
Accuracy and Reproducibility of a Modified Echocardiographic Method for Right Ventricular Output Calculation in Neonates

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Data
2.2. Echocardiography
2.3. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Echocardiographic Data
3.3. Accuracy of Tip-RVO and Hinge-RVO
3.4. Intra- and Inter-Observer Reproducibility
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de Boode, W.P.; van der Lee, R.; Eriksen, B.H.; Nestaas, E.; Dempsey, E.; Singh, Y.; Austin, T.; El-Khuffash, A. The role of Neonatologist Performed Echocardiography in the assessment and management of neonatal shock. Pediatr. Res. 2018, 84, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, C.E.; Dempsey, E.M. Management of Neonatal Hypotension and Shock. Semin. Fetal Neonatal Med. 2020, 25, 101121. [Google Scholar] [CrossRef] [PubMed]
- Groves, A.M.; Singh, Y.; Dempsey, E.; Molnar, Z.; Austin, T.; El-Khuffash, A.; de Boode, W.P. Introduction to neonatologist-performed echocardiography. Pediatr. Res. 2018, 84, 1–2. [Google Scholar] [CrossRef]
- El-Khuffash, A.F.; McNamara, P.J. Neonatologist-performed functional echocardiography in the neonatal intensive care unit. Semin. Fetal Neonatal Med. 2011, 16, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Barrington, K.; El-Khuffash, A.; Dempsey, E. Intervention and Outcome for Neonatal Hypotension. Clin. Perinatol. 2020, 47, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Corsini, I.; Ficial, B.; Fiocchi, S.; Schena, F.; Capolupo, I.; Cerbo, R.M.; Condò, M.; Doni, D.; La Placa, S.; Porzio, S.; et al. Neonatologist performed echocardiography (NPE) in Italian neonatal intensive care units: A national survey. Ital. J. Pediatr. 2019, 45, 131. [Google Scholar] [CrossRef]
- Alfarano, A.; Marzollo, R.; Bosio, M.I.; Tomasi, C.; Codega, A.; Picciau, L.; Motta, M.; Risso, F.M. Inter-observer variability of right ventricular output measurement in newborn infants: An observational study. Int. J. Cardiovasc. Imaging 2024, 40, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- McNamara, P.J.; Jain, A.; El-Khuffash, A.; Giesinger, R.; Weisz, D.; Freud, L.; Levy, P.T.; Bhombal, S.; de Boode, W.; Leone, T.; et al. Guidelines and Recommendations for Targeted Neonatal Echocardiography and Cardiac Point-of-Care Ultrasound in the Neonatal Intensive Care Unit: An Update from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2024, 37, 171–215. [Google Scholar] [CrossRef] [PubMed]
- Popat, H.; Robledo, K.P.; Sebastian, L.; Evans, N.; Gill, A.; Kluckow, M.; Sinhal, S.; de Waal, K.; Tarnow-Mordi, W.; Osborn, D. Interobserver agreement and image quality of functional cardiac ultrasound measures used in a randomised trial of delayed cord clamping in preterm infants. Arch. Dis. Child.-Fetal Neonatal Ed. 2018, 103, F257–F263. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [PubMed]
- Ficial, B.; Bonafiglia, E.; Gangemi, A.; Clemente, M.; Cappelleri, A.; Corsini, I.; Biban, P. Impact of Aortic Diameter Measurements at Three Anatomical Landmarks on Left Ventricular Output Calculation in Neonates. J. Ultrasound Med. 2022, 41, 1187–1194. [Google Scholar] [CrossRef]
- Koestenberger, M.; Nagel, B.; Ravekes, W.; Urlesberger, B.; Raith, W.; Avian, A.; Halb, V.; Cvirn, G.; Fritsch, P.; Gamillscheg, A. Systolic Right Ventricular Function in Preterm and Term Neonates: Reference Values of the Tricuspid Annular Plane Systolic Excursion (TAPSE) in 258 Patients and Calculation of Z-Score Values. Neonatology 2011, 100, 85–92. [Google Scholar] [CrossRef]
- Koestenberger, M.; Nagel, B.; Ravekes, W.; Gamillscheg, A.; Pichler, G.; Avian, A.; Heinzl, B.; Binder, C.; Cvirn, G.; Urlesberger, B. Right Ventricular Performance in Preterm and Term Neonates: Reference Values of the Tricuspid Annular Peak Systolic Velocity Measured by Tissue Doppler Imaging. Neonatology 2013, 103, 281–286. [Google Scholar] [CrossRef]
- Ficial, B.; Corsini, I.; Clemente, M.; Cappelleri, A.; Remaschi, G.; Quer, L.; Urbani, G.; Sandrini, C.; Biban, P.; Dani, C.; et al. Feasibility, Reproducibility and Reference Ranges of Left Atrial Strain in Preterm and Term Neonates in the First 48 h of Life. Diagnostics 2022, 12, 350. [Google Scholar] [CrossRef]
- Colan, S.D.; Shirali, G.; Margossian, R.; Gallagher, D.; Altmann, K.; Canter, C.; Chen, S.; Golding, F.; Radojewski, E.; Camitta, M.; et al. The Ventricular Volume Variability Study of the Pediatric Heart Network: Study Design and Impact of Beat Averaging and Variable Type on the Reproducibility of Echocardiographic Measurements in Children with Chronic Dilated Cardiomyopathy. J. Am. Soc. Echocardiogr. 2012, 25, 842. [Google Scholar] [CrossRef] [PubMed]
- Ficial, B.; Finnemore, A.E.; Cox, D.J.; Broadhouse, K.M.; Price, A.N.; Durighel, G.; Ekitzidou, G.; Hajnal, J.V.; Edwards, A.D.; Groves, A.M. Validation study of the accuracy of echocardiographic measurements of systemic blood flow volume in newborn infants. J. Am. Soc. Echocardiogr. 2013, 26, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Stamm, C.; Anderson, R.H.; Yen, S.H.; Yen Ho, S. Clinical Anatomy of the Normal Pulmonary Root Compared With That in Isolated Pulmonary Valvular Stenosis. J. Am. Coll. Cardiol. 1998, 31, 1420–1425. [Google Scholar] [CrossRef]
- Hokken, R.B.; Bartelings, M.M.; Bogers, A.J.J.C.; Gittonberger-De Groot, A.C. Morphology of the pulmonary and aortic roots with regard to the pulmonary autograft procedure. J. Thorac. Cardiovasc. Surg. 1997, 113, 453–461. [Google Scholar] [CrossRef]
- Sievers, H.H.; Hemmer, W.; Beyersdorf, F.; Moritz, A.; Moosdorf, R.; Lichtenberg, A.; Misfeld, M.; Charitos, E.I. The everyday used nomenclature of the aortic root components: The tower of babel? Eur. J. Cardio-Thorac. Surg. 2012, 41, 478–482. [Google Scholar] [CrossRef]
- Lis, M.; Krawczyk-Ożóg, A.; Hołda, J.; Tyrak, K.; Dudkiewicz, D.; Yakovliev, A.; Strona, M.; Bolechała, F.; Jakiel, R.; Jakiel, M.; et al. Pulmonary valve morphometry revisited: Clinical implications for valvular and supravalvular interventions. Clin. Anat. 2023, 36, 234–241. [Google Scholar] [CrossRef]
- Tsai-Goodman, B.; Martin, R.P.; Marlow, N.; Skinner, J.R. The repeatability of echocardiographic determination of right ventricular output in the newborn. Cardiol. Young 2001, 11, 188–194. [Google Scholar] [CrossRef]
- de Boode, W.P.; Singh, Y.; Molnar, Z.; Schubert, U.; Savoia, M.; Sehgal, A.; Levy, P.; McNamara, P.; El-Khuffash, A. Application of Neonatologist Performed Echocardiography in the assessment and management of persistent pulmonary hypertension of the newborn. Pediatr. Res. 2018, 84, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Beker, F.; Davis, P.G.; Sehgal, A.; Rogerson, S. Echocardiographic assessment of left ventricular outflow tract diameter in preterm infants. Australas. J. Ultrasound Med. 2014, 17, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Sloot, S.C.; De Waal, K.A.; Van Der Lee, J.H.; Van Kaam, A.H. Central blood flow measurements in stable preterm infants after the transitional period. Arch. Dis. Child. Fetal Neonatal Ed. 2010, 95, F369–F372. [Google Scholar] [CrossRef]
- Patel, N.; Dodsworth, M.; Mills, J.F. Cardiac output measurement in newborn infants using the ultrasonic cardiac output monitor: An assessment of agreement with conventional echocardiography, repeatability and new user experience. Arch. Dis. Child. Fetal Neonatal Ed. 2011, 96, F206–F211. [Google Scholar] [CrossRef]
- Ficial, B.; Bonafiglia, E.; Padovani, E.M.; Prioli, M.A.; Finnemore, A.E.; Cox, D.J.; Broadhouse, K.M.; Price, A.N.; Durighel, G.; Groves, A.M. A modified echocardiographic approach improves reliability of superior vena caval flow quantification. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F7–F11. [Google Scholar] [CrossRef] [PubMed]
- Cappelleri, A.; Bussmann, N.; Harvey, S.; Levy, P.T.; Franklin, O.; El-Khuffash, A. Myocardial function in late preterm infants during the transitional period: Comprehensive appraisal with deformation mechanics and non-invasive cardiac output monitoring. Cardiol. Young 2020, 30, 249–255. [Google Scholar] [CrossRef]
- Fraga, M.V.; Dysart, K.C.; Rintoul, N.; Chaudhary, A.S.; Ratcliffe, S.J.; Fedec, A.; Kren, S.; Cohen, M.S.; Kirpalani, H. Cardiac Output Measurement Using the Ultrasonic Cardiac Output Monitor: A Validation Study in Newborn Infants. Neonatology 2019, 116, 260–268. [Google Scholar] [CrossRef]
- Van Wyk, L.; Gupta, S.; Lawrenson, J.; de Boode, W.P. Accuracy and Trending Ability of Electrical Biosensing Technology for Non-invasive Cardiac Output Monitoring in Neonates: A Systematic Qualitative Review. Front. Pediatr. 2022, 10, 851850. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | |
|---|---|
| Gestational age (week) | 35.4 ± 3.8 |
| Birth weight (g) | 2380 ± 933 |
| Sex (F) | 23 (51.1%) |
| Cesarean section | 32 (71.1%) |
| 5 APGAR score | 9 [2–10] |
| Antenatal steroids | 12 (26.6%) |
| Clinical Data at the Time of Echocardiography | |
|---|---|
| Current weight (g) | 2306 ± 877 |
| Postnatal age (hours) | 24 [2–168] |
| Fluids (mL/kg/die) | 110 ± 45 |
| Systolic blood pressure (mmHg) | 71 ± 8 |
| Mean blood pressure (mmHg) | 50 ± 8 |
| Diastolic blood pressure (mmHg) | 41 ± 8 |
| Respiratory support: | |
| None | 35 (77.7%) |
| CPAP | 4 (8.8%) |
| Non-invasive ventilation | 7 (15.5%) |
| FiO2 (%) | 21 [21–28] |
| Left Ventricular Output (LVO) | |
|---|---|
| Aortic VTI (cm) | 10.4 ± 2.8 |
| Aortic HR (bpm) | 135 ± 17 |
| Aortic diameter (mm) | 5.5 ± 0.8 |
| LVO (mL/kg/min) | 138 ± 32 |
| Right Ventricular Output (RVO) | |
| Pulmonary Valve VTI (cm) | 11.2 ± 2.8 |
| Pulmonary HR (bpm) | 134 ± 20 |
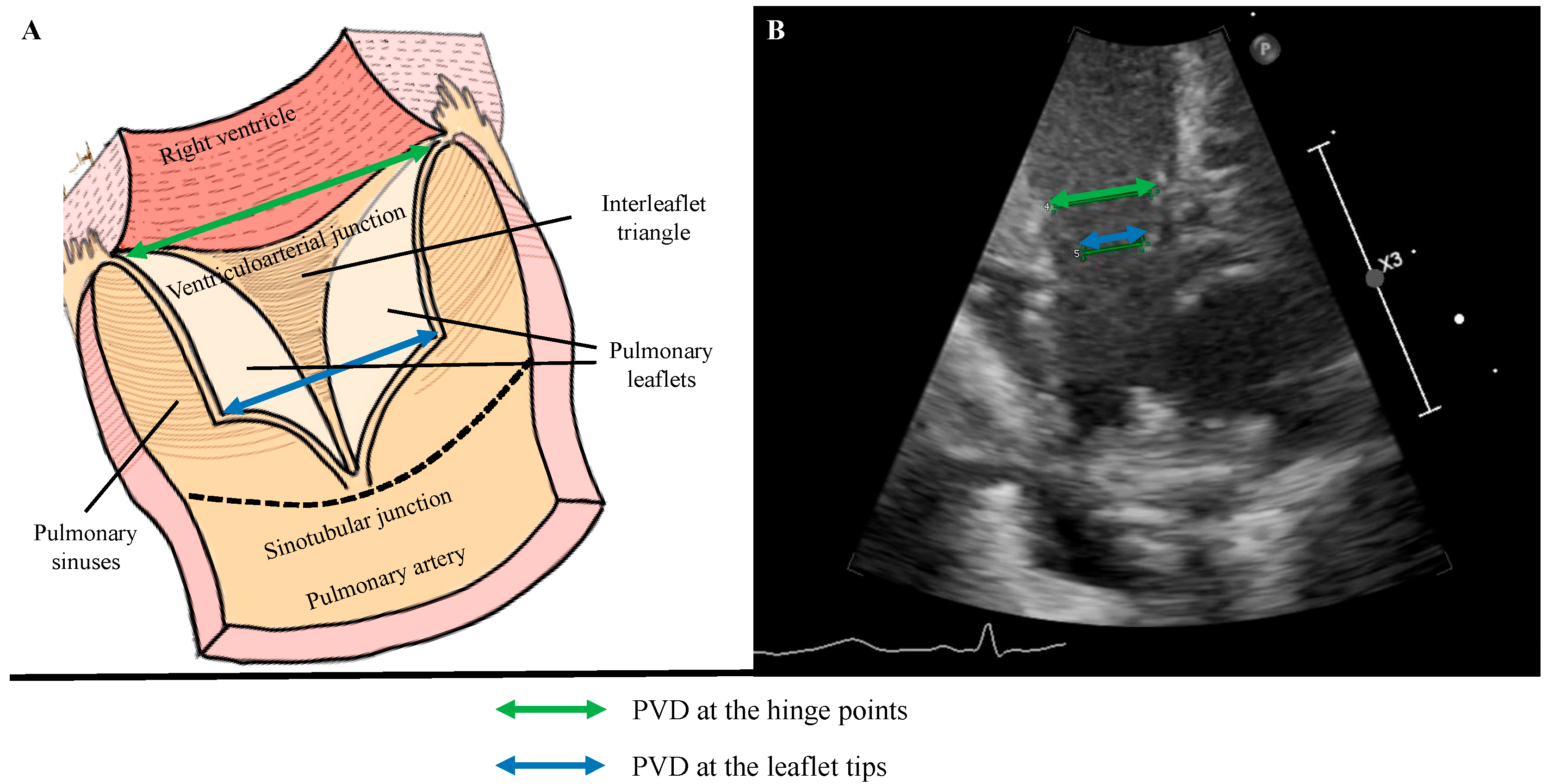
| tip-PVD (mm) | 5.1 ± 0.9 |
| tip-RVO (mL/kg/min) | 141 ± 36 |
| hinge-PVD (mm) | 6.1 ± 1.0 |
| hinge-RVO (mL/kg/min) | 198 ± 50 |
| Intra-Observer Reproducibility | Inter-Observer Reproducibility | |||||
|---|---|---|---|---|---|---|
| Bias (95% LOA) | ICC (95% CI) | COV (%) | Bias (95% LOA) | ICC (95% CI) | COV (%) | |
| Pulmonary valve diameter at the hinge points (mm) | −0.3 (−1.0 to 0.5) | 0.94 (0.88 to 0.98) | 6 | −0.3 (−1.8 to 1.2) | 0.73 (0.35 to 0.88) | 12 |
| Pulmonary valve diameter at the tips (mm) | −0.2 (−0.8 to 0.5) | 0.94 (0.86 to 0.97) | 6 | 0.1 (−1.4 to 1.6) | 0.70 (0.30 to 0.87) | 14.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milocchi, C.; Nogara, S.; Mazzuca, G.; Runfola, F.; Ciarcià, M.; Corsini, I.; Ficial, B. Accuracy and Reproducibility of a Modified Echocardiographic Method for Right Ventricular Output Calculation in Neonates. J. Cardiovasc. Dev. Dis. 2025, 12, 18. https://doi.org/10.3390/jcdd12010018
Milocchi C, Nogara S, Mazzuca G, Runfola F, Ciarcià M, Corsini I, Ficial B. Accuracy and Reproducibility of a Modified Echocardiographic Method for Right Ventricular Output Calculation in Neonates. Journal of Cardiovascular Development and Disease. 2025; 12(1):18. https://doi.org/10.3390/jcdd12010018
Chicago/Turabian StyleMilocchi, Carlotta, Silvia Nogara, Giorgia Mazzuca, Federica Runfola, Martina Ciarcià, Iuri Corsini, and Benjamim Ficial. 2025. "Accuracy and Reproducibility of a Modified Echocardiographic Method for Right Ventricular Output Calculation in Neonates" Journal of Cardiovascular Development and Disease 12, no. 1: 18. https://doi.org/10.3390/jcdd12010018
APA StyleMilocchi, C., Nogara, S., Mazzuca, G., Runfola, F., Ciarcià, M., Corsini, I., & Ficial, B. (2025). Accuracy and Reproducibility of a Modified Echocardiographic Method for Right Ventricular Output Calculation in Neonates. Journal of Cardiovascular Development and Disease, 12(1), 18. https://doi.org/10.3390/jcdd12010018