

A Sphincter-like Function of Pulmonary Vein Ostia in Normal and Atrial Fibrillation Subjects

Abstract
1. Introduction
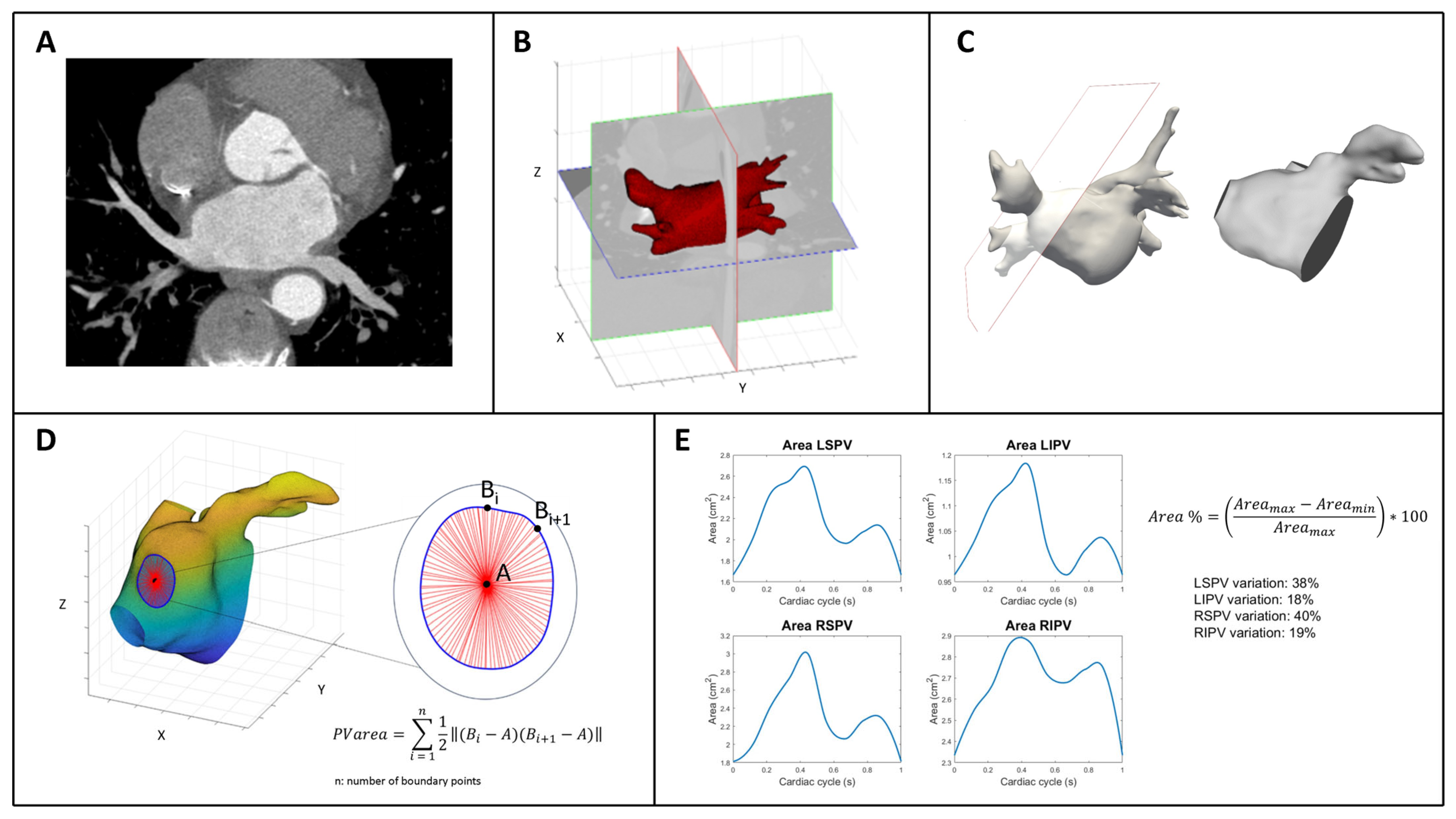
2. Methods
Statistical Analysis
3. Results
4. Discussion
4.1. Pathophysiological Considerations
4.2. Clinical Implications
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Lloyd-Jones, D.M.; Wang, T.J.; Leip, E.P.; Larson, M.G.; Levy, D.; Vasan, R.S.; D’agostino, R.B.; Massaro, J.M.; Beiser, A.; Wolf, P.A.; et al. Lifetime risk for development of atrial fibrillation: The Framingham Heart Study. Circulation 2004, 110, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- Heeringa, J.; Van Der Kuip, D.A.M.; Hofman, A.; Kors, J.A.; Van Herpen, G.; Stricker, B.H.C.; Stijnen, T.; Lip, G.Y.H.; Witteman, J.C.M. Prevalence, incidence and lifetime risk of atrial fibrillation: The Rotterdam study. Eur. Heart J. 2006, 27, 949–953. [Google Scholar] [CrossRef] [PubMed]
- Vinter, N.; Cordsen, P.; Johnsen, S.P.; Staerk, L.; Benjamin, E.J.; Frost, L.; Trinquart, L. Temporal trends in lifetime risks of atrial fibrillation and its complications between 2000 and 2022: Danish, nationwide, population based cohort study. BMJ 2024, 385, e077209. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jaïs, P.; Haïssaguerre, M.; Shah, D.C.; Chouairi, S.; Gencel, L.; Hocini, M.; Clémenty, J. A focal source of atrial fibrillation treated by discrete radiofrequency ablation. Circulation 1997, 95, 572–576. [Google Scholar] [CrossRef] [PubMed]
- Haïssaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.L.; Tajik, A.J. Doppler assessment of pulmonary venous flow in healthy subjects and in patients with heart disease. J. Am. Soc. Echocardiogr. 1991, 4, 379–392. [Google Scholar] [CrossRef] [PubMed]
- Nathan, H.; Eliakim, M. The junction between the left atrium and the pulmonary veins. An anatomic study of human hearts. Circulation 1966, 34, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Gurfinkel’, V.S.; Kapuller, L.L.; Shik, M.L. Sphincters of the pulmonary veins in man, and their significance. Bull. Exp. Biol. Med. 1961, 51, 651–653. [Google Scholar] [CrossRef]
- Ho, S.Y.; Cabrera, J.A.; Tran, V.H.; Farré, J.; Anderson, R.H.; Sánchez-Quintana, D. Architecture of the pulmonary veins: Relevance to radiofrequency ablation. Heart Br. Card. Soc. 2001, 86, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Unser, M. Splines: A perfect fit for signal and image processing. IEEE Signal Process. Mag. 1999, 16, 22–38. [Google Scholar] [CrossRef]
- Masci, A.; Alessandrini, M.; Forti, D.; Menghini, F.; Dedé, L.; Tomasi, C.; Quarteroni, A.; Corsi, C. A Proof of Concept for Computational Fluid Dynamic Analysis of the Left Atrium in Atrial Fibrillation on a Patient-Specific Basis. J. Biomech. Eng. 2020, 142, 011002. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.Y.; Li, H.; Wachsmann-Hogiu, S.; Chen, L.S.; Chen, P.S.; Fishbein, M.C. Autonomic innervation and segmental muscular disconnections at the human pulmonary vein-atrial junction: Implications for catheter ablation of atrial-pulmonary vein junction. J. Am. Coll. Cardiol. 2006, 48, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Thiagalingam, A.; Reddy, V.Y.; Cury, R.C.; Abbara, S.; Holmvang, G.; Thangaroopan, M.; Ruskin, J.N.; d’Avila, A. Pulmonary vein contraction: Characterization of dynamic changes in pulmonary vein morphology using multiphase multislice computed tomography scanning. Heart Rhythm. 2008, 5, 1645–1650. [Google Scholar] [CrossRef] [PubMed]
- Cronin, P.; Kelly, A.M.; Desjardins, B.; Patel, S.; Gross, B.H.; Kazerooni, E.A.; Morady, F.; Oral, H.; Carlos, R.C. Normative Analysis of pulmonary vein drainage patterns on multidetector CT with measurements of pulmonary vein ostial diameter and distance to first bifurcation. Acad. Radiol. 2007, 14, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Hirsh, B.J.; Copeland-Halperin, R.S.; Halperin, J.L. Fibrotic atrial cardiomyopathy, atrial fibrillation, and thromboembolism: Mechanistic links and clinical inferences. J. Am. Coll. Cardiol. 2015, 65, 2239–2251. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| LSPVs | RSPVs | RIPVs | LIPVs | p -Value | |
|---|---|---|---|---|---|
| PV Area changes (%) | |||||
| Normal | 33.1 ± 12.3 | 38.7 ± 14.6 | 20.3 ± 10.8 | 24.5 ± 10.3 | 0.007 |
| Paroxysmal AF | 19.4 ± 8.3 | 26.1 ± 8.4 | 13.6 ± 8.2 | 12.5 ± 5.3 | 0.0003 |
| Persistent AF | 16.0 ± 5.4 | 20.8 ± 10.3 | 12.3 ± 5.8 | 12.6 ± 7.0 | 0.04 |
| Normal Subjects | Paroxysmal AF | Persistent AF | p-Value | |
| PV ostia area (cm2) | ||||
| LSPVs | 2.20 ± 0.59 | 2.19 ± 0.51 | 2.38 ± 1.02 | 0.75 |
| RSPVs | 3.20 ± 1.04 | 3.27 ± 1.06 | 3.58 ± 1.03 | 0.61 |
| RIPVs | 2.25 ± 0.60 | 2.42 ± 0.85 | 2.22 ± 0.63 | 0.71 |
| LIPVs | 1.50 ± 0.4 | 1.75 ± 0.06 | 2.06 ± 0.68 | 0.044 |
| PV area changes (%) | ||||
| LSPVs | 33.1 ± 12.3 | 19.4 ± 8.3 | 16.0 ± 5.4 | <0.001 |
| RSPVs | 38.7 ± 14.6 | 26.1 ± 8.4 | 20.8 ± 10.3 | <0.001 |
| RIPVs | 20.3 ± 10.8 | 13.6 ± 8.2 | 12.3 ± 5.8 | 0.037 |
| LIPVs | 24.5 ± 10.3 | 12.5 ± 5.3 | 12.6 ± 7.0 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonapace, S.; Falanga, M.; Cicciò, C.; Corsi, C.; Molon, G. A Sphincter-like Function of Pulmonary Vein Ostia in Normal and Atrial Fibrillation Subjects. J. Cardiovasc. Dev. Dis. 2025, 12, 203. https://doi.org/10.3390/jcdd12060203
Bonapace S, Falanga M, Cicciò C, Corsi C, Molon G. A Sphincter-like Function of Pulmonary Vein Ostia in Normal and Atrial Fibrillation Subjects. Journal of Cardiovascular Development and Disease. 2025; 12(6):203. https://doi.org/10.3390/jcdd12060203
Chicago/Turabian StyleBonapace, Stefano, Matteo Falanga, Carmelo Cicciò, Cristiana Corsi, and Giulio Molon. 2025. "A Sphincter-like Function of Pulmonary Vein Ostia in Normal and Atrial Fibrillation Subjects" Journal of Cardiovascular Development and Disease 12, no. 6: 203. https://doi.org/10.3390/jcdd12060203
APA StyleBonapace, S., Falanga, M., Cicciò, C., Corsi, C., & Molon, G. (2025). A Sphincter-like Function of Pulmonary Vein Ostia in Normal and Atrial Fibrillation Subjects. Journal of Cardiovascular Development and Disease, 12(6), 203. https://doi.org/10.3390/jcdd12060203