
Mitral Valve Surgery for Mitral Regurgitation Results in Reduced Left Ventricular Ejection Fraction in Barlow’s Disease as Compared with Fibro-Elastic Deficiency

 , , ,
, , ,
Abstract
1. Introduction
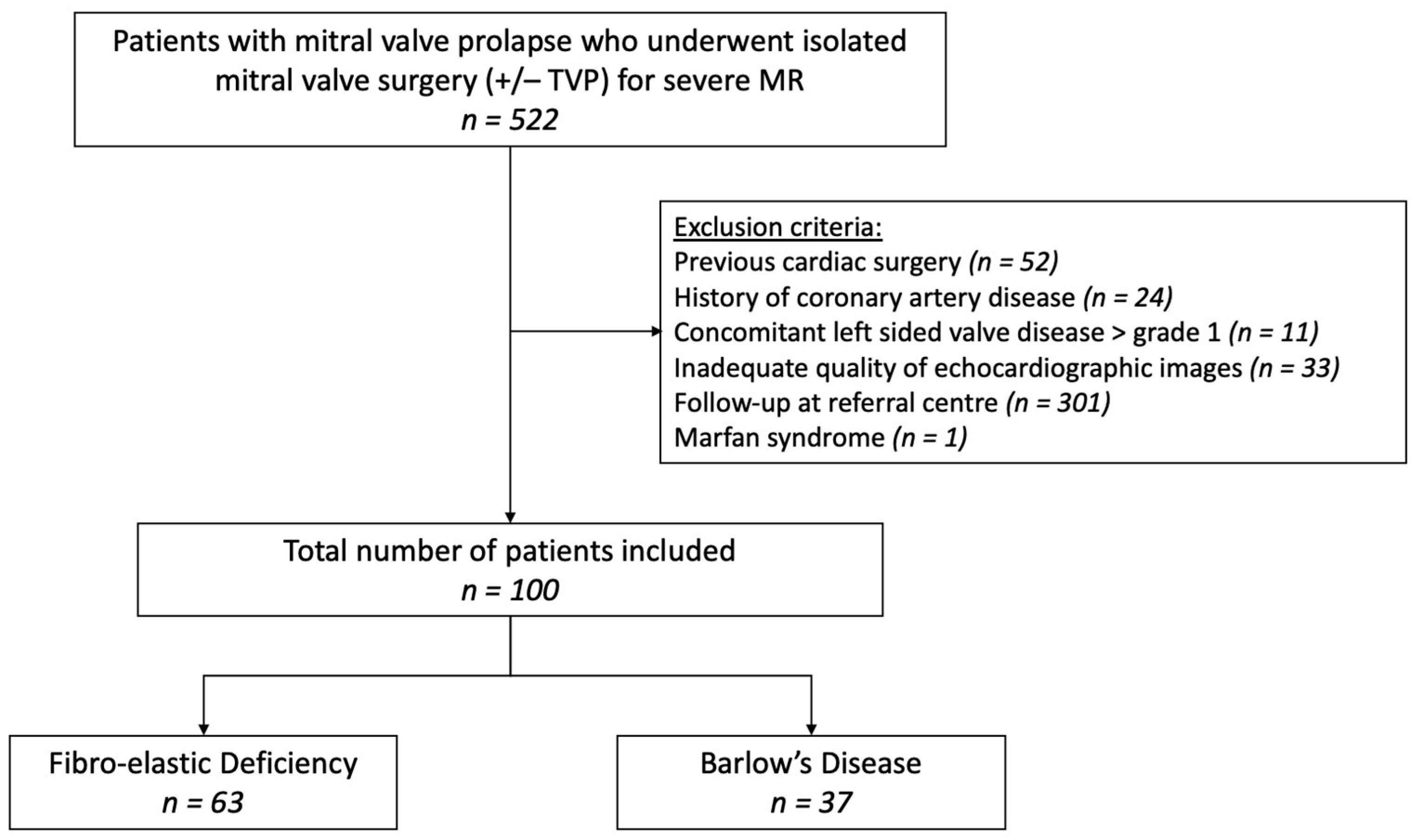
2. Materials and Methods
3. Results
3.1. Baseline Characteristics
3.2. Baseline Echocardiography
3.3. Surgical Intervention
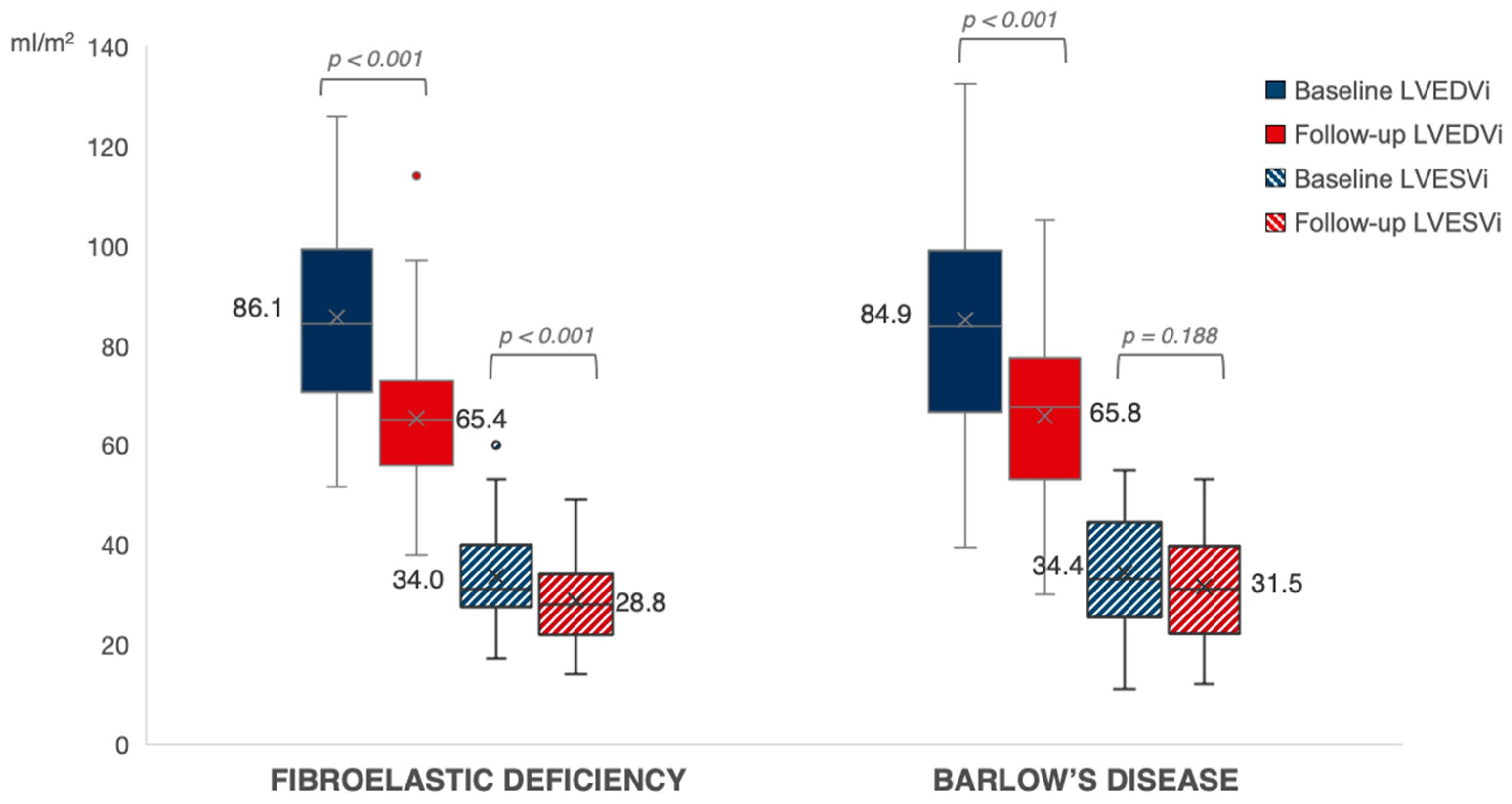
3.4. Follow-Up Echocardiography
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Freed, L.A.; Levy, D.; Levine, R.A.; Larson, M.G.; Evans, J.C.; Fuller, D.L.; Lehman, B.; Benjamin, E.J. Prevalence and clinical outcome of mitral-valve prolapse. N. Engl. J. Med. 1999, 341, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Delling, F.N.; Vasan, R.S. Epidemiology and pathophysiology of mitral valve prolapse: New insights into disease progression, genetics, and molecular basis. Circulation 2014, 129, 2158–2170. [Google Scholar] [CrossRef] [PubMed]
- Pype, L.L.; Bertrand, P.B.; Paelinck, B.P.; Heidbuchel, H.; Van Craenenbroeck, E.M.; Van De Heyning, C.M. Left Ventricular Remodeling in Non-syndromic Mitral Valve Prolapse: Volume Overload or Concomitant Cardiomyopathy? Front. Cardiovasc. Med. 2022, 9, 862044. [Google Scholar] [CrossRef] [PubMed]
- Anyanwu, A.C.; Adams, D.H. Etiologic classification of degenerative mitral valve disease: Barlow’s disease and fibroelastic deficiency. Semin. Thorac. Cardiovasc. Surg. 2007, 19, 90–96. [Google Scholar] [CrossRef]
- Adams, D.H.; Rosenhek, R.; Falk, V. Degenerative mitral valve regurgitation: Best practice revolution. Eur. Heart J. 2010, 31, 1958–1966. [Google Scholar] [CrossRef] [PubMed]
- Yiginer, O.; Keser, N.; Ozmen, N.; Tokatli, A.; Kardesoglu, E.; Isilak, Z.; Uz, O.; Uzun, M. Classic mitral valve prolapse causes enlargement in left ventricle even in the absence of significant mitral regurgitation. Echocardiography 2012, 29, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Malev, E.; Reeva, S.; Vasina, L.; Timofeev, E.; Pshepiy, A.; Korshunova, A.; Prokudina, M.; Zemtsovsky, E. Cardiomyopathy in young adults with classic mitral valve prolapse. Cardiol. Young 2014, 24, 694–701. [Google Scholar] [CrossRef]
- Yang, L.T.; Ahn, S.W.; Li, Z.; Benfari, G.; Mankad, R.; Takeuchi, M.; Levine, R.A.; Enriquez-Sarano, M.; Michelena, H.I. Mitral Valve Prolapse Patients with Less than Moderate Mitral Regurgitation Exhibit Early Cardiac Chamber Remodeling. J. Am. Soc. Echocardiogr. 2020, 33, 815–825.e2. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 75, 524. [Google Scholar] [CrossRef]
- Lancellotti, P.; Pibarot, P.; Chambers, J.; La Canna, G.; Pepi, M.; Dulgheru, R.; Dweck, M.; Delgado, V.; Garbi, M.; Vannan, M.A.; et al. Multi-modality imaging assessment of native valvular regurgitation: An EACVI and ESC council of valvular heart disease position paper. Eur. Heart J. Cardiovasc. Imaging 2022, 23, e171–e232. [Google Scholar] [CrossRef] [PubMed]
- Luyten, P.; Heuts, S.; Cheriex, E.; Olsthoorn, J.R.; Crijns, H.J.G.M.; Winkens, B.; Roos-Hesselink, J.W.; Nia, P.S.; Schalla, S. Mitral prolapsing volume is associated with increased cardiac dimensions in patients with mitral annular disjunction. Neth. Heart J. 2021, 30, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Le Tourneau, T.; Topilsky, Y.; Inamo, J.; Mahoney, D.W.; Suri, R.; Schaff, H.V.; Sarano, M. Reverse Left Ventricular Remodeling after Surgery in Primary Mitral Regurgitation: A Volume-Related Phased Process. Struct. Heart 2019, 3, 383–390. [Google Scholar] [CrossRef]
- Althunayyan, A.M.; Alborikan, S.; Badiani, S.; Wong, K.; Uppal, R.; Patel, N.; Petersen, S.E.; Lloyd, G.; Bhattacharyya, S. Determinants of post-operative left ventricular dysfunction in degenerative mitral regurgitation. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 1252–1257. [Google Scholar] [CrossRef]
- Enriquez-Sarano, M.; Tajik, A.; Schaff, H.V.; Orszulak, T.A.; McGoon, M.D.; Bailey, K.R.; Frye, R.L. Echocardiographic prediction of left ventricular function after correction of mitral regurgitation: Results and clinical implications. J. Am. Coll. Cardiol. 1994, 24, 1536–1543. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-Sarano, M.; Schaff, H.V.; Orszulak, T.A.; Tajik, A.J.; Bailey, K.R.; Frye, R.L. Valve repair improves the outcome of surgery for mitral regurgitation. A multivariate analysis. Circulation 1995, 91, 1022–1028. [Google Scholar] [CrossRef]
- Craven, T.P.; Chew, P.G.; Dobson, L.E.; Gorecka, M.; Parent, M.; Brown, L.A.E.; Saunderson, C.E.D.; Das, A.; Chowdhary, A.; Jex, N.; et al. Cardiac reverse remodeling in primary mitral regurgitation: Mitral valve replacement vs. mitral valve repair. J. Cardiovasc. Magn. Reson. 2023, 25, 43. [Google Scholar] [CrossRef]
- Constant Dit Beaufils, A.L.; Huttin, O.; Jobbe-Duval, A.; Senage, T.; Filippetti, L.; Piriou, N.; Cueff, C.; Venner, C.; Mandry, D.; Sellal, J.M.; et al. Replacement Myocardial Fibrosis in Patients with Mitral Valve Prolapse: Relation to Mitral Regurgitation, Ventricular Remodeling and Arrhythmia. Circulation 2021, 18, 1763–1774. [Google Scholar] [CrossRef]
- Le Tourneau, T.; Mérot, J.; Rimbert, A.; Le Scouarnec, S.; Probst, V.; Le Marec, H.; A Levine, R.; Schott, J.-J. Genetics of syndromic and non-syndromic mitral valve prolapse. Heart 2018, 104, 978–984. [Google Scholar] [CrossRef]
- van Wijngaarden, A.L.; Hiemstra, Y.L.; Koopmann, T.T.; Ruivenkamp, C.A.L.; Aten, E.; Schalij, M.J.; Bax, J.J.; Delgado, V.; Barge-Schaapveld, D.Q.C.M.; Marsan, N.A. Identification of known and unknown genes associated with mitral valve prolapse using an exome slice methodology. J. Med. Genet. 2020, 57, 843–850. [Google Scholar] [CrossRef]
- Essayagh, B.; Sabbag, A.; Antoine, C.; Benfari, G.; Yang, L.-T.; Maalouf, J.; Asirvatham, S.; Michelena, H.; Enriquez-Sarano, M. Presentation and Outcome of Arrhythmic Mitral Valve Prolapse. J. Am. Coll. Cardiol. 2020, 76, 637–649. [Google Scholar] [CrossRef] [PubMed]
- El-Tallawi, K.C.; Kitkungvan, D.; Xu, J.; Cristini, V.; Yang, E.Y.; Quinones, M.A.; Lawrie, G.M.; Zoghbi, W.A.; Shah, D.J. Resolving the Disproportionate Left Ventricular Enlargement in Mitral Valve Prolapse Due to Barlow Disease: Insights From Cardiovascular Magnetic Resonance. JACC Cardiovasc. Imaging 2020, 14, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Levy, F.; Iacuzio, L.; Marechaux, S.; Civaia, F.; Dommerc, C.; Wautot, F.; Tribouilloy, C.; Eker, A. Influence of Prolapse Volume in Mitral Valve Prolapse. Am. J. Cardiol. 2021, 157, 64–70. [Google Scholar] [CrossRef]
- Van De Heyning, C.M.; Magne, J.; Piérard, L.A.; Bruyère, P.-J.; Davin, L.; De Maeyer, C.; Paelinck, B.P.; Vrints, C.J.; Lancellotti, P. Assessment of left ventricular volumes and primary mitral regurgitation severity by 2D echocardiography and cardiovascular magnetic resonance. Cardiovasc. Ultrasound 2013, 11, 46. [Google Scholar] [CrossRef] [PubMed][Green Version]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 100) | BD (n = 37) | FED (n = 63) | p-Value (BD vs. FED) | |
|---|---|---|---|---|
| Male (%) | 71 (71.0) | 21 (56.8) | 50 (79.4) | 0.016 |
| Age (years old) | 60 ± 12 | 57 ± 13 | 62 ± 11 | 0.066 |
| BMI (kg/m2) | 25.2 ± 3.9 | 23.6 ± 3.0 | 26.2 ± 4.1 | <0.001 |
| BSA (m2) | 1.92 ± 0.24 | 1.87 ± 0.24 | 1.96 ± 0.23 | 0.088 |
| Smoking (%) | 32 (32.0) | 10 (27.8) | 22 (34.9) | 0.465 |
| Arterial hypertension (%) | 46 (46.0) | 14 (37.8) | 32 (50.8) | 0.209 |
| Hypercholesterolemia (%) | 33 (33.0) | 12 (32.4) | 21 (33.3) | 0.926 |
| Diabetes (%) | 2 (2.0) | 0 (0) | 2 (3.2) | 0.274 |
| Chronic kidney disease (%) | 8 (8.0) | 2 (5.4) | 6 (9.5) | 0.464 |
| Familial history of CV disease (%) | 44 (44.0) | 16 (48.5) | 28 (49.1) | 0.953 |
| Familial history of valve disease (%) | 10 (10.0) | 5 (16.7) | 5 (8.9) | 0.286 |
| Heart failure (%) | 4 (4) | 2 (5.4) | 2 (3.2) | 0.583 |
| Atrial fibrillation (%) | 30 (30.0) | 12 (32.4) | 18 (28.6) | 0.684 |
| Medication | ||||
| Beta-blocker (%) | 41 (41) | 11 (30.6) | 30 (47.6) | 0.097 |
| ACE-I or ARB (%) | 44 (44) | 14 (38.7) | 30 (47.6) | 0.400 |
| Anticoagulation (%) | 18 (18.0) | 6 (16.7) | 12 (19.0) | 0.768 |
| MRA (%) | 11 (11.0) | 2 (5.6) | 9 (14.3) | 0.184 |
| Non potassium sparing diuretics (%) | 20 (20.0) | 4 (11.1) | 15 (23.8) | 0.123 |
| Symptoms | ||||
| Symptomatic (%) | 78 (78.0) | 29 (82.9) | 49 (81.7) | 0.884 |
| Dyspnea (%) | 0.335 | |||
| NYHA class I | 28 (28.0) | 11 (31.4) | 17 (28.3) | |
| NYHA class II | 40 (40.0) | 12 (34.3) | 28 (46.7) | |
| NYHA class III | 19 (19.0) | 10 (28.6) | 9 (15.0) | |
| NYHA class IV | 8 (8.0) | 2 (5.7) | 6 (10.0) | |
| Chest pain (%) | 25 (25.0) | 9 (25.7) | 16 (26.7) | 0.919 |
| Palpitations (%) | 40 (40.0) | 19 (54.3) | 21 (35.0) | 0.066 |
| Syncope (%) | 6 (6.0) | 3 (8.6) | 3 (5.0) | 0.490 |
| All Patients (n = 100) | BD (n = 37) | FED (n = 63) | p-Value (BD vs. FED) | |
|---|---|---|---|---|
| LV IVS (mm) | 11.0 (9.0–13.0) | 11.0 (8.0–13.0) | 11.0 (10.0–13.0) | 0.050 |
| LVEDD (mm) | 52.1 ± 7.5 | 51.5 ± 8.6 | 52.5 ± 6.7 | 0.498 |
| LVESD (mm) | 32.5 ± 6.9 | 31.7 ± 6.6 | 33.0 ± 7.1 | 0.370 |
| E/A ratio | 1.7 ± 0.7 | 1.7 ± 0.8 | 1.7 ± 0.6 | 0.743 |
| E/e’ ratio | 14.6 ± 5.8 | 13.8 ± 6.5 | 15.1 ± 5.4 | 0.390 |
| LAVi (mL/m2) | 43.3 (32.0–58.1) | 45.4 (31.2–57.9) | 41.7 (32.2–58.6) | 0.810 |
| Mitral regurgitation | 0.082 | |||
| Grade 3 | 16 (16.0) | 9 (24.3) | 7 (11.1) | |
| Grade 4 | 84 (84.0) | 28 (75.7) | 56 (88.9) | |
| MR Rvol (mL) | 70.0 (52.0–78.5) | 66.0 (32.3–78.3) | 72.0 (56.5–79.5) | 0.342 |
| MR EROA (mm2) | 44.4 ± 15.9 | 40.4 ± 19.0 | 47.4 ± 12.7 | 0.185 |
| MV VTI (cm) | 136.3 ± 33.6 | 126.7 ± 44.1 | 141.6 ± 25.2 | 0.186 |
| Prolapse volume (mL) | 6.0 (1.0–9.5) | 9.0 (4.5–13.5) | 3.8 (0–7.1) | 0.001 |
| MV annulus AP diameter (mm) | 35.0 ± 5.6 | 36.9 ± 5.8 | 33.7 ± 5.1 | 0.017 |
| MV thickness (mm) | 4.0 (3.0–6.0) | 6.0 (5.0–7.3) | 4.0 (3.0–4.5) | <0.001 |
| Single leaflet prolapse | 66 (66.0) | 4 (10.8) | 62 (98.4) | |
| AML (%) | 8 (12.1) | 0 (0) | 8 (12.9) | 0.025 |
| PML (%) | 58 (87.9) | 4 (100) | 54 (87.1) | <0.001 |
| Bileaflet prolapse (%) | 34 (34.0) | 33 (89.2) | 1 (1.6) | <0.001 |
| Chordal rupture (%) | 40 (54.1) | 6 (21.4) | 34 (73.9) | <0.001 |
| LVEF (%) | 61.0 (56.0–65.0) | 60.0 (54.5–66.0) | 61.0 (56.0–65.0) | 0.685 |
| LV EDVi (mL/m2) | 85.7 ± 19.4 | 84.9 ± 21.5 | 86.1 ± 18.3 | 0.772 |
| LV ESVi (mL/m2) | 34.1 ± 10.5 | 34.4 ± 11.1 | 34.0 ± 10.1 | 0.863 |
| Tricuspid regurgitation | 0.174 | |||
| Grade 0 | 3 (40.2) | 19 (51.4) | 20 (33.3) | |
| Grade 1 | 45 (46.2) | 13 (35.1) | 32 (53.3) | |
| Grade 2 | 10 (10.3) | 4 (10.8) | 6 (10.0) | |
| Grade 3 | 2 (2.1) | 0 (0) | 2 (3.3) | |
| Grade 4 | 1 (1.0) | 1 (2.7) | 0 (0) | |
| PASP (mmHg) | 31.0 (26.0–42.0) | 30.0 (24.5–38.0) | 32.5 (27.0–43.3) | 0.121 |
| TAPSE (mm) | 22.0 (18.5–25.5) | 24.0 (21.0–25.8) | 20.0 (16.0–27.5) | 0.063 |
| All Patients (n = 100) | BD (n = 37) | FED (n = 63) | p-Value (BD vs. FED) | |
|---|---|---|---|---|
| Hospitalization duration (days) | 10 (9–13) | 10 (9–13.3) | 10 (9–13) | 0.582 |
| Mitral valve repair (%) | 76 (76.0) | 20 (54.1) | 56 (88.9) | <0.001 |
| Mitral valve annuloplasty (%) | 72 (94.7) | 20 (100.0) | 52 (92.9) | 0.002 |
| Neochord (%) | 51 (67.1) | 11 (55.0) | 40 (71.4) | 0.001 |
| Quadrangular or triangular resection (%) | 24 (31.6) | 8 (40.0) | 16 (28.6) | 0.670 |
| Mitral valve replacement (MVR) (%) | 24 (24.0) | 17 (45.9) | 7 (11.1) | <0.001 |
| MVR bio (%) | 10 (41.7) | 7 (41.2) | 3 (42.9) | 0.036 |
| MVR mech (%) | 14 (58.3) | 10 (58.8) | 4 (57.1) | 0.004 |
| Preservation of subvalvular apparatus (%) | 14 (58.3) | 8 (47.1) | 6 (85.7) | 0.090 |
| LAA occlusion (%) | 21 (21.2) | 7 (19.1) | 14 (22.2) | 0.745 |
| All Patients (n = 100) | BD (n = 37) | FED (n = 63) | p-Value (BD vs. FED) | |
|---|---|---|---|---|
| FU since surgery (days) | 278 (215–388) | 278 (211–364) | 288 (216–401) | 0.753 |
| LAVi (mL/m2) | 33.2 (26.9–45.6) | 33.2 (26.4–42.9) | 33.3 (27.3–47.7) | 0.570 ° |
| MR grade ≥ 2 (%) | 11 (11.0) | 2 (5.4) | 9 (14.3) | 0.205 |
| MV gradient (mmHg) | ||||
| Mean | 3.0 (2.2–5.0) | 3.0 (2.0–4.0) | 4.0 (3.0–5.0) | 0.033 |
| Max | 8.0 (6.0–12.0) | 7.0 (6.0–10.0) | 9.0 (6.0–12.0) | 0.147 |
| LVEF (%) | 55.0 (51.0–59.5) | 54.4 (48.5–56.0) | 57.0 (52.3–61.0) | <0.001 ° |
| LVEF < 50% | 17 (17.9) | 10 (27.8) | 7 (11.9) | 0.060 ° |
| LV EDVi (mL/m2) | 65.5 ± 16.2 | 65.8 ± 18.3 | 65.4 ± 14.8 | 0.843 ° |
| LV ESVi (mL/m2) | 29.8 ± 9.4 | 31.5 ± 11.2 | 28.8 ± 8.1 | 0.154 ° |
| ΔLV EDVi (mL/m2) | −20.3 ± 17.9 | −19.8 ± 19.8 | −20.6 ± 16.9 | 0.843 ° |
| ΔLV ESVi (mL/m2) | −4.4 ± 9.9 | −3.0 ± 11.2 | −5.3 ± 9.0 | 0.154 ° |
| ΔLVEF (%) | −5.6 ± 8.3 | −8.3 ± 9.6 | −3.9 ± 6.9 | <0.001 ° |
| Relative change LVEF (%) | −8.3 ± 13.4 | −12.4 ± 15.4 | −5.8 ± 11.4 | 0.018 |
| TR grade ≥ 2 (%) | 2 (2.4) | 1 (2.8) | 1 (2.1) | 1.000 |
| PAPs (mmHg) | 30.0 (25.0–32.0) | 29.0 (23.8–31.0) | 30.0 (26.0–34.0) | 0.136 ° |
| TAPSE (mm) | 17.2 ± 4.0 | 16.7 ± 3.5 | 17.5 ± 4.4 | 0.891 ° |
| Variables | Univariable Analysis | |
|---|---|---|
| B (95% CI) | p-Value | |
| Baseline LVEF (%) | −0.74 (−0.92, −0.56) | <0.001 |
| Baseline LVESVi (mL/m2) | 0.32 (0.17, 0.47) | <0.001 |
| LAVI (mL/m2) | −0.05 (−0.13, 0.03) | 0.196 |
| Barlow’s Disease | −4.34 (−7.71, −0.97) | 0.012 |
| Mitral valve replacement | −5.89 (−9.71, −2.07) | 0.003 |
| MR reg vol (mL) | −0.09 (−0.22, 0.04) | 0.161 |
| MR grade ≥ 2 at follow up | 1.92 (−3.35, 7.20) | 0.471 |
| BMI (kg/m2) | 0.18 (−0.26, 0.62) | 0.416 |
| Age (years) | −0.05 (−0.19, 0.09) | 0.506 |
| Atrial fibrillation | 1.21 (−2.46, 4.87) | 0.515 |
| Male sex | 0.986 (−2.72, 4.91) | 0.599 |
| Variables | Univariable Analysis | Collinearity Statistics | ||
|---|---|---|---|---|
| B (95% CI) | p-Value | Tolerance | VIF | |
| Baseline LVEF (%) | −0.77 (−0.99, −0.55) | <0.001 | 0.568 | 1.761 |
| Barlow’s Disease | −3.58 (−6.29, 0.88) | 0.010 | 0.839 | 1.192 |
| Mitral valve replacement | −2.62 (−5.76, 0.53) | 0.102 | 0.822 | 1.216 |
| LVESVi (mL/m2) | −0.05 (−0.20, 0.11) | 0.558 | 0.570 | 1.755 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pype, L.L.; Bertrand, P.B.; Debonnaire, P.; Dhont, S.; Hoekman, B.; Paelinck, B.P.; De Bock, D.; Heidbuchel, H.; Van Craenenbroeck, E.M.; Van De Heyning, C.M. Mitral Valve Surgery for Mitral Regurgitation Results in Reduced Left Ventricular Ejection Fraction in Barlow’s Disease as Compared with Fibro-Elastic Deficiency. J. Cardiovasc. Dev. Dis. 2024, 11, 71. https://doi.org/10.3390/jcdd11030071
Pype LL, Bertrand PB, Debonnaire P, Dhont S, Hoekman B, Paelinck BP, De Bock D, Heidbuchel H, Van Craenenbroeck EM, Van De Heyning CM. Mitral Valve Surgery for Mitral Regurgitation Results in Reduced Left Ventricular Ejection Fraction in Barlow’s Disease as Compared with Fibro-Elastic Deficiency. Journal of Cardiovascular Development and Disease. 2024; 11(3):71. https://doi.org/10.3390/jcdd11030071
Chicago/Turabian StylePype, Lobke L., Philippe B. Bertrand, Philippe Debonnaire, Sebastiaan Dhont, Boukje Hoekman, Bernard P. Paelinck, Dina De Bock, Hein Heidbuchel, Emeline M. Van Craenenbroeck, and Caroline M. Van De Heyning. 2024. "Mitral Valve Surgery for Mitral Regurgitation Results in Reduced Left Ventricular Ejection Fraction in Barlow’s Disease as Compared with Fibro-Elastic Deficiency" Journal of Cardiovascular Development and Disease 11, no. 3: 71. https://doi.org/10.3390/jcdd11030071
APA StylePype, L. L., Bertrand, P. B., Debonnaire, P., Dhont, S., Hoekman, B., Paelinck, B. P., De Bock, D., Heidbuchel, H., Van Craenenbroeck, E. M., & Van De Heyning, C. M. (2024). Mitral Valve Surgery for Mitral Regurgitation Results in Reduced Left Ventricular Ejection Fraction in Barlow’s Disease as Compared with Fibro-Elastic Deficiency. Journal of Cardiovascular Development and Disease, 11(3), 71. https://doi.org/10.3390/jcdd11030071