
Vectorcardiography in CRT: What We Know and What There Is to Learn
 , , , and
, , , and
Abstract
1. Introduction
2. Limitations of Standard 12-Lead ECG
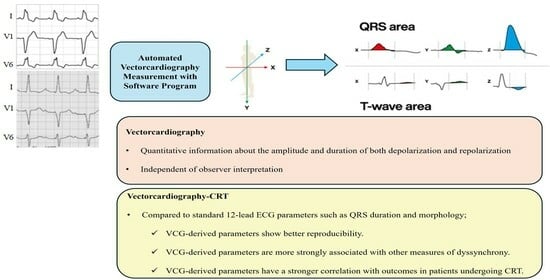
3. Vectorcardiographic QRS Area and CRT
4. Vectorcardiographic T-Wave Area and CRT Response
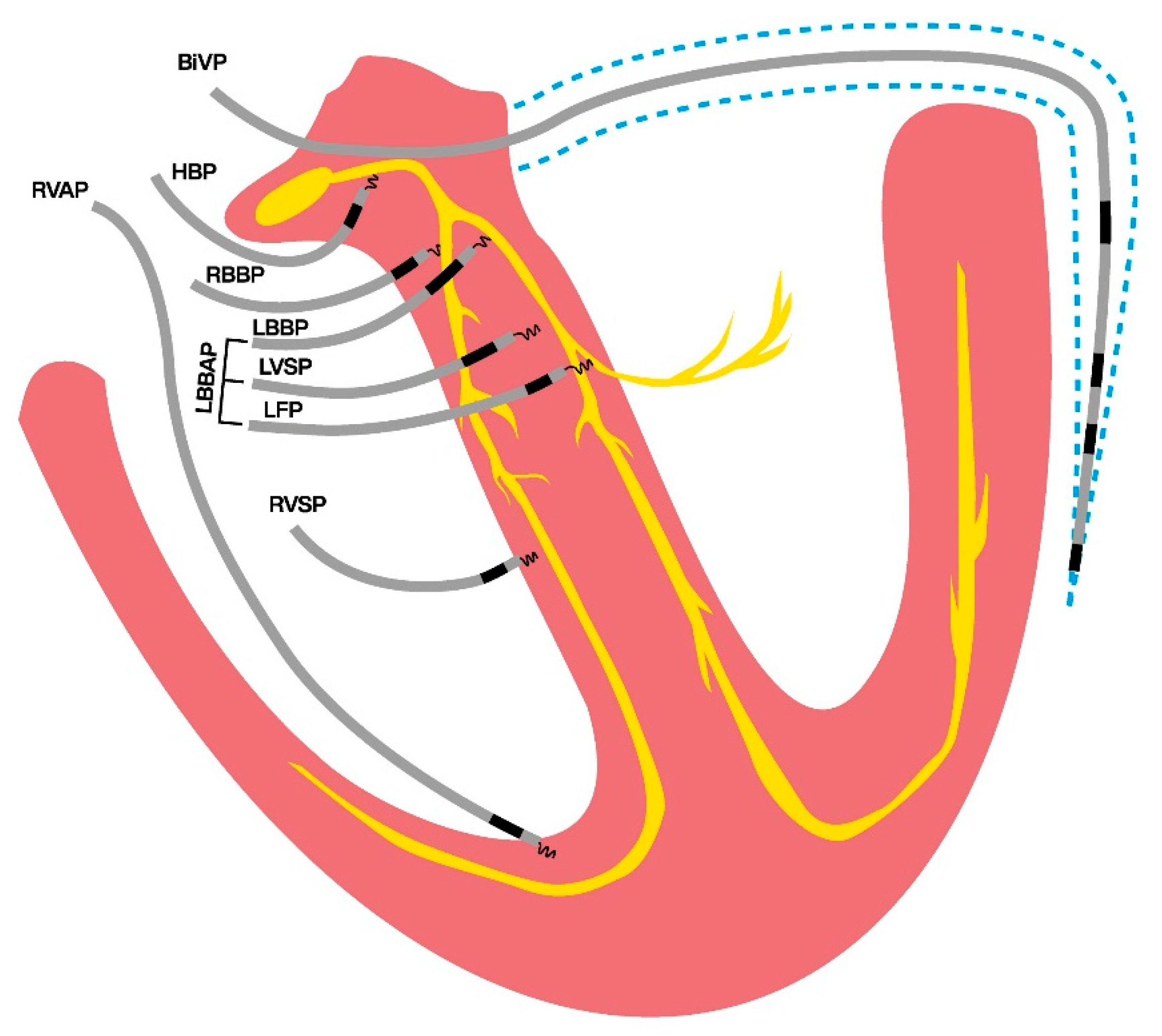
5. Vectorcardiography in Conduction System Pacing
6. Clinical Implications and Future Perspectives
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Cleland, J.G.; Daubert, J.C.; Erdmann, E.; Freemantle, N.; Gras, D.; Kappenberger, L.; Tavazzi, L. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N. Engl. J. Med. 2005, 352, 1539–1549. [Google Scholar] [CrossRef] [PubMed]
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Klein, H.; Brown, M.W.; Daubert, J.P.; Estes, N.A., 3rd; Foster, E.; Greenberg, H.; Higgins, S.L.; et al. Cardiac-resynchronization therapy for the prevention of heart-failure events. N. Engl. J. Med. 2009, 361, 1329–1338. [Google Scholar] [CrossRef]
- Linde, C.; Abraham, W.T.; Gold, M.R.; St John Sutton, M.; Ghio, S.; Daubert, C.; REVERSE Study Group. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J. Am. Coll. Cardiol. 2008, 52, 1834–1843. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Fisher, W.G.; Smith, A.L.; Delurgio, D.B.; Leon, A.R.; Loh, E.; Kocovic, D.Z.; Packer, M.; Clavell, A.L.; Hayes, D.L.; et al. Cardiac resynchronization in chronic heart failure. N. Engl. J. Med. 2002, 346, 1845–1853. [Google Scholar] [CrossRef]
- Daubert, C.; Gold, M.R.; Abraham, W.T.; Ghio, S.; Hassager, C.; Goode, G.; Szili-Torok, T.; Linde, C.; REVERSE Study Group. Prevention of disease progression by cardiac resynchronization therapy in patients with asymptomatic or mildly symptomatic left ventricular dysfunction: Insights from the European cohort of the REVERSE (Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction) trial. J. Am. Coll. Cardiol. 2009, 54, 1837–1846. [Google Scholar] [CrossRef]
- Tang, A.S.; Wells, G.A.; Talajic, M.; Arnold, M.O.; Sheldon, R.; Connolly, S.; Hohnloser, S.H.; Nichol, G.; Birnie, D.H.; Sapp, J.L.; et al. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N. Engl. J. Med. 2010, 363, 2385–2395. [Google Scholar] [CrossRef]
- Linde, C.; Leclercq, C.; Rex, S.; Garrigue, S.; Lavergne, T.; Cazeau, S.; McKenna, W.; Fitzgerald, M.; Deharo, J.C.; Alonso, C.; et al. Long-term benefits of biventricular pacing in congestive heart failure: Results from the MUltisite STimulation in cardiomyopathy (MUSTIC) study. J. Am. Coll. Cardiol. 2002, 40, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Sutton, M.G.; Plappert, T.; Hilpisch, K.E.; Abraham, W.T.; Hayes, D.L.; Chinchoy, E. Sustained reverse left ventricular structural remodeling with cardiac resynchronization at one year is a function of etiology: Quantitative Doppler echocardiographic evidence from the Multicenter InSync Randomized Clinical Evaluation (MIRACLE). Circulation 2006, 113, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Bristow, M.R.; Saxon, L.A.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; DiCarlo, L.; DeMets, D.; White, B.G.; et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N. Engl. J. Med. 2004, 350, 2140–2150. [Google Scholar] [CrossRef]
- Young, J.B.; Abraham, W.T.; Smith, A.L.; Leon, A.R.; Lieberman, R.; Wilkoff, B.; Canby, R.C.; Schroeder, J.S.; Liem, L.B.; Hall, S.; et al. Combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure: The MIRACLE ICD Trial. JAMA 2003, 289, 2685–2694. [Google Scholar] [CrossRef]
- Bryant, A.R.; Wilton, S.B.; Lai, M.P.; Exner, D.V. Association between QRS duration and outcome with cardiac resynchronization therapy: A systematic review and meta-analysis. J. Electrocardiol. 2013, 46, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Egoavil, C.A.; Ho, R.T.; Greenspon, A.J.; Pavri, B.B. Cardiac resynchronization therapy in patients with right bundle branch block: Analysis of pooled data from the MIRACLE and Contak CD trials. Heart Rhythm 2005, 2, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Gervais, R.; Leclercq, C.; Shankar, A.; Jacobs, S.; Eiskjaer, H.; Johannessen, A.; Freemantle, N.; Cleland, J.G.; Tavazzi, L.; Daubert, C.; et al. Surface electrocardiogram to predict outcome in candidates for cardiac resynchronization therapy: A sub-analysis of the CARE-HF trial. Eur. J. Heart Fail. 2009, 11, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.G.F.; Bristow, M.R.; Freemantle, N.; Olshansky, B.; Gras, D.; Saxon, L.; Tavazzi, L.; Boehmer, J.; Ghio, S.; Feldman, A.M.; et al. The effect of cardiac resynchronization without a defibrillator on morbidity and mortality: An individual patient data meta-analysis of COMPANION and CARE-HF. Eur. J. Heart Fail. 2022, 24, 1080–1090. [Google Scholar] [CrossRef]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabes, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef]
- Auricchio, A.; Prinzen, F.W. Non-responders to cardiac resynchronization therapy: The magnitude of the problem and the issues. Circ. J. 2011, 75, 521–527. [Google Scholar] [CrossRef]
- van Stipdonk, A.M.W.; Ter Horst, I.; Kloosterman, M.; Engels, E.B.; Rienstra, M.; Crijns, H.; Vos, M.A.; van Gelder, I.C.; Prinzen, F.W.; Meine, M.; et al. QRS Area Is a Strong Determinant of Outcome in Cardiac Resynchronization Therapy. Circ. Arrhythmia Electrophysiol. 2018, 11, e006497. [Google Scholar] [CrossRef]
- Dural, M.; van Stipdonk, A.M.W.; Salden, F.; Ter Horst, I.; Crijns, H.; Meine, M.; Maass, A.H.; Kloosterman, M.; Vernooy, K. Association of ECG characteristics with clinical and echocardiographic outcome to CRT in a non-LBBB patient population. J. Interv. Card. Electrophysiol. 2021, 62, 9–19. [Google Scholar] [CrossRef]
- Dural, M.; Ghossein, M.A.; Gerrits, W.; Daniels, F.; Meine, M.; Maass, A.H.; Rienstra, M.; Prinzen, F.W.; Vernooy, K.; van Stipdonk, A.M.W. Association of vectorcardiographic T-wave area with clinical and echocardiographic outcomes in cardiac resynchronization therapy. Europace 2023, 26, euad370. [Google Scholar] [CrossRef]
- Durrer, D.; van Dam, R.T.; Freud, G.E.; Janse, M.J.; Meijler, F.L.; Arzbaecher, R.C. Total excitation of the isolated human heart. Circulation 1970, 41, 899–912. [Google Scholar] [CrossRef]
- Spach, M.S.; Miller, W.T., 3rd; Geselowitz, D.B.; Barr, R.C.; Kootsey, J.M.; Johnson, E.A. The discontinuous nature of propagation in normal canine cardiac muscle. Evidence for recurrent discontinuities of intracellular resistance that affect the membrane currents. Circ. Res. 1981, 48, 39–54. [Google Scholar] [CrossRef] [PubMed]
- De Pooter, J.; El Haddad, M.; Timmers, L.; Van Heuverswyn, F.; Jordaens, L.; Duytschaever, M.; Stroobandt, R. Different Methods to Measure QRS Duration in CRT Patients: Impact on the Predictive Value of QRS Duration Parameters. Ann. Noninvasive Electrocardiol. 2016, 21, 305–315. [Google Scholar] [CrossRef]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.A.; Cleland, J.; Deharo, J.C.; Elliott, P.M.; Gorenek, B.; et al. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: The task force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Europace 2013, 15, 1070–1118. [Google Scholar] [CrossRef]
- Surawicz, B.; Childers, R.; Deal, B.J.; Gettes, L.S.; Bailey, J.J.; Gorgels, A.; Hancock, E.W.; Josephson, M.; Kligfield, P.; Kors, J.A.; et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part III: Intraventricular conduction disturbances: A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: Endorsed by the International Society for Computerized Electrocardiology. Circulation 2009, 119, e235–e240. [Google Scholar] [CrossRef] [PubMed]
- Strauss, D.G.; Selvester, R.H.; Wagner, G.S. Defining left bundle branch block in the era of cardiac resynchronization therapy. Am. J. Cardiol. 2011, 107, 927–934. [Google Scholar] [CrossRef]
- Zareba, W.; Klein, H.; Cygankiewicz, I.; Hall, W.J.; McNitt, S.; Brown, M.; Cannom, D.; Daubert, J.P.; Eldar, M.; Gold, M.R.; et al. Effectiveness of Cardiac Resynchronization Therapy by QRS Morphology in the Multicenter Automatic Defibrillator Implantation Trial-Cardiac Resynchronization Therapy (MADIT-CRT). Circulation 2011, 123, 1061–1072. [Google Scholar] [CrossRef]
- van Stipdonk, A.M.W.; Vanbelle, S.; Ter Horst, I.A.H.; Luermans, J.G.; Meine, M.; Maass, A.H.; Auricchio, A.; Prinzen, F.W.; Vernooy, K. Large variability in clinical judgement and definitions of left bundle branch block to identify candidates for cardiac resynchronisation therapy. Int. J. Cardiol. 2019, 286, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Caputo, M.L.; van Stipdonk, A.; Illner, A.; D’Ambrosio, G.; Regoli, F.; Conte, G.; Moccetti, T.; Klersy, C.; Prinzen, F.W.; Vernooy, K.; et al. The definition of left bundle branch block influences the response to cardiac resynchronization therapy. Int. J. Cardiol. 2018, 269, 165–169. [Google Scholar] [CrossRef]
- Varma, N. Left ventricular conduction delays and relation to QRS configuration in patients with left ventricular dysfunction. Am. J. Cardiol. 2009, 103, 1578–1585. [Google Scholar] [CrossRef]
- Bacharova, L.; Szathmary, V.; Mateasik, A. Electrocardiographic patterns of left bundle-branch block caused by intraventricular conduction impairment in working myocardium: A model study. J. Electrocardiol. 2011, 44, 768–778. [Google Scholar] [CrossRef]
- Fantoni, C.; Kawabata, M.; Massaro, R.; Regoli, F.; Raffa, S.; Arora, V.; Salerno-Uriarte, J.A.; Klein, H.U.; Auricchio, A. Right and left ventricular activation sequence in patients with heart failure and right bundle branch block: A detailed analysis using three-dimensional non-fluoroscopic electroanatomic mapping system. J. Cardiovasc. Electrophysiol. 2005, 16, 112–119; discussion 120–121. [Google Scholar] [CrossRef]
- Frank, E. An accurate, clinically practical system for spatial vectorcardiography. Circulation 1956, 13, 737–749. [Google Scholar] [CrossRef] [PubMed]
- Engels, E.B.; Alshehri, S.; van Deursen, C.J.; Wecke, L.; Bergfeldt, L.; Vernooy, K.; Prinzen, F.W. The synthesized vectorcardiogram resembles the measured vectorcardiogram in patients with dyssynchronous heart failure. J. Electrocardiol. 2015, 48, 586–592. [Google Scholar] [CrossRef]
- Plesinger, F.; van Stipdonk, A.M.W.; Smisek, R.; Halamek, J.; Jurak, P.; Maass, A.H.; Meine, M.; Vernooy, K.; Prinzen, F.W. Fully automated QRS area measurement for predicting response to cardiac resynchronization therapy. J. Electrocardiol. 2020, 63, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Draisma, H.H.; Schalij, M.J.; van der Wall, E.E.; Swenne, C.A. Elucidation of the spatial ventricular gradient and its link with dispersion of repolarization. Heart Rhythm 2006, 3, 1092–1099. [Google Scholar] [CrossRef] [PubMed]
- Man, S.; Maan, A.C.; Schalij, M.J.; Swenne, C.A. Vectorcardiographic diagnostic & prognostic information derived from the 12-lead electrocardiogram: Historical review and clinical perspective. J. Electrocardiol. 2015, 48, 463–475. [Google Scholar] [CrossRef]
- Abbott-Smith, C.W.; Chou, T.C. Vectorcardiographic criteria for the diagnosis of left ventricular hypertrophy. Am. Heart J. 1970, 79, 361–369. [Google Scholar] [CrossRef]
- Vine, D.L.; Finchum, R.N.; Dodge, H.T.; Bancroft, W.H., Jr.; Hurst, D.C. Comparison of the vectorcardiogram with the electrocardiogram in the prediction of left ventricular size. Circulation 1971, 43, 547–558. [Google Scholar] [CrossRef]
- Perez Riera, A.R.; Uchida, A.H.; Filho, C.F.; Meneghini, A.; Ferreira, C.; Schapacknik, E.; Dubner, S.; Moffa, P. Significance of vectorcardiogram in the cardiological diagnosis of the 21st century. Clin. Cardiol. 2007, 30, 319–323. [Google Scholar] [CrossRef]
- Hurd, H.P., 2nd; Starling, M.R.; Crawford, M.H.; Dlabal, P.W.; O’Rourke, R.A. Comparative accuracy of electrocardiographic and vectorcardiographic criteria for inferior myocardial infarction. Circulation 1981, 63, 1025–1029. [Google Scholar] [CrossRef]
- Vernooy, K.; Cornelussen, R.N.; Verbeek, X.A.; Vanagt, W.Y.; van Hunnik, A.; Kuiper, M.; Arts, T.; Crijns, H.J.; Prinzen, F.W. Cardiac resynchronization therapy cures dyssynchronopathy in canine left bundle-branch block hearts. Eur. Heart J. 2007, 28, 2148–2155. [Google Scholar] [CrossRef] [PubMed]
- Rad, M.M.; Blaauw, Y.; Dinh, T.; Pison, L.; Crijns, H.J.; Prinzen, F.W.; Vernooy, K. Left ventricular lead placement in the latest activated region guided by coronary venous electroanatomic mapping. Europace 2015, 17, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Mafi Rad, M.; Wijntjens, G.W.; Engels, E.B.; Blaauw, Y.; Luermans, J.G.; Pison, L.; Crijns, H.J.; Prinzen, F.W.; Vernooy, K. Vectorcardiographic QRS area identifies delayed left ventricular lateral wall activation determined by electroanatomic mapping in candidates for cardiac resynchronization therapy. Heart Rhythm 2016, 13, 217–225. [Google Scholar] [CrossRef] [PubMed]
- van Deursen, C.J.; Vernooy, K.; Dudink, E.; Bergfeldt, L.; Crijns, H.J.; Prinzen, F.W.; Wecke, L. Vectorcardiographic QRS area as a novel predictor of response to cardiac resynchronization therapy. J. Electrocardiol. 2015, 48, 45–52. [Google Scholar] [CrossRef]
- Nguyen, U.C.; Claridge, S.; Vernooy, K.; Engels, E.B.; Razavi, R.; Rinaldi, C.A.; Chen, Z.; Prinzen, F.W. Relationship between vectorcardiographic QRS(area), myocardial scar quantification, and response to cardiac resynchronization therapy. J. Electrocardiol. 2018, 51, 457–463. [Google Scholar] [CrossRef]
- Tereshchenko, L.G.; Cheng, A.; Park, J.; Wold, N.; Meyer, T.E.; Gold, M.R.; Mittal, S.; Singh, J.; Stein, K.M.; Ellenbogen, K.A.; et al. Novel measure of electrical dyssynchrony predicts response in cardiac resynchronization therapy: Results from the SMART-AV Trial. Heart Rhythm 2015, 12, 2402–2410. [Google Scholar] [CrossRef]
- Maass, A.H.; Vernooy, K.; Wijers, S.C.; van ‘t Sant, J.; Cramer, M.J.; Meine, M.; Allaart, C.P.; De Lange, F.J.; Prinzen, F.W.; Gerritse, B.; et al. Refining success of cardiac resynchronization therapy using a simple score predicting the amount of reverse ventricular remodelling: Results from the Markers and Response to CRT (MARC) study. Europace 2018, 20, e1–e10. [Google Scholar] [CrossRef]
- Emerek, K.; Friedman, D.J.; Sorensen, P.L.; Hansen, S.M.; Larsen, J.M.; Risum, N.; Thogersen, A.M.; Graff, C.; Kisslo, J.; Sogaard, P.; et al. Vectorcardiographic QRS area is associated with long-term outcome after cardiac resynchronization therapy. Heart Rhythm 2019, 16, 213–219. [Google Scholar] [CrossRef]
- Okafor, O.; Zegard, A.; van Dam, P.; Stegemann, B.; Qiu, T.; Marshall, H.; Leyva, F. Changes in QRS Area and QRS Duration After Cardiac Resynchronization Therapy Predict Cardiac Mortality, Heart Failure Hospitalizations, and Ventricular Arrhythmias. J. Am. Heart Assoc. 2019, 8, e013539. [Google Scholar] [CrossRef]
- Ghossein, M.A.; van Stipdonk, A.M.W.; Plesinger, F.; Kloosterman, M.; Wouters, P.C.; Salden, O.A.E.; Meine, M.; Maass, A.H.; Prinzen, F.W.; Vernooy, K. Reduction in the QRS area after cardiac resynchronization therapy is associated with survival and echocardiographic response. J. Cardiovasc. Electrophysiol. 2021, 32, 813–822. [Google Scholar] [CrossRef]
- Bose, A.; Kandala, J.; Upadhyay, G.A.; Riedl, L.; Ahmado, I.; Padmanabhan, R.; Gewirtz, H.; Mulligan, L.J.; Singh, J.P. Impact of myocardial viability and left ventricular lead location on clinical outcome in cardiac resynchronization therapy recipients with ischemic cardiomyopathy. J. Cardiovasc. Electrophysiol. 2014, 25, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.J.; Umar, F.; Panting, J.R.; Stegemann, B.; Leyva, F. Left ventricular lead position, mechanical activation, and myocardial scar in relation to left ventricular reverse remodeling and clinical outcomes after cardiac resynchronization therapy: A feature-tracking and contrast-enhanced cardiovascular magnetic resonance study. Heart Rhythm 2016, 13, 481–489. [Google Scholar] [CrossRef]
- Khan, F.Z.; Virdee, M.S.; Palmer, C.R.; Pugh, P.J.; O’Halloran, D.; Elsik, M.; Read, P.A.; Begley, D.; Fynn, S.P.; Dutka, D.P. Targeted left ventricular lead placement to guide cardiac resynchronization therapy: The TARGET study: A randomized, controlled trial. J. Am. Coll. Cardiol. 2012, 59, 1509–1518. [Google Scholar] [CrossRef]
- Parreira, L.; Tsyganov, A.; Artyukhina, E.; Vernooy, K.; Tondo, C.; Adragao, P.; Ascione, C.; Carmo, P.; Carvalho, S.; Egger, M.; et al. Non-invasive three-dimensional electrical activation mapping to predict cardiac resynchronization therapy response: Site of latest left ventricular activation relative to pacing site. Europace 2023, 25, 1458–1466. [Google Scholar] [CrossRef]
- Nguyen, U.C.; Cluitmans, M.J.M.; Strik, M.; Luermans, J.G.; Gommers, S.; Wildberger, J.E.; Bekkers, S.; Volders, P.G.A.; Mihl, C.; Prinzen, F.W.; et al. Integration of cardiac magnetic resonance imaging, electrocardiographic imaging, and coronary venous computed tomography angiography for guidance of left ventricular lead positioning. Europace 2019, 21, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Marallo, C.; Landra, F.; Taddeucci, S.; Collantoni, M.; Martini, L.; Lunghetti, S.; Pagliaro, A.; Menci, D.; Baiocchi, C.; Fineschi, M.; et al. Cardiac resynchronization therapy guided by interventricular conduction delay: How to choose between biventricular pacing or conduction system pacing. J. Cardiovasc. Electrophysiol. 2024, 35, 2345–2353. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Landra, F.; Marallo, C.; Taddeucci, S.; Sisti, N.; Pica, A.; Stefanini, A.; Tavera, M.C.; Pagliaro, A.; Baiocchi, C.; et al. Biventricular or Conduction System Pacing for Cardiac Resynchronization Therapy: A Strategy for Cardiac Resynchronization Based on a Hybrid Approach. J. Cardiovasc. Dev. Dis. 2023, 10, 169. [Google Scholar] [CrossRef] [PubMed]
- Okafor, O.; Umar, F.; Zegard, A.; van Dam, P.; Walton, J.; Stegemann, B.; Marshall, H.; Leyva, F. Effect of QRS area reduction and myocardial scar on the hemodynamic response to cardiac resynchronization therapy. Heart Rhythm 2020, 17, 2046–2055. [Google Scholar] [CrossRef]
- Ghossein, M.A.; Zanon, F.; Salden, F.; van Stipdonk, A.; Marcantoni, L.; Engels, E.; Luermans, J.; Westra, S.; Prinzen, F.; Vernooy, K. Left Ventricular Lead Placement Guided by Reduction in QRS Area. J. Clin. Med. 2021, 10, 5935. [Google Scholar] [CrossRef]
- Tomaselli, G.F.; Beuckelmann, D.J.; Calkins, H.G.; Berger, R.D.; Kessler, P.D.; Lawrence, J.H.; Kass, D.; Feldman, A.M.; Marban, E. Sudden cardiac death in heart failure. The role of abnormal repolarization. Circulation 1994, 90, 2534–2539. [Google Scholar] [CrossRef]
- Beltrami, C.A.; Finato, N.; Rocco, M.; Feruglio, G.A.; Puricelli, C.; Cigola, E.; Quaini, F.; Sonnenblick, E.H.; Olivetti, G.; Anversa, P. Structural basis of end-stage failure in ischemic cardiomyopathy in humans. Circulation 1994, 89, 151–163. [Google Scholar] [CrossRef]
- Acar, B.; Yi, G.; Hnatkova, K.; Malik, M. Spatial, temporal and wavefront direction characteristics of 12-lead T-wave morphology. Med. Biol. Eng. Comput. 1999, 37, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.C.; Lin, L.Y.; Yu, H.Y.; Ho, Y.L. Risk stratification by T-wave morphology for cardiovascular mortality in patients with systolic heart failure. Europace 2009, 11, 1522–1528. [Google Scholar] [CrossRef] [PubMed]
- Narayan, S.M. T-wave alternans and the susceptibility to ventricular arrhythmias. J. Am. Coll. Cardiol. 2006, 47, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Anh, D.; Srivatsa, U.; Bui, H.M.; Vasconcellos, S.; Narayan, S.M. Biventricular pacing attenuates T-wave alternans and T-wave amplitude compared to other pacing modes. Pacing Clin. Electrophysiol. 2008, 31, 714–721. [Google Scholar] [CrossRef]
- Huang, H.C.; Chien, K.L.; Chang, Y.C.; Lin, L.Y.; Wang, J.; Liu, Y.B. Increases in repolarization heterogeneity predict left ventricular systolic dysfunction and response to cardiac resynchronization therapy in patients with left bundle branch block. J. Cardiovasc. Electrophysiol. 2020, 31, 1770–1778. [Google Scholar] [CrossRef]
- Shvilkin, A.; Bojovic, B.; Vajdic, B.; Gussak, I.; Zimetbaum, P.; Josephson, M.E. Vectorcardiographic determinants of cardiac memory during normal ventricular activation and continuous ventricular pacing. Heart Rhythm 2009, 6, 943–948. [Google Scholar] [CrossRef]
- Shvilkin, A.; Huang, H.D.; Josephson, M.E. Cardiac memory: Diagnostic tool in the making. Circ. Arrhythmia Electrophysiol. 2015, 8, 475–482. [Google Scholar] [CrossRef]
- Engels, E.B.; Vegh, E.M.; Van Deursen, C.J.; Vernooy, K.; Singh, J.P.; Prinzen, F.W. T-wave area predicts response to cardiac resynchronization therapy in patients with left bundle branch block. J. Cardiovasc. Electrophysiol. 2015, 26, 176–183. [Google Scholar] [CrossRef]
- Vegh, E.M.; Engels, E.B.; van Deursen, C.J.; Merkely, B.; Vernooy, K.; Singh, J.P.; Prinzen, F.W. T-wave area as biomarker of clinical response to cardiac resynchronization therapy. Europace 2016, 18, 1077–1085. [Google Scholar] [CrossRef]
- Diaz, J.C.; Gabr, M.; Tedrow, U.B.; Duque, M.; Aristizabal, J.; Marin, J.; Nino, C.; Bastidas, O.; Koplan, B.A.; Hoyos, C.; et al. Improved all-cause mortality with left bundle branch area pacing compared to biventricular pacing in cardiac resynchronization therapy: A meta-analysis. J. Interv. Card. Electrophysiol. 2024, 67, 1463–1476. [Google Scholar] [CrossRef] [PubMed]
- Heckman, L.I.B.; Luermans, J.; Jastrzebski, M.; Weijs, B.; Van Stipdonk, A.M.W.; Westra, S.; den Uijl, D.; Linz, D.; Mafi-Rad, M.; Prinzen, F.W.; et al. A single-centre prospective evaluation of left bundle branch area pacemaker implantation characteristics. Neth. Heart J. 2022, 30, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Gu, M.; Niu, H.X.; Chen, X.; Cai, C.; Zhao, J.; Cai, M.; Zhou, X.; Gold, M.R.; Zhang, S.; et al. A Comparison of the Electrophysiological and Anatomic Characteristics of Pacing Different Branches of the Left Bundle Conduction System. Front. Cardiovasc. Med. 2021, 8, 781845. [Google Scholar] [CrossRef]
- Heckman, L.I.B.; Luermans, J.; Curila, K.; Van Stipdonk, A.M.W.; Westra, S.; Smisek, R.; Prinzen, F.W.; Vernooy, K. Comparing Ventricular Synchrony in Left Bundle Branch and Left Ventricular Septal Pacing in Pacemaker Patients. J. Clin. Med. 2021, 10, 822. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Design | Patients (n) | Inclusion | Follow-Up | Outcomes | Parameters | Results |
|---|---|---|---|---|---|---|---|
| Van Deursen, et al. [44] (2014) | Prospective | 81 | Class I and II | 6 mo | Echocardiographic response (LVESV reduction ≥ 15%) | - QRS area > 98 μVs - QRS duration > 156 ms - LBBB
| - OR 10.2; 95% CI: 3.4–31.1 - OR 2.5; 95% CI: 0.9–6.6 - LBBB
|
| Mafi-Rad, et al. [43] (2016) | Prospective | 51 | Class I and II | - | Delayed LV activation (>75% of QRS duration) | - QRS area - QRS area > 69 μVs - QRS duration - LBBB (ESC) | - AUC 0.89; 95% CI: 0.79–0.99 - Sens: 87%; spec: 92% - AUC 0.49; 95% CI: 0.33–0.65 (ns) - Sens 76%; spec 100% |
| Nguyen, et al. [45] (2018) | Prospective | 33 | Class I and II | 6 mo | Echocardiographic response (LVESV reduction ≥ 15%) | - QRS area - QRS duration | - AUC 0.74; 95% CI: 0.56–0.91 - AUC 0.64; 95% CI: 0.44–0.83 (ns) |
| MARC Study [47] (2018) | Prospective | 213 | Class I and II | 6 mo |
| - QRS area - QRS duration - LBBB | * Adjusted effect estimate - 10.4%, 95% CI: (−14.9, −5.8), p < 0.001 - ns - ns |
| Van Stipdonk, et al. [17] (2018) | Retrospective | 1.491 | Class I and II | 3.4 yrs | A. Echocardiographic response (LVESV reduction ≥ 15%) B. Clinical outcome-All-cause mortality C. Clinical outcome-HF hospitalization | 1. QRS area quartiles 2. LBBB + QRSd | A-1. ** OR 1.65; 95%CI: 1.43–1.90 2. OR 1.29; 95%CI: 1.09–1.52 B-1. ** HR: 0.75; 95% CI: 0.69–0.83 2. HR: 0.93; 95% CI: 0.69–1.02 (ns) C-1. HR: 0.76; 95% CI: 0.60–0.96 2. HR: 0.96; 95% CI: 0.71–1.21 (ns) |
| Emerek, et al. [48] (2019) | Retrospective | 705 | Class I and II | 3.1 yrs | All-cause mortality | QRS area ≤ 95 μVs | *** HR: 1.65; 95% CI: 1.25–2.18 |
| Okafor, et al. [49] (2019) | Retrospective | 380 | Class I and II | 3.8 yrs | Cardiac mortality | 1. QRS area 2. QRS duration 3. LBBB | 1. † HR: 0.99; 95% CI: 0.98–0.99 2. † HR: 1.01; 95% CI: 0.99–1.02 (ns) 3. HR: 0.79; 95% CI: 0.79–1.27 (ns) |
| Dural, et al. [18] (2021) | Retrospective | 790 | Class II (non-LBBB) | 3.7 yrs | A. Clinical outcome-All-cause mortality B. Echocardiographic response (LVESV reduction ≥ 15%) | 1. QRS area ≥ 109 μVs 2. QRSd ≥ 150 ms 3. RBBB 4. IVCD | A-1. ** HR: 2.33; 95% CI: 1.44–3.77 2. ns 3. ns 4. ns B-1. OR: 2.00; 95% CI: 1.09–3.66 2. ns 3. ns 4. ns |
| Ghossein, et al. [50] (2021) | Retrospective | 1.299 | Class I and II | 3.9 yrs | A. Clinical outcome-All-cause mortality B. Echocardiographic response (LVESV reduction ≥ 15%) | 1. QRS area ≥ 109 μVs 2. QRSd ≥ 150 ms 3. LBBB (ESC) | A-1. ‡ HR: 0.72; 95% CI: 0.56–0.96 2. ‡ HR: 1.1; 95% CI: 0.89–1.49 (ns) 3. ‡ HR: 0.78; 95% CI: 0.61–1.00 (ns) B-1. ‡ OR: 1.7; 95% CI: 1.2–2.5 2. ‡ OR: 1.4; 95% CI: 0.97–2.0 3. ‡ OR: 1.8; 95% CI: 1.2–2.7 |
| Study | Design | Patients (n) | Inclusion | Follow-Up (Years) | Outcomes | Parameters | Results |
|---|---|---|---|---|---|---|---|
| Engels, et al. [69] (2015) | Retrospective | 244 | Class I and II | 6 mo | Echocardiographic response (LVEF increase ≥ 5%) | - T-wave area, μVs - QRS duration, ms - QRS area, µVs | - * OR: 1.17; 95% CI: 1.08–1.25 - OR: 0.99; 95% CI: 0.92–1.08 (ns) - OR: 1.12; 95% CI: 1.05–1.19 |
| Vegh, et al. [70] (2016) | Retrospective | 335 | Class I and II | 2.4 yrs | All-cause mortality | - T-wave area, μVs - QRS duration > 150 ms - QRS area, μVs - LBBB | - ** HR 0.63; 95% CI: 0.42–0.96 - ns - ns - HR 0.65; 95% CI: 0.44–0.98 |
| Dural, et al. [19] (2024) | Retrospective | 1.355 | Class I and II | 3.7 yrs | A. All-cause mortality B. Echocardiographic response (LVESV reduction ≥ 15%) | 1. T-wave area, μVs 2. QRS duration, ms ≥ 150 ms 3. LBBB (ESC) | A-1. *** HR 0.46; 95% CI: 0.31–0.69 2. HR 0.72; 95% CI: 0.47–1.10 (ns) 3. HR 1.15; 95% CI: 0.75–1.77 (ns) B-1. *** OR: 3.10; 95% CI: 2.02–4.76 2. OR: 1.34; 95% CI: 0.83–2.18 (ns) 3. OR: 2.34; 95% CI: 1.37–4.00) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dural, M.; Eerenberg, F.; Smits, K.C.; Nguyên, U.C.; Vernooy, K.; van Stipdonk, A.M.W. Vectorcardiography in CRT: What We Know and What There Is to Learn. J. Cardiovasc. Dev. Dis. 2025, 12, 177. https://doi.org/10.3390/jcdd12050177
Dural M, Eerenberg F, Smits KC, Nguyên UC, Vernooy K, van Stipdonk AMW. Vectorcardiography in CRT: What We Know and What There Is to Learn. Journal of Cardiovascular Development and Disease. 2025; 12(5):177. https://doi.org/10.3390/jcdd12050177
Chicago/Turabian StyleDural, Muhammet, Frederieke Eerenberg, Karin C. Smits, Uyên Châu Nguyên, Kevin Vernooy, and Antonius M. W. van Stipdonk. 2025. "Vectorcardiography in CRT: What We Know and What There Is to Learn" Journal of Cardiovascular Development and Disease 12, no. 5: 177. https://doi.org/10.3390/jcdd12050177
APA StyleDural, M., Eerenberg, F., Smits, K. C., Nguyên, U. C., Vernooy, K., & van Stipdonk, A. M. W. (2025). Vectorcardiography in CRT: What We Know and What There Is to Learn. Journal of Cardiovascular Development and Disease, 12(5), 177. https://doi.org/10.3390/jcdd12050177