
Sex-Specific Patterns in Blood Pressure and Vascular Parameters: The MUJER-EVA Project

 , , ,
, , ,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Sample Characteristics
2.2. Ethical Considerations
2.3. Variables
2.3.1. Dependent Variables
2.3.2. Independent Variable
2.3.3. Covariates
- Continuous covariates included age (in years), body mass index (BMI, kg/m2), and waist circumference (cm).
- The categorical covariates included educational level, employment status, family history of myocardial infarction, family history of stroke, and smoking status.
2.4. Statistical Analysis
- Model 1 (Unadjusted).
- Model 2: Age and peripheral systolic and diastolic blood pressure (this adjustment was used in all models, except when the independent variable was peripheral systolic and diastolic blood pressure and pulse pressure, to avoid overadjustment).
- Model 3 (adjusted for continuous variables): Age, BMI, and waist circumference were included as covariates.
- Model 4 (fully adjusted): This included both continuous and categorical covariates (education level, employment status, family history of CVD (myocardial infarction, stroke), and smoking status).
3. Results
3.1. Demographic, Anthropometric, and Socioeconomic Variables
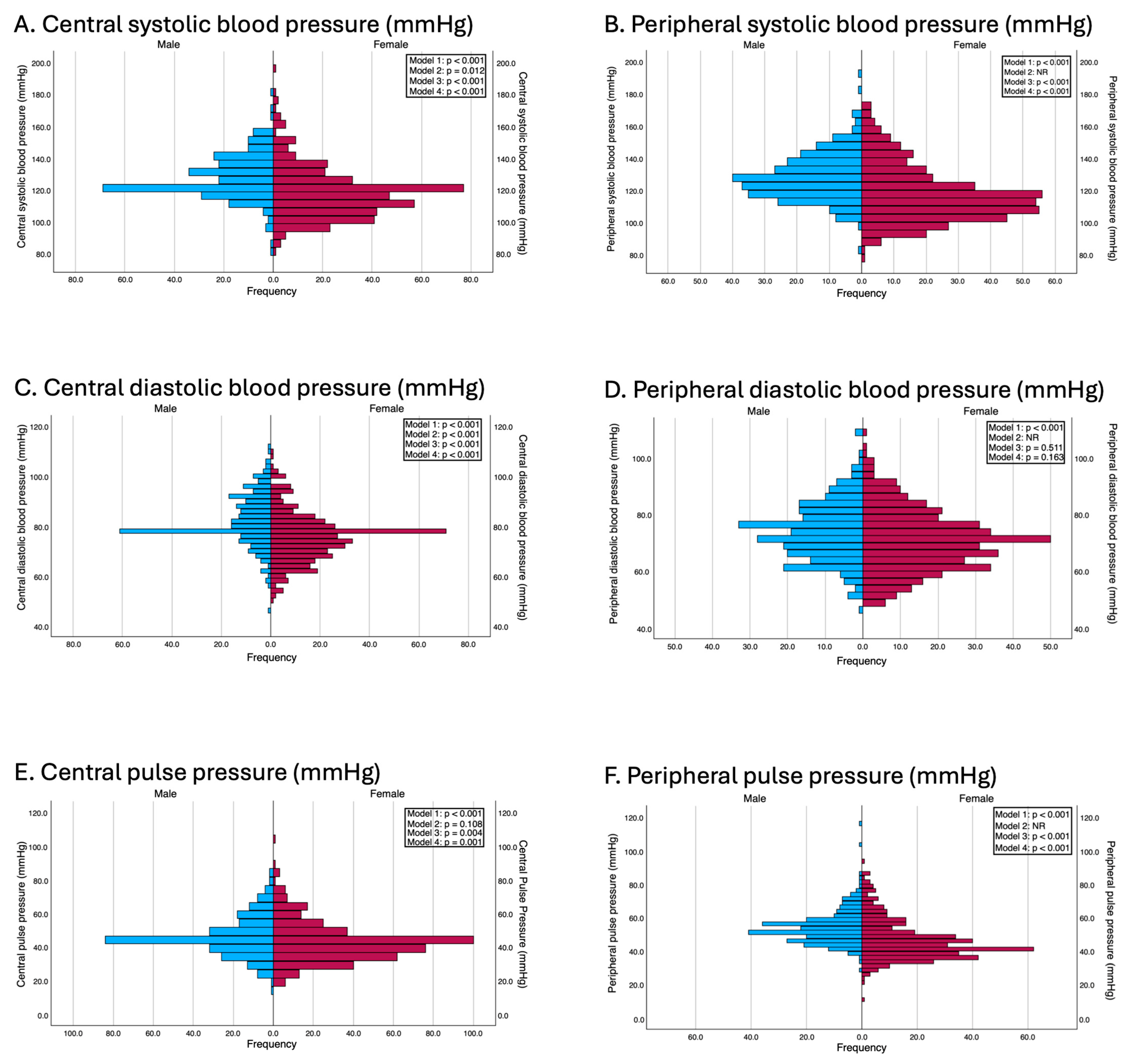
3.2. Blood Pressure Parameters
3.3. Hemodynamic Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AIx75 | Augmentation index, normalized to 75 beats per minute |
| BMI | Body mass index |
| CVD | Cardiovascular disease |
| IQR | Interquartile range |
| OLS | Ordinary least squares |
| PWv | Pulse wave velocity |
References
- World Health Organization. Cardiovascular Diseases (CVDs). 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 3 February 2025).
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Safar, M.E.; London, G.M. Therapeutic studies and arterial stiffness in hypertension: Recommendations of the European Society of Hypertension. J. Hypertens. 2000, 18, 1527–1535. [Google Scholar] [CrossRef]
- Nilsson, P.M.; Boutouyrie, P.; Laurent, S. Vascular aging: A tale of EVA and ADAM in cardiovascular risk assessment and prevention. Hypertension 2009, 54, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [PubMed]
- Regitz-Zagrosek, V.; Oertelt-Prigione, S.; Prescott, E.; Franconi, F.; Gerdts, E.; Foryst-Ludwig, A.; Maas, A.H.; Kautzky-Willer, A.; Knappe-Wegner, D.; Kintscher, U.; et al. Gender in cardiovascular diseases: Impact on clinical manifestations, management, and outcomes. Eur. Heart J. 2016, 37, 24–34. [Google Scholar] [CrossRef]
- Maas, A.H.E.M.; Appelman, Y.E.A. Gender differences in coronary heart disease. Neth. Heart J. 2010, 18, 598–602. [Google Scholar] [CrossRef]
- García, M.; Mulvagh, S.L.; Merz, C.N.; Buring, J.E.; Manson, J.E. Cardiovascular disease in women: Clinical perspectives. Circ. Res. 2016, 118, 1273–1293. [Google Scholar] [CrossRef]
- Bots, S.H.; Peters, S.A.E.; Woodward, M. Sex differences in coronary heart disease and stroke mortality: A global assessment of the effect of ageing between 1980 and 2010. BMJ Glob. Health 2017, 2, e000298. [Google Scholar] [CrossRef]
- Seeland, U.; Nemcsik, J.; Lønnebakken, M.T.; Kublickiene, K.; Schluchter, H.; Park, C.; Pucci, G.; Mozos, I.; Bruno, R.-M.; Sex and Gender VascAgeNet Expert Group. Sex and gender aspects in vascular ageing: Focus on epidemiology, pathophysiology, and outcomes. Heart Lung Circ. 2021, 30, 1637–1646. [Google Scholar] [CrossRef]
- Hayward, C.S.; Kelly, R.P.; Collins, P. The roles of gender, the menopause and hormone replacement on cardiovascular function. Cardiovasc. Res. 2000, 46, 28–49. [Google Scholar] [CrossRef]
- Smulyan, H.; Marchais, S.J.; Pannier, B.; Guerin, A.P.; Levy, B.I.; London, G.M. Influence of body height on pulsatile arterial hemodynamic data. J. Am. Coll. Cardiol. 1998, 31, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F.; Parise, H.; Benjamin, E.J.; Larson, M.G.; Keyes, M.J.; Vita, J.A.; Vasan, R.S.; Levy, D. Changes in arterial stiffness and wave reflection with advancing age in healthy men and women: The Framingham Heart Study. Hypertension. 2004, 43, 1239–1245. [Google Scholar] [CrossRef]
- Cecelja, M.; Chowienczyk, P. Role of arterial stiffness in cardiovascular disease. JRSM Cardiovasc. Dis. 2012, 1, cvd.2012.012016. [Google Scholar] [CrossRef]
- Adkisson, E.J.; Casey, D.P.; Beck, D.T.; Gurovich, A.N.; Martin, J.S.; Braith, R.W. Central, peripheral and resistance arterial reactivity fluctuates during the menstrual cycle. Exp. Biol. Med. (Maywood) 2010, 235, 111–118. [Google Scholar] [CrossRef]
- Parker, B.A.; Kalasky, M.J.; Proctor, D.N. Evidence for sex differences in cardiovascular aging and adaptive responses to physical activity. Eur. J. Appl. Physiol. 2010, 110, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Saz-Lara, A.; Cavero-Redondo, I.; Martínez-García, I.; Rodríguez-Gutiérrez, E.; Lucerón-Lucas-Torres, M.; Pascual-Morena, C.; Bizzozero-Peroni, B.; Moreno-Herráiz, N.; Martínez-Rodrigo, A. Early vascular aging as an index of cardiovascular risk in healthy adults: Confirmatory factor analysis from the EVasCu study. Cardiovasc. Diabetol. 2023, 22, 209. [Google Scholar] [CrossRef] [PubMed]
- Cavero-Redondo, I.; Saz-Lara, A.; Martínez-García, I.; Bizzozero-Peroni, B.; Díaz-Goñi, V.; Díez-Fernández, A.; Moreno-Herráiz, N.; Pascual-Morena, C. Comparative effect of two types of physical exercise for the improvement of exercise capacity, diastolic function, endothelial function and arterial stiffness in participants with heart failure with preserved ejection fraction (ExIC-FEp study): Protocol for a randomized controlled trial. J. Clin. Med. 2023, 12, 3535. [Google Scholar] [CrossRef]
- Weiss, W.; Gohlisch, C.; Harsch-Gladisch, C.; Tölle, M.; Zidek, W.; van der Giet, M. Oscillometric estimation of central blood pressure: Validation of the Mobil-O-Graph in comparison with the SphygmoCor device. Blood Press. Monit. 2012, 17, 128–131. [Google Scholar] [CrossRef]
- Omboni, S.; Riva, I.; Giglio, A.; Caldara, G.; Groppelli, A.; Parati, G. Validation of the Omron M5-I, R5-I and HEM-907 automated blood pressure monitors in elderly individuals according to the International Protocol of the European Society of Hypertension. Blood Press. Monit. 2007, 12, 233–242. [Google Scholar] [CrossRef]
- Segers, P.; Rietzschel, E.R.; De Buyzere, M.L.; Vermeersch, S.J.; De Bacquer, D.; Van Bortel, L.M.; De Backer, G.; Gillebert, T.C.; Verdonck, P.R. Noninvasive (input) impedance, pulse wave velocity, and wave reflection in healthy middle-aged men and women. Hypertension 2007, 49, 1248–1255. [Google Scholar] [CrossRef]
- Najjar, S.S.; Scuteri, A.; Shetty, V.; Wright, J.G.; Muller, D.C.; Fleg, J.L.; Spurgeon, H.P.; Ferrucci, L.; Lakatta, E.G. Pulse wave velocity is an independent predictor of cardiovascular events and all-cause mortality in the Baltimore Longitudinal Study of Aging. J. Am. Coll. Cardiol. 2008, 51, 1404–1410. [Google Scholar] [CrossRef]
- Kim, H.L.; Kim, S.H. Pulse wave velocity in atherosclerosis. Front. Cardiovasc. Med. 2019, 6, 41. [Google Scholar] [CrossRef]
- Greenwald, S.E. Ageing of the conduit arteries. J. Pathol. 2007, 211, 157–172. [Google Scholar] [CrossRef]
- Mozzini, C.; Casadei, A.; Roscia, G.; Cominacini, L. Young smoker “ABCD” vascular assessment: A four-step ultrasound examination for detecting peripheral, extra and intra-cranial early arterial damage. BMC Cardiovasc. Disord. 2016, 16, 147. [Google Scholar] [CrossRef]
- Steptoe, A.; Kivimäki, M. Stress and cardiovascular disease. Nat. Rev. Cardiol. 2012, 9, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Hart, E.C.; Charkoudian, N.; Wallin, B.G.; Curry, T.B.; Eisenach, J.H.; Joyner, M.J. Sex and ageing differences in resting arterial pressure regulation: The role of the β-adrenergic receptors. J. Physiol. 2011, 589 Pt 21, 5285–5297. [Google Scholar] [CrossRef]
- Redfield, M.M.; Jacobsen, S.J.; Borlaug, B.A.; Rodeheffer, R.J.; Kass, D.A. Age- and gender-related ventricular-vascular stiffening: A community-based study. Circulation 2005, 112, 2254–2262. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Barnes, J.N.; Hart, E.C.; Wallin, B.G.; Charkoudian, N. Neural control of the circulation: How sex and age differences interact in humans. Compr. Physiol. 2015, 5, 193–215. [Google Scholar] [CrossRef]
- Moreau, K.L.; Hildreth, K.L.; Meditz, A.L.; Deane, K.D.; Kohrt, W.M. Endothelial function is impaired across the stages of the menopause transition in healthy women. J. Clin. Endocrinol. Metab. 2012, 97, 4692–4700. [Google Scholar] [CrossRef] [PubMed]
- Xiang, D.; Liu, Y.; Zhou, S.; Zhou, E.; Wang, Y. Protective effects of estrogen on cardiovascular disease mediated by oxidative stress. Oxid. Med. Cell Longev. 2021, 2021, 5523516. [Google Scholar] [CrossRef]
- Lu, J.; Yin, L. Sex differences in left ventricular stroke work and cardiac power output per unit myocardium relate to blood pressure in apparently healthy adults. PLoS ONE 2023, 18, e0280143. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Su, L.; Lang, M. A systematic review and meta-analysis of sex differences in clinical outcomes of hypertrophic cardiomyopathy. Front. Cardiovasc. Med. 2023, 10, 1252266. [Google Scholar] [CrossRef]
- Gomez-Sanchez, M.; Gomez-Sanchez, L.; Patino-Alonso, M.C.; Cunha, P.G.; Recio-Rodriguez, J.I.; Alonso-Dominguez, R.; Sanchez-Aguadero, N.; Rodriguez-Sanchez, E.; Maderuelo-Fernandez, J.A.; Garcia-Ortiz, L.; et al. Vascular aging and its relationship with lifestyles and other risk factors in the general Spanish population: Early Vascular Ageing Study. J. Hypertens. 2020, 38, 1110–1122. [Google Scholar] [CrossRef] [PubMed]
- Purohit, A.; Kim, Y.J.; Michos, E.D. Cardiovascular disease prevention in women: The current state in 2023. Curr. Opin. Cardiol. 2024, 39, 54–60. [Google Scholar] [CrossRef]
- National Heart Foundation of Australia. Australian Guideline for Assessing and Managing Cardiovascular Disease Risk. 2023. Available online: https://www.heartfoundation.org.au/for-professionals/guideline-for-managing-cvd (accessed on 28 April 2025).
- Arnold, A.P.; Cassis, L.A.; Eghbali, M.; Reue, K.; Sandberg, K. Sex hormones and sex chromosomes cause sex differences in the development of cardiovascular diseases. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 746–756. [Google Scholar] [CrossRef]
- Asunción-Alvarez, D.; Palacios, J.; Ybañez-Julca, R.O.; Rodriguez-Silva, C.N.; Nwokocha, C.; Cifuentes, F.; Greensmith, D.J. Calcium signaling in endothelial and vascular smooth muscle cells: Sex differences and the influence of estrogens and androgens. Am. J. Physiol. Heart Circ. Physiol. 2024, 326, H950–H970. [Google Scholar] [CrossRef] [PubMed]
- Weber, T.; Wassertheurer, S.; Rammer, M.; Haiden, A.; Hametner, B.; Eber, B. Validation of a brachial cuff-based method for estimating central systolic blood pressure. Hypertension 2011, 58, 825–832. [Google Scholar] [CrossRef]
- Tokioka, S.; Nakaya, N.; Nakaya, K.; Takase, M.; Kogure, M.; Hatanaka, R.; Chiba, I.; Kanno, I.; Nochioka, K.; Metoki, H.; et al. Association of central blood pressure and carotid intima media thickness with new-onset hypertension in people with high normal blood pressure. J. Atheroscler. Thromb. 2023, 30, 1905–1916. [Google Scholar] [CrossRef]
- Mann, C.J. Observational research methods. Research design II: Cohort, cross sectional, and case-control studies. Emerg. Med. J. 2003, 20, 54–60. [Google Scholar] [CrossRef]
- Heidari, S.; Babor, T.F.; De Castro, P.; Tort, S.; Curno, M. Sex and gender equity in research: Rationale for the SAGER guidelines and recommended use. Res. Integr. Peer Rev. 2016, 1, 2. [Google Scholar] [CrossRef]
- Seals, D.R.; Desouza, C.A.; Donato, A.J.; Tanaka, H. Habitual exercise and arterial aging. J. Appl. Physiol. (1985) 2008, 105, 1323–1332. [Google Scholar] [CrossRef] [PubMed]
- van der Meer, I.M.; Bots, M.L.; Hofman, A.; del Sol, A.I.; van der Kuip, D.A.; Witteman, J.C. Predictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: The Rotterdam Study. Circulation 2004, 109, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Ferdinand, K.C.; Nasser, S.A. Racial/ethnic disparities in prevalence and care of patients with type 2 diabetes mellitus. Curr. Med. Res. Opin. 2015, 31, 913–923. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variable | Men | Women | Cohen’s d | p-Value | |
|---|---|---|---|---|---|
| n = 260 | n = 409 | ||||
| Demographic, anthropometric, and socioeconomic variables | |||||
| Age (years) | Median (IQR) | 49.00 (38.00–61.00) | 48.00 (36.00–58.00) | 0.13 (−0.03–0.28) | 0.113 |
| Mean (SD) | 49.61 (16.80) | 47.39 (17.83) | |||
| Weight (kg) | Median (IQR) | 80.53 (73.29–89.54) | 66.45 (56.65–74.05) | 1.13 (0.96–1.30) | <0.001 |
| Mean (SD) | 82.02 (14.25) | 66.28 (13.75) | |||
| Height (cm) | Median (IQR) | 174.05 (168.74–178.38) | 161.05 (156.15–165.40) | 1.68 (1.50–1.86) | <0.001 |
| Mean (SD) | 173.76 (8.12) | 160.66 (7.58) | |||
| BMI (kg/m2) | Median (IQR) | 26.71 (24.20–29.40) | 24.84 (21.68–23.03) | 0.30 (0.15–0.46) | <0.001 |
| Mean (SD) | 27.18 (4.44) | 25.70 (5.19) | |||
| Waist Circumference (cm) | Median (IQR) | 92.55 (84.19–102.59) | 81.35 (70.80–90.55) | 0.86 (0.70–1.02) | <0.001 |
| Mean (SD) | 94.14 (14.45) | 82.00 (13.94) | |||
| Education Level | |||||
| Cannot read or write | n (%) | 0 (0.0) | 2 (100.0) | - | 0.308 |
| No education | n (%) | 10 (32.3) | 21 (67.7) | ||
| Elementary education | n (%) | 24 (53.3) | 21 (46.7) | ||
| School graduate | n (%) | 46 (37.4) | 77 (62.6) | ||
| High school education | n (%) | 74 (38.9) | 116 (61.1) | ||
| University degree completed | 106 (38.1) | 172 (61.9) | |||
| Employment Status (n, %) | |||||
| Householder | n (%) | 3 (6.4) | 44 (93.6) | - | <0.001 |
| Student | n (%) | 23 (28.8) | 57 (71.2) | ||
| Unemployed | n (%) | 56 (56.6) | 43 (43.4) | ||
| Employee | n (%) | 128 (35.7) | 231 (64.3) | ||
| Self-employed worker or business owner | n (%) | 50 (59.5) | 34 (40.5) | ||
| Family History of myocardial infarction | |||||
| Yes | n (%) | 74 (43.8) | 95 (56.2) | - | 0.153 |
| No | n (%) | 186 (37.2) | 314 (62.8) | ||
| Family History of Stroke | |||||
| Yes | n (%) | 31 (25.6) | 90 (74.4) | - | 0.001 |
| No | n (%) | 229 (41.8) | 319 (58.2) | ||
| Smoking status | |||||
| Yes | n (%) | 34 (37.0) | 58 (63.0) | - | 0.031 |
| Ex-smoker, 0–1 year | n (%) | 8 (38.1) | 13 (61.9) | ||
| Ex-smoker, 1–5 years | n (%) | 12 (48.0) | 13 (52.0) | ||
| Ex-smoker, >5 years | n (%) | 65 (50.4) | 64 (49.6) | ||
| Non-smoker | n (%) | 141 (35.1) | 261 (64.9) | ||
| Blood pressure parameters | |||||
| Central systolic blood pressure (mmHg) | Median (IQR) | 124.00 (120.00–136.00) | 117.00 (107.00–125.00) | 0.60 (0.44–0.76) | <0.001 |
| Mean (SD) | 127.27 (13.90) | 118.09 (16.24) | |||
| Peripheral systolic blood pressure (mmHg) | Median (IQR) | 126.00 (117.00–136.62) | 113.00 (105.00–126.00) | 0.63 (0.47–0.79) | <0.001 |
| Mean (SD) | 127.48 (14.86) | 116.93 (17.70) | |||
| Central diastolic blood pressure (mmHg) | Median (IQR) | 79.50 (77.00–89.00) | 76.00 (68.00–80.00) | 0.63 (0.47–0.78) | <0.001 |
| Mean (SD) | 81.58 (10.22) | 75.25 (10.05) | |||
| Peripheral diastolic blood pressure (mmHg) | Median (IQR) | 73.00 (66.00–80.50) | 70.00 (63.00–77.00) | 0.27 (0.12–0.43) | <0.001 |
| Mean (SD) | 73.53 (10.50) | 70.59 (10.87) | |||
| Central pulse pressure (mmHg) | Median (IQR) | 42.00 (40.00–51.00) | 42.00 (35.00–48.00) | 0.24 (0.08–0.39) | <0.001 |
| Mean (SD) | 45.57 (11.64) | 42.73 (12.17) | |||
| Peripheral pulse pressure (mmHg) | Median (IQR) | 52.75 (47.00–58.25) | 44.00 (38.00–52.00) | 0.65 (0.50–0.81) | <0.001 |
| Mean (SD) | 53.95 (10.47) | 46.38 (12.21) | |||
| Vascular parameters | |||||
| Pulse wave velocity (m/s) | Median (IQR) | 7.00 (5.90–8.90) | 6.70 (5.20–8.10) | 0.16 (0.00–0.32) | 0.003 |
| Mean (SD) | 7.54 (2.15) | 7.17 (2.41) | |||
| AIx75 (%) | Median (IQR) | 13.00 (4.00–21.00) | 24.00 (16.00–32.00) | −0.85 (−1.01–−0.69) | <0.001 |
| Mean (SD) | 13.20 (12.17) | 23.29 (11.74) | |||
| Cardiac output (L/min) | Median (IQR) | 5.00 (4.50–5.50) | 4.40 (4.00–5.00) | 0.70 (0.54–0.86) | <0.001 |
| Mean (SD) | 5.01 (0.76) | 4.50 (0.71) | |||
| Stroke volume (mL) | Median (IQR) | 76.50 (67.70–85.85) | 63.60 (56.10–72.30) | 0.86 (0.70–1.02) | <0.001 |
| Mean (SD) | 77.27 (15.49) | 65.24 (13.02) | |||
| Peripheral vascular resistance (din-seg-m2/cm5) | Median (IQR) | 1651.85 (1451.50–1834.00) | 1716.80 (1570.20–1869.90) | −0.41 (−0.57–−0.25) | 0.002 |
| Mean (SD) | 1641.22 (261.03) | 1707.88 (10.05) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saz-Lara, A.; Martínez-Rodrigo, A.; Galán-Moya, E.M.; Martínez-García, I.; Otero-Luis, I.; Lever-Megina, C.G.; Moreno-Herraiz, N.; Cavero-Redondo, I. Sex-Specific Patterns in Blood Pressure and Vascular Parameters: The MUJER-EVA Project. J. Cardiovasc. Dev. Dis. 2025, 12, 175. https://doi.org/10.3390/jcdd12050175
Saz-Lara A, Martínez-Rodrigo A, Galán-Moya EM, Martínez-García I, Otero-Luis I, Lever-Megina CG, Moreno-Herraiz N, Cavero-Redondo I. Sex-Specific Patterns in Blood Pressure and Vascular Parameters: The MUJER-EVA Project. Journal of Cardiovascular Development and Disease. 2025; 12(5):175. https://doi.org/10.3390/jcdd12050175
Chicago/Turabian StyleSaz-Lara, Alicia, Arturo Martínez-Rodrigo, Eva María Galán-Moya, Irene Martínez-García, Iris Otero-Luis, Carla Geovanna Lever-Megina, Nerea Moreno-Herraiz, and Iván Cavero-Redondo. 2025. "Sex-Specific Patterns in Blood Pressure and Vascular Parameters: The MUJER-EVA Project" Journal of Cardiovascular Development and Disease 12, no. 5: 175. https://doi.org/10.3390/jcdd12050175
APA StyleSaz-Lara, A., Martínez-Rodrigo, A., Galán-Moya, E. M., Martínez-García, I., Otero-Luis, I., Lever-Megina, C. G., Moreno-Herraiz, N., & Cavero-Redondo, I. (2025). Sex-Specific Patterns in Blood Pressure and Vascular Parameters: The MUJER-EVA Project. Journal of Cardiovascular Development and Disease, 12(5), 175. https://doi.org/10.3390/jcdd12050175