
The Prevalence and Impact of Atrial Fibrillation on Patients with Chronic Total Occlusions: Insights from the National Inpatient Sample


 ,
,  , ,
, ,
Abstract
1. Introduction
2. Methods
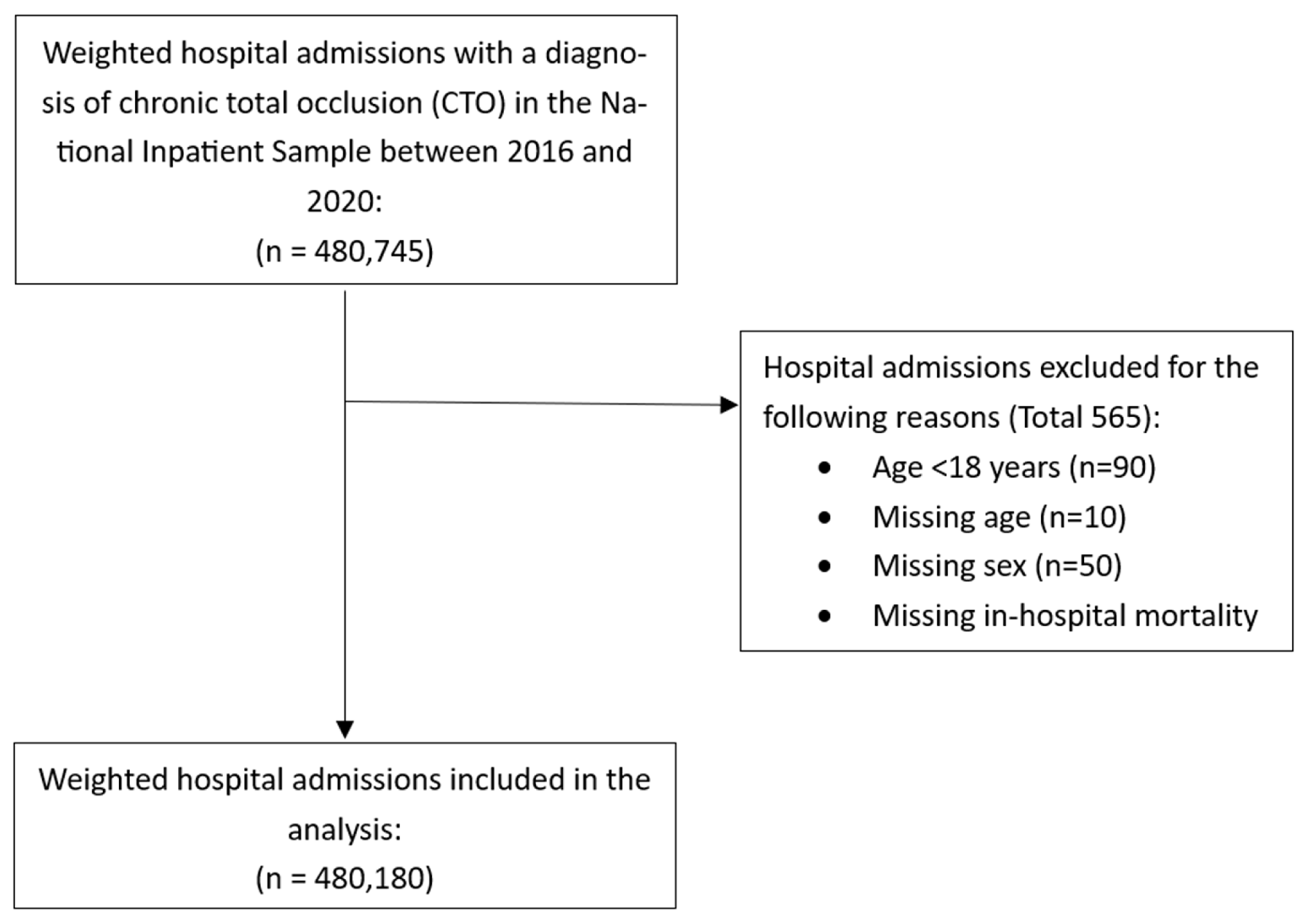
2.1. Study Design and Dataset
2.2. Variable Definition
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.C.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001, 285, 2370–2375. [Google Scholar] [CrossRef] [PubMed]
- Michniewicz, E.; Mlodawska, E.; Lopatowska, P.; Tomaszuk-Kazberuk, A.; Malyszko, J. Patients with atrial fibrillation and coronary artery disease—Double trouble. Adv. Med. Sci. 2018, 63, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Mekhael, M.; Marrouche, N.; Hajjar AHEl Donnellan, E. The relationship between atrial fibrillation and coronary artery disease: Understanding common denominators. Trends Cardiovasc. Med. 2022, 34, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Fefer, P.; Knudtson, M.L.; Cheema, A.N.; Galbraith, P.D.; Osherov, A.B.; Yalonetsky, S.; Gannot, S.; Samuel, M.; Weisbrod, M.; Bierstone, D.; et al. Current Perspectives on Coronary Chronic Total Occlusions: The Canadian Multicenter Chronic Total Occlusions Registry. J. Am. Coll. Cardiol. 2012, 59, 991–997. [Google Scholar] [CrossRef]
- Godino, C.; Giannattasio, A.; Scotti, A.; Baldetti, L.; Pivato, C.A.; Munafò, A.; Cappelletti, A.; Beneduce, A.; Melillo, F.; Chiarito, M.; et al. Risk of cardiac and sudden death with and without revascularisation of a coronary chronic total occlusion. Heart 2019, 105, 1096–1102. [Google Scholar] [CrossRef]
- van der Schaaf, R.J.; Vis, M.M.; Sjauw, K.D.; Koch, K.T.; Baan, J., Jr.; Tijssen, J.G.; de Winter, R.J.; Piek, J.J.; Henriques, J.P. Impact of multivessel coronary disease on long-term mortality in patients with ST-elevation myocardial infarction is due to the presence of a chronic total occlusion. Am. J. Cardiol. 2006, 98, 1165–1169. [Google Scholar] [CrossRef]
- Park, T.K.; Lee, S.H.; Choi, K.H.; Lee, J.M.; Yang, J.H.; Song, Y.B.; Hahn, J.Y.; Choi, J.H.; Gwon, H.C.; Lee, S.H.; et al. Late Survival Benefit of Percutaneous Coronary Intervention Compared With Medical Therapy in Patients with Coronary Chronic Total Occlusion: A 10-Year Follow-Up Study. J. Am. Heart Assoc. 2021, 10, e019022. [Google Scholar] [CrossRef]
- Galassi, A.R.; Brilakis, E.S.; Boukhris, M.; Tomasello, S.D.; Sianos, G.; Karmpaliotis, D.; Di Mario, C.; Strauss, B.H.; Rinfret, S.; Yamane, M.; et al. Appropriateness of percutaneous revascularization of coronary chronic total occlusions: An overview. Eur. Heart J. 2016, 37, 2692–2700. [Google Scholar] [CrossRef]
- Werner, G.S.; Martin-Yuste, V.; Hildick-Smith, D.; Boudou, N.; Sianos, G.; Gelev, V.; Rumoroso, J.R.; Erglis, A.; Christiansen, E.H.; Escaned, J.; et al. A randomized multicentre trial to compare revascularization with optimal medical therapy for the treatment of chronic total coronary occlusions cardiology. Eur. Heart J. 2018, 39, 2484–2493. [Google Scholar] [CrossRef]
- Brilakis, E.S.; Mashayekhi, K.; Tsuchikane, E.; Abi Rafeh, N.; Alaswad, K.; Araya, M.; Avran, A.; Azzalini, L.; Babunashvili, A.M.; Bayani, B.; et al. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention: A Global Expert Consensus Document. Circulation 2019, 140, 420–433. [Google Scholar] [CrossRef]
- Alexandrou, M.; Rempakos, A.; Kostantinis, S.; Simsek, B.; Karacsonyi, J.; Choi, J.W.; Poommipanit, P.; Khatri, J.J.; Young, L.; Davies, R.; et al. Atrial fibrillation and chronic total occlusion percutaneous coronary intervention outcomes: Insights from the Progress-CTO registry. J. Invasive Cardiol. 2023, 35, 20–26. [Google Scholar] [CrossRef]
- Stähli, B.E.; Gebhard, C.; Gick, M.; Mashayekhi, K.; Ferenc, M.; Buettner, H.J.; Neumann, F.J.; Toma, A. Outcomes of patients with periprocedural atrial fibrillation undergoing percutaneous coronary intervention for chronic total occlusion. Clin. Res. Cardiol. 2017, 106, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Råmunddal, T.; Hoebers, L.; Henriques, J.P.; Dworeck, C.; Angerås, O.; Odenstedt, J.; Ioanes, D.; Olivecrona, G.; Harnek, J.; Jensen, U.; et al. Chronic total occlusions in Sweden–a report from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR). PLoS ONE 2014, 9, e103850. [Google Scholar] [CrossRef]
- Lee, S.W.; Lee, P.H.; Ahn, J.M.; Park, D.W.; Yun, S.C.; Han, S.; Kang, H.; Kang, S.J.; Kim, Y.H.; Lee, C.W.; et al. Randomized Trial Evaluating Percutaneous Coronary Intervention for the Treatment of Chronic Total Occlusion: The DECISION-CTO Trial. Circulation 2019, 139, 1674–1683. [Google Scholar] [CrossRef]
- Shanmugasundaram, M.; Dhakal, B.P.; Murugapandian, S.; Hashemzadeh, M.; Paul, T.; Movahed, M.R. Outcomes of Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Analysis of National Inpatient Sample. Cardiovasc. Revasc. Med. 2020, 21, 14–19. [Google Scholar] [CrossRef]
- Garg, L.; Agrawal, S.; Agarwal, M.; Shah, M.; Garg, A.; Patel, B.; Agarwal, N.; Nanda, S.; Sharma, A.; Cox, D. Influence of Atrial Fibrillation on Outcomes in Patients Who Underwent Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction. Am. J. Cardiol. 2018, 121, 684–689. [Google Scholar] [CrossRef]
- Chung, M.K.; Eckhardt, L.L.; Chen, L.Y.; Ahmed, H.M.; Gopinathannair, R.; Joglar, J.A.; Noseworthy, P.A.; Pack, Q.R.; Sanders, P.; Trulock, K.M. Lifestyle and Risk Factor Modification for Reduction of Atrial Fibrillation: A Scientific Statement From the American Heart Association. Circulation 2020, 141, e750–e772. [Google Scholar] [CrossRef]
- Grymonprez, M.; Petrovic, M.; De Backer, T.L.; Steurbaut, S.; Lahousse, L. The Impact of Polypharmacy on the Effectiveness and Safety of Non-vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Thromb. Haemost. 2024, 124, 135–148. [Google Scholar] [CrossRef]
- Zheng, Y.; Li, S.; Liu, X.; Lip, G.Y.H.; Guo, L.; Zhu, W. Effect of Oral Anticoagulants in Atrial Fibrillation Patients with Polypharmacy: A Meta-analysis. Thromb. Haemost. 2023, 122, 166–177. [Google Scholar] [CrossRef]
- Romiti, G.F.; Proietti, M.; Bonini, N.; Ding, W.Y.; Boriani, G.; Huisman, M.V.; Lip, G.Y.; GLORIA-AF Investigators. Clinical Complexity Domains, Anticoagulation, and Outcomes in Patients with Atrial Fibrillation: A Report from the GLORIA-AF Registry Phase II and III. Thromb. Haemost. 2022, 122, 2030–2041. [Google Scholar] [CrossRef]
- Chao, T.F.; Joung, B.; Takahashi, Y.; Lim, T.W.; Choi, E.K.; Chan, Y.H.; Guo, Y.; Sriratanasathavorn, C.; Oh, S.; Okumura, K.; et al. 2021 Focused Update Consensus Guidelines of the Asia Pacific Heart Rhythm Society on Stroke Prevention in Atrial Fibrillation: Executive Summary. Thromb. Haemost. 2022, 122, 20–47. [Google Scholar] [CrossRef] [PubMed]
- Romiti, G.F.; Pastori, D.; Rivera-Caravaca, J.M.; Ding, W.Y.; Gue, Y.X.; Menichelli, D.; Gumprecht, J.; Kozieł, M.; Yang, P.S.; Guo, Y.; et al. Adherence to the “Atrial Fibrillation Better Care” Pathway in Patients with Atrial Fibrillation: Impact on Clinical Outcomes—A Systematic Review and Meta-Analysis of 285,000 Patients. Thromb. Haemost. 2022, 122, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Romiti, G.F.; Guo, Y.; Corica, B.; Proietti, M.; Zhang, H.; Lip, G.Y.H. Mobile Health-Technology-Integrated Care for Atrial Fibrillation: A Win Ratio Analysis from the mAFA-II Randomized Clinical Trial. Thromb. Haemost. 2023, 123, 1042–1048. [Google Scholar] [CrossRef]
- Gorog, D.A.; Gue, Y.X.; Chao, T.F.; Fauchier, L.; Ferreiro, J.L.; Huber, K.; Konstantinidis, S.V.; Lane, D.A.; Marin, F.; Oldgren, J.; et al. Assessment and Mitigation of Bleeding Risk in Atrial Fibrillation and Venous Thromboembolism: Executive Summary of a European and Asia-Pacific Expert Consensus Paper. Thromb. Haemost. 2022, 122, 1625–1652. [Google Scholar] [CrossRef]
- Simsek, B.; Gorgulu, S.; Kostantinis, S.; Karacsonyi, J.; Alaswad, K.; Jaffer, F.A.; Doshi, D.; Goktekin, O.; Kerrigan, J.; Haddad, E.; et al. Radial access for chronic total occlusion percutaneous coronary intervention: Insights from the PROGRESS-CTO registry. Catheter. Cardiovasc. Interv. 2022, 100, 730–736. [Google Scholar] [CrossRef]
- Packer, M.; Lam, C.S.P.; Lund, L.H.; Redfield, M.M. Interdependence of Atrial Fibrillation and Heart Failure with a Preserved Ejection Fraction Reflects a Common Underlying Atrial and Ventricular Myopathy. Circulation 2020, 141, 4–6. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
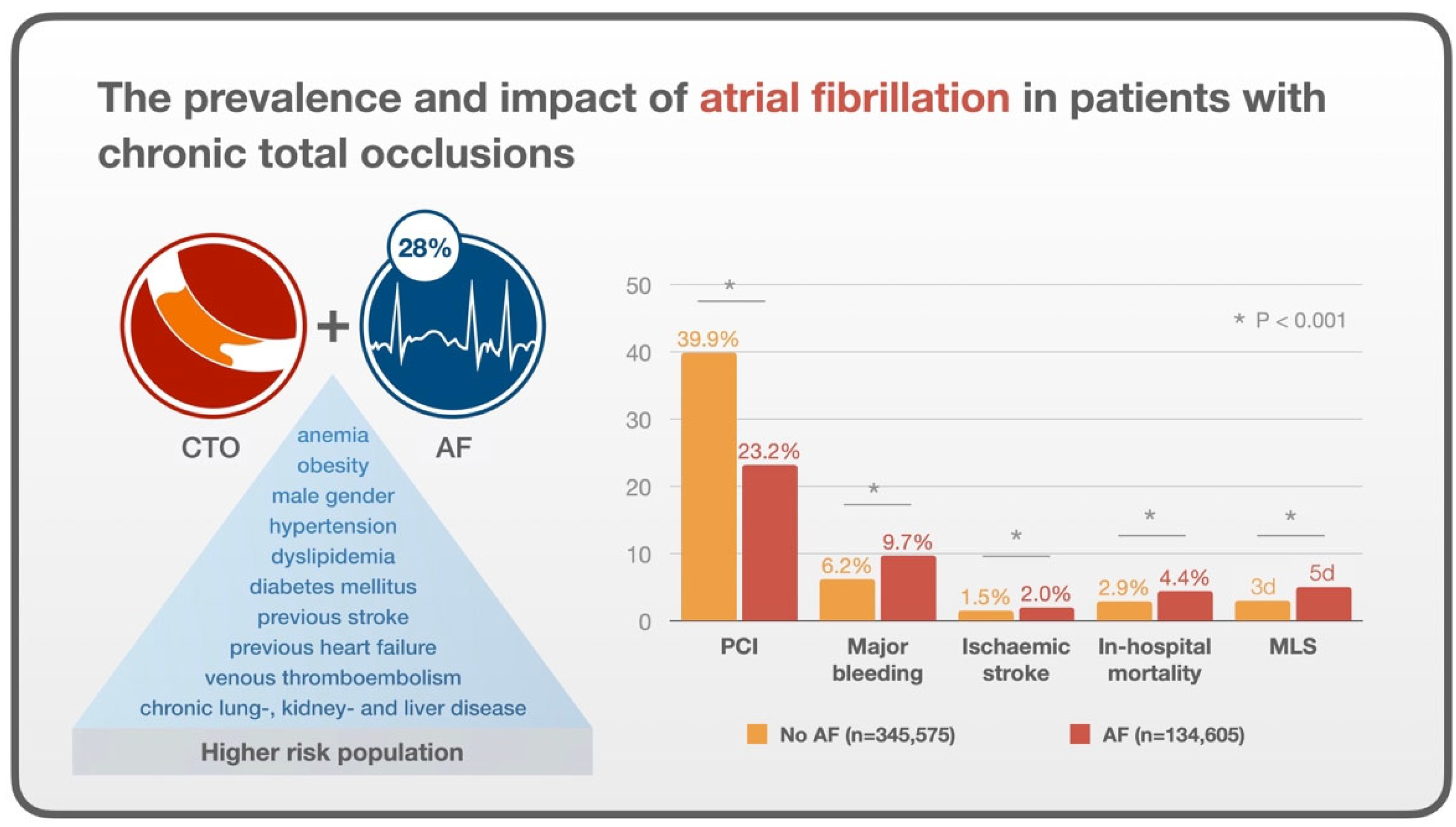
| Variable | No AF (n = 345,575) | AF (n = 134,605) | p-Value |
|---|---|---|---|
| Median age [IQR] | 66 [58 to 74] | 73 [66 to 80] | <0.001 |
| Female | 27.9% | 25.0% | <0.001 |
| Smoking | 1.4% | 0.9% | <0.001 |
| Alcohol misuse | 1.8% | 1.5% | 0.014 |
| Obesity | 21.5% | 21.9% | 0.15 |
| Hypertension | 86.9% | 90.7% | <0.001 |
| Hypercholesterolaemia | 76.4% | 75.6% | 0.006 |
| Diabetes mellitus | 48.5% | 47.7% | 0.023 |
| Previous myocardial infarction | 29.6% | 31.5% | <0.001 |
| Previous stroke | 11.5% | 14.1% | <0.001 |
| Previous heart failure | 28.8% | 48.4% | <0.001 |
| Previous venous thromboembolism | 3.9% | 5.0% | <0.001 |
| Chronic lung disease | 24.7% | 31.4% | <0.001 |
| Chronic kidney disease | 26.0% | 37.5% | <0.001 |
| Liver disease | 3.9% | 5.1% | <0.001 |
| Anemia | 7.8% | 10.2% | <0.001 |
| Cancer | 3.6% | 5.0% | <0.001 |
| Dementia | 3.1% | 4.7% | <0.001 |
| Major bleeding | 6.2% | 9.7% | <0.001 |
| Percutaneous coronary intervention | 39.9% | 23.2% | <0.001 |
| Ischemic stroke | 1.5% | 2.0% | <0.001 |
| In-hospital mortality | 2.9% | 4.4% | <0.001 |
| Median length of stay [IQR] | 3 [2 to 6] | 5 [3 to 9] | <0.001 |
| Median hospital cost [IQR] | USD 18,747 [11,252 to 31,695] | USD 21,671 [11,148 to 40,884] | <0.001 |
| Variable | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Age | 1.05 (1.04–1.05) | <0.001 |
| Female sex | 0.75 (0.73–0.78) | <0.001 |
| Race vs. White | ||
| Black | 0.59 (0.55–0.62) | <0.001 |
| Hispanic | 0.62 (0.58–0.66) | <0.001 |
| Asian or Pacific Islander | 0.81 (0.73–0.89) | <0.001 |
| Native American | 0.60 (0.48–0.75) | <0.001 |
| Other | 0.69 (0.63–0.76) | <0.001 |
| Smoking | 0.85 (0.73–0.99) | 0.042 |
| Alcohol misuse | 1.15 (1.01–1.130) | 0.029 |
| Primary expected payer vs. Medicare | ||
| Medicaid | 0.82 (0.77–0.88) | <0.001 |
| Private insurance | 0.91 (0.87–0.95) | <0.001 |
| Self-pay | 0.74 (0.66–0.83) | <0.001 |
| ZIP income quartile vs. 0th–25th | ||
| 51st–75th | 1.05 (1.00–1.10) | 0.039 |
| 76th–100th | 1.08 (1.03–1.13) | 0.002 |
| Obesity | 1.25 (1.20–1.30) | <0.001 |
| Hypertension | 1.17 (1.11–1.23) | <0.001 |
| Diabetes mellitus | 0.92 (0.84–0.90) | <0.001 |
| Previous stroke | 1.15 (0.89–0.95) | <0.001 |
| Previous heart failure | 1.98 (1.92–2.05) | <0.001 |
| Previous venous thromboembolism | 1.18 (1.09–1.27) | <0.001 |
| Chronic lung disease | 1.18 (1.14–1.23) | <0.001 |
| Chronic kidney disease | 1.20 (1.16–1.24) | <0.001 |
| Liver disease | 1.37 (1.27–1.48) | <0.001 |
| Dementia | 0.92 (0.85–0.99) | 0.036 |
| Anemia | 1.16 (1.10–1.22) | <0.001 |
| Impact of AF on Outcomes for Patient with CTO | |||
|---|---|---|---|
| Outcome | n | Odds ratio (95% CI) | p-value |
| In-hospital mortality | 454,110 | 1.29 (1.18–1.40) | <0.001 |
| Ischemic stroke | 454,110 | 1.27 (1.13–1.42) | <0.001 |
| Major bleeding | 454,110 | 1.38 (1.30–1.46) | <0.001 |
| Outcome | n | Coefficient [95% CI) | p-value |
| Length of stay | 454,110 | 1.58 [1.50 to 1.67] | <0.001 |
| Cost | 450,800 | 6219 [5811 to 6627] | <0.001 |
| Impact of AF on Outcomes for Patient with CTO in Patients with PCI | |||
| Outcome | n | Odds ratio (95% CI) | p-value |
| In-hospital mortality | 159,525 | 1.55 (1.35–1.78) | <0.001 |
| Ischemic stroke | 159,525 | 1.53 (1.19–1.96) | 0.001 |
| Major bleeding | 159,525 | 1.44 (1.26–1.64) | <0.001 |
| Outcome | n | Coefficient [95% CI) | p-value |
| Length of stay | 159,525 | 1.47 (1.34–1.60) | <0.001 |
| Cost | 158,340 | 5342 [4684 to 6000) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Will, M.; Schwarz, K.; Holroyd, E.; Borovac, J.A.; Qureshi, A.I.; Lip, G.Y.H.; Mascherbauer, J.; Leibundgut, G.; Weiss, T.W.; Kwok, C.S. The Prevalence and Impact of Atrial Fibrillation on Patients with Chronic Total Occlusions: Insights from the National Inpatient Sample. J. Cardiovasc. Dev. Dis. 2025, 12, 100. https://doi.org/10.3390/jcdd12030100
Will M, Schwarz K, Holroyd E, Borovac JA, Qureshi AI, Lip GYH, Mascherbauer J, Leibundgut G, Weiss TW, Kwok CS. The Prevalence and Impact of Atrial Fibrillation on Patients with Chronic Total Occlusions: Insights from the National Inpatient Sample. Journal of Cardiovascular Development and Disease. 2025; 12(3):100. https://doi.org/10.3390/jcdd12030100
Chicago/Turabian StyleWill, Maximilian, Konstantin Schwarz, Eric Holroyd, Josip A. Borovac, Adnan I. Qureshi, Gregory Y. H. Lip, Julia Mascherbauer, Gregor Leibundgut, Thomas W. Weiss, and Chun Shing Kwok. 2025. "The Prevalence and Impact of Atrial Fibrillation on Patients with Chronic Total Occlusions: Insights from the National Inpatient Sample" Journal of Cardiovascular Development and Disease 12, no. 3: 100. https://doi.org/10.3390/jcdd12030100
APA StyleWill, M., Schwarz, K., Holroyd, E., Borovac, J. A., Qureshi, A. I., Lip, G. Y. H., Mascherbauer, J., Leibundgut, G., Weiss, T. W., & Kwok, C. S. (2025). The Prevalence and Impact of Atrial Fibrillation on Patients with Chronic Total Occlusions: Insights from the National Inpatient Sample. Journal of Cardiovascular Development and Disease, 12(3), 100. https://doi.org/10.3390/jcdd12030100