
Current Role of Electrocardiographic Imaging in Patient Selection for Cardiac Resynchronization Therapy

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Electrocardiographic Imaging: Technical Aspects
2.1. Acquisition Method
2.2. Limitations
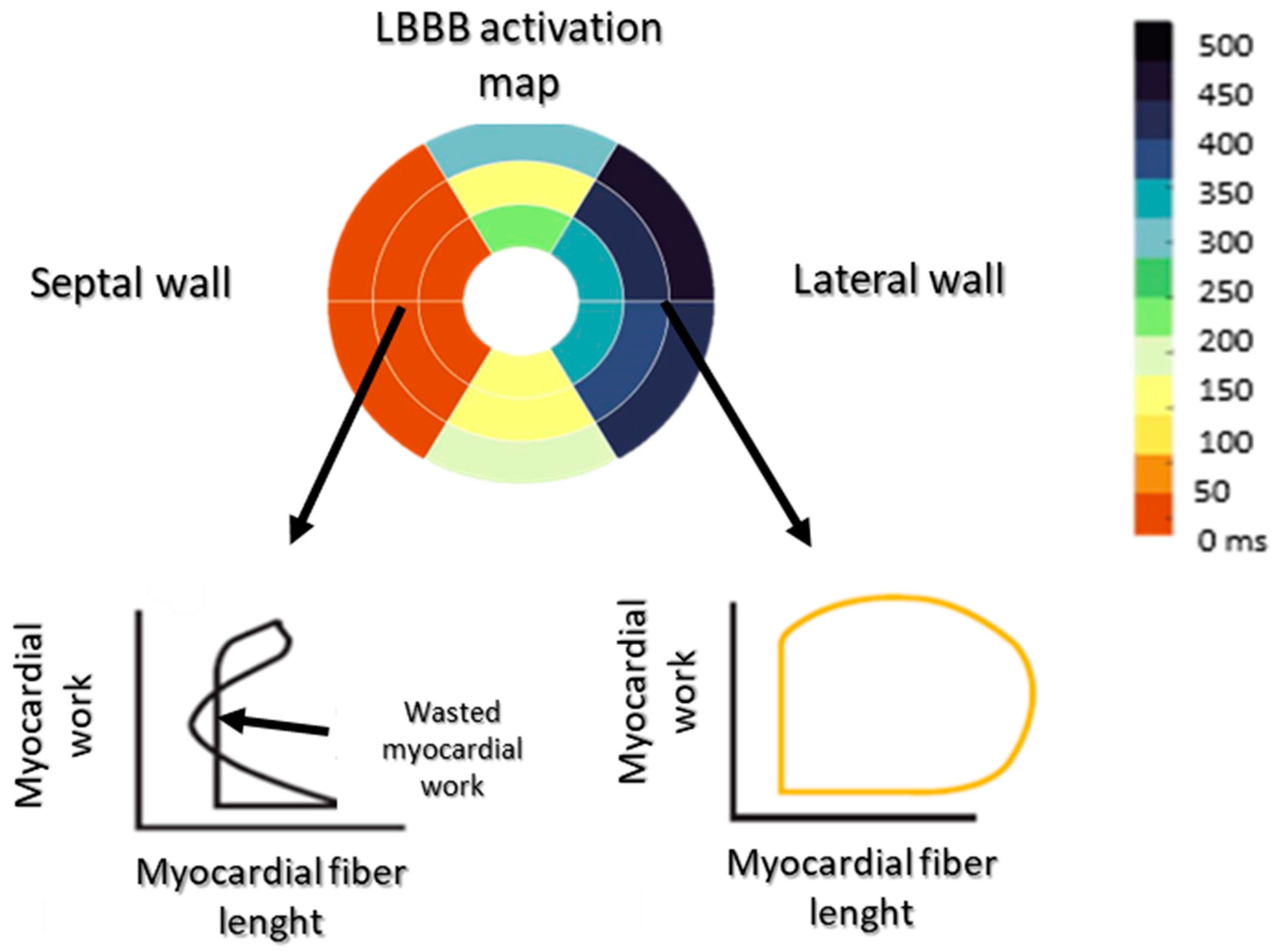
3. Impact of Electrical Asynchronism on Myocardial Contraction
4. Role of Electrocardiographic Imaging in Patient Selection
4.1. Electrocardiographic Imaging Allows a Better Understanding of Ventricular Activation
4.2. Electrical Dyssynchrony and Interventricular Dyssynchrony Are the Main Parameters for CRT Response
5. CRT Optimization Using Electrocardiographic Imaging
5.1. Correction of Dyssynchrony in Non-Responders and Responders
5.2. Place of ECGi in LV Lead Placement
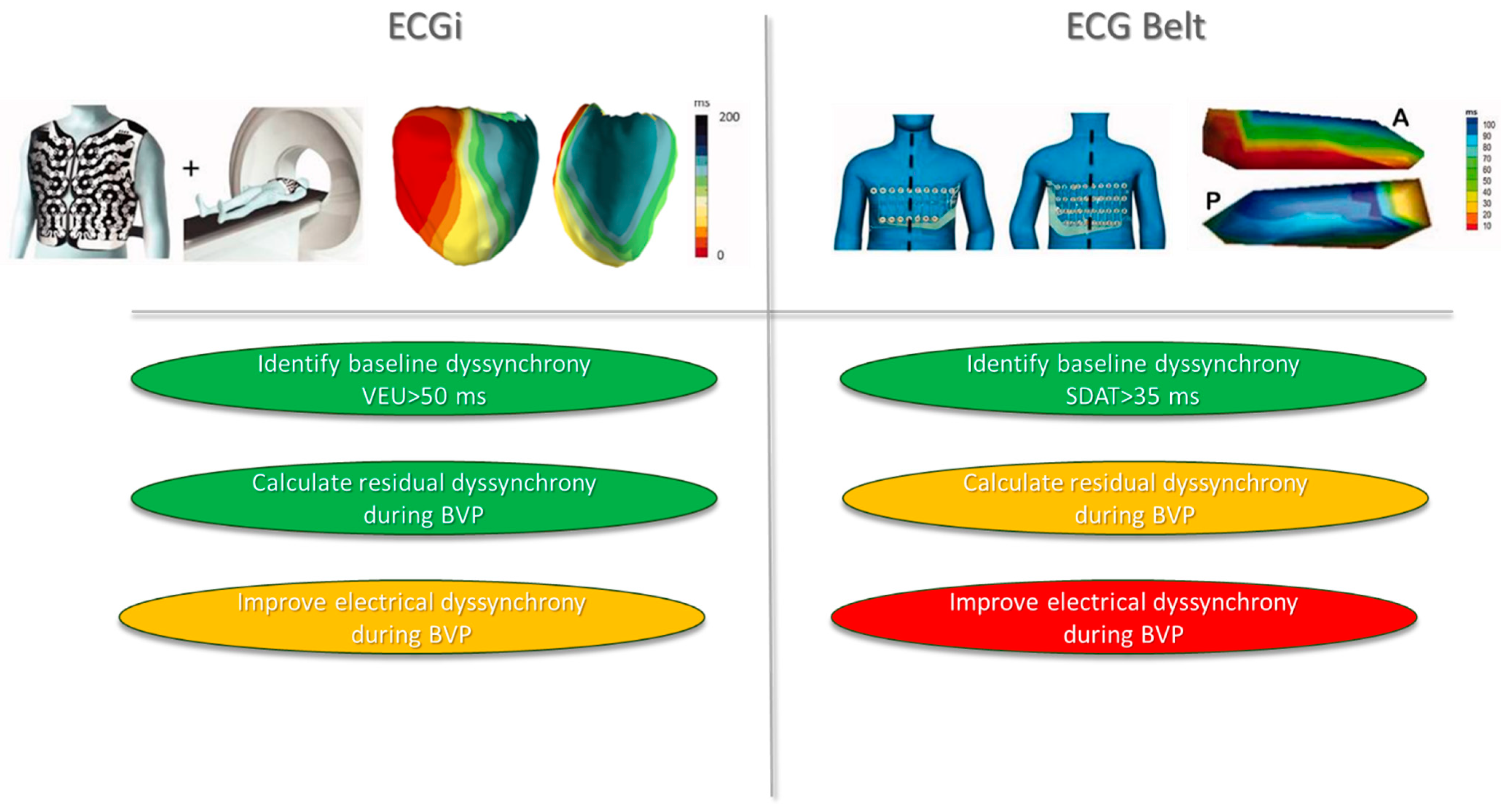
6. ECG Belt
7. Limitations and Perspectives
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADV | Activation delay vector |
| BVP | Biventricular pacing |
| CRT | Cardiac resynchronization therapy |
| ECGi | Electrocardiographic imaging |
| HFrEF | Heart failure with reduced ejection fraction |
| LBBB | Left bundle branch block |
| LV | Left ventricle |
| LTAT | Left thorax activation times |
| NICD | Non-specific intraventricular conduction delay |
| RV | Right ventricle |
| RVAP | Right ventricular apical pacing |
| SDAT | Standard deviation of activation times |
| SSI | Systolic stretch index |
| TAT | Total activation time |
| VEU | Ventricular electrical uncoupling |
References
- Adabag, S.; Roukoz, H.; Anand, I.S.; Moss, A.J. Cardiac Resynchronization Therapy in Patients with Minimal Heart Failure: A Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2011, 58, 935–941. [Google Scholar] [CrossRef]
- 2021 ESC Guidelines on Cardiac Pacing and Cardiac Resynchronization Therapy|European Heart Journal|Oxford Academic. Available online: https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehab364/6358547 (accessed on 2 September 2021).
- Maass, A.H.; Vernooy, K.; Wijers, S.C.; van’t Sant, J.; Cramer, M.J.; Meine, M.; Allaart, C.P.; De Lange, F.J.; Prinzen, F.W.; Gerritse, B.; et al. Refining Success of Cardiac Resynchronization Therapy Using a Simple Score Predicting the Amount of Reverse Ventricular Remodelling: Results from the Markers and Response to CRT (MARC) Study. Europace 2018, 20, e1–e10. [Google Scholar] [CrossRef]
- Strik, M.; Ploux, S.; Jankelson, L.; Bordachar, P. Non-Invasive Cardiac Mapping for Non-Response in Cardiac Resynchronization Therapy. Ann. Med. 2019, 51, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Strik, M.; Ploux, S.; Vernooy, K.; Prinzen, F.W. Cardiac Resynchronization Therapy: Refocus on the Electrical Substrate. Circ. J. 2011, 75, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Abu-Alrub, S.; Strik, M.; Huntjens, P.; Haïssaguerre, M.; Eschalier, R.; Bordachar, P.; Ploux, S. The Role of Electrocardiographic Imaging in Patient Selection for Cardiac Resynchronization Therapy. J. Geriatr. Cardiol. 2021, 18, 836–843. [Google Scholar] [CrossRef]
- Jia, P.; Ramanathan, C.; Ghanem, R.N.; Ryu, K.; Varma, N.; Rudy, Y. Electrocardiographic Imaging of Cardiac Resynchronization Therapy in Heart Failure: Observation of Variable Electrophysiologic Responses. Heart Rhythm. 2006, 3, 296–310. [Google Scholar] [CrossRef]
- Duchateau, J.; Sacher, F.; Pambrun, T.; Derval, N.; Chamorro-Servent, J.; Denis, A.; Ploux, S.; Hocini, M.; Jaïs, P.; Bernus, O.; et al. Performance and Limitations of Noninvasive Cardiac Activation Mapping. Heart Rhythm. 2019, 16, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Myerburg, R.J.; Nilsson, K.; Gelband, H. Physiology of Canine Intraventricular Conduction and Endocardial Excitation. Circ. Res. 1972, 30, 217–243. [Google Scholar] [CrossRef]
- Rodriguez, L.-M.; Timmermans, C.; Nabar, A.; Beatty, G.; Wellens, H.J.J. Variable Patterns of Septal Activation in Patients with Left Bundle Branch Block and Heart Failure. J. Cardiovasc. Electrophysiol. 2003, 14, 135–141. [Google Scholar] [CrossRef]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Gjesdal, O.; Edvardsen, T.; Smiseth, O.A. Assessment of Wasted Myocardial Work: A Novel Method to Quantify Energy Loss Due to Uncoordinated Left Ventricular Contractions. Am. J. Physiol.-Heart Circ. Physiol. 2013, 305, H996–H1003. [Google Scholar] [CrossRef]
- Prinzen, F.W.; Hunter, W.C.; Wyman, B.T.; McVeigh, E.R. Mapping of Regional Myocardial Strain and Work during Ventricular Pacing: Experimental Study Using Magnetic Resonance Imaging Tagging. J. Am. Coll. Cardiol. 1999, 33, 1735–1742. [Google Scholar] [CrossRef] [PubMed]
- van Oosterhout, M.F.M.; Prinzen, F.W.; Arts, T.; Schreuder, J.J.; Vanagt, W.Y.R.; Cleutjens, J.P.M.; Reneman, R.S. Asynchronous Electrical Activation Induces Asymmetrical Hypertrophy of the Left Ventricular Wall. Circulation 1998, 98, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Boerth, R.C.; Covell, J.W. Mechanical Performance and Efficiency of the Left Ventricle during Ventricular Stimulation. Am. J. Physiol.-Leg. Content 1971, 221, 1686–1691. [Google Scholar] [CrossRef] [PubMed]
- Caputo, M.L.; van Stipdonk, A.; Illner, A.; D’Ambrosio, G.; Regoli, F.; Conte, G.; Moccetti, T.; Klersy, C.; Prinzen, F.W.; Vernooy, K.; et al. The Definition of Left Bundle Branch Block Influences the Response to Cardiac Resynchronization Therapy. Int. J. Cardiol. 2018, 269, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Jastrzębski, M.; Kukla, P.; Kisiel, R.; Fijorek, K.; Moskal, P.; Czarnecka, D. Comparison of Four LBBB Definitions for Predicting Mortality in Patients Receiving Cardiac Resynchronization Therapy. Ann. Noninvasive Electrocardiol. 2018, 23, e12563. [Google Scholar] [CrossRef] [PubMed]
- Ploux, S.; Lumens, J.; Whinnett, Z.; Montaudon, M.; Strom, M.; Ramanathan, C.; Derval, N.; Zemmoura, A.; Denis, A.; De Guillebon, M.; et al. Noninvasive Electrocardiographic Mapping to Improve Patient Selection for Cardiac Resynchronization Therapy: Beyond QRS Duration and Left Bundle Branch Block Morphology. J. Am. Coll. Cardiol. 2013, 61, 2435–2443. [Google Scholar] [CrossRef]
- Abu-Alrub, S.; Strik, M.; Huntjens, P.; Ramirez, F.D.; Potse, M.; Cochet, H.; Marchand, H.; Buliard, S.; Eschalier, R.; Haïssaguerre, M.; et al. Left-Axis Deviation in Patients with Nonischemic Heart Failure and Left Bundle Branch Block Is a Purely Electrical Phenomenon. Heart Rhythm. 2021, 18, 1352–1360. [Google Scholar] [CrossRef]
- Eschalier, R.; Ploux, S.; Lumens, J.; Whinnett, Z.; Varma, N.; Meillet, V.; Ritter, P.; Jaïs, P.; Haïssaguerre, M.; Bordachar, P. Detailed Analysis of Ventricular Activation Sequences during Right Ventricular Apical Pacing and Left Bundle Branch Block and the Potential Implications for Cardiac Resynchronization Therapy. Heart Rhythm. 2015, 12, 137–143. [Google Scholar] [CrossRef]
- Strik, M.; Ploux, S.; Huntjens, P.R.; Nguyên, U.C.; Frontera, A.; Eschalier, R.; Dubois, R.; Ritter, P.; Klotz, N.; Vernooy, K.; et al. Response to Cardiac Resynchronization Therapy Is Determined by Intrinsic Electrical Substrate Rather than by Its Modification. Int. J. Cardiol. 2018, 270, 143–148. [Google Scholar] [CrossRef]
- van Stipdonk, A.M.W.; ter Horst, I.; Kloosterman, M.; Engels, E.B.; Rienstra, M.; Crijns, H.J.G.M.; Vos, M.A.; van Gelder, I.C.; Prinzen, F.W.; Meine, M.; et al. QRS Area Is a Strong Determinant of Outcome in Cardiac Resynchronization Therapy. Circ. Arrhythmia Electrophysiol. 2018, 11, e006497. [Google Scholar] [CrossRef]
- Ploux, S.; Eschalier, R.; Whinnett, Z.I.; Lumens, J.; Derval, N.; Sacher, F.; Hocini, M.; Jaïs, P.; Dubois, R.; Ritter, P.; et al. Electrical Dyssynchrony Induced by Biventricular Pacing: Implications for Patient Selection and Therapy Improvement. Heart Rhythm. 2015, 12, 782–791. [Google Scholar] [CrossRef]
- van Stipdonk, A.M.W.; Rad, M.M.; Luermans, J.G.L.M.; Crijns, H.J.; Prinzen, F.W.; Vernooy, K. Identifying Delayed Left Ventricular Lateral Wall Activation in Patients with Non-Specific Intraventricular Conduction Delay Using Coronary Venous Electroanatomical Mapping. Neth. Heart J. 2016, 24, 58–65. [Google Scholar] [CrossRef]
- Massacesi, C.; Ceriello, L.; Maturo, F.; Porreca, A.; Appignani, M.; Di Girolamo, E. Cardiac Resynchronization Therapy with Multipoint Pacing via Quadripolar Lead versus Traditional Biventricular Pacing: A Systematic Review and Meta-Analysis of Clinical Studies on Hemodynamic, Clinical, and Prognostic Parameters. Heart Rhythm O2 2021, 2, 682–690. [Google Scholar] [CrossRef]
- Leclercq, C.; Burri, H.; Delnoy, P.P.; Rinaldi, C.A.; Sperzel, J.; Calò, L.; Concha, J.F.; Fusco, A.; Al Samadi, F.; Lee, K.; et al. Cardiac Resynchronization Therapy Non-Responder to Responder Conversion Rate in the MORE-CRT MPP Trial. Europace 2023, 25, euad294. [Google Scholar] [CrossRef]
- Elliott, M.K.; Strocchi, M.; Sieniewicz, B.J.; Sidhu, B.; Mehta, V.; Wijesuriya, N.; Behar, J.M.; Thorpe, A.; Martic, D.; Wong, T.; et al. Biventricular Endocardial Pacing and Left Bundle Branch Area Pacing for Cardiac Resynchronization: Mechanistic Insights from Electrocardiographic Imaging, Acute Hemodynamic Response, and Magnetic Resonance Imaging. Heart Rhythm. 2023, 20, 207–216. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, H.; Hou, X.; Wang, Z.; Zou, F.; Qian, Z.; Wei, Y.; Wang, X.; Zhang, L.; Li, X.; et al. Randomized Trial of Left Bundle Branch vs Biventricular Pacing for Cardiac Resynchronization Therapy. J. Am. Coll. Cardiol. 2022, 80, 1205–1216. [Google Scholar] [CrossRef]
- Parreira, L.; Tsyganov, A.; Artyukhina, E.; Vernooy, K.; Tondo, C.; Adragao, P.; Ascione, C.; Carmo, P.; Carvalho, S.; Egger, M.; et al. Non-Invasive Three-Dimensional Electrical Activation Mapping to Predict Cardiac Resynchronization Therapy Response: Site of Latest Left Ventricular Activation Relative to Pacing Site. EP Eur. 2023, 25, 1458–1466. [Google Scholar] [CrossRef]
- Nguyên, U.C.; Cluitmans, M.J.M.; Strik, M.; Luermans, J.G.; Gommers, S.; Wildberger, J.E.; Bekkers, S.C.A.M.; Volders, P.G.A.; Mihl, C.; Prinzen, F.W.; et al. Integration of Cardiac Magnetic Resonance Imaging, Electrocardiographic Imaging, and Coronary Venous Computed Tomography Angiography for Guidance of Left Ventricular Lead Positioning. EP Eur. 2019, 21, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Whinnett, Z.I.; Francis, D.P.; Denis, A.; Willson, K.; Pascale, P.; van Geldorp, I.; De Guillebon, M.; Ploux, S.; Ellenbogen, K.; Haïssaguerre, M.; et al. Comparison of Different Invasive Hemodynamic Methods for AV Delay Optimization in Patients with Cardiac Resynchronization Therapy: Implications for Clinical Trial Design and Clinical Practice. Int. J. Cardiol. 2013, 168, 2228–2237. [Google Scholar] [CrossRef] [PubMed]
- Huntjens, P.R.; Ploux, S.; Strik, M.; Walmsley, J.; Ritter, P.; Haissaguerre, M.; Prinzen, F.W.; Delhaas, T.; Lumens, J.; Bordachar, P. Electrical Substrates Driving Response to Cardiac Resynchronization Therapy: A Combined Clinical–Computational Evaluation. Circ. Arrhythm. Electrophysiol. 2018, 11, e005647. [Google Scholar] [CrossRef] [PubMed]
- Lumens, J.; Ploux, S.; Strik, M.; Gorcsan, J.; Cochet, H.; Derval, N.; Strom, M.; Ramanathan, C.; Ritter, P.; Haïssaguerre, M.; et al. Comparative Electromechanical and Hemodynamic Effects of Left Ventricular and Biventricular Pacing in Dyssynchronous Heart Failure. J. Am. Coll. Cardiol. 2013, 62, 2395–2403. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.K.; Blauer, J.; Mehta, V.S.; Sidhu, B.S.; Gould, J.; Jackson, T.; Sieniewicz, B.; Niederer, S.; Ghosh, S.; Rinaldi, C.A. Comparison of Electrical Dyssynchrony Parameters between Electrocardiographic Imaging and a Simulated ECG Belt. J. Electrocardiol. 2021, 68, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Gage, R.M.; Curtin, A.E.; Burns, K.V.; Ghosh, S.; Gillberg, J.M.; Bank, A.J. Changes in Electrical Dyssynchrony by Body Surface Mapping Predict Left Ventricular Remodeling in Patients with Cardiac Resynchronization Therapy. Heart Rhythm. 2017, 14, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Rickard, J.; Jackson, K.; Gold, M.; Biffi, M.; Ziacchi, M.; Silverstein, J.; Ramza, B.; Metzl, M.; Grubman, E.; Abben, R.; et al. Electrocardiogram Belt Guidance for Left Ventricular Lead Placement and Biventricular Pacing Optimization. Heart Rhythm. 2023, 20, 537–544. [Google Scholar] [CrossRef]
- Lumens, J.; Tayal, B.; Walmsley, J.; Delgado-Montero, A.; Huntjens, P.R.; Schwartzman, D.; Althouse, A.D.; Delhaas, T.; Prinzen, F.W.; Gorcsan, J. Differentiating Electromechanical From Non–Electrical Substrates of Mechanical Discoordination to Identify Responders to Cardiac Resynchronization Therapy. Circ. Cardiovasc. Imaging 2015, 8, e003744. [Google Scholar] [CrossRef]
- Gorcsan, J.; Anderson, C.P.; Tayal, B.; Sugahara, M.; Walmsley, J.; Starling, R.C.; Lumens, J. Systolic Stretch Characterizes the Electromechanical Substrate Responsive to Cardiac Resynchronization Therapy. JACC Cardiovasc. Imaging 2018, 12, 1741–1752. [Google Scholar] [CrossRef]
- Thibault, B.; Harel, F.; Ducharme, A.; White, M.; Ellenbogen, K.A.; Frasure-Smith, N.; Roy, D.; Philippon, F.; Dorian, P.; Talajic, M.; et al. Cardiac Resynchronization Therapy in Patients With Heart Failure and a QRS Complex < 120 Milliseconds. Circulation 2013, 127, 873–881. [Google Scholar] [CrossRef]
- Wong, J.A.; Yee, R.; Stirrat, J.; Scholl, D.; Krahn, A.D.; Gula, L.J.; Skanes, A.C.; Leong-Sit, P.; Klein, G.J.; McCarty, D.; et al. Influence of Pacing Site Characteristics on Response to Cardiac Resynchronization Therapy. Circ. Cardiovasc. Imaging 2013, 6, 542–550. [Google Scholar] [CrossRef]
- Chen, Z.; Sohal, M.; Sammut, E.; Child, N.; Jackson, T.; Claridge, S.; Cooklin, M.; O’Neill, M.; Wright, M.; Gill, J.; et al. Focal But Not Diffuse Myocardial Fibrosis Burden Quantification Using Cardiac Magnetic Resonance Imaging Predicts Left Ventricular Reverse Modeling Following Cardiac Resynchronization Therapy. J. Cardiovasc. Electrophysiol. 2016, 27, 203–209. [Google Scholar] [CrossRef]
- Arts, T.; Delhaas, T.; Bovendeerd, P.; Verbeek, X.; Prinzen, F.W. Adaptation to Mechanical Load Determines Shape and Properties of Heart and Circulation: The CircAdapt Model. Am. J. Physiol.-Heart Circ. Physiol. 2005, 288, H1943–H1954. [Google Scholar] [CrossRef]
- de Roest, G.J.; Allaart, C.P.; Kleijn, S.A.; Delnoy, P.P.H.M.; Wu, L.; Hendriks, M.L.; Bronzwaer, J.G.F.; van Rossum, A.C.; de Cock, C.C. Prediction of Long-Term Outcome of Cardiac Resynchronization Therapy by Acute Pressure-Volume Loop Measurements. Eur. J. Heart Fail. 2013, 15, 299–307. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Alrub, S.; Strik, M.; Huntjens, P.; Haïssaguerre, M.; Eschalier, R.; Bordachar, P.; Ploux, S. Current Role of Electrocardiographic Imaging in Patient Selection for Cardiac Resynchronization Therapy. J. Cardiovasc. Dev. Dis. 2024, 11, 24. https://doi.org/10.3390/jcdd11010024
Abu-Alrub S, Strik M, Huntjens P, Haïssaguerre M, Eschalier R, Bordachar P, Ploux S. Current Role of Electrocardiographic Imaging in Patient Selection for Cardiac Resynchronization Therapy. Journal of Cardiovascular Development and Disease. 2024; 11(1):24. https://doi.org/10.3390/jcdd11010024
Chicago/Turabian StyleAbu-Alrub, Saer, Marc Strik, Peter Huntjens, Michel Haïssaguerre, Romain Eschalier, Pierre Bordachar, and Sylvain Ploux. 2024. "Current Role of Electrocardiographic Imaging in Patient Selection for Cardiac Resynchronization Therapy" Journal of Cardiovascular Development and Disease 11, no. 1: 24. https://doi.org/10.3390/jcdd11010024
APA StyleAbu-Alrub, S., Strik, M., Huntjens, P., Haïssaguerre, M., Eschalier, R., Bordachar, P., & Ploux, S. (2024). Current Role of Electrocardiographic Imaging in Patient Selection for Cardiac Resynchronization Therapy. Journal of Cardiovascular Development and Disease, 11(1), 24. https://doi.org/10.3390/jcdd11010024