | p-Value 1 | Spearman’s r | p-Value 1 | |
| Age (years) | 0.125 | 0.134 | 0.143 | 0.087 | −0.039 | 0.651 |
| BMI (kg/m2) | 0.155 | 0.064 | 0.307 | 1.85 × 10−4 | 0.002 | 0.978 |
| WC (cm) | 0.170 | 0.042 | 0.344 | 2.38 × 10−5 | 0.012 | 0.886 |
| SBP (mmHg) | 0.246 | 0.003 | 0.271 | 1.03 × 10−3 | 0.194 | 0.024 |
| DBP (mmHg) | 0.227 | 0.006 | 0.276 | 7.98 × 10−4 | 0.197 | 0.022 |
| HR (bpm) | 0.0003 | 0.997 | 0.130 | 0.122 | 0.023 | 0.795 |
| Glucose (mmol/L) | 0.124 | 0.139 | 0.177 | 0.033 | 0.003 | 0.969 |
| Total cholesterol (mmol/L) | −0.069 | 0.411 | −0.127 | 0.129 | −0.090 | 0.299 |
| HDL-cholesterol (mmol/L) | −0.044 | 0.600 | −0.249 | 0.003 | −0.018 | 0.838 |
| LDL-cholesterol (mmol/L) | −0.010 | 0.234 | −0.107 | 0.201 | −0.078 | 0.366 |
| Non-HDL-cholesterol (mmol/L) | −0.079 | 0.344 | −0.080 | 0.339 | −0.110 | 0.205 |
| Remnant cholesterol (mmol/L) | 0.091 | 0.279 | 0.079 | 0.348 | −0.089 | 0.306 |
| TAG (mmol/L) | 0.090 | 0.283 | 0.077 | 0.356 | −0.082 | 0.343 |
| Apo B (g/L) | 0.098 | 0.300 | 0.070 | 0.462 | −0.019 | 0.845 |
| Apo A1 (g/L) | 0.049 | 0.607 | −0.158 | 0.093 | 0.030 | 0.762 |
| Apo A2 (g/L) | 0.054 | 0.571 | −0.126 | 0.180 | 0.018 | 0.857 |
| Apo E (mg/L) | 0.191 | 0.041 | 0.128 | 0.176 | 0.085 | 0.384 |
| Apo A1/Apo B | −0.024 | 0.803 | −0.102 | 0.279 | 0.027 | 0.781 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazgelytė, E.; Burokienė, N.; Vysocka, A.; Narkevičius, M.; Petrėnas, T.; Kaminskas, A.; Songailienė, J.; Utkus, A.; Karčiauskaitė, D. Higher Levels of Stress-Related Hair Steroid Hormones Are Associated with the Increased SCORE2 Risk Prediction Algorithm in Apparently Healthy Women. J. Cardiovasc. Dev. Dis. 2022, 9, 70. https://doi.org/10.3390/jcdd9030070
Mazgelytė E, Burokienė N, Vysocka A, Narkevičius M, Petrėnas T, Kaminskas A, Songailienė J, Utkus A, Karčiauskaitė D. Higher Levels of Stress-Related Hair Steroid Hormones Are Associated with the Increased SCORE2 Risk Prediction Algorithm in Apparently Healthy Women. Journal of Cardiovascular Development and Disease. 2022; 9(3):70. https://doi.org/10.3390/jcdd9030070
Chicago/Turabian StyleMazgelytė, Eglė, Neringa Burokienė, Agata Vysocka, Martynas Narkevičius, Tomas Petrėnas, Andrius Kaminskas, Jurgita Songailienė, Algirdas Utkus, and Dovilė Karčiauskaitė. 2022. "Higher Levels of Stress-Related Hair Steroid Hormones Are Associated with the Increased SCORE2 Risk Prediction Algorithm in Apparently Healthy Women" Journal of Cardiovascular Development and Disease 9, no. 3: 70. https://doi.org/10.3390/jcdd9030070
APA StyleMazgelytė, E., Burokienė, N., Vysocka, A., Narkevičius, M., Petrėnas, T., Kaminskas, A., Songailienė, J., Utkus, A., & Karčiauskaitė, D. (2022). Higher Levels of Stress-Related Hair Steroid Hormones Are Associated with the Increased SCORE2 Risk Prediction Algorithm in Apparently Healthy Women. Journal of Cardiovascular Development and Disease, 9(3), 70. https://doi.org/10.3390/jcdd9030070