The Clinical Spectrum of Kommerell’s Diverticulum in Adults with a Right-Sided Aortic Arch: A Case Series and Literature Overview


 ,
, 
 and
and
Abstract
1. Introduction: From Embryology to Clinical Presentation
2. Case Presentation
2.1. Patient 1
2.2. Patient 2
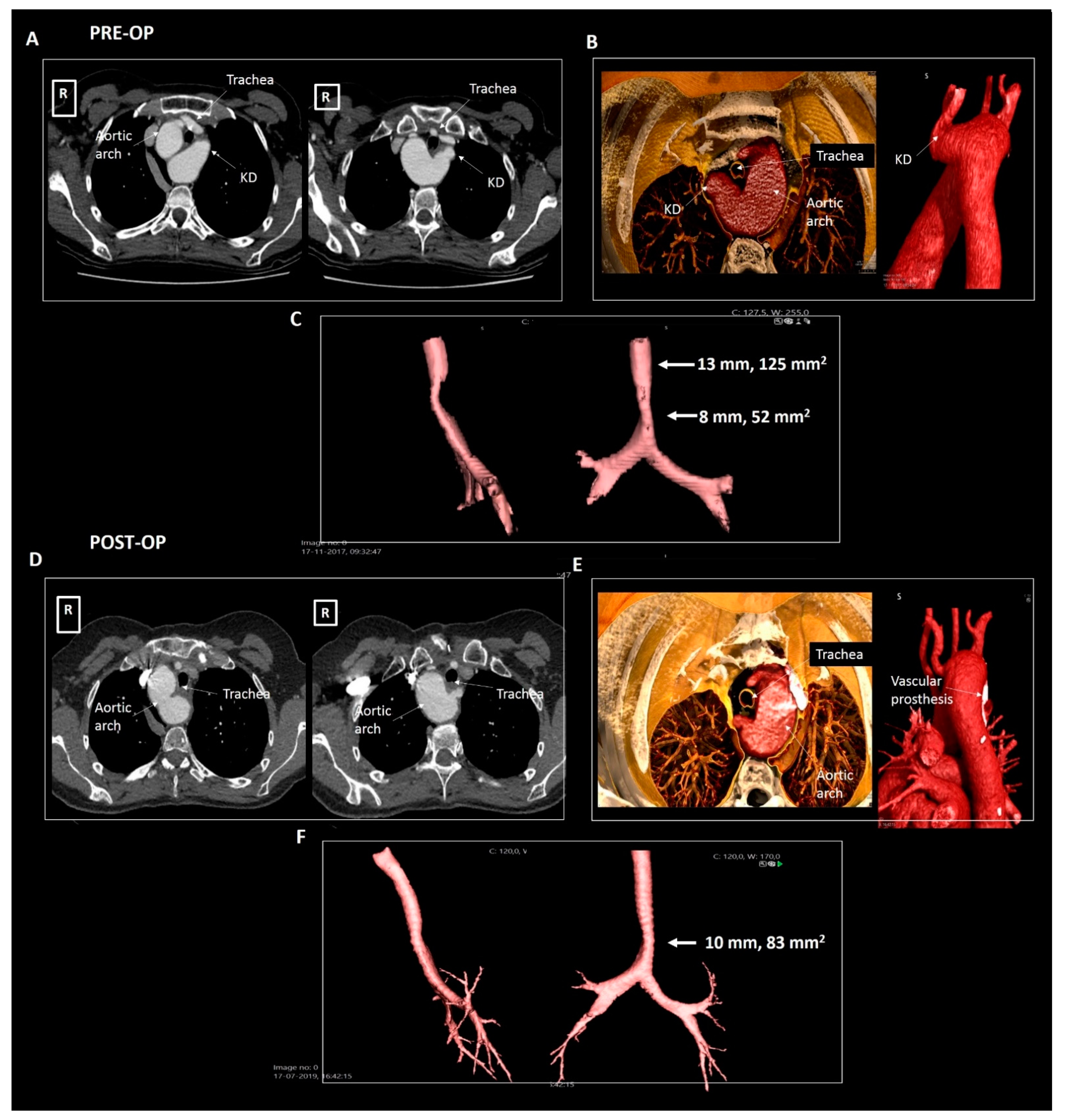
2.3. Patient 3
2.4. Patient 4
2.5. Patient 5
2.6. Patient 6
2.7. Patient 7
3. Discussion: Clinical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Bogerijen, G.H.; van Bogerijen, G.H.; Patel, H.J.; Eliason, J.L.; Criado, E.; Williams, D.M.; Knepper, J.; Yang, B.; Deeb, G.M. Evolution in the Management of Aberrant Subclavian Arteries and Related Kommerell Diverticulum. Ann. Thorac. Surg. 2015, 100, 47–53. [Google Scholar] [CrossRef]
- Kommerell, B. Verlagerung des osophagus durch eine abnorm verlaufende arteria subclavia dextra (arteria lusoria). Fortschr Roentgenstrahlen 1936, 54, 590–595. [Google Scholar]
- Tanaka, A.; Milner, R.; Ota, T. Kommerell’s diverticulum in the current era: A comprehensive review. Gen. Thorac. Cardiovasc. Surg. 2015, 63, 245–259. [Google Scholar] [CrossRef] [PubMed]
- Backer, C.L.; Bharadwaj, S.N.; Eltayeb, O.M.; Forbess, J.M.; Popescu, A.R.; Mongé, M.C. Double Aortic Arch With Kommerell Diverticulum. Ann. Thorac. Surg. 2019, 108, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Shu, C.; Li, M.; Li, Q.; Kopp, R. Aberrant Subclavian Artery Pathologies and Kommerell’s Diverticulum: A Review and Analysis of Published Endovascular/Hybrid Treatment Options. J. Endovasc. Ther. 2012, 19, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Hanneman, K.; Newman, B.; Chan, F. Congenital Variants and Anomalies of the Aortic Arch. Radiographics 2017, 37, 32–51. [Google Scholar] [CrossRef] [PubMed]
- Erben, Y.; Brownstein, A.J.; Velasquez, C.A.; Li, Y.; Rizzo, J.A.; Mojibian, H.; Tanweer, M.; Zafar, M.A.; Ziganshin, B.A.; Elefteriades, J.A. Natural history and management of Kommerell’s diverticulum in a single tertiary referral center. J. Vasc. Surg. 2020, 71, 2004–2011. [Google Scholar] [CrossRef] [PubMed]
- Poterucha, J.; Anavekar, N.; Niaz, T.; Agarwal, A.; Young, P.; Dearani, J.; Ammash, N.; Warnes, C.; Connolly, H. Incidence and clinical presentation of kommerell diverticulum and aneurysm. J. Am. Coll. Cardiol. 2015, 65, A524. [Google Scholar] [CrossRef]
- Stewart, J.R.; Kindcaid, O.W.; Edwards, J.E. An Atlas of Vascular Rings and Related Malformations of the Aortic Arch System; Thomas: Springfield, IL, USA, 1964. [Google Scholar]
- Gittenberger-de Groot, A.C.; Azhar, M.; Molin, D.G. Transforming growth factor beta-SMAD2 signaling and aortic arch development. Trends Cardiovasc. Med. 2006, 16, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Molin, D.G.; DeRuiter, M.C.; Wisse, L.J.; Azhar, M.; Doetschman, T.; Poelmann, R.E.; Gittenberger-de Groot, A.C. Altered apoptosis pattern during pharyngeal arch artery remodelling is associated with aortic arch malformations in Tgfbeta2 knock-out mice. Cardiovasc. Res. 2002, 56, 312–322. [Google Scholar] [CrossRef]
- Molin, D.G.; Roest, P.A.; Nordstrand, H.; Wisse, L.J.; Poelmann, R.E.; Eriksson, U.J.; Gittenberger-De Groot, A.C. Disturbed morphogenesis of cardiac outflow tract and increased rate of aortic arch anomalies in the offspring of diabetic rats. Birth Defects Res. A Clin. Mol. Teratol. 2004, 70, 927–938. [Google Scholar] [CrossRef] [PubMed]
- Bergwerff, M.; DeRuiter, M.C.; Hall, S.; Poelmann, R.E.; Groot, A.C.G.-D. Unique vascular morphology of the fourth aortic arches: Possible implications for pathogenesis of type-B aortic arch interruption and anomalous right subclavian artery. Cardiovasc. Res. 1999, 44, 185–196. [Google Scholar] [CrossRef]
- Ernst, A.; Feller-Kopman, D.; Becker, H.D.; Mehta, A.C. Central Airway Obstruction. Am. J. Respir. Crit. Care Med. 2004, 169, 1278–1297. [Google Scholar] [CrossRef] [PubMed]
- Cinà, C.; Althani, H.; Pasenau, J.; Abouzahr, L. Kommerell’s diverticulum and right-sided aortic arch: A cohort study and review of the literature. J. Vasc. Surg. 2004, 39, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Cambria, R.P.; Isselbacher, E.M.; Baker, J.N.; Lamuraglia, G.M.; Stone, J.R.; MacGillivray, T.E. Contemporary Surgical Approaches and Outcomes in Adults With Kommerell Diverticulum. Ann. Thorac. Surg. 2014, 98, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Ota, T.; Okada, K.; Takanashi, S.; Yamamoto, S.; Okita, Y. Surgical treatment for Kommerell’s diverticulum. J. Thorac. Cardiovasc. Surg. 2006, 131, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Idrees, J.; Keshavamurthy, S.; Subramanian, S.; Clair, D.G.; Svensson, L.G.; Roselli, E.E. Hybrid repair of Kommerell diverticulum. J. Thorac. Cardiovasc. Surg. 2014, 147, 973–976. [Google Scholar] [CrossRef] [PubMed]
- Backer, C.L.; Russell, H.M.; Wurlitzer, K.C.; Rastatter, J.C.; Rigsby, C.K. Primary Resection of Kommerell Diverticulum and Left Subclavian Artery Transfer. Ann. Thorac. Surg. 2012, 94, 1612–1617. [Google Scholar] [CrossRef] [PubMed]
- Vinnakota, A.; Idrees, J.J.; Rosinski, B.F.; Tucker, N.J.; Roselli, E.E.; Pettersson, G.B.; Vekstein, A.M.; Stewart, R.D.; Raja, S.; Svensson, L.G. Outcomes of Repair of Kommerell Diverticulum. Ann. Thorac. Surg. 2019, 108, 1745–1750. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age at Diagnosis (Years) | Gender | Anatomy | Compression | Dimensions of KD | Symptoms | Management | |
|---|---|---|---|---|---|---|---|
| Patient 1 | 40 | Male | Right-sided arch, aberrant LSA and KD | Mild tracheal compression | 22 × 20 mm, 319 mm2 | Incidental finding | Structural imaging follow-up |
| Patient 2 | 40 | Male | Right-sided arch, aberrant LSA and KD | Partial tracheal compression | 22 × 21 mm, 357 mm2 | Incidental finding | Structural imaging follow-up |
| Patient 3 | 50 | Female | Right-sided arch, aberrant LSA and KD | Symptomatic tracheal and esophageal compression | 30 × 29 mm, 870 mm2 | Dysphagia and dyspnea | Surgical resection |
| Patient 4 | 55 | Male | Right-sided arch, aberrant LSA and KD | Mild tracheal compression | 25 × 23 mm, 575 mm2 | Mild dyspnea, although excellent objective exercise capacity | Structural imaging follow-up |
| Patient 5 | 63 | Male | Right-sided arch, aberrant LSA and KD | Asymptomatic esophageal compression | 24 × 19 mm, 343 mm2 | Incidental finding | Structural imaging follow-up |
| Patient 6 | 23 | Male | Right-sided arch, mirror imaging branching and KD | Mild tracheal and esophageal compression | 27 × 21 mm, 440 mm2 | Dyspnea, although excellent objective exercise capacity | Structural imaging follow-up |
| Patient 7 | 25 | Female | Right-sided arch, aberrant LSA and KD | Mild tracheal and esophageal compression | 19 × 21 mm, 399 mm2 | Incidental finding | Structural imaging follow-up |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Rosendael, P.J.; Stöger, J.L.; Kiès, P.; Vliegen, H.W.; Hazekamp, M.G.; Koolbergen, D.R.; Lamb, H.J.; Jongbloed, M.R.M.; Egorova, A.D. The Clinical Spectrum of Kommerell’s Diverticulum in Adults with a Right-Sided Aortic Arch: A Case Series and Literature Overview. J. Cardiovasc. Dev. Dis. 2021, 8, 25. https://doi.org/10.3390/jcdd8030025
van Rosendael PJ, Stöger JL, Kiès P, Vliegen HW, Hazekamp MG, Koolbergen DR, Lamb HJ, Jongbloed MRM, Egorova AD. The Clinical Spectrum of Kommerell’s Diverticulum in Adults with a Right-Sided Aortic Arch: A Case Series and Literature Overview. Journal of Cardiovascular Development and Disease. 2021; 8(3):25. https://doi.org/10.3390/jcdd8030025
Chicago/Turabian Stylevan Rosendael, Philippe J., J. Lauran Stöger, Philippine Kiès, Hubert W. Vliegen, Mark G. Hazekamp, David R. Koolbergen, Hildo J. Lamb, Monique R. M. Jongbloed, and Anastasia D. Egorova. 2021. "The Clinical Spectrum of Kommerell’s Diverticulum in Adults with a Right-Sided Aortic Arch: A Case Series and Literature Overview" Journal of Cardiovascular Development and Disease 8, no. 3: 25. https://doi.org/10.3390/jcdd8030025
APA Stylevan Rosendael, P. J., Stöger, J. L., Kiès, P., Vliegen, H. W., Hazekamp, M. G., Koolbergen, D. R., Lamb, H. J., Jongbloed, M. R. M., & Egorova, A. D. (2021). The Clinical Spectrum of Kommerell’s Diverticulum in Adults with a Right-Sided Aortic Arch: A Case Series and Literature Overview. Journal of Cardiovascular Development and Disease, 8(3), 25. https://doi.org/10.3390/jcdd8030025