
Increasing Lifestyle Walking by 3000 Steps per Day Reduces Blood Pressure in Sedentary Older Adults with Hypertension: Results from an e-Health Pilot Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
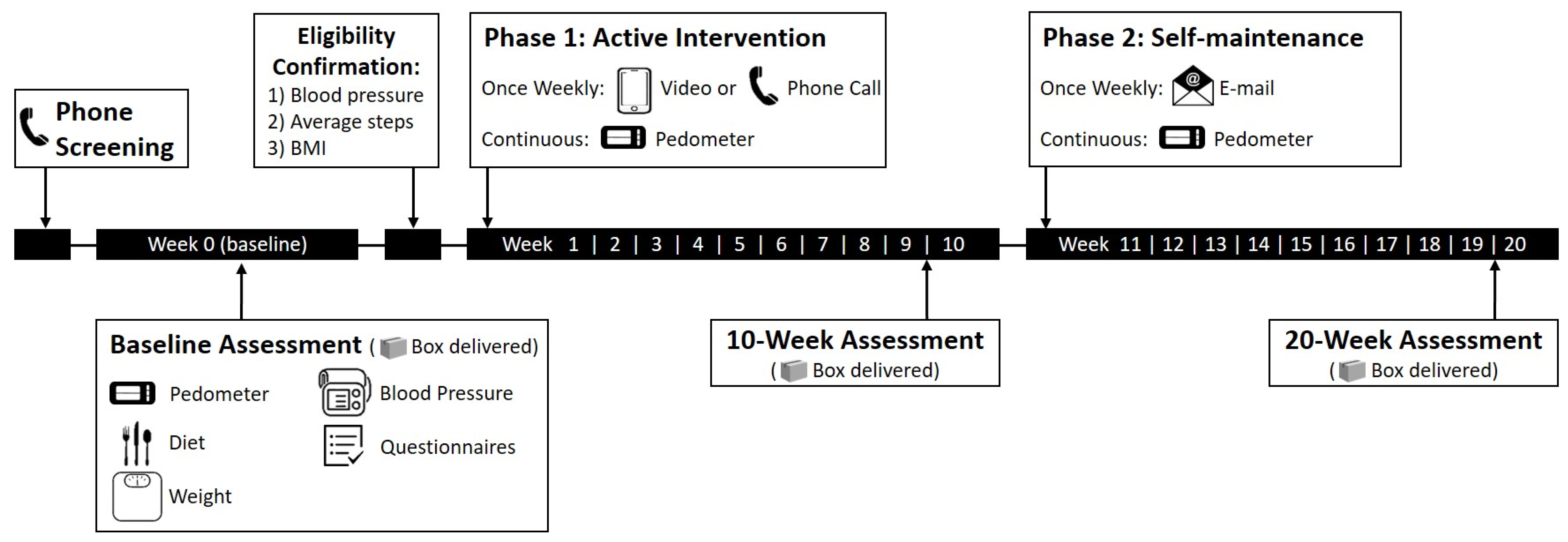
2.2. Study Design
2.2.1. Assessments
2.2.2. Intervention
2.3. Statistical Analysis
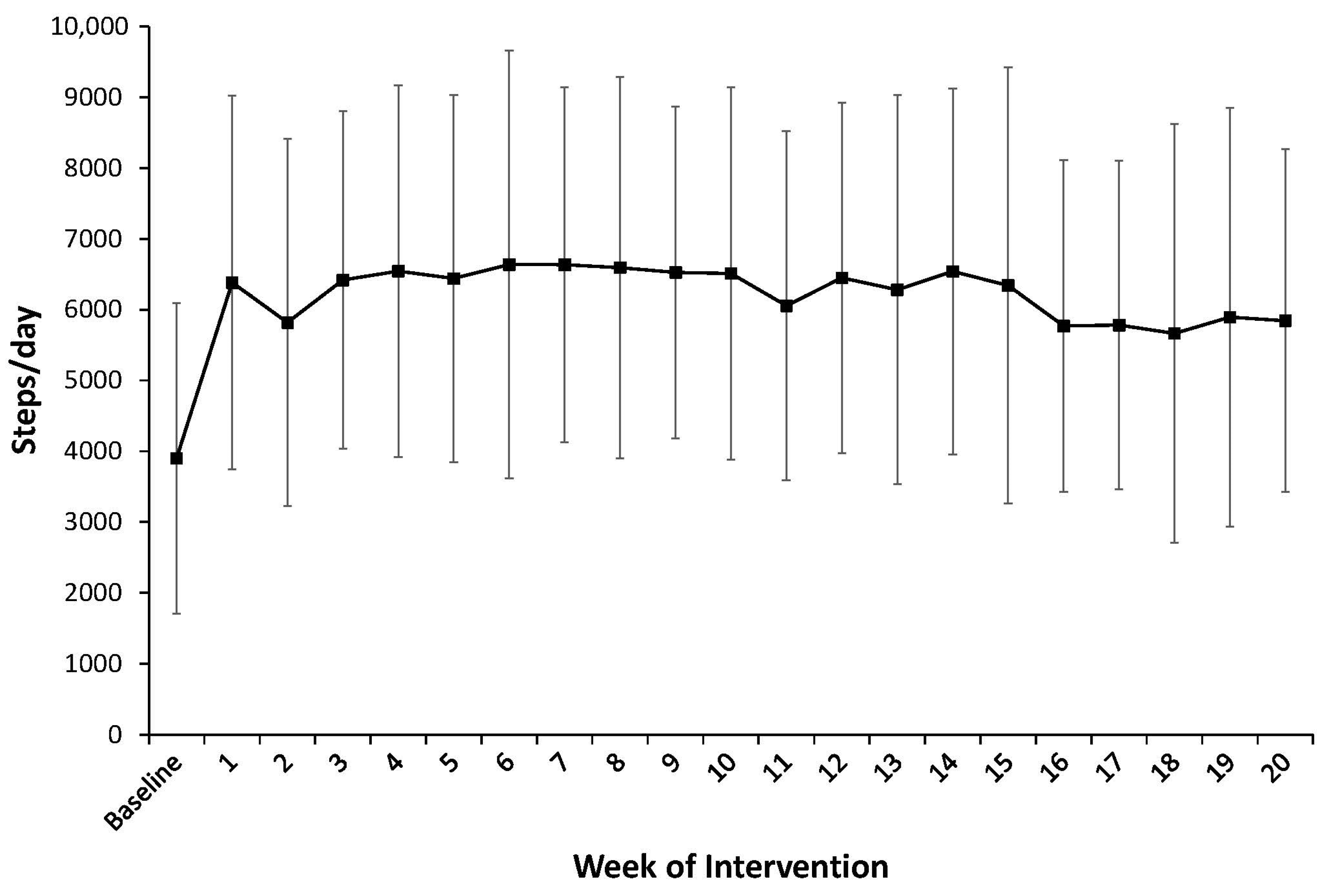
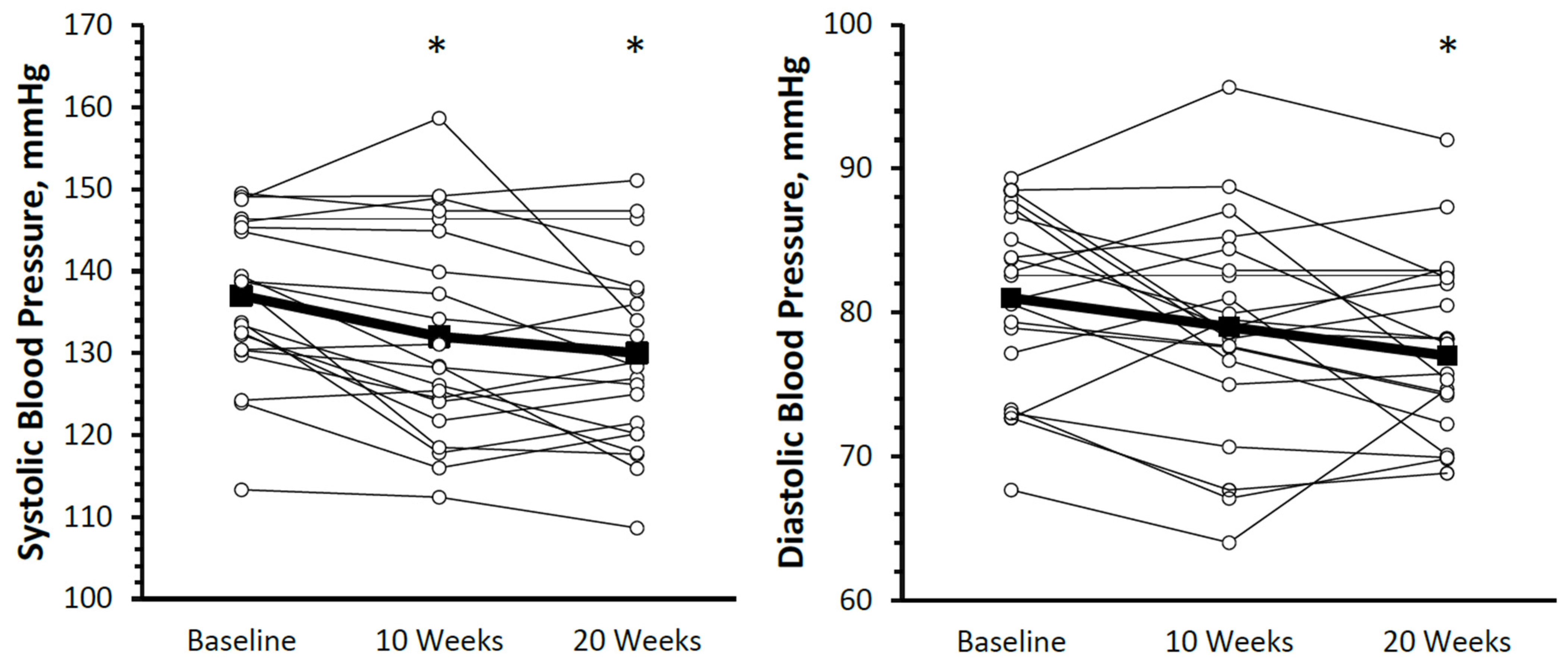
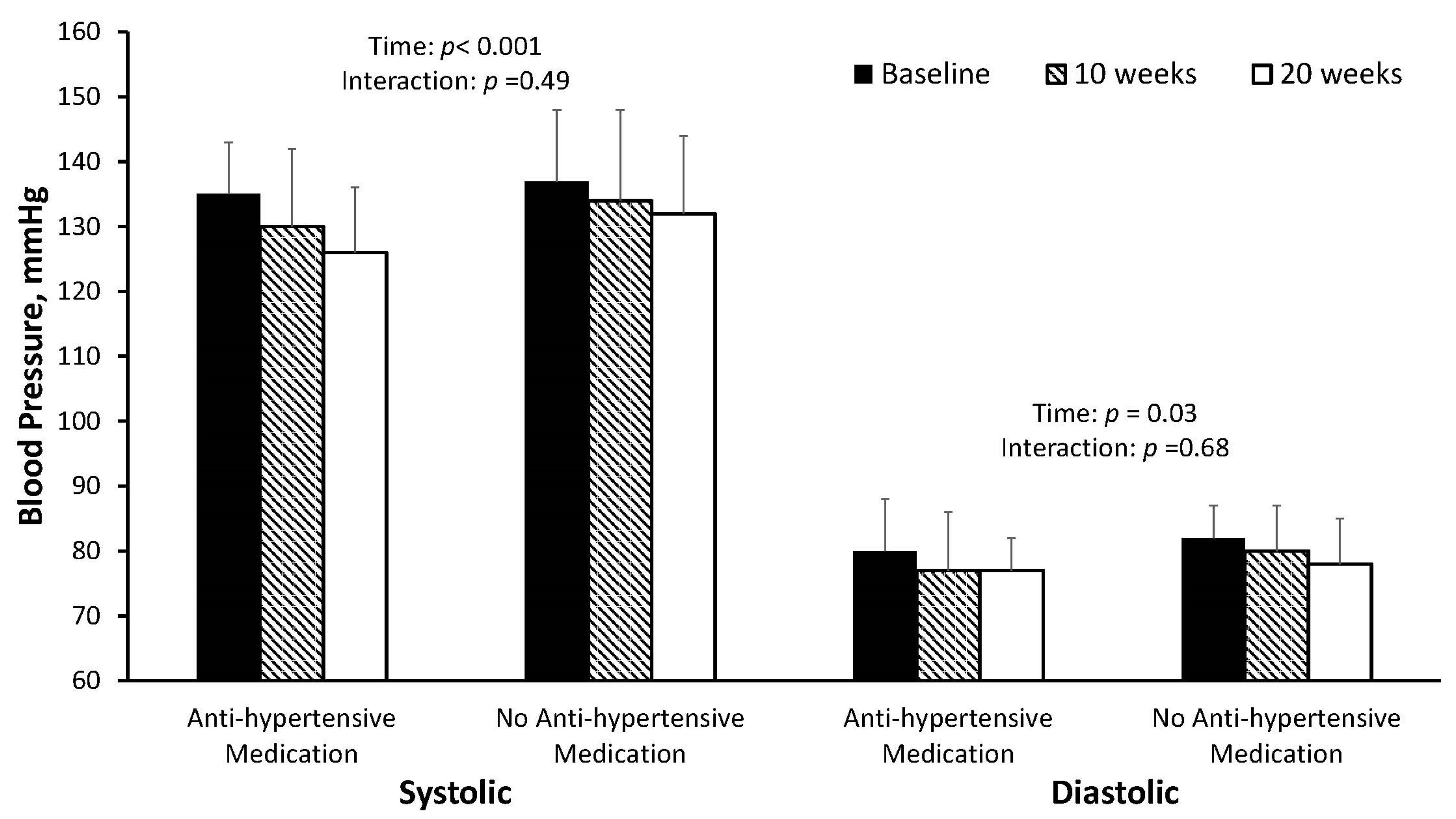
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, B.B.; Hivert, M.-F.; Jerome, G.J.; Kraus, W.E.; Rosenkranz, S.K.; Schorr, E.N.; Spartano, N.L.; Lobelo, F.; American Heart Association Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; et al. Physical activity as a critical component of first-line treatment for elevated blood pressure or cholesterol: Who, what, and how? A scientific statement from the American Heart Association. Hypertension 2021, 78, e26–e37. [Google Scholar]
- Schutzer, K.A.; Graves, B.S. Barriers and motivations to exercise in older adults. Prev. Med. 2004, 39, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Van Roie, E.; Delecluse, C.; Opdenacker, J.; De Bock, K.; Kennis, E.; Boen, F. Effectiveness of a lifestyle physical activity versus a structured exercise intervention in older adults. J. Aging Phys. Act. 2010, 18, 335–352. [Google Scholar] [CrossRef]
- Dunn, A.L.; Marcus, B.H.; Kampert, J.B.; Garcia, M.E.; Kohl, H.W.; Blair, S.N. Comparison of lifestyle and structured interventions to increase physical activity and cardiorespiratory fitness: A randomized trial. J. Am. Med. Assoc. 1999, 281, 327–334. [Google Scholar] [CrossRef]
- Valenti, G.; Bonomi, A.G.; Westerterp, K.R. Walking as a contributor to physical activity in healthy older adults: 2 week longitudinal study using accelerometry and the doubly labeled water method. JMIR mHealth uHealth 2016, 4, e56. [Google Scholar] [CrossRef]
- Kwan, R.Y.C.; Salihu, D.; Lee, P.H.; Tse, M.; Cheung, D.S.K.; Roopsawang, I.; Choi, K.S. The effect of e-health interventions promoting physical activity in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 7–17. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Bassett, D.R., Jr.; Rutherford, W.J.; Ainsworth, B.E.; Chan, C.B.; Croteau, K.; Giles-Corti, B.; Le Masurier, G.; Moreau, K.; Mrozek, J.; et al. BMI-referenced cut points for pedometer-determined steps per day in adults. J. Phys. Act. Health 2008, 5 (Suppl. S1), S126–S139. [Google Scholar] [CrossRef]
- Wyatt, H.R.; Peters, J.C.; Reed, G.W.; Barry, M.; Hill, J.O. A Colorado statewide survey of walking and its relation to excessive weight. Med. Sci. Sports Exerc. 2005, 37, 724–730. [Google Scholar] [CrossRef]
- Paluch, A.E.; Bajpai, S.; Bassett, D.R.; Carnethon, M.R.; Ekelund, U.; Evenson, K.R.; Galuska, D.A.; Jefferis, B.J.; Kraus, W.E.; Lee, I.-M. Daily steps and all-cause mortality: A meta-analysis of 15 international cohorts. Lancet Public Health 2022, 7, e219–e228. [Google Scholar] [CrossRef]
- Bassett, D.R.; Wyatt, H.R.; Thompson, H.; Peters, J.C.; Hill, J.O. Pedometer-measured physical activity and health behaviors in U.S. adults. Med. Sci. Sports Exerc. 2010, 42, 1819–1825. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Schuna, J.M.; Barreira, T.V.; Mire, E.F.; Broyles, S.T.; Katzmarzyk, P.T.; Johnson, W.D. Normative steps/day values for older adults: NHANES 2005–2006. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 1426–1432. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; US Dept of Health and Human Services: Washington, DC, USA, 2018. [Google Scholar]
- Bravata, D.M.; Smith-Spangler, C.; Sundaram, V.; Gienger, A.L.; Lin, N.; Lewis, R.; Stave, C.D.; Olkin, I.; Sirard, J.R. Using pedometers to increase physical activity and improve health: A systematic review. J. Am. Med. Assoc. 2007, 298, 2296–2304. [Google Scholar] [CrossRef]
- Tudor-locke, C.; Bassett, D.R. How many steps/day are enough? Preliminary pedometer indices for public health. Sport. Med. 2004, 34, 1–8. [Google Scholar] [CrossRef]
- Baker, G.; Gray, S.R.; Wright, A.; Fitzsimons, C.; Nimmo, M.; Lowry, R.; Mutrie, N.; The Scottish Physical Activity Research Collaboration (SPARColl). The effect of a pedometer-based community walking intervention “Walking for Wellbeing in the West” on physical activity levels and health outcomes: A 12-week randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 44. [Google Scholar] [CrossRef]
- Moreau, K.L.; Degarmo, R.; Langley, J.; McMahon, C.; Howley, E.T.; Bassett, D.R.; Thompson, D. Increasing daily walking lowers blood pressure in postmenopausal women. Med. Sci. Sports. Exerc. 2001, 33, 1825–1831. [Google Scholar] [CrossRef]
- Hornbuckle, L.M.; Kingsley, J.D.; Kushnick, M.R.; Moffatt, R.J.; Haymes, E.M.; Miles, R.; Toole, T.; Panton, L.B. Effects of a 12-month pedometer-based walking intervention in women of low socioeconomic status. Clin. Med. Insights Women’s Health 2016, 9 (Suppl. S1), 75–84. [Google Scholar] [CrossRef]
- van der Bij, A.K.; Laurant, M.G.H.; Wensing, M. Effectiveness of physical activity interventions for older adults. Am. J. Prev. Med. 2002, 22, 120–133. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Jordan, A.N.; Jurca, G.M.; Locke, C.T.; Church, T.S.; Blair, S.N. Pedometer indices for weekly physical activity recommendations in postmenopausal women. Med. Sci. Sports Exerc. 2005, 37, 1627–1632. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Pr. Hypertension 2018, 71, 1269–1324. [Google Scholar] [CrossRef] [PubMed]
- Albin, E.E.; Brellenthin, A.G.; Lang, J.A.; Meyer, J.D.; Lee, D. Cardiorespiratory fitness and muscular strength on arterial stiffness in older adults. Med. Sci. Sport. Exerc. 2020, 52, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Kirkpatrick, S.I.; Mittl, B.; Zimmerman, T.P.; Thompson, F.E.; Bingley, C.; Willis, G.; Islam, N.G.; Baranowski, T.; McNutt, S.; et al. The Automated Self-Administered 24-hour dietary recall (ASA24): A resource for researchers, clinicians, and educators from the National Cancer Institute. J. Acad. Nutr. Diet. 2012, 112, 1134–1137. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Dixit-Joshi, S.; Potischman, N.; Dodd, K.W.; Kirkpatrick, S.I.; Kushi, L.H.; Alexander, G.L.; Coleman, L.A.; Zimmerman, T.P.; Sundaram, M.E. Comparison of Interviewer-Administered and Automated Self-Administered 24-Hour Dietary Recalls in 3 Diverse Integrated Health Systems. Am. J. Epidemiol. 2015, 181, 970–978. [Google Scholar] [CrossRef] [PubMed]
- Verplanken, B.; Orbell, S. Reflections on past behavior: A self-report index of habit strength. J. Appl. Soc. Psychol. 2003, 33, 1313–1330. [Google Scholar] [CrossRef]
- Caudroit, J.; Stephan, Y.; Le Scanff, C. Social cognitive determinants of physical activity among retired older individuals: An application of the health action process approach. Br. J. Health Psychol. 2011, 16, 404–417. [Google Scholar] [CrossRef]
- Parschau, L.; Barz, M.; Richert, J.; Knoll, N.; Lippke, S.; Schwarzer, R. Physical activity among adults with obesity: Testing the health action process approach. Rehabil. Psychol. 2014, 59, 42–49. [Google Scholar] [CrossRef]
- Boulton, E.; Hawley-Hague, H.; French, D.P.; Mellone, S.; Zacchi, A.; Clemson, L.; Vereijken, B.; Todd, C. Implementing behaviour change theory and techniques to increase physical activity and prevent functional decline among adults aged 61–70: The PreventIT project. Prog. Cardiovasc. Dis. 2019, 62, 147–156. [Google Scholar] [CrossRef]
- Huang, Y.; Xu, J.; Yu, B.; Shull, P.B. Validity of FitBit, Jawbone UP, Nike+ and other wearable devices for level and stair walking. Gait. Posture 2016, 48, 36–41. [Google Scholar] [CrossRef]
- Lefferts, E.C.; Bakker, E.A.; Carbone, S.; Lavie, C.J.; Lee, D. Associations of total and aerobic steps with the prevalence and incidence of frailty in older adults with hypertension. Prog. Cardiovasc. Dis. 2021, 67, 18–25. [Google Scholar] [CrossRef]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef]
- Kolt, G.S.; Schofield, G.M.; Kerse, N.; Garrett, N.; Ashton, T.; Patel, A. Healthy Steps Trial: Pedometer-based advice and physical activity for low-active older adults. Ann. Fam. Med. 2012, 10, 206–212. [Google Scholar] [CrossRef]
- Lee, L.L.; Arthur, A.; Avis, M. Evaluating a community-based walking intervention for hypertensive older people in Taiwan: A randomized controlled trial. Prev. Med. 2007, 44, 160–166. [Google Scholar] [CrossRef]
- Tully, M.A.; Cupples, M.E.; Chan, W.S.; McGlade, K.; Young, I.S. Brisk walking, fitness, and cardiovascular risk: A randomized controlled trial in primary care. Prev. Med. 2005, 41, 622–628. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Bell, R.C.; Myers, A.M.; Harris, S.B.; Ecclestone, N.A.; Lauzon, N.; Rodger, N.W. Controlled outcome evaluation of the First Step Program: A daily physical activity intervention for individuals with type II diabetes. Int. J. Obes. 2004, 28, 113–119. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Schuna, J.M.; Swift, D.L.; Dragg, A.T.; Davis, A.B.; Martin, C.K.; Johnson, W.D.; Church, T.S. Evaluation of step-counting interventions differing on intensity messages. J. Phys. Act. Health 2020, 17, 21–28. [Google Scholar] [CrossRef]
- Hamdorf, P.A.; Penhall, R.K. Walking with its training effects on the fitness and activity patterns of 79–91 year old females. Aust. N. Z. J. Med. 1999, 29, 22–28. [Google Scholar] [CrossRef]
- Chan, A.W.K.; Chair, S.Y.; Lee, D.T.F.; Leung, D.Y.P.; Sit, J.W.H.; Cheng, H.Y.; Taylor-Piliae, R.E. Tai Chi exercise is more effective than brisk walking in reducing cardiovascular disease risk factors among adults with hypertension: A randomised controlled trial. Int. J. Nurs. Stud. 2018, 88, 44–52. [Google Scholar] [CrossRef]
- Dasgupta, K.; Rosenberg, E.; Joseph, L.; Cooke, A.B.; Trudeau, L.; Bacon, S.L.; Chan, D.; Sherman, M.; Rabasa-Lhoret, R.; Daskalopoulou, S.S.; et al. Physician step prescription and monitoring to improve ARTERial health (SMARTER): A randomized controlled trial in patients with type 2 diabetes and hypertension. Diabetes Obes. Metab. 2017, 19, 695–704. [Google Scholar] [CrossRef]
- Seals, D.R.; Silverman, H.G.; Reiling, M.J.; Davy, K.P. Effect of regular aerobic exercise on elevated blood pressure in postmenopausal women. Am. J. Cardiol. 1997, 80, 49–55. [Google Scholar] [CrossRef]
- Stewart, K.J.; Bacher, A.C.; Turner, K.L.; Fleg, J.L.; Hees, P.S.; Shapiro, E.P.; Tayback, M.; Ouyang, P. Effect of exercise on blood pressure in older persons. Arch. Intern. Med. 2005, 165, 756. [Google Scholar] [CrossRef] [PubMed]
- Ohkubo, T.; Hozawa, A.; Nagatomi, R.; Fujita, K.; Sauvaget, C.; Watanabe, Y.; Anzai, Y.; Tamagawa, A.; Tsuji, I.; Imai, Y.; et al. Effects of exercise training on home blood pressure values in older adults: A randomized controlled trial. J. Hypertens. 2001, 19, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Hear. Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef] [PubMed]
- Herrod, P.J.; Doleman, B.; Blackwell, J.E.; O’Boyle, F.; Williams, J.P.; Lund, J.N.; Phillips, B.E. Exercise and other nonpharmacological strategies to reduce blood pressure in older adults: A systematic review and meta-analysis. J. Am. Soc. Hypertens. 2018, 12, 248–267. [Google Scholar] [CrossRef]
- Lyons, E.J.; Swartz, M.C.; Lewis, Z.H.; Martinez, E.; Jennings, K. Feasibility and acceptability of a wearable technology physical activity intervention with telephone counseling for mid-aged and older adults: A randomized controlled pilot trial. JMIR mHealth uHealth 2017, 5, e28. [Google Scholar] [CrossRef]
- Rowley, T.W.; Lenz, E.K.; Swartz, A.M.; Miller, N.E.; Maeda, H.; Strath, S.J. Efficacy of an individually tailored, internet-mediated physical activity intervention in older adults: A randomized controlled trial. J. Appl. Gerontol. 2019, 38, 1011–1022. [Google Scholar] [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W.; The Lancet Physical Activity Series Working Group. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Lim, C. Understanding action control of daily walking behavior among dog owners: A community survey. BMC Public Health 2016, 16, 1165. [Google Scholar] [CrossRef]
- Whelton, P.K.; He, J.; Appel, L.J.; Cutler, J.A.; Havas, S.; Kotchen, T.A.; Roccella, E.J.; Stout, R.; Vallbona, C.; Winston, M.C.; et al. Primary prevention of hypertension: Clinical and public health advisory from The National High Blood Pressure Education Program. JAMA 2002, 288, 1882–1888. [Google Scholar] [CrossRef]
- Cook, N.R.; Cohen, J.; Hebert, P.R.; Taylor, J.O.; Hennekens, C.H. Implications of small reductions in diastolic blood pressure for primary prevention. Arch. Intern. Med. 1995, 155, 701–709. [Google Scholar] [CrossRef]
- Pal, S.; Cheng, C.; Egger, G.; Binns, C.; Donovan, R. Using pedometers to increase physical activity in overweight and obese women: A pilot study. BMC Public Health 2009, 9, 309. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All | Male | Female |
|---|---|---|---|
| n | 21 | 8 | 13 |
| Age, yrs | 73 ± 5 | 73 ± 6 | 73 ± 5 |
| Height, cm | 167.6 ± 8.9 | 174.5 ± 7.9 | 162.4 ± 5.1 |
| Weight, kg | 85.9 ± 13.9 | 93.8 ± 12.2 | 81.1 ± 12.9 |
| BMI, kg/m2 | 30.7 ± 4.2 | 30.9 ± 4.1 | 30.7 ± 4.3 |
| Steps, steps/day | 3899 ± 2198 | 4656 ± 2093 | 3434 ± 2208 |
| Systolic blood pressure, mm Hg | 137 ± 10 | 138 ± 9 | 136 ± 10 |
| Diastolic blood pressure, mm Hg | 81 ± 6 | 83 ± 7 | 80 ± 6 |
| Resting heart rate, bpm | 70 ± 7 | 69 ± 6 | 72 ± 7 |
| Medication usage, n (%) | |||
| Anti-hypertensives | 8 (39) | 3 (38) | 5 (38) |
| Statins | 9 (43) | 2 (25) | 7 (54) |
| Characteristic | Baseline | 10 Weeks | 20 Weeks | Overall Time Effect p-Value | Effect Size a (Hedges gav) |
|---|---|---|---|---|---|
| Weight, kg | 85.9 ± 13.9 | 85.1 ± 13.7 | 84.8 ± 14.9 | 0.056 | 0.08 |
| BMI, kg/m2 | 30.6 ± 4.3 | 30.6 ± 4.2 | 30.4 ± 4.5 | 0.051 | 0.10 |
| Total kilocalories, kcals | 2043 ± 640 | 1816 ± 753 | 1802 ± 576 | 0.145 | 0.29 |
| Protein, g | 88 ± 36 | 77 ± 29 | 80 ± 32 | 0.329 | 0.14 |
| Fat, g | 87 ± 28 | 75 ± 32 | 75 ± 30 | 0.126 | 0.37 |
| Carbohydrates, g | 227 ± 89 | 212 ± 121 | 204 ± 85 | 0.569 | 0.15 |
| Fiber, g | 21 ± 8 | 18 ± 9 | 19 ± 7 | 0.641 | 0.09 |
| Sodium, mg | 3331 ± 1133 | 3519 ± 1353 | 2961 ± 1143 | 0.080 | 0.29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lefferts, E.C.; Saavedra, J.M.; Song, B.K.; Brellenthin, A.G.; Pescatello, L.S.; Lee, D.-c. Increasing Lifestyle Walking by 3000 Steps per Day Reduces Blood Pressure in Sedentary Older Adults with Hypertension: Results from an e-Health Pilot Study. J. Cardiovasc. Dev. Dis. 2023, 10, 317. https://doi.org/10.3390/jcdd10080317
Lefferts EC, Saavedra JM, Song BK, Brellenthin AG, Pescatello LS, Lee D-c. Increasing Lifestyle Walking by 3000 Steps per Day Reduces Blood Pressure in Sedentary Older Adults with Hypertension: Results from an e-Health Pilot Study. Journal of Cardiovascular Development and Disease. 2023; 10(8):317. https://doi.org/10.3390/jcdd10080317
Chicago/Turabian StyleLefferts, Elizabeth C., Joseph M. Saavedra, Bong Kil Song, Angelique G. Brellenthin, Linda S. Pescatello, and Duck-chul Lee. 2023. "Increasing Lifestyle Walking by 3000 Steps per Day Reduces Blood Pressure in Sedentary Older Adults with Hypertension: Results from an e-Health Pilot Study" Journal of Cardiovascular Development and Disease 10, no. 8: 317. https://doi.org/10.3390/jcdd10080317
APA StyleLefferts, E. C., Saavedra, J. M., Song, B. K., Brellenthin, A. G., Pescatello, L. S., & Lee, D.-c. (2023). Increasing Lifestyle Walking by 3000 Steps per Day Reduces Blood Pressure in Sedentary Older Adults with Hypertension: Results from an e-Health Pilot Study. Journal of Cardiovascular Development and Disease, 10(8), 317. https://doi.org/10.3390/jcdd10080317