
The Dilemma of Surgical Timing in Acute Aortic Valve Endocarditis: Does Early Surgery Improve Risks or Prognosis?

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Definitions, Endpoints and Follow-Up
2.3. Statistical Analysis
3. Results
3.1. Preoperative
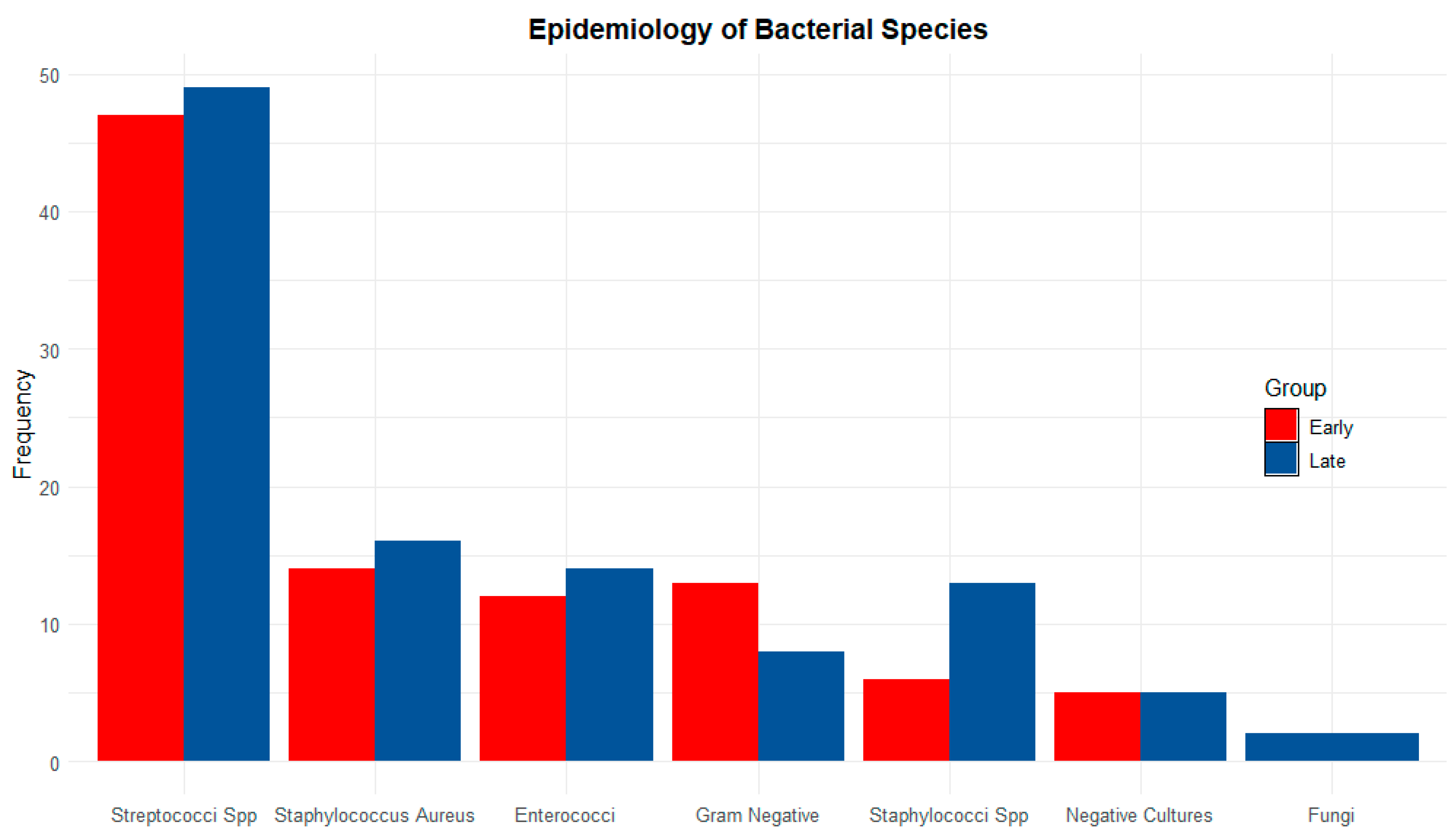
3.2. Causative Microorganism
3.3. Surgical Technique
3.4. Perioperative (In-Hospital Course)
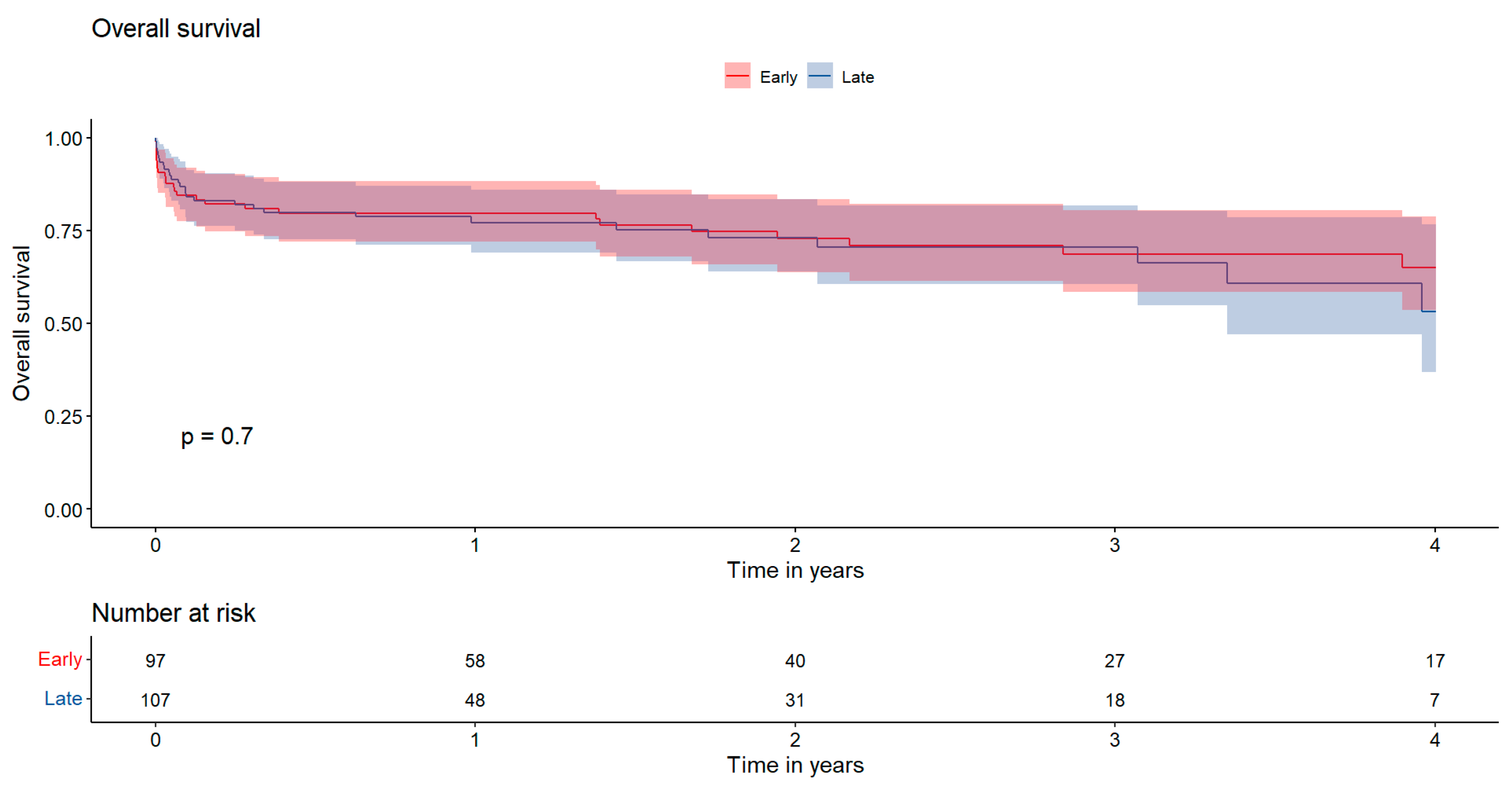
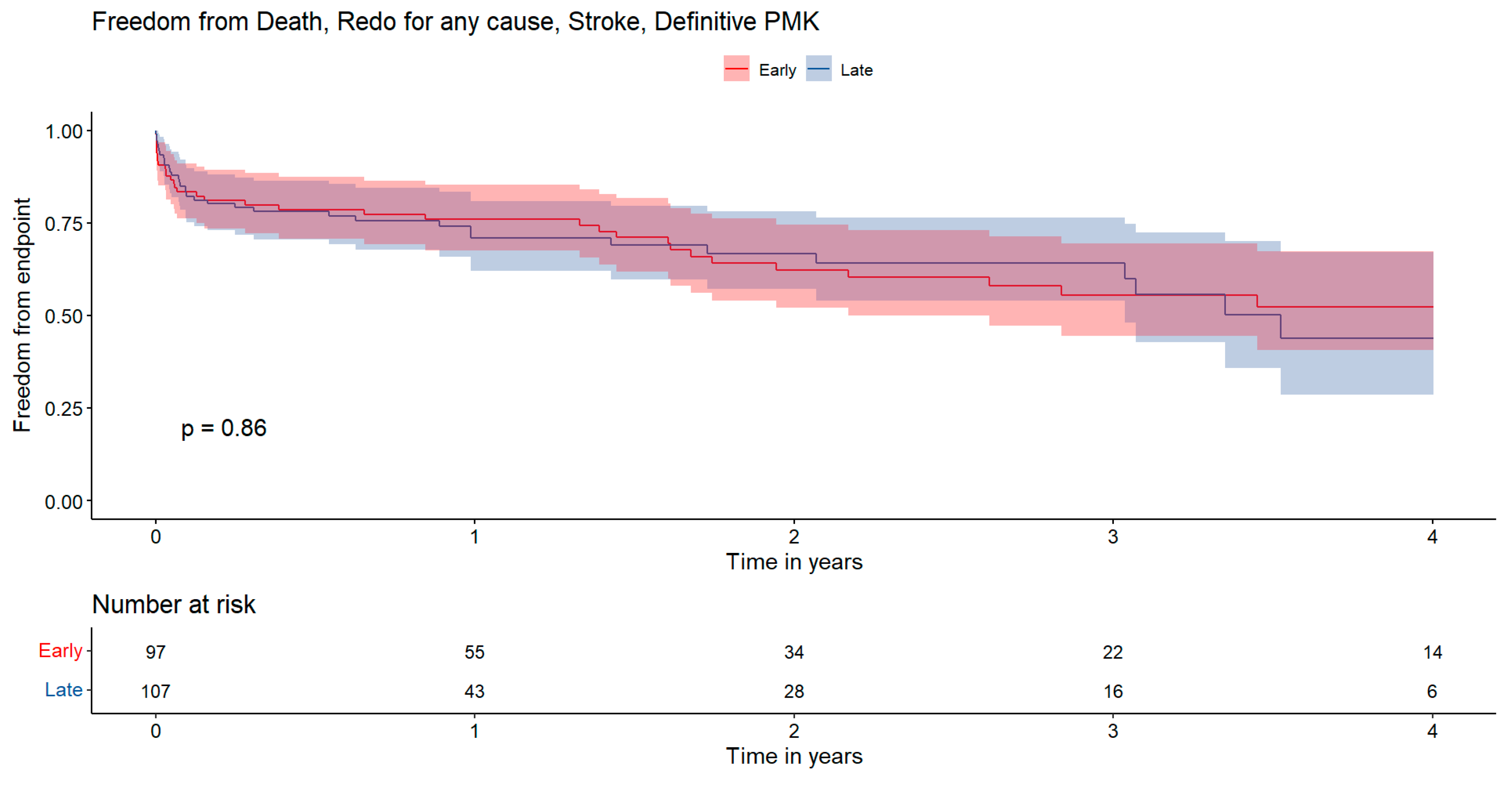
3.5. Follow-Up (Out-Hospital Course)
3.6. Logistic Regression
4. Discussion
- In-hospital mortality was not influenced by timing, with both early and late surgery groups showing a mortality rate of 16%.
- A higher incidence of permanent pacemaker implantation was observed in patients who experienced delays before surgery.
- Early surgery after a short course of antibiotics is sufficient for local sterilization and does not increase the risk of endocarditis recurrence.
- Predictors of adverse outcomes at 1 year after surgery include preoperative chronic kidney disease, presence of annular abscess, postoperative ECMO, and prolonged mechanical assisted ventilation. Additionally, PCR values and cardiopulmonary bypass duration are also linked to adverse outcomes, while factors such as surgical timing do not affect survival.
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AF | Atrial Fibrillation |
| AVR | Aortic Valve Replacement |
| BMI | Body Mass Index |
| BSA | Body Surface Area |
| CABG | Coronary Artery Bypass Grafting |
| CC | Cross-Clamping |
| CKD | Chronic Kidney Disease |
| CPB | Cardiopulmonary Bypass |
| CPOD | Chronic Pulmonary Obstructive Disease |
| CRP | C-Reactive Protein |
| CVE | Cerebrovascular Event |
| ECMO | Extracorporeal Membrane Oxygenation |
| ESC | European Society of Cardiology |
| IE | Infective Endocarditis |
| IABP | Intra-Aortic Balloon Pump |
| KDIGO | Kidney Disease Improving Global Outcomes |
| LVEF | Left Ventricular Ejection Fraction |
| MACCEs | Major Adverse Cardiac and Cerebrovascular Events |
| MAV | Mechanical Assisted Ventilation |
| MRI | Magnetic Resonance Imaging |
| NYHA | New York Heart Association |
| PET | Positron Emission Tomography |
| PMK | Permanent Pacemaker |
| PV | Prosthetic Valve |
| sPAP | Systolic Pulmonary Arterial Pressure |
References
- Cahill, T.J.; Prendergast, B.D. Infective Endocarditis. Lancet 2016, 387, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Dayer, M.J.; Jones, S.; Prendergast, B.; Baddour, L.M.; Lockhart, P.B.; Thornhill, M.H. Incidence of Infective Endocarditis in England, 2000–2013: A Secular Trend, Interrupted Time-Series Analysis. Lancet 2015, 385, 1219–1228. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the Management of Infective Endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC)Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.; Ajmone Marsan, N.; De Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; et al. 2023 ESC Guidelines for the Management of Endocarditis. Eur. Heart J. 2023, 44, 3948–4042. [Google Scholar] [CrossRef]
- Aranki, S.F.; Santini, F.; Adams, D.H.; Rizzo, R.J.; Couper, G.S.; Kinchla, N.M.; Gildea, J.S.; Collins, J.J.; Cohn, L.H. Aortic Valve Endocarditis. Determinants of Early Survival and Late Morbidity. Circulation 1994, 90, II175–II182. [Google Scholar]
- Renzulli, A.; Carozza, A.; Romano, G.; De Feo, M.; Della Corte, A.; Gregorio, R.; Cotrufo, M. Recurrent Infective Endocarditis: A Multivariate Analysis of 21 Years of Experience. Ann. Thorac. Surg. 2001, 72, 39–43. [Google Scholar] [CrossRef]
- Hill, E.E.; Herijgers, P.; Herregods, M.-C.; Peetermans, W.E. Evolving Trends in Infective Endocarditis. Clin. Microbiol. Infect. 2006, 12, 5–12. [Google Scholar] [CrossRef]
- Di Bacco, L.; D’Alonzo, M.; Di Mauro, M.; Petruccelli, R.D.; Baudo, M.; Palacios, C.M.; Benussi, S.; Muneretto, C.; Rosati, F. Mitral Valve Surgery in Acute Infective Endocarditis: Long-Term Outcomes of Mitral Valve Repair versus Replacement. J. Cardiovasc. Med. 2023, 25, 30–37. [Google Scholar] [CrossRef]
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical Presentation, Aetiology and Outcome of Infective Endocarditis. Results of the ESC-EORP EURO-ENDO (European Infective Endocarditis) Registry: A Prospective Cohort Study. Eur. Heart J. 2019, 40, 3222–3232. [Google Scholar] [CrossRef]
- Lalani, T. In-Hospital and 1-Year Mortality in Patients Undergoing Early Surgery for Prosthetic Valve Endocarditis. JAMA Intern. Med. 2013, 173, 1495. [Google Scholar] [CrossRef]
- Liang, F.; Song, B.; Liu, R.; Yang, L.; Tang, H.; Li, Y. Optimal Timing for Early Surgery in Infective Endocarditis: A Meta-Analysis. Interact. Cardiovasc. Thorac. Surg. 2016, 22, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Anantha Narayanan, M.; Mahfood Haddad, T.; Kalil, A.C.; Kanmanthareddy, A.; Suri, R.M.; Mansour, G.; Destache, C.J.; Baskaran, J.; Mooss, A.N.; Wichman, T.; et al. Early versus Late Surgical Intervention or Medical Management for Infective Endocarditis: A Systematic Review and Meta-Analysis. Heart 2016, 102, 950–957. [Google Scholar] [CrossRef]
- Mihos, C.G.; Pineda, A.M.; Santana, O. A Meta-Analysis of Early versus Delayed Surgery for Valvular Infective Endocarditis Complicated by Embolic Ischemic Stroke. Innov. Technol. Technol. Cardiothorac. Vasc. Surg. 2016, 11, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Chu, V.H.; Athan, E.; Delahaye, F.; Freiberger, T.; Lamas, C.; Miro, J.M.; Strahilevitz, J.; Tribouilloy, C.; Durante-Mangoni, E.; et al. Association between the Timing of Surgery for Complicated, Left-Sided Infective Endocarditis and Survival. Am. Heart J. 2019, 210, 108–116. [Google Scholar] [CrossRef]
- Kang, D.-H.; Kim, Y.-J.; Kim, S.-H.; Sun, B.J.; Kim, D.-H.; Yun, S.-C.; Song, J.-M.; Choo, S.J.; Chung, C.-H.; Song, J.-K.; et al. Early Surgery versus Conventional Treatment for Infective Endocarditis. N. Engl. J. Med. 2012, 366, 2466–2473. [Google Scholar] [CrossRef]
- Kiefer, T.; Park, L.; Tribouilloy, C.; Cortes, C.; Casillo, R.; Chu, V.; Delahaye, F.; Durante-Mangoni, E.; Edathodu, J.; Falces, C.; et al. Association Between Valvular Surgery and Mortality Among Patients With Infective Endocarditis Complicated by Heart Failure. JAMA 2011, 306, 2239–2247. [Google Scholar] [CrossRef]
- Hill, T.E.; Kiehl, E.L.; Shrestha, N.K.; Gordon, S.M.; Pettersson, G.B.; Mohan, C.; Hussein, A.; Hussain, S.; Wazni, O.; Wilkoff, B.L.; et al. Predictors of Permanent Pacemaker Requirement after Cardiac Surgery for Infective Endocarditis. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 329–334. [Google Scholar] [CrossRef]
- Thuny, F.; Beurtheret, S.; Mancini, J.; Gariboldi, V.; Casalta, J.-P.; Riberi, A.; Giorgi, R.; Gouriet, F.; Tafanelli, L.; Avierinos, J.-F.; et al. The Timing of Surgery Influences Mortality and Morbidity in Adults with Severe Complicated Infective Endocarditis: A Propensity Analysis. Eur. Heart J. 2011, 32, 2027–2033. [Google Scholar] [CrossRef]
- Hoen, B. Changing Profile of Infective EndocarditisResults of a 1-Year Survey in France. JAMA 2002, 288, 75. [Google Scholar] [CrossRef]
- Della Corte, A.; Di Mauro, M.; Actis Dato, G.; Barili, F.; Cugola, D.; Gelsomino, S.; Santè, P.; Carozza, A.; Della Ratta, E.; Galletti, L.; et al. Surgery for Prosthetic Valve Endocarditis: A Retrospective Study of a National Registry†. Eur. J. Cardiothorac. Surg. 2017, 52, 105–111. [Google Scholar] [CrossRef]
- D’Alonzo, M.; Chabry, Y.; Melica, G.; Gallien, S.; Lim, P.; Aouate, D.; Huguet, R.; Galy, A.; Lepeule, R.; Fihman, V.; et al. Reintervention for Acute Aortic Prosthesis Endocarditis: Early and Mid-Term Outcomes. J. Clin. Med. 2024, 13, 7690. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Felix, B.M.; Barca, L.V.; Garcia-Esquinas, E.; Correa-Pérez, A.; Fernández-Hidalgo, N.; Muriel, A.; Lopez-Alcalde, J.; Álvarez-Diaz, N.; Pijoan, J.I.; Ribera, A.; et al. Prognostic Models for Mortality after Cardiac Surgery in Patients with Infective Endocarditis: A Systematic Review and Aggregation of Prediction Models. Clin. Microbiol. Infect. 2021, 27, 1422–1430. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Overall (204 pts) | Early (97 pts) | Late (107 pts) | p-Value | |
|---|---|---|---|---|
| Delay, days | 8.0 [3.0–16.0] | 3.0 [2.0–4.0] | 15.0 [10.0–25.5] | <0.001 |
| Age, years old | 68.3 [60.0–75.0] | 67.0 [58.0–75.0] | 69.0 [62.0–75.0] | 0.3 |
| Gender, male | 169 (83%) | 79 (81%) | 90 (84%) | 0.6 |
| BSA, m2 | 1.9 ± 0.2 | 1.9 ± 0.2 | 1.9 ± 0.2 | 0.7 |
| BMI, Kg/m2 | 26.5 ± 5.6 | 26.6 ± 5.7 | 26.4 ± 5.5 | 0.9 |
| Drug abuser | 4 (2.0%) | 1 (1.0%) | 3 (2.8%) | 0.6 |
| Hypertension | 121 (59%) | 53 (55%) | 68 (64%) | 0.2 |
| CPOD | 15 (7.4%) | 6 (6.2%) | 9 (8.4%) | 0.5 |
| CKD | 40 (20%) | 17 (18%) | 23 (21%) | 0.5 |
| Dialysis | 5 (2.5%) | 3 (3.1%) | 2 (1.9%) | 0.7 |
| NYHA III-IV | 63 (31%) | 35 (36%) | 28 (26%) | 0.13 |
| Nosocomial Infection | 5 (2.5%) | 2 (2.1%) | 3 (2.8%) | >0.9 |
| Fever | 160 (78%) | 74 (76%) | 86 (80%) | 0.5 |
| Cardiogenic Shock | 10 (4.9%) | 5 (5.2%) | 5 (4.7%) | >0.9 |
| Previous CVE | 56 (27%) | 25 (26%) | 31 (29%) | 0.6 |
| Splenic Abscess | 33 (16%) | 17 (18%) | 16 (15%) | 0.6 |
| Overall (204 pts) | Early (97 pts) | Late (107 pts) | p-Value | |
|---|---|---|---|---|
| AV prosthesis | 65 (32%) | 26 (27%) | 39 (36%) | 0.14 |
| Mitral valve involvement | 53 (26%) | 30 (31%) | 23 (21%) | 0.12 |
| Large Vegetation * | 165 (81%) | 85 (88%) | 80 (75%) | 0.02 |
| Annular Abscess | 76 (37%) | 34 (35%) | 42 (39%) | 0.5 |
| Fistula | 8 (3.9%) | 4 (4.1%) | 4 (3.7%) | >0.9 |
| LVEF | 57.0 [55.0–64.0] | 55.0 [53.0–63.0] | 58.0 [55.0–64.0] | 0.4 |
| sPAP | 30.0 [28.0–32.3] | 30.0 [28.0–31.0] | 30.0 [28.0–33.0] | 0.7 |
| Haemoglobin, g/dL | 10.5 [9.3–11.8] | 10.6 [9.4–11.6] | 10.3 [9.3–11.9] | 0.6 |
| White Blood Cells,·1/µL | 9.6 [6.7–12.2] | 10.2 [7.7–12.5] | 8.7 [6.4–11.7] | 0.049 |
| Serum Albumin Level, g/dL | 2.8 [2.4–3.3] | 2.7 [2.4–3.1] | 2.9 [2.4–3.4] | 0.4 |
| Peak C-Reactive Protein Level, ng/dL | 94.8 [55.5–145.3] | 93.0 [59.5–152.2] | 95.0 [44.6–133.7] | 0.2 |
| Overall (204 pts) | Early (97 pts) | Late (107 pts) | p-Value | |
|---|---|---|---|---|
| Biological AVR | 178 (87%) | 87 (90%) | 91 (85%) | 0.3 |
| Mechanical AVR | 9 (4.4%) | 5 (5.2%) | 4 (3.7%) | 0.7 |
| Homograft | 12 (5.9%) | 3 (3.1%) | 9 (8.4%) | 0.11 |
| Root/Bentall surgery | 14 (6.9%) | 7 (7.2%) | 7 (6.5%) | 0.8 |
| Associated CABG | 13 (6.4%) | 6 (6.2%) | 7 (6.5%) | >0.9 |
| Associated Mitral surgery | 50 (25%) | 25 (26%) | 25 (23%) | 0.7 |
| Other associated procedures * | 22 (11%) | 9 (9.3%) | 13 (12%) | 0.5 |
| CPB Time, min | 134.5 [97.8–194.3] | 124.0 [97.0–196.0] | 140.0 [99.5–192.0] | 0.5 |
| Aortic CC Time, min | 107.0 [80.0–149.5] | 104.0 [77.0–149.0] | 109.0 [82.0–149.5] | 0.5 |
| Overall (204 pts) | Early (97 pts) | Late (107 pts) | p-Value | |
|---|---|---|---|---|
| IABP | 11 (5.4%) | 3 (3.1%) | 8 (7.5%) | 0.2 |
| ECMO | 13 (6.4%) | 7 (7.2%) | 6 (5.6%) | 0.6 |
| MAV > 48 h | 33 (16%) | 14 (14%) | 19 (18%) | 0.5 |
| Bleeding | 6 (2.9%) | 4 (4.1%) | 2 (1.9%) | 0.4 |
| Sternal Wound Infections | 8 (3.9%) | 4 (4.1%) | 4 (3.7%) | >0.9 |
| Postoperative AF | 62 (30%) | 23 (24%) | 39 (36%) | 0.048 |
| Postoperative Stroke | 3 (1.5%) | 1 (1.0%) | 2 (1.9%) | >0.9 |
| KDIGO | 0.6 | |||
| No Renal impairment | 141 (69%) | 67 (69%) | 74 (69%) | |
| Stage 1 | 21 (10%) | 11 (11%) | 10 (9.3%) | |
| Stage 2 | 22 (11%) | 8 (8.2%) | 14 (13%) | |
| Stage 3 | 20 (9.8%) | 11 (11%) | 9 (8.4%) | |
| Definitive PMK | 25 (12%) | 8 (8.2%) | 17 (16%) | 0.10 |
| Hospital length of stay | 18.0 [12.0–27.3] | 18.0 [12.0–26.0] | 19.0 [10.5–28.5] | 0.8 |
| In-Hospital Death | 33 (16%) | 16 (16%) | 17 (16%) | >0.9 |
| Death at 1 Year | 42 (21%) | 19 (20%) | 23 (21%) | 0.7 |
| Overall (171 pts) | Early (81 pts) | Late (90 pts) | p-Value | |
|---|---|---|---|---|
| Any kind of IE (operated and not operated) | 21 (12%) | 11 (14%) | 10 (11%) | 0.6 |
| Not operated IE relapse | 12 (7.0%) | 6 (7.4%) | 6 (6.7%) | 0.8 |
| Redo for IE relapse | 9 (5.3%) | 5 (6.2%) | 4 (4.4%) | 0.7 |
| New CVE | 5 (2.9%) | 2 (2.5%) | 3 (3.3%) | >0.9 |
| Death at last follow-up | 28 (16%) | 15 (19%) | 13 (14%) | 0.5 |
| Covariate | Odds Ratio | 95%CI Lower | 95%CI Upper | p-Value |
|---|---|---|---|---|
| Timing (early surgery) | 1.12 | 0.57 | 2.24 | 0.74 |
| Age | 1.02 | 1.00 | 1.06 | 0.12 |
| Gender (male) | 0.70 | 0.31 | 1.71 | 0.41 |
| BSA | 0.96 | 0.20 | 4.43 | 0.96 |
| CPOD | 2.83 | 0.90 | 8.38 | 0.06 |
| CKD | 2.62 | 1.20 | 5.60 | 0.01 |
| AV prosthesis | 1.24 | 0.60 | 2.52 | 0.55 |
| Cardiogenic Shock | 1.70 | 0.35 | 6.44 | 0.46 |
| Large Vegetation | 0.50 | 0.23 | 1.12 | 0.08 |
| Annular Abscess | 2.49 | 1.25 | 5.01 | 0.01 |
| Multiple Valve Involvement | 0.99 | 0.41 | 2.19 | 0.98 |
| Pulmonary Hypertension | 1.91 | 0.85 | 4.14 | 0.10 |
| CVE | 1.24 | 0.58 | 2.57 | 0.57 |
| Splenic Abscess | 1.05 | 0.39 | 2.50 | 0.92 |
| Staphylococcus Aureus | 2.10 | 0.87 | 4.81 | 0.09 |
| PCR | 1.00 | 1.00 | 1.01 | 0.02 |
| CPB | 1.01 | 1.00 | 1.01 | 0.00 |
| ECMO | 16.56 | 4.77 | 76.99 | 0.00 |
| MAV > 48 h | 7.35 | 3.29 | 16.78 | 0.00 |
| KDIGO | — | — | ||
| Stage 1 | 1.60 | 0.49 | 4.57 | 0.4 |
| Stage 2 | 2.39 | 0.84 | 6.38 | 0.088 |
| Stage 3 | 2.76 | 0.95 | 7.54 | 0.051 |
| Definitive PMK | 0.30 | 0.05 | 1.08 | 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Alonzo, M.; Di Bacco, L.; Fiore, A.; Baudo, M.; Zanin, F.; Baldelli, C.; Moini, C.; Folliguet, T.; Muneretto, C. The Dilemma of Surgical Timing in Acute Aortic Valve Endocarditis: Does Early Surgery Improve Risks or Prognosis? J. Cardiovasc. Dev. Dis. 2025, 12, 153. https://doi.org/10.3390/jcdd12040153
D’Alonzo M, Di Bacco L, Fiore A, Baudo M, Zanin F, Baldelli C, Moini C, Folliguet T, Muneretto C. The Dilemma of Surgical Timing in Acute Aortic Valve Endocarditis: Does Early Surgery Improve Risks or Prognosis? Journal of Cardiovascular Development and Disease. 2025; 12(4):153. https://doi.org/10.3390/jcdd12040153
Chicago/Turabian StyleD’Alonzo, Michele, Lorenzo Di Bacco, Antonio Fiore, Massimo Baudo, Francesca Zanin, Chiara Baldelli, Cyrus Moini, Thierry Folliguet, and Claudio Muneretto. 2025. "The Dilemma of Surgical Timing in Acute Aortic Valve Endocarditis: Does Early Surgery Improve Risks or Prognosis?" Journal of Cardiovascular Development and Disease 12, no. 4: 153. https://doi.org/10.3390/jcdd12040153
APA StyleD’Alonzo, M., Di Bacco, L., Fiore, A., Baudo, M., Zanin, F., Baldelli, C., Moini, C., Folliguet, T., & Muneretto, C. (2025). The Dilemma of Surgical Timing in Acute Aortic Valve Endocarditis: Does Early Surgery Improve Risks or Prognosis? Journal of Cardiovascular Development and Disease, 12(4), 153. https://doi.org/10.3390/jcdd12040153