
Cardioneuroablation Using Epicardial Pulsed Field Ablation for the Treatment of Atrial Fibrillation

 ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Pulsed Field Ablation
3. Cardiac Autonomic Nervous System
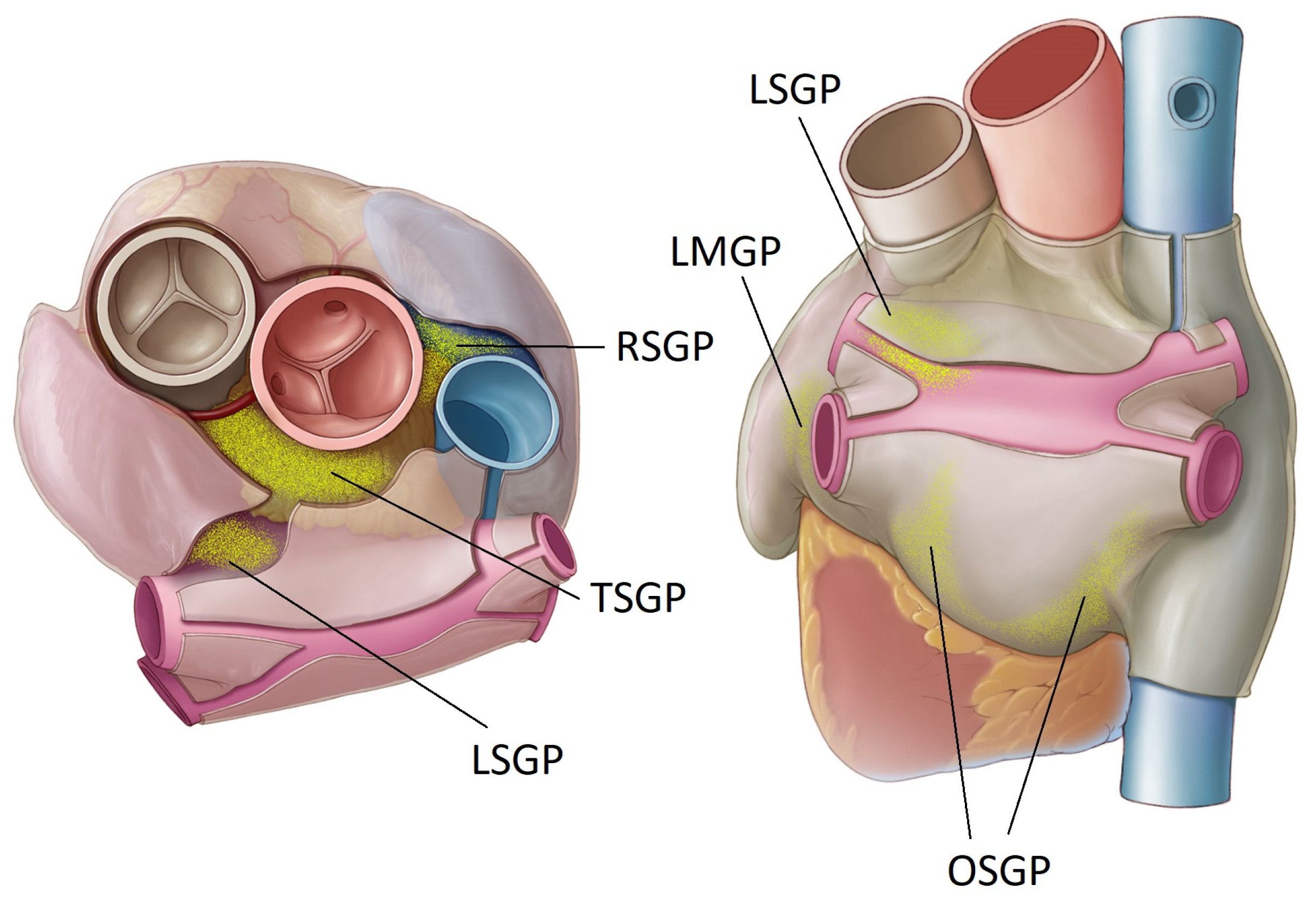
- The right superior GP (RSGP) is located on the anterosuperior surface of the right atrium, medial to the superior vena cava/right atrium junction and lateral to the aortic root. It is also sometimes known as the aortocaval (SVC-Ao) GP.
- The left superior GP (LSGP) is located at the junction of the left superior pulmonary vein with the posterior left atrium, in the left superolateral area.
- The inferior right and left GPs (IRGP, ILGP) are located at the inferior aspect of the posterior wall of the left atrium, below the right and left PVs. These are sometimes identified as the oblique sinus GP (OSGP).
- The ligament of Marshall also contains autonomic neurons and is considered a target ganglion in this context (LMGP). This is located between the anterior aspect of the left pulmonary veins and the posterior left atrial appendage. It is also known as the vein of Marshall GP (VMGP).
4. Ablation of Ganglionated Plexi—Early Studies
5. Pulsed Field Ablation of Ganglionated Plexi—Pre-Clinical Studies
6. In Vitro Cellular Studies
7. Electric Field Models
8. First-in-Human Clinical Studies
9. Discussion
10. Future Work
10.1. Access
10.2. Localization
10.3. Navigation
10.4. Further Pre-Clinial and Safety Studies
11. Future Applications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chugh, S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.; Gillum, R.; Kim, Y.-H.; McAnulty, J.; Zheng, Z.-J.; et al. Worldwide Epidemiology of Atrial Fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef]
- Kornej, J.; Borschel, C.; Benjamin, E.; Schnabel, R. Epidemiology of Atrial Fibrillation in the 21st Century: Novel Methods and New Insights. Circ. Res. 2020, 127, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Escudero-Martinez, I.; Morales-Caba, L.; Segura, T. Atrial fibrillation and stroke: A review and new insights. Trends Cardiovasc. Med. 2023, 33, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Odutayo, A.; Wong, C.; Hsiao, A.; Hopewell, S.; Altman, D.; Edmin, D. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: Systematic review and meta-analysis. BMJ 2016, 354, 14482. [Google Scholar] [CrossRef] [PubMed]
- Zimetbaum, P. Antiarrhythmic Drug Therapy for Atrial Fibrillation. Circulation 2012, 125, 381–389. [Google Scholar] [CrossRef]
- Dan, G.H.; Martinez-Rubio, A.; Agewall, S.; Boriani, G.; Borggrefe, M.; Gaita, F.; van Gelder, I.; Gorenek, B.; Kaski, J.C.; Kjeldsen, K.; et al. Antiarrhythmic drugs–clinical use and clinical decision making: A consensus document from the European Heart Rhythm Association (EHRA) and European Society of Cardiology (ESC) Working Group on Cardiovascular Pharmacology, endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS) and International Society of Cardiovascular Pharmacotherapy (ISCP). Europace 2018, 20, 731–732. [Google Scholar]
- Haissaguerre, M.; Jais, P.; Shah, D.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Metayer, P.; Clementy, J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef]
- Kuck, K.H.; Brugada, J.; Furnkranz, A.; Metzner, A.; Ouyang, F.; Chun, K.R.J.; Elvan, A.; Arentz, T.; Bestehorn, K.; Pocock, S.; et al. Cryoballoon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2016, 374, 2235–2245. [Google Scholar] [CrossRef]
- Luik, A.; Kunzmann, K.; Hormann, P.; Schmidt, K.; Radzewitz, A.; Bramlage, P.; Schenk, T.; Schymik, G.; Merkel, M.; Kieser, M.; et al. Cryoballoon vs. open irrigated radiofrequency ablation for paroxysmal atrial fibrillation: Long-term FreezeAF outcomes. BMC Cardiovasc. Disord. 2017, 17, 135. [Google Scholar] [CrossRef]
- Ullah, W.; McLean, A.; Tayebjee, M.; Gupta, D.; Ginks, M.; Haywood, G.; O’Neill, M.; Lambiase, P.; Earley, M.; Schilling, R.; et al. Randomized trial comparing pulmonary vein isolation using the SmartTouch catheter with or without real-time contact force data. Heart Rhythm 2016, 13, 1761–1767. [Google Scholar] [CrossRef]
- Knecht, S.; Sticherling, C.; Roten, L.; Badertscher, P.; Krisai, P.; Chollet, L.; Kueffer, T.; Spies, F.; Voellmin, G.; Madaffari, A.; et al. Efficacy and safety of a novel cryoballoon ablation system: Multicentre comparison of 1-year outcome. Europace 2022, 24, 1926–1932. [Google Scholar] [CrossRef]
- Fisher, J.; Brodman, R.; Kim, S.; Matos, J.; Brodman, L.; Wallerson, D.; Waspe, L. Attempted Nonsurgical Electrical Ablation of Accessory Pathways via the Coronary Sinus in the Wolf-Parkinson-White Syndrome. J. Am. Coll. Cardiol. 1984, 4, 685–694. [Google Scholar] [CrossRef]
- Morady, F.; Scheinman, M.; Kou, W.; Griffin, J.; Dick, M.; Herre, J.; Kadish, A.; Langberg, J. Long-term Results of Catheter Ablation of a Posteroseptal Accessory Atrioventricular Connection in 48 Patients. Circulation 1989, 79, 1160–1170. [Google Scholar] [CrossRef]
- Bardy, G.; Coltorti, F.; Stewart, R.; Greene, H.; Ivey, T. Catheter-Mediated Electrical Ablation: The Relationship between Current and Pulse Width on Voltage Breakdown and Shock-Wave Generation. Circ. Res. 1988, 63, 409–414. [Google Scholar] [CrossRef]
- Bertacchini, C.; Margotti, P.M.; Bergamini, E.; Lodi, A.; Ronchetti, M.; Cadossi, R. Design of an Irreversible Electroporation System for Clinical Use. Technol. Cancer Res. Treat. 2007, 6, 313–320. [Google Scholar] [CrossRef]
- Wittkampf, F.; van Driel, V.; van Wessel, H.; Vink, A.; Hof, I.; Gruendeman, P.; Hauer, R.; Loh, P. Feasibility of Electroporation for the Creation of Pulmonary Vein Ostial Lesions. J. Cardiovasc. Electrophysiol. 2011, 22, 302–309. [Google Scholar] [CrossRef]
- Wittkampf, F.; van Driel, V.; van Wessel, H.; Neven, K.; Gruendeman, P.; Vink, A.; Loh, P.; Doevendans, P. Myocardial Lesion Depth with Circular Electroporation Ablation. Circ. Arrhythm. Electrophysiol. 2012, 5, 581–586. [Google Scholar] [CrossRef]
- Neven, K.; van Driel, V.; van Wessel, H.; van Es, R.; du Pre, B.; Doevendans, P.; Wittkampf, F. Safety and Feasibility of Closed Chest Epicardial Catheter Ablation Using Electroporation. Circ. Arrhythm. Electrophysiol. 2014, 7, 913–919. [Google Scholar] [CrossRef]
- du Pre, B.; van Driel, V.; van Wessel, H.; Loh, P.; Doevendans, P.; Goldschmeding, R.; Wittkampf, F.; Vink, A. Minimal coronary artery damage by myocardial electroporation ablation. Europace 2013, 15, 144–149. [Google Scholar] [CrossRef]
- Reddy, V.; Koruth, J.; Jais, P.; Petru, J.; Timko, F.; Skalsky, I.; Hebeler, R.; Labrousse, L.; Barandon, L.; Kralovec, S.; et al. Ablation of Atrial Fibrillation with Pulsed Electric Fields. An Ultra-Rapid, Tissue-Selective Modality for Cardiac Ablation. J. Am. Coll. Cardiol. 2018, 4, 987–995. [Google Scholar]
- Di Biasi, L.; Diaz, J.C.; Zhang, X.D.; Romero, J. Pulsed field catheter ablation in atrial fibrillation. Trends Cardiovasc. Med. 2022, 32, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.; Anic, A.; Koruth, J.; Petru, J.; Funasako, M.; Minami, K.; Breskovic, T.; Sikiric, I.; Dukkipati, S.; Kawamura, I.; et al. Pulsed Field Ablation in Patients with Persistent Atrial Fibrillation. J. Am. Coll. Cardiol. 2020, 76, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Barbhaiya, C.; Kumar, S.; Guo, Y.; Zhong, J.; John, R.; Tedrow, U.; Koplan, B.; Epstein, L.; Stevenson, W.; Michaud, G. Global Survey of Esophageal Injury in Atrial Fibrillation Ablation. J. Am. Coll. Cardiol. 2016, 2, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Parikh, V.; Kowalski, M. Comparison of Phrenic Nerve Injury during Atrial Fibrillation Ablation between Different Modalities, Pathophysiology and Management. J. Atr. Fibrillation 2015, 8, 1314. [Google Scholar] [PubMed]
- Saad, E.B.; Rossillo, A.; Saad, C.P.; Martin, D.; Bhargava, M.; Erciyes, D.; Bash, D.; Williams-Andrews, M.; Beheiry, S.; Marrouche, N.; et al. Pulmonary Vein Stenosis after Radiofrequency Ablation of Atrial Fibrillation: Functional Characterization, Evolution, and Influence of the Ablation Strategy. Circulation 2003, 108, 3102–3107. [Google Scholar] [CrossRef]
- Neven, K.; van Es, R.; van Driel, V.; van Wessel, H.; Fidder, H.; Vink, A.; Doevendans, P.; Wittkampf, F. Acute and Long-Term Effects of Full-Power Electroporation Ablation Directly on the Porcine Esophagus. Circ. Arrhythm. Electrophysiol. 2017, 10, e004672. [Google Scholar] [CrossRef]
- Song, Y.; Yang, L.; He, J.; Zhao, X.; Zheng, J.; Fan, L. Ultra-microhistological study of the nonthermal irreversible electroporation on the esophagus. Heart Rhythm 2023, 20, 343–351. [Google Scholar] [CrossRef]
- van Driel, V.; Neven, K.; van Wessel, H.; Vink, A.; Doevendans, P.; Wittkampf, F. Low vulnerability of the right phrenic nerve to electroporation ablation. Heart Rhythm 2015, 12, 1838–1844. [Google Scholar] [CrossRef]
- Howard, B.; Haines, D.; Verma, A.; Kirchof, N.; Barka, N.; Onal, B.; Stewart, M.; Sigg, D. Characterization of Phrenic Nerve Response to Pulsed Field Ablation. Circ. Arrhythm. Electrophysiol. 2022, 15, e010127. [Google Scholar] [CrossRef]
- Cochet, H.; Nakatani, Y.; Sridi-Cheniti, S.; Cheniti, G.; Ramirez, D.; Nakashima, T.; Eggert, C.; Schneider, C.; Viswanathan, J.; Derval, N.; et al. Pulsed field ablation selectively spares the oesophagus during pulmonary vein isolation for atrial fibrillation. Europace 2021, 23, 1391–1399. [Google Scholar] [CrossRef]
- Pansera, F.; Bordignon, S.; Bologna, F.; Tohoku, S.; Chen, S.; Urbanek, L.; Schmidt, B.; Chun, K.R.J. Catheter ablation induced phrenic nerve palsy by pulsed field ablation–completely impossible? A case series. Eur. Heart J. Case Rep. 2022, 6, ytac361. [Google Scholar] [CrossRef]
- Witt, C.M.; Sugrue, A.; Padmanabhan, D.; Vaidya, V.; Gruba, S.; Rohl, J.; DeSimone, C.; Pederson, J.; Suddendorf, S.; Ladewig, D.J.; et al. Intrapulmonary Vein Ablation without Stenosis: A Novel Balloon-Based Direct Current Electroporation Approach. J. Am. Heart Assoc. 2018, 7, e009575. [Google Scholar] [CrossRef]
- Reddy, V.; Neuzil, P.; Koruth, J.; Petru, J.; Funosako, M.; Cochet, H.; Sediva, L.; Chovanec, M.; Dukkipati, S.; Jais, P. Pulsed Field Ablation for Pulmonary Vein Isolation in Atrial Fibrillation. J. Am. Coll. Cardiol. 2019, 74, 315–326. [Google Scholar] [CrossRef]
- Kawamura, I.; Neuzil, P.; Shrivamurthy, P.; Petru, J.; Funasako, M.; Minami, K.; Kuroki, K.; Dukkipati, S.; Koruth, J.; Reddy, V. Does pulsed field ablation regress over time? A quantitative temporal analysis of pulmonary vein isolation. Heart Rhythm 2021, 18, 878–994. [Google Scholar] [CrossRef]
- Reddy, V.; Dukkipati, S.; Neuzil, P.; Anic, A.; Petru, J.; Funasako, M.; Cochet, H.; Minami, K.; Breskovic, T.; Sikiric, I.; et al. Pulsed Field Ablation of Paroxysmal Atrial Fibrillation. 1-Year Outcomes of IMPULSE, PEFCAT, and PEFCAT II. JACC Clin. Electrophysiol. 2021, 7, 614–627. [Google Scholar] [CrossRef]
- Ekanem, E.; Reddy, V.; Schmidt, B.; Reichlin, T.; Neven, K.; Metzner, A.; Hansen, J.; Blaauw, Y.; Maury, P.; Arentz, T.; et al. Multi-national survey on the methods, efficacy, and safety on the post-approval clinical use of pulsed field ablation (MANIFEST-PF). Europace 2022, 24, 1256–1266. [Google Scholar] [CrossRef]
- Turagam, M.; Neuzil, P.; Schmidt, B.; Reichlin, B.; Neven, K.; Metzner, A.; Hansen, J.; Blaauw, Y.; Maury, P.; Arentz, T.; et al. Safety and Effectiveness of Pulsed Field Ablation to Treat Atrial Fibrillation: One-Year Outcomes from the MANIFEST-PF Registry. Circulation 2023, 147, 1. [Google Scholar] [CrossRef]
- Armour, J.A.; Iiageman, G.R.; Randalll, W.C. Arrhythmias induced by local cardiac nerve stimulation. Am. J. Physiol. 1972, 223, 1068–1075. [Google Scholar] [CrossRef]
- Armour, J.A.; Murphy, D.A.; Yuan, B.-X.; Macdonald, S.; Hopkins, D.A. Gross and Microscopic Anatomy of the Human Intrinsic Cardiac Nervous System. Anat. Rec. 1997, 247, 289–298. [Google Scholar] [CrossRef]
- Scherlag, B.; Yamanashi, W.; Patel, U.; Lazzara, R.; Jackman, W. Autonomically Induced Conversion of Pulmonary Vein Focal Firing into Atrial Fibrillation. J. Am. Coll. Cardiol. 2005, 45, 1878–1886. [Google Scholar] [CrossRef]
- Patterson, E.; Po, S.; Scherlag, B.J.; Lazzara, R. Triggered firing in pulmonary veins initiated by in vitro autonomic nerve stimulation. Heart Rhythm 2005, 2, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Po, S.; Scherlag, B.J.; Yamanashi, W.; Edwards, J.; Zhou, J.; Wu, R.; Geng, N.; Lazzara, R.; Jackman, W. Experimental model for paroxysmal atrial fibrillation arising at the pulmonary vein-atrial junctions. Heart Rhythm 2006, 3, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Scherlag, B.J.; Edwards, J.; Jackman, W.; Lazzara, R.; Po, S. Gradients of atrial refractoriness and inducibility of atrial fibrillation due to stimulation of the ganglionated plexi. J. Cardiovasc. Electrophysiol. 2007, 18, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Pappone, C.; Santinelli, V.; Manguso, F.; Vicedomini, G.; Gugliotta, F.; Augello, G.; Mazzone, P.; Tortoriello, V.; Landoni, G.; Zangrillo, A.; et al. Pulmonary Vein Denervation Enhances Long-Term Benefit after Circumferential Ablation for Paroxysmal Atrial Fibrillation. Circulation 2004, 109, 327–334. [Google Scholar] [CrossRef]
- Scherlag, B.; Nakagawa, H.; Jackman, W.; Yamanashi, W.; Patterson, E.; Po, S.; Lazzara, R. Electrical Stimulation to Identify Neural Elements on the Heart: Their Role in Atrial Fibrillation. J. Interv. Card. 2005, 13, 37–42. [Google Scholar] [CrossRef]
- Katritsis, D.G.; Pokushalov, E.; Romanov, A.; Giazitzoglou, E.; Siontis, G.; Po, S.; Camm, J.; Ioannidis, J. Autonomic Denervation Added to Pulmonary Vein Isolation for Paroxysmal Atrial Fibrillation. J. Am. Coll. Cardiol. 2013, 62, 2318–2325. [Google Scholar] [CrossRef]
- Driessen, A.; Berger, W.; Krul, S.; van den Berg, N.; Neefs, J.; Piersma, F.; Chan Pin Yin, D.; de Jong, J.; van Boven, W.J.; de Groot, J.R. Ganglion Plexus Ablation in Advanced Atrial Fibrillation. The AFACT Study. J. Am. Coll. Cardiol. 2016, 68, 1155–1165. [Google Scholar] [CrossRef]
- Kampaktis, P.; Oikonomou, E.; Choi, D.; Cheung, J. Efficacy of ganglionated plexi ablation in addition to pulmonary vein isolation for paroxysmal versus persistent atrial fibrillation: A meta-analysis of randomized clinical trials. J. Interv. Card. Electrophysiol. 2017, 50, 253–260. [Google Scholar] [CrossRef]
- Xu, F.-Q.; Yu, R.-H.; Guo, J.-J.; Bai, R.; Liu, N.; An, Y.; Guo, X.-Y.; Tang, R.-B.; Long, D.-Y.; Sang, C.-H.; et al. Catheter Ablation of Recurrent Paroxysmal Atrial Fibrillation: Is Gap-Closure Combining Ganglionated Plexi Ablation More Effective? Pacing Clin. Electrophysiol. 2017, 40, 672–682. [Google Scholar] [CrossRef]
- Pokushalov, E.; Kozlov, B.; Romanov, A.; Strelnikov, A.; Bayramova, S.; Sergeevichev, D.; Bogachev-Prokophiev, A.; Zheleznev, S.; Shipulin, V.; Lomivorotov, V.; et al. Long-Term Suppression of Atrial Fibrillation by Botulinum Toxin Injection into Epicardial Fat Pads in Patients Undergoing Cardiac Surgery–One-Year Follow-Up of a Randomized Pilot Study. Circ. Arrhythm. Electrophysiol. 2015, 8, 1334–1341. [Google Scholar] [CrossRef]
- Romanov, A.; Pokushalov, E.; Ponomarev, D.; Bayramova, S.; Shabanov, V.; Losik, D.; Stenin, I.; Elesin, D.; Mikheenko, I.; Strelnikov, A.; et al. Long-term suppression of atrial fibrillation by botulinum toxin injection into epicardial fat pads in patients undergoing cardiac surgery: Three-year follow-up of a randomized study. Heart Rhythm 2019, 16, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Lo, L.-W.; Chang, H.-Y.; Scherlag, B.; Lin, Y.-J.; Chou, Y.-H.; Lin, W.-L.; Chen, S.-A.; Po, S. Temporary Suppression of Cardiac Ganglionated Plexi Leads to Long-Term Suppression of Atrial Fibrillation: Evidence of Early Autonomic Intervention to Break the Vicious Cycle of “AF Begets AF”. J. Am. Heart Assoc. 2016, 5, e003309. [Google Scholar] [CrossRef] [PubMed]
- Dizon, J.; Chen, K.; Bacchetta, M.; Argenziano, M.; Mancini, D.; Biviano, A.; Sonett, J.; Garan, H. A Comparison of Atrial Arrhythmias after Heart or Double-Lung Transplantation at a Single Center. J. Am. Coll. Cardiol. 2009, 54, 2043–2048. [Google Scholar] [CrossRef] [PubMed]
- Noheria, A.; Patel, S.; Mirzoyev, S.; Madhavan, M.; Friedman, P.; Packer, D.; Daly, R.; Kushwaha, S.; Edwards, B.; Asirvatham, S. Decreased Postoperative Atrial Fibrillation Following Cardiac Transplantation: The Significance of Autonomic Denervation. Pacing Clin. Electrophysiol. 2013, 36, 741–747. [Google Scholar] [CrossRef]
- Madhavan, M.; Venkatachalam, K.; Swale, M.J.; DeSimone, C.; Gard, J.; Johnson, S.; Suddendorf, S.; Mikell, S.; Ladewig, D.J.; Grabinger Nobush, T.; et al. Novel Percutaneous Epicardial Autonomic Modulation in the Canine for Atrial Fibrillation: Results of an Efficacy ad Safety Study. Pacing Clin. Electrophysiol. 2016, 39, 407–417. [Google Scholar] [CrossRef]
- Padmanabhan, D.; Naksuk, N.; Killu, A.; Kapa, S.; Witt, C.; Sugrue, A.; DeSimone, C.; Madhavan, M.; de Groot, J.R.; O’Brien, B.; et al. Electroporation of epicardial autonomic ganglia: Safety and efficacy in medium-term models. J. Cardiovasc. Electrophysiol. 2019, 30, 607–615. [Google Scholar] [CrossRef]
- van Zyl, M.; Khabsa, M.; Tri, J.; Ladas, T.; Yasin, O.; Ladejobi, A.; Reilly, J.; O’Brien, B.; Coffey, K.; Asirvatham, S. Open-Chest Pulsed Electric Field Ablation of Cardiac Ganglionated Plexi in Acute Canine Models. J. Innov. Card. Rhythm Manag. 2022, 13, 5061–5069. [Google Scholar] [CrossRef]
- Kaminska, I.; Kotulska, M.; Stecka, A.; Saczko, J.; Drag-Zalesinska, M.; Wysocka, T.; Choromanska, A.; Skolucka, N.; Nowicki, R.; Marczak, J.; et al. Electroporation-induced changes in normal immature rat myoblasts (H9C2). Gen. Physiol. Biophys. 2012, 31, 19–25. [Google Scholar] [CrossRef]
- Avazzadeh, S.; O’Brien, B.; Coffey, K.; O’Halloran, M.; Keane, D.; Quinlan, L. Establishing Irreversible Electroporation Electric Field Potential Threshold in a Suspension In Vitro Model for Cardiac and Neuronal Cells. J. Clin. Med. 2021, 10, 5443. [Google Scholar] [CrossRef]
- Avazzadeh, S.; Dehkordi, M.; Owens, P.; Jalali, A.; O’Brien, B.; Coffey, K.; O’Halloran, M.; Fernhead, H.; Keane, D.; Quinlan, L. Establishing electroporation thresholds for targeted cell specific cardiac ablation in a 2D culture model. J. Cardiovasc. Electrophysiol. 2022, 33, 2050–2061. [Google Scholar] [CrossRef]
- Vizintin, A.; Vidmar, J.; Scancar, J.; Miklavcic, D. Effect of interphase and interpulse delay in high-frequency irreversible electroporation pulses on cell survival, membrane permeabilization and electrode material release. Bioelectrochemistry 2020, 134, 107523. [Google Scholar] [CrossRef]
- Gehl, J. Electroporation: Theory and methods, perspectives for drug delivery, gene therapy and research. Acta Physiol. Scand. 2003, 177, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Ivey, J.; Latouche, E.; Sano, M.; Rossmeisl, J.; Davalos, R.; Verbridge, S. Targeted cellular ablation based on the morphology of malignant cells. Sci. Rep. 2015, 5, 17157. [Google Scholar] [CrossRef]
- Li, W.; Fan, Q.; Ji, Z.; Qui, X.; Li, Z. The Effects of Irreversible Electroporation (IRE) on Nerves. PLoS ONE 2011, 6, e18831. [Google Scholar] [CrossRef]
- Martinez, C.; Hollenbeck, P. Transfection of primary CNS and PNS neurons by electroporation. Methods Cell Biol. 2003, 71, 321–332. [Google Scholar]
- González-Suárez, A.; O’Brien, B.; O’Halloran, M.; Elahi, A. Pulsed Electric Field Ablation of Epicardial Autonomic Ganglia: Computer Analysis of Monopolar Electric Field across the Tissues Involved. Bioengineering 2022, 9, 731. [Google Scholar] [CrossRef]
- González-Suárez, A.; Irastorza, R.; Deane, S.; O’Brien, B.; O’Halloran, M.; Elahi, A. Full torso and limited-domain computer models for epicardial pulsed electric field ablation. Comput. Methods Programs Biomed. 2022, 221, 106886. [Google Scholar] [CrossRef]
- Song, Y.; Zheng, J.; Fan, L. Nonthermal Irreversible Electroporation to Esophagus: Evaluation of Acute and Long-Term Pathological Effects in a Rabbit Model. J. Am. Heart Assoc. 2021, 10, e020731. [Google Scholar] [CrossRef]
- Satkauskas, S.; Batiuskaite, D.; Salomskaite-Davalgiene, S.; Venslauskas, M. Effectiveness of tumor electrochemotherapy as a function of electric pulse strength and duration. Bioelectrochemistry 2005, 65, 105–111. [Google Scholar] [CrossRef]
- González-Suárez, A.; Perez, J.; O’Brien, B.; Elahi, A. In Silico Modelling to Assess the Electrical and Thermal Disturbance Provoked by a Metal Intracoronary Stent during Epicardial Pulsed Electric Field Ablation. J. Cardiovasc. Dev. Dis. 2022, 9, 458. [Google Scholar] [CrossRef]
- De Groot, J.R.; Shaburishvili, T.; van Zyl, M.; Skalsky, I.; O’Brien, B.; Reilly, J.; Coffey, K.; Neuzil, P.; Reddy, V. Selective epicardial pulsed field ablation of ganglionated plexi causes anti-arrhythmic prolongation of refractoriness: Demonstration of feasibility in cardiac surgery patients. Europace 2022, 24 (Suppl. 1), 40458. [Google Scholar] [CrossRef]
- Po, S.; Nakagawa, H.; Jackman, W. Localization of Left Atrial Ganglionated Plexi in Patients with Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2009, 20, 1186–1189. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Scherlag, B.; Patterson, E.; Ikeda, A.; Lockwood, D.; Jackman, W. Pathophysiologic basis of autonomic ganglionated plexus ablation in patients with atrial fibrillation. Heart Rhythm 2009, 6, s26–s34. [Google Scholar] [CrossRef] [PubMed]
- Garabelli, P.; Stavrakis, S.; Kenney, J.; Po, S. Effect of 28-mm Cryoballoon Ablation on Major Atrial Ganglionated Plexi. J. Am. Coll. Cardiol. 2018, 4, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Okumura, Y.; Watanabe, I.; Nagashima, K.; Watanabe, R.; Arai, M.; Iso, K.; Kurokawa, S.; Okubo, K.; Nakai, T.; et al. Effect of Cryoballoon Ablation vs Radiofrequency Ablation on Left Atrial Ganglionated Plexi in Patients with Atrial Fibrillation. J. Nihon Univ. Med. Ass. 2018, 77, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Qin, M.; Jiang, W.-F.; Wu, S.-H.; Zhang, X.-D.; Po, S. Vagal response during pulmonary vein isolation: RE-recognizing its characteristics and implications in lone paroxysmal atrial fibrillation. Int. J. Cardiol. 2016, 211, 7–13. [Google Scholar] [CrossRef]
- Kurotobi, T.; Shimida, Y.; Kino, N.; Ito, K.; Tonomura, D.; Yano, K.; Tanaka, C.; Yoshida, M.; Tsuchida, T.; Fukumoto, H. Features of intrinsic ganglionated plexi in both atria after extensive pulmonary isolation and their clinical significance after catheter ablation in patients with atrial fibrillation. Heart Rhythm 2015, 12, 470–476. [Google Scholar] [CrossRef]
- Musikantow, D.; Neuzil, P.; Petru, P.; Koruth, J.; Kralovec, S.; Miller, M.; Funasako, M.; Chovanec, M.; Turugam, M.; Whang, W.; et al. Pulsed Field Ablation to Treat Atrial Fibrillation: Autonomic Nervous System Effects. JACC Clin. Electrophysiol. 2023, 9, 481–493. [Google Scholar] [CrossRef]
- Stojadinovic, P.; Wichterle, D.; Peichl, P.; Nakagawa, H.; Cihak, R.; Haskova, J.; Kautzner, J. Autonomic Changes Are More Durable after Radiofrequency than Pulsed Electric Field Pulmonary Vein Isolation. J. Am. Coll. Cardiol. 2022, 8, 895–904. [Google Scholar]
- Tang, L.; Hawkins, N.; Ho, K.; Tam, R.; Deyell, M.; Macle, L.; Verma, A.; Khairy, P.; Sheldon, R.; Andrade, J.; et al. Autonomic Alterations after Pulmonary Vein Isolation in the CIRCA-DOSE (Cryoballoon vs Irrigated Radiofrequency Catheter Ablation) Study. J. Am. Heart Assoc. 2021, 10, e018610. [Google Scholar] [CrossRef]
- Krisai, P.; Knecht, S.; Badertscher, P.; Muehl, A.; Osswald, S.; Roten, L.; Reichlin, T.; Sticherling, C.; Kuehne, M. Troponin release after pulmonary vein isolation using pulsed field ablation compared to radiofrequency and cryoballoon ablation. Heart Rhythm 2022, 19, 1471–1472. [Google Scholar] [CrossRef]
- Lemoine, M.; Mencke, C.; Nies, M.; Obergassel, J.; Scherschel, K.; Wieboldt, H.; Schleberger, R.; My, I.; Rottner, L.; Moser, J.; et al. Pulmonary Vein Isolation by Pulsed-Field Ablation Induces Less Neurocardiac Damage Than Cryoballoon Ablation. Circ. Arrhythm. Electrophysiol. 2023, 16, e011598. [Google Scholar] [CrossRef]
- Rehorn, M.; Daubert, J. Pulsed field catheter ablation in atrial fibrillation: The promising future of an old technology. Trends Cardiovasc. Med. 2022, 32, 388–389. [Google Scholar] [CrossRef]
- De Asmundis, C.; Chierchia, G.-B. Pulsed field ablation: Have we finally found the holy grail? Europace 2021, 23, 1691–1692. [Google Scholar] [CrossRef]
- Guo, F.; Wang, J.; Deng, Q.; Feng, H.; Xie, M.; Zhou, Z.; Zhou, L.; Wang, Y.; Li, X.; Xu, S.; et al. Effects of pulsed field ablation on autonomic nervous system in paroxysmal atrial fibrillation: A pilot study. Heart Rhythm 2023, 20, 329–338. [Google Scholar] [CrossRef]
- Kim, M.-Y.; Coyle, C.; Tomlinson, D.; Sikkel, M.; Sohaib, A.; Luther, V.; Leong, K.; Malcolme-Lawes, L.; Low, B.; Sandler, B.; et al. Ectopy-triggering ganglionated plexuses ablation to prevent atrial fibrillation: GANGLIA-AF study. Heart Rhythm 2022, 19, 516–524. [Google Scholar] [CrossRef]
- Kim, M.-Y.; Lim, P.; Coyle, C.; Sandler, B.; Koa-Wing, M.; Kanagaratnam, P. Single Ectopy-Triggering Ganglionated Plexus Ablation without Pulmonary Vein Isolation Prevents Atrial Fibrillation. JACC Case Rep. 2020, 2, 2004–2009. [Google Scholar] [CrossRef]
- Futyma, P.; Zarebski, L.; Wrzos, A.; Futyma, M.; Kulakowski, P. Right anterior ganglionated plexus ablation for the treatment of vagally-mediated atrial fibrillation. Europace 2022, 24 (Suppl. 1), i151. [Google Scholar] [CrossRef]
- Karatela, M.; Fudim, M.; Matthew, J.; Piccini, J. Neuromodulation therapy for atrial fibrillation. Heart Rhythm 2023, 20, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Pachon, J.; Pachon, E.; Pachon, J.C.; Lobo, T.; Pachon, M.Z.; Vargas, R.; Jatene, A. “Cardioneuroablation”–new treatment for neurocardiogenic syncope, functional AV block and sinus dysfunction using catheter RF-ablation. Europace 2005, 7, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.; Marquez, M.; Fierro, E.; Baez, J.; Rockbrand, L.; Gomez-Flores, J. Cardioinhibitory syncope: From pathophysiology to treatment–should we think on cardioneuroablation? J. Interv. Card. Electrophysiol. 2020, 59, 441–461. [Google Scholar] [CrossRef]
- Gopinathannair, R.; Olshansky, B.; Turugam, M.; Gautam, S.; Futyma, P.; Akella, K.; Tanboga, H.; Bozyel, S.; Yalin, K.; Padmanabhan, D.; et al. Permanent pacing versus cardioneuroablation for cardioinhibitory vasovagal syncope. J. Interv. Card. Electrophysiol. 2023. [Google Scholar] [CrossRef]
- Qin, M.; Zhang, Y.; Liu, X.; Jiang, W.-F.; Wu, S.-H.; Po, S. Atrial Ganglionated Plexus Modification–A Novel Approach to Treat Symptomatic Sinus Bradycardia. J. Am. Coll. Cardiol. 2017, 3, 950–959. [Google Scholar]
- Thurber, C.; Sneider, D.; Sauer, W.; Kapur, S. Recurrent vasovagal syncope following successful cardioneuroablation. Heart Rhythm Case Rep. 2023, 8, 465–468. [Google Scholar] [CrossRef]
- Mao, J.; Yin, X.; Zhang, Y.; Yan, Q.; Dong, J.; Ma, C.; Liu, X. Ablation of Epicardial Ganglionated Plexi Increases Atrial Vulnerability to Arrhythmias in Dogs. Circ. Arrhythm. Electrophysiol. 2014, 7, 711–817. [Google Scholar] [CrossRef]
- Sakamoto, S.; Schuessler, R.; Lee, A.; Aziz, A.; Lall, S.; Damiano, R. Vagal denervation and reinnervation after ablation of ganglionated plexi. J. Thorac. Cardiovasc. Surg. 2010, 139, 444–452. [Google Scholar] [CrossRef]
- Park, J.; Hong, S.; Wi, J.; Lee, D.; Joung, B.; Lee, M.; Pak, H.-N. Catheter Ablation of Atrial Fibrillation Raises the Plasma Level of NGF-β Which Is Associated with Sympathetic Nerve Activity. Yonsei Med. J. 2015, 56, 1530–1537. [Google Scholar] [CrossRef]
- Kangavari, S.; Oh, Y.-S.; Zhou, S.; Youn, H.-J.; Lee, M.-Y.; Jung, W.-S.; Rho, T.-H.; Hong, S.-J.; Kar, S.; Kerwin, W.; et al. Radiofrequency catheter ablation and nerve growth factor concentration in humans. Heart Rhythm 2006, 3, 1150–1155. [Google Scholar] [CrossRef]
- Benali, K.; Barre, B.; Hermida, A.; Galand, V.; Milhem, A.; Philibert, S.; Boveda, S.; Bars, C.; Anselme, F.; Maille, B.; et al. Recurrences of Atrial Fibrillation Despite Durable Pulmonary Vein Isolation: The PARTY-PVI Study. Circ. Arrhythm. Electrophysiol. 2023, 16, e011354. [Google Scholar] [CrossRef]
- Nagai, M.; Dote, K.; Forster, C.Y. Denervation or stimulation? Role of sympatho-vagal imbalance in HFpEF with hypertension. Hypertens. Res. 2023. [Google Scholar] [CrossRef]
- Jungen, C.; Scherschel, K.; Eickholt, C.; Kuklik, P.; Klatt, N.; Bork, N.; Salzbrunn, T.; Alken, F.; Angendohr, S.; Klene, C.; et al. Disruption of cardiac cholinergic neurons enhances susceptibility to ventricular arrhythmias. Nat. Commun. 2017, 8, 14155. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Lu, Z.; He, W.; Wu, L.; Cui, B.; Hu, X.; Yu, L.; Huang, C.; Jiang, H. Effects of ganglionated plexi ablation on ventricular electrophysiological properties in normal hearts and after acute myocardial ischemia. Int. J. Cardiol. 2013, 168, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Osman, F.; Kundu, S.; Tuan, J.; Jeilan, M.; Stafford, P.; Ng, A. Ganglionated Plexus Ablation during Pulmonary Vein Isolation–Predisposing to Ventricular Arrhythmias? Indian Pacing Electrophysiol. J. 2010, 10, 104–107. [Google Scholar] [PubMed]
- Chakraborty, P.; Po, S. The role of autonomic denervation in the success of atrial fibrillation ablation: Can Pulsed-Field Ablation provide the answer? Heart Rhythm 2023, 20, 341–342. [Google Scholar] [CrossRef]
- Romero, J.; Shivkumar, K.; Di Biasi, L.; Avendano, R.; Anderson, R.; Natale, A.; Kumar, S. Mastering the art of epicardial access in cardiac electrophysiology. Heart Rhythm 2019, 16, 1738–1749. [Google Scholar] [CrossRef]
- Aryana, A.; d’Avila, A. Epicardial Catheter Ablation of Ventricular Tachycardia. Card. Electrophysiol. Clin. 2017, 9, 119–131. [Google Scholar] [CrossRef]
- Keramati, A.; DeMazumder, D.; Misra, S.; Chrispin, J.; Assis, F.; Raghuram, C.; Dey, S.; Calkins, H.; Tandri, H. Anterior pericardial access to facilitate electrophysiology study and catheter ablation of ventricular arrhythmias: A single tertiary center experience. J. Cardiovasc. Electrophysiol. 2017, 28, 1189–1195. [Google Scholar] [CrossRef]
- Massumi, A.; Chelu, M.; Nazeri, A.; May, S.; Afshar-Kharaghan, H.; Saeed, M.; Razavi, M.; Rasekh, A. Initial Experience with a Novel Percutaneous Left Atrial Appendage Exclusion Device in Patients with Atrial Fibrillation, Increased Stroke Risk, and Contraindications to Anticoagulation. J. Am. Coll. Cardiol. 2013, 111, 869–873. [Google Scholar] [CrossRef]
- Di Biase, L.; Burkhardt, J.D.; Reddy, V.; Romero, J.; Neuzil, P.; Petru, J.; Sadiva, L.; Skoda, J.; Ventura, M.; Carbucicchio, C.; et al. Initial international multicenter human experience with a novel epicardial access needle embedded with a real-time pressure/frequency monitoring to facilitate epicardial access: Feasibility and safety. Heart Rhythm 2017, 14, 981–988. [Google Scholar] [CrossRef]
- Opfermann, J.; Contento, J.; Mass, P.; Krieger, A.; Berul, C.; Kumthekar, R. A novel videoscope and tool kit for percutaneous pericardial access under direct visualization. BioMed. Eng. Online 2023, 22, 19. [Google Scholar] [CrossRef]
- Julia, J.; Bokhari, F.; Uuetoa, H.; Derejko, P.; Traykov, V.; Gwizdala, A.; Sebag, F.; Hegbom, F.; Anfinsen, O.-G.; Al Quibbany, A.; et al. A New Era in Epicardial Access for the Ablation of Ventricular Arrhythmias–The Epi-CO2 Registry. J. Am. Coll. Cardiol. 2021, 7, 85–96. [Google Scholar]
- Ahmed, A.; Garg, J.; Kabra, R.; Charate, R.; Eliaz, R.; Demma, J.; Menshes, Z.; Hazan, O.; Lakkireddy, D. Feasibility and safety of a novel blunt tip concealed needle device for pericardial access in porcine models. J. Interv. Card. Electrophysiol. 2022. [Google Scholar] [CrossRef]
- Derejko, P.; Dzwonkowska, D.; Wrobel, K.; Kusnierz, J.; Bardyszewski, A.; Menshes, Z.; Hazan, O.; Leon, A.; Luria, D.; Lakkireddy, D. Safety and Efficacy of a Novel Blunt-Tip Concealed-Needle Epicardial Access Device: First-in-Human Feasibility Study. JACC Clin. Electrophysiol. 2022, 8, 908–912. [Google Scholar] [CrossRef]
- Gunda, S.; Reddy, M.; Pillarisetti, J.; Atoui, M.; Badhwar, N.; Swarup, V.; Di Biase, L.; Mohanty, S.; Mohanty, P.; Nagaraj, H.; et al. Differences in complication rates between large bore needle and a long micropuncture needle during epicardial access: Time to change clinical practice? Circ. Arrhythm. Electrophysiol. 2015, 8, 890–895. [Google Scholar] [CrossRef]
- Pokushalov, E.; Romanov, A.; Shugayev, P.; Artyomenko, S.; Shirokova, N.; Turov, A.; Katritsis, D. Selective ganglionated plexi ablation for paroxysmal atrial fibrillation. Heart Rhythm 2009, 6, 1257–1264. [Google Scholar] [CrossRef]
- Aksu, T.; Guler, T.; Mutluer, F.; Bozyel, S.; Golcuk, S.; Yalin, K. Electroanatomic-mapping-guided cardioneuroablation versus combined approach for vasovagal syncope. J. Interv. Card. Electrophysiol. 2019, 54, 177–188. [Google Scholar] [CrossRef]
- John, L.; Mullis, A.; Payne, J.; Tung, R.; Aksu, T.; Winterfield, J. Fractionated Mapping of the Ganglionated Plexi for Cardioneuroablation. J. Innov. Cardiac. Rhythm Manag. 2021, 12, 4473–4476. [Google Scholar] [CrossRef]
- Aksu, T.; De Potter, T.; John, L.; Osorio, J.; Singh, D.; Alyesh, D.; Baysal, E.; Kumar, K.; Mikaeili, J.; Dal Forno, A.; et al. Procedural and short-term results of electroanatomic-mapping-guided ganglionated plexus ablation by first-time operators: A multicenter study. J. Cardiovasc. Electrophysiol. 2021, 33, 117–122. [Google Scholar] [CrossRef]
- Aksu, T.; Guler, T.; Bozyel, S.; Yalin, K. Usage of a new mapping algorithm to detect possible critical substrate for continuity of atrial fibrillation: Fractionation mapping in preliminary experience. J. Interv. Card. Electrophysiol. 2020, 58, 29–34. [Google Scholar] [CrossRef]
- Aksu, T.; Skeete, J.; Huang, H. Ganglionic Plexus Ablation: A Step-by-step Guide for Electrophysiologists and Review of Modalities for Neuromodulation for the Management of Atrial Fibrillation. Arrhythmia Electrophysiol. Rev. 2023, 12, e02. [Google Scholar] [CrossRef]
- Shi, R.; Chen, Z.; Kontogeorgis, A.; Sacher, F.; Della Bella, P.; Bisceglia, C.; Martin, R.; Meyer, C.; Willems, S.; Markides, V.; et al. Epicardial Ventricular Tachycardia Ablation Guided by a Novel High-Resolution Contact Mapping System: A Multicenter Study. J. Am. Heart Assoc. 2018, 7, e010549. [Google Scholar] [CrossRef]
- Stirrup, J.; Gregg, S.; Baavour, R.; Roth, N.; Breault, C.; Agostini, D.; Ernst, S.; Underwood, S. Hybrid solid-state SPECT/CT left atrial innervation imaging for identification of left atrial ganglionated plexi: Technique and validation in patients with atrial fibrillation. J. Nuc. Cardiol. 2020, 27, 1939–1950. [Google Scholar] [CrossRef] [PubMed]
- Buszman, P.; Lukasik, K.; Deane, S.; Mazur, M.; Konopko, M.; Fernandez, C.; Glanc, M.; Kazmierczak, P.; O’Brien, B.; Reilly, J.; et al. TCT-245 Safety and Feasibility of Epicardial Access and Maneuverability with a Novel Ablation Catheter for the Treatment of Atrial Fibrillation in a Porcine Model. J. Am. Coll. Cardiol. 2021, 78, 19. [Google Scholar] [CrossRef]
- Reddy, V.; Petru, J.; Funasako, M.; Kopriva, K.; Hala, P.; Chovanec, M.; Janotka, M.; Kralovec, S.; Neuzil, P. Coronary Arterial Spasm during Pulsed Field Ablation to Treat Atrial Fibrillation. Circulation 2022, 146, 1808–1819. [Google Scholar] [CrossRef] [PubMed]
- Hachisuka, M.; Fujimoto, Y.; Oka, E.; Hayashi, H.; Yamamoto, T.; Murata, H.; Yodogawa, K.; Iwasaki, Y.-K.; Hayashi, M.; Miyauchi, Y.; et al. Perioperative coronary artery spasms in patients undergoing catheter ablation of atrial fibrillation. J. Interv. Card. Electrophysiol. 2022, 64, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Yajima, K.; Yamase, Y.; Oishi, H.; Ikehara, N.; Asai, Y. Coronary Artery Spasm during Cryoballoon Ablation in a Patient with Atrial Fibrillation. Intern. Med. 2018, 57, 819–822. [Google Scholar] [CrossRef]
- Gaudino, M.; Di Franco, A.; Rong, L.; Picicini, J.; Mack, M. Postoperative atrial fibrillation from mechanisms to treatment. Eur. Heart J. 2023, 44, 1020–1039. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Brien, B.; Reilly, J.; Coffey, K.; González-Suárez, A.; Quinlan, L.; van Zyl, M. Cardioneuroablation Using Epicardial Pulsed Field Ablation for the Treatment of Atrial Fibrillation. J. Cardiovasc. Dev. Dis. 2023, 10, 238. https://doi.org/10.3390/jcdd10060238
O’Brien B, Reilly J, Coffey K, González-Suárez A, Quinlan L, van Zyl M. Cardioneuroablation Using Epicardial Pulsed Field Ablation for the Treatment of Atrial Fibrillation. Journal of Cardiovascular Development and Disease. 2023; 10(6):238. https://doi.org/10.3390/jcdd10060238
Chicago/Turabian StyleO’Brien, Barry, John Reilly, Ken Coffey, Ana González-Suárez, Leo Quinlan, and Martin van Zyl. 2023. "Cardioneuroablation Using Epicardial Pulsed Field Ablation for the Treatment of Atrial Fibrillation" Journal of Cardiovascular Development and Disease 10, no. 6: 238. https://doi.org/10.3390/jcdd10060238
APA StyleO’Brien, B., Reilly, J., Coffey, K., González-Suárez, A., Quinlan, L., & van Zyl, M. (2023). Cardioneuroablation Using Epicardial Pulsed Field Ablation for the Treatment of Atrial Fibrillation. Journal of Cardiovascular Development and Disease, 10(6), 238. https://doi.org/10.3390/jcdd10060238