
Remote Heart Failure Patients Telemonitoring: Results of the TreC Heart Failure Study

 ,
,  , , , and
, , , and
Abstract
1. Introduction
Aims
2. Methods
2.1. TreC Cardiology Application
2.2. Study Population
2.3. Statistical Analysis
3. Results
3.1. Study Population
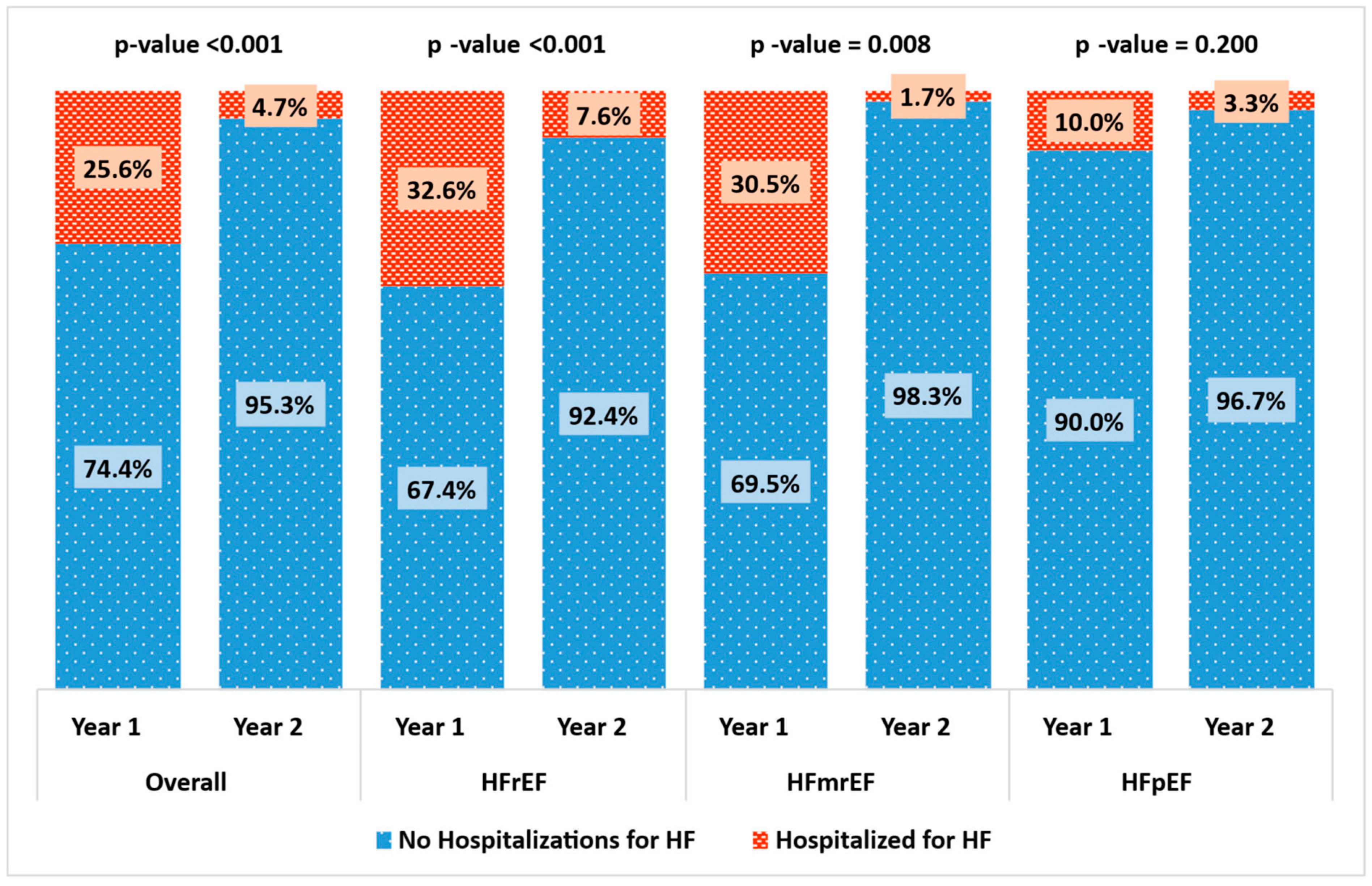
3.2. Primary Outcome
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, 1757–1780. [Google Scholar] [CrossRef] [PubMed]
- Dunlay, S.M.; Redfield, M.M.; Weston, S.A.; Therneau, T.M.; Hall Long, K.; Shah, N.D.; Roger, V.L. Hospitalizations after heart failure diagnosis a community perspective. J. Am. Coll. Cardiol. 2009, 54, 1695–1702. [Google Scholar] [CrossRef] [PubMed]
- Chun, S.; Tu, J.V.; Wijeysundera, H.C.; Austin, P.C.; Wang, X.; Levy, D.; Lee, D.S. Lifetime analysis of hospitalizations and survival of patients newly admitted with heart failure. Circ. Heart Fail. 2012, 5, 414–421. [Google Scholar] [CrossRef]
- Roger, V.L. Epidemiology of heart failure. Circ. Res. 2013, 113, 646–659. [Google Scholar] [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Conrad, N.; Judge, A.; Tran, J.; Mohseni, H.; Hedgecott, D.; Crespillo, A.P.; Allison, M.; Hemingway, H.; Cleland, J.G.; McMurray, J.J.V.; et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet 2018, 391, 572–580. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Polsinelli, V.B.; Sun, J.L.; Greene, S.J.; Chiswell, K.; Grunwald, G.K.; Allen, L.A.; Peterson, P.; Pandey, A.; Fonarow, G.C.; Heidenreich, P.; et al. Hospital Heart Failure Medical Therapy Score and Associated Clinical Outcomes and Costs. JAMA Cardiol. 2024, 9, 1029–1038. [Google Scholar] [CrossRef]
- Cleland, J.G.F.; Clark, R.A.; Pellicori, P.; Inglis, S.C. Caring for people with heart failure and many other medical problems through and beyond the COVID-19 pandemic: The advantages of universal access to home telemonitoring. Eur. J. Heart Fail. 2020, 22, 995–998. [Google Scholar] [CrossRef] [PubMed]
- Galinier, M.; Roubille, F.; Berdague, P.; Brierre, G.; Cantie, P.; Dary, P.; Ferradou, J.M.; Fondard, O.; Labarre, J.P.; Mansourati, J.; et al. Telemonitoring versus standard care in heart failure: A randomised multicentre trial. Eur. J. Heart Fail. 2020, 22, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Inglis, S.C.; Clark, R.A.; Dierckx, R.; Prieto-Merino, D.; Cleland, J.G. Structured telephone support or non-invasive telemonitoring for patients with heart failure. Heart 2017, 103, 255–257. [Google Scholar] [CrossRef]
- Radhoe, S.P.; Veenis, J.F.; Brugts, J.J. Invasive Devices and Sensors for Remote Care of Heart Failure Patients. Sensors 2021, 21, 2014. [Google Scholar] [CrossRef]
- Dierckx, R.; Inglis, S.C.; Clark, R.A.; Prieto-Merino, D.; Cleland, J.G. Telemedicine in heart failure: New insights from the Cochrane meta-analyses. Eur. J. Heart Fail. 2017, 19, 304–306. [Google Scholar] [CrossRef]
- Scholte, N.T.B.; Gürgöze, M.T.; Aydin, D.; Theuns, D.A.M.J.; Manintveld, O.C.; Ronner, E.; Boersma, E.; de Boer, R.A.; van der Boon, R.M.A.; Brugts, J.J. Telemonitoring for heart failure: A meta-analysis. Eur. Heart J. 2023, 44, 2911–2926. [Google Scholar] [CrossRef]
- Roubille, F.; Mercier, G.; Lancman, G.; Pasche, H.; Alami, S.; Delval, C.; Bessou, A.; Vadel, J.; Rey, A.; Duret, S.; et al. Weight telemonitoring of heart failure versus standard of care in a real-world setting: Results on mortality and hospitalizations in a 6-month nationwide matched cohort study. Eur. J. Heart Fail. 2024, 26, 1201–1214. [Google Scholar] [CrossRef]
- Survey on Heart Failure in Italian Hospital Cardiology Units. Results of the SEOSI study. SEOSI Investigators. Eur. Heart J. 1997, 18, 1457–1464. [Google Scholar] [CrossRef]
- Maggioni, A.P.; Orso, F.; Calabria, S.; Rossi, E.; Cinconze, E.; Baldasseroni, S.; Martini, N.; Observatory, A. The real-world evidence of heart failure: Findings from 41,413 patients of the ARNO database. Eur. J. Heart Fail. 2016, 18, 402–410. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Committee, A.S.A. The Acute Decompensated Heart Failure National Registry (ADHERE): Opportunities to improve care of patients hospitalized with acute decompensated heart failure. Rev. Cardiovasc. Med. 2003, 4 (Suppl. S7), S21–S30. [Google Scholar]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2023, 44, 3627–3639. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Davison, B.; Chioncel, O.; Cohen-Solal, A.; Diaz, R.; Filippatos, G.; Metra, M.; Ponikowski, P.; Sliwa, K.; Voors, A.A.; et al. Safety, tolerability and efficacy of up-titration of guideline-directed medical therapies for acute heart failure (STRONG-HF): A multinational, open-label, randomised, trial. Lancet 2022, 400, 1938–1952. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Study Population | |
|---|---|
| N | 211 |
| Age, years | 71.5 ± 12.6 |
| Male sex, % | 70.1% |
| Etiology, % | |
| Ischemic heart disease | 32.2% |
| Dilated cardiomyopathy | 35.1% |
| Valvular heart disease | 15.2% |
| Hypertensive heart disease | 8.5% |
| Other | 9.0% |
| Heart failure, % | |
| HFrEF | 43.6% |
| HFmrEF | 28.0% |
| HFpEF | 28.4% |
| LV-EF, % | 43.2 ± 11.9 |
| LGE, % | 74.6% |
| NYHA class, % | |
| I | 28.9% |
| II | 56.9% |
| III | 13.7% |
| IV | 0.5% |
| Atrial fibrillation, % | 42.2% |
| Paroxysmal | 17.5% |
| Persistent | 7.6% |
| Permanent | 17.5% |
| Diabetes mellitus, % | 26.1% |
| Device, % | |
| Pacemaker | 12.8% |
| ICD | 38.9% |
| CRT | 26.1% |
| Laboratory | |
| Hemoglobin, g/dL | 13.5 ± 1.8 |
| Creatinine, mg/dL, | 1.2 ± 0.5 |
| Potassium, mg/dL | 4.5 ± 0.5 |
| NT-proBNP, pg/mL * | 1783 (530–4180) |
| TreC chat utilization, % | 51.7% |
| TreC data entry, % | 81.0% |
| N° data entry/month | 5.1 ± 6.8 |
| Therapy | Year Pre-TreC | Year Post-TreC | p-Value |
|---|---|---|---|
| BB | 84.4% | 88.0% | 0.026 |
| ACEi | 39.8% | 30.2% | 0.003 |
| ARB | 13.7% | 16.7% | 0.088 |
| ARNI | 26.5% | 35.9% | <0.001 |
| MRA | 64.9% | 70.3% | 0.022 |
| SGLT2i | 26.1% | 35.9% | 0.001 |
| Furosemide | 66.4% | 59.9% | 0.009 |
| OMT in HFrEF | 34.4% | 55.1% | <0.001 |
| Outpatient Visits | Hospital Admission for HF | |||||
|---|---|---|---|---|---|---|
| Year Pre-TreC | Year Post-TreC | p-Value | Year Pre-TreC | Year Post-TreC | p-Value | |
| Study population | 2.0 ± 1.2 | 1.6 ± 1.3 | 0.002 | 25.6% | 4.7% | <0.001 |
| HFrEF population | 2.1 ± 1.4 | 2.1 ± 1.3 | 0.795 | 32.6% | 7.6% | <0.001 |
| HFmrEF population | 2.0 ± 1.0 | 1.5 ± 1.3 | 0.025 | 30.5% | 1.7% | 0.008 |
| HFpEF population | 2.0 ± 1.1 | 1.0 ± 0.8 | <0.001 | 10.0% | 3.3% | 0.200 |
| HF Hospital Admissions OR (95% CI) | p-Value | Outpatient Visits IRR (95% CI) | p-Value | |
|---|---|---|---|---|
| TreC introduction | 0.08 (0.04–0.19) | <0.001 | 0.81 (0.71–0.92) | 0.002 |
| Age | 1.01 (0.98–1.04) | 0.623 | 0.99 (0.99–1.00) | 0.039 |
| Female sex | 0.82 (0.35–1.93) | 0.650 | 1.11 (0.07–1.27) | 0.130 |
| Monthly reports | 0.98 (0.92–1.04) | 0.424 | 1.01 (1.00–1.01) | 0.217 |
| TreC chat utilization | 1.08 (0.52–2.23) | 0.840 | 0.99 (0.87–1.12) | 0.845 |
| NYHA class | 5.25 (3.06–8.99) | <0.001 | 1.12 (1.02–1.23) | 0.015 |
| LV-EF | 0.95 (0.92–0.98) | 0.001 | 0.99 (0.98–0.99) | <0.001 |
| Atrial fibrillation | 2.30 (1.16–4.58) | 0.017 | 1.18 (1.04–1.33) | 0.011 |
| PM | 1.25 (0.46–3.41) | 0.659 | 1.01 (0.85–1.19) | 0.950 |
| CRT | 0.40 (0.17–0.95) | 0.037 | 1.16 (1.02–1.32) | 0.020 |
| Diabetes mellitus | 2.31 (1.12–4.74) | 0.023 | 1.01 (0.88–1.16) | 0.884 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maines, M.; Benini, A.; Vinci, A.; Manica, A.; Erbogasto, E.; Tomasi, G.; Poian, L.; Martinelli, L.; Gios, L.; Forti, S.; et al. Remote Heart Failure Patients Telemonitoring: Results of the TreC Heart Failure Study. J. Cardiovasc. Dev. Dis. 2025, 12, 182. https://doi.org/10.3390/jcdd12050182
Maines M, Benini A, Vinci A, Manica A, Erbogasto E, Tomasi G, Poian L, Martinelli L, Gios L, Forti S, et al. Remote Heart Failure Patients Telemonitoring: Results of the TreC Heart Failure Study. Journal of Cardiovascular Development and Disease. 2025; 12(5):182. https://doi.org/10.3390/jcdd12050182
Chicago/Turabian StyleMaines, Massimiliano, Annachiara Benini, Annalisa Vinci, Anna Manica, Elisa Erbogasto, Giancarlo Tomasi, Luisa Poian, Luigi Martinelli, Lorenzo Gios, Stefano Forti, and et al. 2025. "Remote Heart Failure Patients Telemonitoring: Results of the TreC Heart Failure Study" Journal of Cardiovascular Development and Disease 12, no. 5: 182. https://doi.org/10.3390/jcdd12050182
APA StyleMaines, M., Benini, A., Vinci, A., Manica, A., Erbogasto, E., Tomasi, G., Poian, L., Martinelli, L., Gios, L., Forti, S., Patil, L., Mantovani, W., & Del Greco, M. (2025). Remote Heart Failure Patients Telemonitoring: Results of the TreC Heart Failure Study. Journal of Cardiovascular Development and Disease, 12(5), 182. https://doi.org/10.3390/jcdd12050182