
The Influence of IL-11 on Cardiac Fibrosis in Experimental Models: A Systematic Review
 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction and Risk of Bias Assessment

{kind=link}
{kind=link}
{kind=link}
| Intervention | Treatment Schedule | Intervention Concentration of/Treatment route | Experimental Model | Fibrosis Model | Form of Induction of Cardiac Fibrosis | Euthanasia | Organ and Region Evaluated | Methodology Used for Fibrosis Analysis | Fibrosis | IL-11 Cardiac Levels | Cell Death | Cardiac Function | Fibrosis Markers | Mortality rate % | Body Weight | Immunomodulatory Effects | Fibrosis Pathway | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anti-IL11 (X203) Anti-IL11RA (X209) | 24 h post-surgery biweekly for 2 weeks | 20 mg/kg intraperitoneal | Male mice C57BL/6J (10- to 12-week-old) | Cardiac fibrosis | Ascending aortic constriction (AAC) | 2 weeks post-AAC | - | Masson’s trichrome | X203 and X209 decrease cardiac and perivascular fibrosis | X209 reduced IL11 | - | X203 and X209: increased aortic flow velocities and pressure gradients X209: decreased aortic root diameter. HW/BW rate not changed | X203 and X209 decrease. RNA expression: Col1a1, Col1a2, Col3a1, Fn1, Mmp2 and Timp1 X203 and X209 decrease. Protein expression: collagen and collagen III | Not changed | Not changed | - | X203 and X209 not changed: SMAD2, SMAD3. STAT3 X203, and X209 decreased ERK1/2 | [27] |
| Anti-IL11 (X203) | 24 h post- surgery biweekly for 2 weeks or 4 weeks | 20 mg/kg−1 intraperitoneal | Male mice C57BL/6J (10–12 weeks old) | Cardiac fibrosis | Transverse aortic constriction (TAC) AngII-subcutaneous | 2 weeks 4 weeks | Left ventricular | Masson’s trichrome | X203 decrease cardiac and perivascular fibrosis | X203 not changed IL11 levels | - | Not changed | X203 decrease Col1a2, Col3a, and FN1 | Not changed | - | - | - | [26] |
| Lentivirus (LV)-IL-11 + lutein | LV-IL-11: Two weeks before Ang II | LV-IL-11: Five separate intramyocardial injections (5 μL) into the front, side, and back of the left ventricle. | - | Cardiac fibrosis | AngII | Chronic | Left ventricular | Picrosirius red | lutein + LV-IL-11 increase | - | - | lutein + LV-IL-11 increased HW/BW, LVEDD and decreased EF | lutein + LV-IL-11 increased expression of ROS, Col1, TGF-β1 NOX2, and NOX4 | - | - | - | - | [5] |
| Recombinant human IL-11 (rhIL-11) | 10 min before the heart was isolated for cold ischemia | 12 µg/kg intravenously | Male Sprague- Dawley rats | Myocardial infarction | Ischemia/reperfusion | - | Left ventricular | - | - | - | Recombinant human IL-11 decrease apoptotic cells | Recombinant human IL-11 recovery of cardiac contractile function with increased LVDP and ±dP/dt | - | - | - | - | - | [32] |
| Recombinant mouse IL-11 (rmIL-11) | Daily for 6 successive days. | Dose not found. Subcutaneous | Male mice C57BL/6 (10–12 weeks) | Myocardial infarction | Ischemia/reperfusion | - | - | Masson’s trichrome | Recombinant mouse IL-11 increase | - | - | Recombinant mouse IL-11 increased end-systolic volume, epicardial thickness, and decreased ejection fraction (%) | - | - | - | - | - | [15] |
| Recombinant human IL-11 (rhIL-11) | At start of reperfusion | 3, 8, 20, 50 µg/kg intravenously | C57BL/6 e (8 to 12 week old) | Myocardial infarction | Ischemia/reperfusion | Twenty-four hours after reperfusion | Left ventricular | - | - | - | 20 µg/kg: decreased apoptotic cells | 20 and 50 µg/kg: decreased risk area size and infarct size 20 µg/kg; increased ejection fraction, fractional shortening, and hemodynamics | 20 µg/kg: increased MT1, MT2, and decreased ROS | Not changed | - | - | 20 µg/kg: increased STAT3 | [18] |
| Recombinant human IL-11 (rhIL-11) | 24 h after MI operation for 5 days consecutively | 3 µg/kg, 8 µg/kg, and 20 µg/kg intravenously | C57BL/6 (10 weeks old) | Myocardial infarction | Ischemia/reperfusion | 14 days after MI | Left ventricular | Masson’s trichrome | Both fibrotic circumference and fibrotic area were reduced by IL-11 in a dose-dependent manner | - | Decrease apoptotic cells | IL-11 treatment ameliorated cardiac dysfunction in a dose-dependent manner | - | - | - | - | IL-11 treatment increase STAT3 in a dose-dependent manner | [25] |
| Recombinant human IL-11 (rhIL-11) | 15 h before the ischemia/reperfusion injury | 8 µg/kg intravenously | C57Bl/6 (10 weeks old) | Myocardial infarction | Ischemia/reperfusion | 14 days after MI | - | - | - | - | - | Recombinant human IL-11 decreased risk area size and infarct size | - | - | - | - | - | [33] |
3. Results
3.1. Search for Studies and PRISMA Flowchart
3.2. Characteristics of the Studies
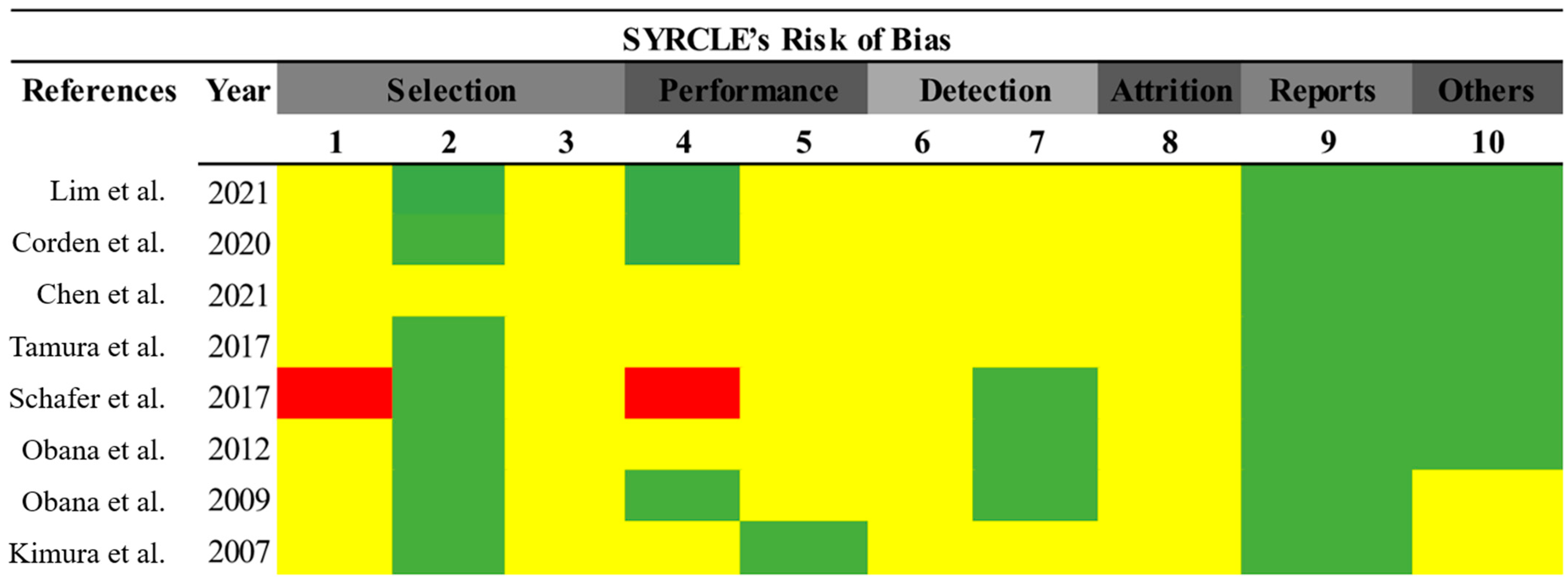
3.3. Risk of Bias Assessment
3.4. Relationship between IL-11 and Cardiac Fibrosis
3.5. Relation between IL-11 and Fibrosis Markers
3.6. Relationship between IL-11/Fibrosis Pathways
3.7. Relation between IL-11 and Cardiac Function
3.8. Relationship between Treatment and General Parameters of the Experimental Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bacmeister, L.; Schwarzl, M.; Warnke, S.; Stoffers, B.; Blankenberg, S.; Westermann, D.; Lindner, D. Inflammation and Fibrosis in Murine Models of Heart Failure; Springer: Berlin/Heidelberg, Germany, 2019; Volume 114, ISBN 0123456789. [Google Scholar]
- Kemp, C.D.; Conte, J.V. The Pathophysiology of Heart Failure. Cardiovasc. Pathol. 2012, 21, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Sinnenberg, L.; Givertz, M.M. Acute Heart Failure. Trends Cardiovasc. Med. 2020, 30, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Baman, J.R.; Ahmad, F.S. Heart Failure. JAMA -J. Am. Med. Assoc. 2020, 324, 1015. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, L.; Huang, S.; Ke, J.; Wang, Q.; Zhou, Z.; Chang, W. Lutein Attenuates Angiotensin II- Induced Cardiac Remodeling by Inhibiting AP-1/IL-11 Signaling. Redox Biol. 2021, 44, 102020. [Google Scholar] [CrossRef] [PubMed]
- Widjaja, A.A.; Shekeran, S.G.; Adami, E.; Wei Ting, J.G.; Tan, J.; Viswanathan, S.; Lim, S.Y.; Tan, P.H.; Hubner, N.; Coffman, T.; et al. A Neutralizing IL-11 Antibody Improves Renal Function and Increases Lifespan in a Mouse Model of Alport Syndrome. J. Am. Soc. Nephrol. 2022, 33, 717–730. [Google Scholar] [CrossRef] [PubMed]
- Menendez-Castro, C.; Cordasic, N.; Dambietz, T.; Veelken, R.; Amann, K.; Hartner, A.; Hilgers, K.F. Correlations between Interleukin-11 Expression and Hypertensive Kidney Injury in a Rat Model of Renovascular Hypertension. Am. J. Hypertens. 2020, 33, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Corden, B.; Adami, E.; Sweeney, M.; Schafer, S.; Cook, S.A. IL-11 in Cardiac and Renal Fibrosis: Late to the Party but a Central Player. Br. J. Pharmacol. 2020, 177, 1695–1708. [Google Scholar] [CrossRef]
- Dong, J.; Viswanathan, S.; Adami, E.; Singh, B.K.; Chothani, S.P.; Ng, B.; Lim, W.W.; Zhou, J.; Tripathi, M.; Ko, N.S.J.; et al. Hepatocyte-Specific IL11 Cis-Signaling Drives Lipotoxicity and Underlies the Transition from NAFLD to NASH. Nat. Commun. 2021, 12, 66. [Google Scholar] [CrossRef]
- Widjaja, A.; Singh, B.; Adami, E.; Viswanathan, S.; D’Agostino, G.; Dong, J.; Ng, B.; Tan, J.; Paleja, B.; Tripathi, M.; et al. IL-11 Neutralising Therapies Target Hepatic Stellate Cell-Induced Liver Inflammation and Fibrosis in NASH. bioRxiv 2018, 470062. [Google Scholar] [CrossRef]
- Zhu, M.; Lu, B.; Cao, Q.; Wu, Z.; Xu, Z.; Li, W.; Yao, X.; Liu, F. IL-11 Attenuates Liver Ischemia/Reperfusion Injury (IRI) through STAT3 Signaling Pathway in Mice. PLoS ONE 2015, 10, e0126296. [Google Scholar] [CrossRef]
- Bai, X.; Zhao, G.; Chen, Q.; Li, Z.; Gao, M.; Ho, W.; Xu, X.; Zhang, X.Q. Inhaled SiRNA Nanoparticles Targeting IL11 Inhibit Lung Fibrosis and Improve Pulmonary Function Post-Bleomycin Challenge. Sci. Adv. 2022, 8, eabn7162. [Google Scholar] [CrossRef]
- Ng, B.; Cook, S.A.; Schafer, S. Interleukin-11 Signaling Underlies Fibrosis, Parenchymal Dysfunction, and Chronic Inflammation of the Airway. Exp. Mol. Med. 2020, 52, 1871–1878. [Google Scholar] [CrossRef]
- Ng, B.; Dong, J.; Viswanathan, S.; Widjaja, A.A.; Paleja, B.S.; Adami, E.; Ko, N.S.J.; Wang, M.; Lim, S.; Tan, J.; et al. Fibroblast-Specific IL11 Signaling Drives Chronic Inflammation in Murine Fibrotic Lung Disease. FASEB J. 2020, 34, 11802–11815. [Google Scholar] [CrossRef] [PubMed]
- Schafer, S.; Viswanathan, S.; Widjaja, A.A.; Lim, W.W.; Moreno-Moral, A.; DeLaughter, D.M.; Ng, B.; Patone, G.; Chow, K.; Khin, E.; et al. IL-11 Is a Crucial Determinant of Cardiovascular Fibrosis. Nature 2017, 552, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Wang, Z.; Ye, D.; Wang, Y.; Wang, M.; Ji, Q.; Huang, Y.; Liu, L.; Shi, Y.; Shi, L.; et al. Increased Interleukin-11 Levels Are Correlated with Cardiac Events in Patients with Chronic Heart Failure. Mediat. Inflamm. 2019, 2019, 1575410. [Google Scholar] [CrossRef]
- Fernández-Ruiz, I. Cardioprotection: IL-11 Is a Potential Therapeutic Target in Cardiovascular Fibrosis. Nat. Rev. Cardiol. 2018, 15, 1. [Google Scholar] [CrossRef]
- Obana, M.; Miyamoto, K.; Murasawa, S.; Iwakura, T.; Hayama, A.; Yamashita, T.; Shiragaki, M.; Kumagai, S.; Miyawaki, A.; Takewaki, K.; et al. Therapeutic Administration of IL-11 Exhibits the Postconditioning Effects against Ischemia-Reperfusion Injury via STAT3 in the Heart. Am. J. Physiol. Hear. Circ. Physiol. 2012, 303, 569–577. [Google Scholar] [CrossRef]
- Du, X.; Williams, D.A. Interleukin-11: Review of Molecular, Cell Biology, and Clinical Use. J. Am. Soc. Hematol. 1997, 89, 3897–3908. [Google Scholar] [CrossRef]
- Lokau, J.; Kespohl, B.; Kirschke, S.; Garbers, C. The Role of Proteolysis in Interleukin-11 Signaling. Biochim. Biophys. Acta Mol. Cell Res. 2022, 1869, 119135. [Google Scholar] [CrossRef] [PubMed]
- Negahdaripour, M.; Nezafat, N.; Ghasemi, Y. Deep Insights into IL-11: A Panoramic Review and in Silico Approach. Cytokine Growth Factor Rev. 2016, 32, 41–61. [Google Scholar] [CrossRef]
- Garbers, C.; Scheller, J. Interleukin-6 and Interleukin-11: Same same but different. Biol. Chem. 2013, 394, 1145–1161. [Google Scholar] [CrossRef]
- Liu, Z.; Zhang, M.; Wu, J.; Zhou, P.; Liu, Y.; Wu, Y.; Yang, Y.; Lu, X. Serum CD121a (Interleukin 1 Receptor, Type I): A Potential Novel Inflammatory Marker for Coronary Heart Disease. PLoS ONE 2015, 10, e0131086. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Ye, J.; Wang, M.; Wang, Y.; Ji, Q.; Huang, Y.; Zeng, T.; Wang, Z.; Ye, D.; Jiang, H.; et al. Increased Interleukin-11 Levels in Thoracic Aorta and Plasma from Patients with Acute Thoracic Aortic Dissection. Clin. Chim. Acta 2018, 481, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Obana, M.; Maeda, M.; Takeda, K.; Hayama, A.; Mohri, T.; Yamashita, T.; Nakaoka, Y.; Komuro, I.; Takeda, K.; Matsumiya, G.; et al. Therapeutic Activation of Signal Transducer and Activator of Transcription 3 by Interleukin-11 Ameliorates Cardiac Fibrosis after Myocardial Infarction. Circulation 2009, 121, 684–691. [Google Scholar] [CrossRef]
- Corden, B.; Lim, W.W.; Song, W.; Chen, X.; Ko, N.S.J.; Su, L.; Tee, N.G.Z.; Adami, E.; Schafer, S.; Cook, S.A. Therapeutic Targeting of Interleukin-11 Signalling Reduces Pressure Overload–Induced Cardiac Fibrosis in Mice. J. Cardiovasc. Transl. Res. 2021, 14, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.W.; Corden, B.; Ye, L.; Viswanathan, S.; Widjaja, A.A.; Xie, C.; Su, L.; Tee, N.G.Z.; Schafer, S.; Cook, S.A. Antibody-Mediated Neutralization of IL11 Signalling Reduces ERK Activation and Cardiac Fibrosis in a Mouse Model of Severe Pressure Overload. Clin. Exp. Pharmacol. Physiol. 2021, 48, 605–613. [Google Scholar] [CrossRef]
- Lim, W.W.; Dong, J.; Ng, B.; Widjaja, A.A.; Xie, C.; Su, L.; Kwek, X.Y.; Tee, N.G.Z.; Jian Pua, C.; Schafer, S.; et al. Inhibition of IL11 Signaling Reduces Aortic Pathology in Murine Marfan Syndrome. Circ. Res. 2022, 130, 728–740. [Google Scholar] [CrossRef]
- Cook, S.A.; Schafer, S. Hiding in Plain Sight: Interleukin-11 Emerges as a Master Regulator of Fibrosis, Tissue Integrity, and Stromal Inflammation. Annu. Rev. Med. 2020, 71, 263–276. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Hooijmans, C.R.; Rovers, M.M.; De Vries, R.B.M.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s Risk of Bias Tool for Animal Studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef]
- Tamura, Y.; Kohno, H.; Mohri, T.; Fujio, Y.; Matsumiya, G. The Cardioprotective Effect of Interleukin-11 against Ischemia-Reperfusion Injury in a Heart Donor Model. Ann. Cardiothorac. Surg. 2017, 7, 99–105. [Google Scholar] [CrossRef]
- Kimura, R.; Maeda, M.; Arita, A.; Oshima, Y. Identification of Cardiac Myocytes as the Target of Interleukin 11, a Cardioprotective Cytokine. Cytokine 2007, 38, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Tepler, I.; Elias, L.; Smith, J.W.; Hussein, M.; Rosen, G.; Chang, A.Y.C.; Moore, J.O.; Gordon, M.S.; Kuca, B.; Beach, K.J.; et al. A Randomized Placebo-Controlled Trial of Recombinant Human Interleukin-11 in Cancer Patients with Severe Thrombocytopenia Due to Chemotherapy. Blood 1996, 87, 3607–3614. [Google Scholar] [CrossRef] [PubMed]
- Widjaja, A.A.; Singh, B.K.; Adami, E.; Viswanathan, S.; Dong, J.; D’Agostino, G.A.; Ng, B.; Lim, W.W.; Tan, J.; Paleja, B.S.; et al. Inhibiting Interleukin 11 Signaling Reduces Hepatocyte Death and Liver Fibrosis, Inflammation, and Steatosis in Mouse Models of Nonalcoholic Steatohepatitis. Gastroenterology 2019, 157, 777–792. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, D.; Liehn, E.A.; Nilcham, P.; Mayan, D.C.; Rattanasopa, C.; Anand, K.; Crespo-Avilan, G.E.; Hernandez-Resendiz, S.; Singaraja, R.R.; Cook, S.A.; et al. A Neutralizing IL-11 Antibody Reduces Vessel Hyperplasia in a Mouse Carotid Artery Wire Injury Model. Sci. Rep. 2021, 11, 20674. [Google Scholar] [CrossRef] [PubMed]
- Ng, B.; Dong, J.; D’Agostino, G.; Viswanathan, S.; Widjaja, A.A.; Lim, W.W.; Ko, N.S.J.; Tan, J.; Chothani, S.P.; Huang, B.; et al. Interleukin-11 Is a Therapeutic Target in Idiopathic Pulmonary Fibrosis. Sci. Transl. Med. 2019, 11, eaaw1237. [Google Scholar] [CrossRef] [PubMed]
- Milara, J.; Roger, I.; Montero, P.; Artigues, E.; Escrivá, J.; Cortijo, J. IL-11 System Participates in Pulmonary Artery Remodeling and Hypertension in Pulmonary Fibrosis. Respir. Res. 2022, 23, 313. [Google Scholar] [CrossRef]
- Guo, Y.T.; Lu, Y.Y.; Lu, X.; He, S.; Li, S.J.; Shao, S.; Zhou, H.D.; Wang, R.Q.; Li, X.D.; Gao, P.J. Krüppel-like Factor 15/Interleukin 11 Axis-Mediated Adventitial Remodeling Depends on Extracellular Signal-Regulated Kinases 1 and 2 Activation in Angiotensin Ii–Induced Hypertension. J. Am. Heart Assoc. 2021, 10, e020554. [Google Scholar] [CrossRef]
- Tang, W.; Yang, L.; Yang, Y.C.; Leng, S.X.; Elias, J.A. Transforming Growth Factor-β Stimulates Interleukin-11 Transcription via Complex Activating Protein-1-Dependent Pathways. J. Biol. Chem. 1998, 273, 5506–5513. [Google Scholar] [CrossRef]
- Wu, P.; Lin, B.; Huang, S.; Meng, J.; Zhang, F.; Zhou, M.; Hei, X.; Ke, Y.; Yang, H.; Huang, D. IL-11 Is Elevated and Drives the Profibrotic Phenotype Transition of Orbital Fibroblasts in Thyroid-Associated Ophthalmopathy. Front. Endocrinol. 2022, 13, 846106. [Google Scholar] [CrossRef]
- Lim, W.W.; Corden, B.; Ng, B.; Vanezis, K.; D’Agostino, G.; Widjaja, A.A.; Song, W.H.; Xie, C.; Su, L.; Kwek, X.Y.; et al. Interleukin-11 Is Important for Vascular Smooth Muscle Phenotypic Switching and Aortic Inflammation, Fibrosis and Remodeling in Mouse Models. Sci. Rep. 2020, 10, 17853. [Google Scholar] [CrossRef]
- Adami, E.; Viswanathan, S.; Widjaja, A.A.; Ng, B.; Chothani, S.; Zhihao, N.; Tan, J.; Lio, P.M.; George, B.L.; Altunoglu, U.; et al. IL11 Is Elevated in Systemic Sclerosis and IL11-Dependent ERK Signalling Underlies TGFβ-Mediated Activation of Dermal Fibroblasts. Rheumatology 2021, 60, 5820–5826. [Google Scholar] [CrossRef]
- Wang, D.; Zheng, X.; Fu, B.; Nian, Z.; Qian, Y.; Sun, R.; Tian, Z.; Wei, H. Hepatectomy Promotes Recurrence of Liver Cancer by Enhancing IL-11-STAT3 Signaling. EBioMedicine 2019, 46, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Heichler, C.; Scheibe, K.; Schmied, A.; Geppert, C.I.; Schmid, B.; Wirtz, S.; Thoma, O.M.; Kramer, V.; Waldner, M.J.; Büttner, C.; et al. STAT3 Activation through IL-6/IL-11 in Cancer-Associated Fibroblasts Promotes Colorectal Tumour Development and Correlates with Poor Prognosis. Gut 2020, 69, 1269–1282. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.; O’Fee, K.; Villanueva-Hayes, C.; Rahman, E.; Lee, M.; Vanezis, K.; Andrew, I.; Lim, W.W.; Widjaja, A.; Barton, P.J.R.; et al. Cardiomyocyte-Restricted Expression of IL11 Causes Cardiac Fibrosis, Inflammation, and Dysfunction. Int. J. Mol. Sci. 2023, 24, 12989. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.; Bchir, M.B.; Mres, K.O.F.; Villanueva-hayes, C. Interleukin 11 Therapy Causes Acute Heart Failure and Its Use in Patients Should Be Reconsidered. bioRxiv 2024. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Braga, Y.L.L.; do Carmo Neto, J.R.; Franco, P.I.R.; Helmo, F.R.; dos Reis, M.A.; de Oliveira, F.A.; Celes, M.R.N.; da Silva, M.V.; Machado, J.R. The Influence of IL-11 on Cardiac Fibrosis in Experimental Models: A Systematic Review. J. Cardiovasc. Dev. Dis. 2024, 11, 65. https://doi.org/10.3390/jcdd11020065
Braga YLL, do Carmo Neto JR, Franco PIR, Helmo FR, dos Reis MA, de Oliveira FA, Celes MRN, da Silva MV, Machado JR. The Influence of IL-11 on Cardiac Fibrosis in Experimental Models: A Systematic Review. Journal of Cardiovascular Development and Disease. 2024; 11(2):65. https://doi.org/10.3390/jcdd11020065
Chicago/Turabian StyleBraga, Yarlla Loyane Lira, José Rodrigues do Carmo Neto, Pablo Igor Ribeiro Franco, Fernanda Rodrigues Helmo, Marlene Antônia dos Reis, Flávia Aparecida de Oliveira, Mara Rúbia Nunes Celes, Marcos Vinícius da Silva, and Juliana Reis Machado. 2024. "The Influence of IL-11 on Cardiac Fibrosis in Experimental Models: A Systematic Review" Journal of Cardiovascular Development and Disease 11, no. 2: 65. https://doi.org/10.3390/jcdd11020065
APA StyleBraga, Y. L. L., do Carmo Neto, J. R., Franco, P. I. R., Helmo, F. R., dos Reis, M. A., de Oliveira, F. A., Celes, M. R. N., da Silva, M. V., & Machado, J. R. (2024). The Influence of IL-11 on Cardiac Fibrosis in Experimental Models: A Systematic Review. Journal of Cardiovascular Development and Disease, 11(2), 65. https://doi.org/10.3390/jcdd11020065