
Semi-Quantification of Myocardial Uptake of Bone-Seeking Agents in Suspected Cardiac Amyloidosis

 , , , , ,
, , , , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
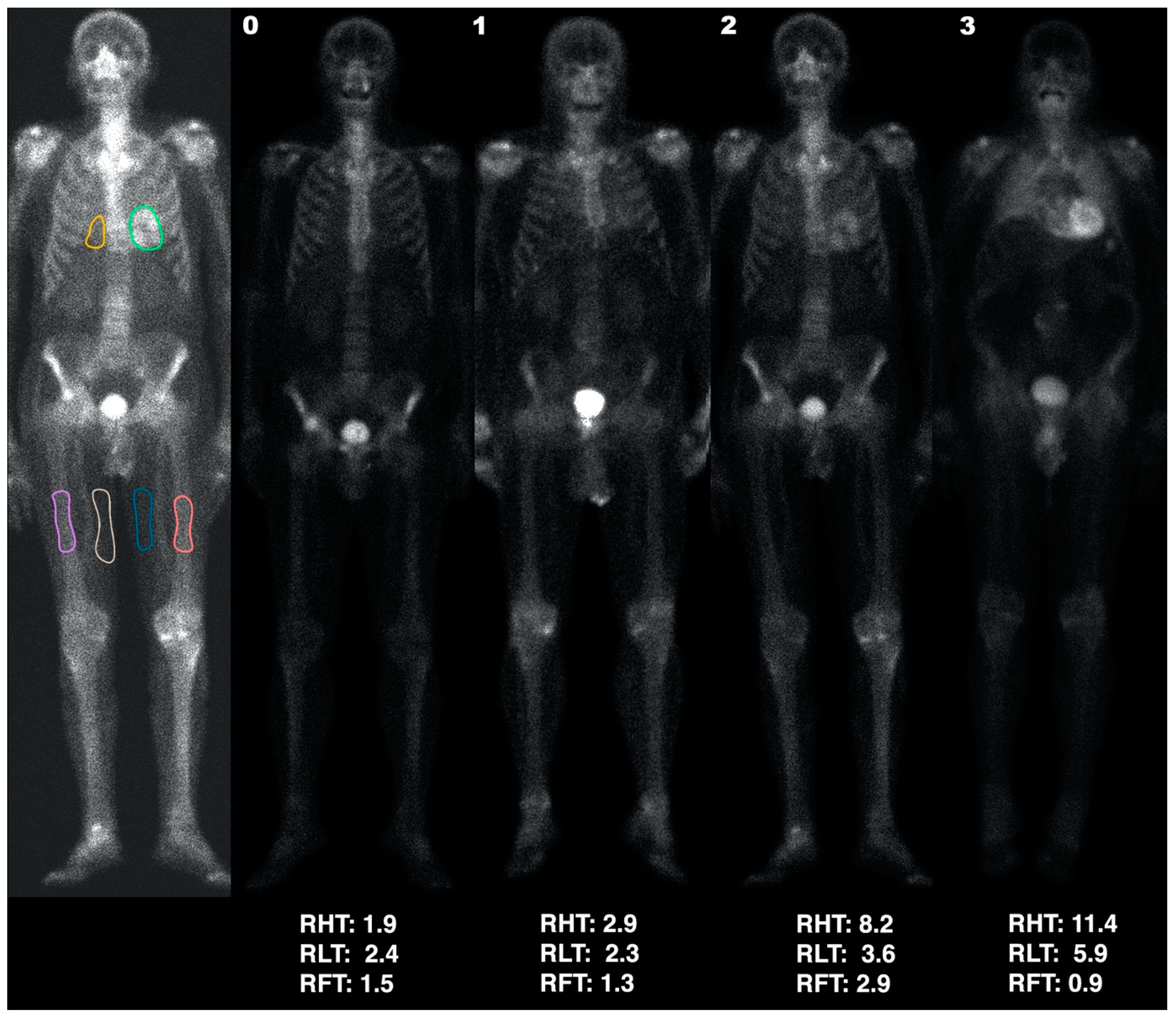
- score 0, no cardiac uptake and normal bone uptake
- score 1, mild cardiac uptake that is less than bone uptake
- score 2, moderate cardiac uptake accompanied by attenuated bone uptake
- score 3, strong cardiac uptake with mild/absent bone uptake
- Heart uptake: regions of interest (ROIs) were manually drawn on the anterior view as accurately as possible around the heart uptake, excluding ribs and sternum, and on the medial portion of the soft tissues (therefore mainly corresponding to adipose tissue) of both the mid-thighs (Figure 1), excluding vessel uptake. The heart-to-thigh ratio (RHT) was then computed as (heart average counts—mid-thigh average counts)/mid-thigh average counts.
- Pulmonary uptake: since most patients with bone tracer cardiac uptake also showed a particularly increased pulmonary uptake, the lungs were also semi-quantitatively assessed. A ROI in the right lung, including part of the mediastinum and excluding ribs (at least in the anterior view) and sternum, was drawn as accurately as possible. The semi-quantitative lung to thigh ratio (RLT) was then computed as (pulmonary average counts—mid-thigh average counts)/mid-thigh average counts.
- Bone uptake: since patients with intense cardiac uptake often showed an apparent reduction in bone uptake, we also defined ROIs on both femoral diaphyses (Figure 1) of each patient with cardiac uptake. The semi-quantitative femur-to-thigh ratio (RFT) was then computed as (femoral average counts—mid-thigh average counts)/mid-thigh average counts.
Statistical Analysis
3. Results
3.1. Analysis
3.1.1. HC Analysis
3.1.2. Overall Analysis
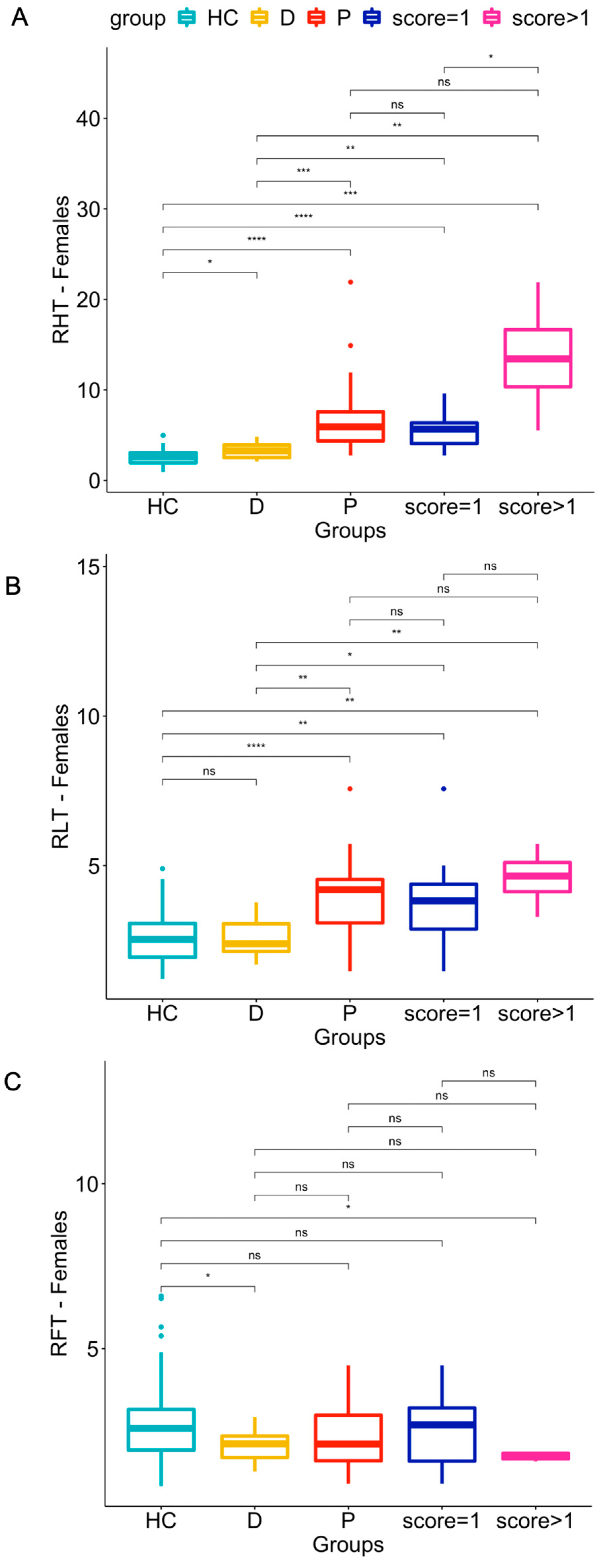
- Regarding the Female Group:
- RHT and RLT were significantly higher in patients than in HCs (p-values ≤ 0.0001) (see panel A and B of Figure 2). Both indices also differed significantly in patients with qualitative scores of 1 or >1 versus HCs (p ranging from ≤0.01 to ≤0.0001, with the lower levels of significance for RLT compared to RHT).
- Only two statistically significant (p ≤ 0.05) differences in RFT were found: between HC and doubtful patients, and between HC and patients with scores > 1 (see Figure 2, panel C).
- Doubtful patients differed significantly (p ≤ 0.05) from HCs in the RHT and RFT indices but not in RLT.
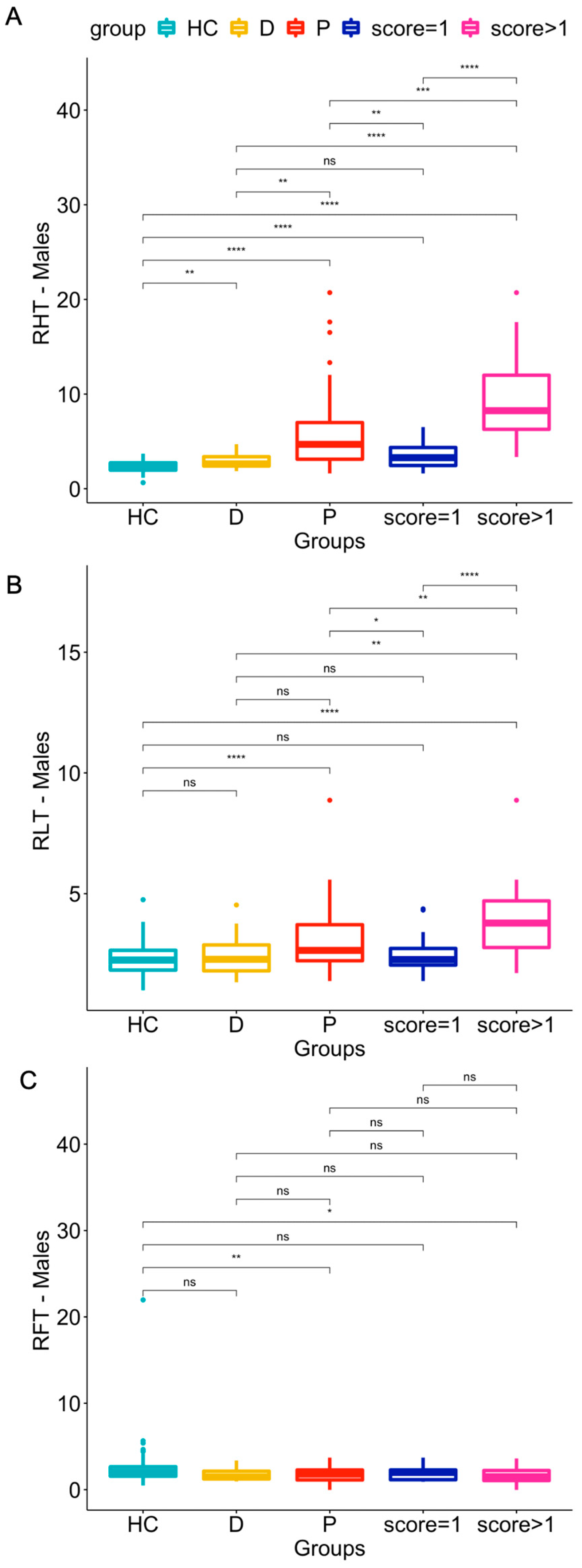
- Regarding the male group:
- The RHT and RLT indices in patients were significantly higher than in HCs (p-values ≤ 0.0001) (see panel A and B of Figure 3). RHT was also significantly higher in patients with qualitative scores of 1 or >1 (p ≤ 0.0001) than in HCs.
- Only two statistically significant differences in RFT were found: between HCs and patients (visual scores from 1 to 3; p ≤ 0.01), and between HCs and patients with scores > 1 (p ≤ 0.05) (see Figure 3, panel C).
- Doubtful patients differed significantly (p ≤ 0.05) from HCs in the RHT index but not in RLT or RFT.
3.1.3. Cut-offs by ROC Curves
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gertz, M.A. Therapy of Transthyretin Cardiomyopathy. J. Am. Coll. Cardiol. 2019, 74, 296–298. [Google Scholar] [CrossRef]
- Maleszewski, J.J. Cardiac amyloidosis: Pathology, nomenclature, and typing. Cardiovasc. Pathol. 2015, 24, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Huang, X.; Li, J. Light chain amyloidosis: Where are the light chains from and how they play their pathogenic role? Blood Rev. 2017, 31, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Naharro, A.; Hawkins, P.N.; Fontana, M. Cardiac amyloidosis. Clin. Med. 2018, 18, s30–s35. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef] [PubMed]
- Ardehali, H.; Qasim, A.; Cappola, T.; Howard, D.; Hruban, R.; Hare, J.M.; Baughman, K.L.; Kasper, E.K. Endomyocardial biopsy plays a role in diagnosing patients with unexplained cardiomyopathy. Am. Heart J. 2004, 147, 919–923. [Google Scholar] [CrossRef]
- Gertz, M.A.; Grogan, M.; Kyle, R.A.; Tajik, A. Endomyocardial biopsy-proven light chain amyloidosis (AL) without echocardiographic features of infiltrative cardiomyopathy. Am. J. Cardiol. 1997, 80, 93–95. [Google Scholar] [CrossRef]
- Damy, T.; Jaccard, A.; Guellich, A.; Lavergne, D.; Galat, A.; Deux, J.-F.; Hittinger, L.; Dupuis, J.; Frenkel, V.; Rigaud, C.; et al. Identification of prognostic markers in transthyretin and AL cardiac amyloidosis. Amyloid 2016, 23, 194–202. [Google Scholar] [CrossRef]
- Bellavia, D.; Pellikka, P.A.; Dispenzieri, A.; Scott, C.G.; Al-Zahrani, G.B.; Grogan, M.; Pitrolo, F.; Oh, J.K.; Miller, F.A., Jr. Comparison of right ventricular longitudinal strain imaging, tricuspid annular plane systolic excursion, and cardiac biomarkers for early diagnosis of cardiac involvement and risk stratification in primary systematic (AL) amyloidosis: A 5-year cohort stud. Eur. Heart J.—Cardiovasc. Imaging 2012, 13, 680–689. [Google Scholar] [CrossRef]
- Boldrini, M.; Cappelli, F.; Chacko, L.; Restrepo-Cordoba, M.A.; Lopez-Sainz, A.; Giannoni, A.; Aimo, A.; Baggiano, A.; Martinez-Naharro, A.; Whelan, C.; et al. Multiparametric Echocardiography Scores for the Diagnosis of Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2020, 13, 909–920. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Treibel, T.A.; Abdel-Gadir, A.; Bulluck, H.; Zumbo, G.; Knight, D.S.; Kotecha, T.; Francis, R.; Hutt, D.F.; Rezk, T.; et al. Magnetic Resonance in Transthyretin Cardiac Amyloidosis. J. Am. Coll. Cardiol. 2017, 70, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M.; Chung, R.; Hawkins, P.N.; Moon, J.C. Cardiovascular magnetic resonance for amyloidosis. Heart Fail. Rev. 2014, 20, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Law, W.P.; Wang, W.Y.; Moore, P.T.; Mollee, P.N.; Ng, A.C. Cardiac Amyloid Imaging with 18F-Florbetaben PET: A Pilot Study. J. Nucl. Med. 2016, 57, 1733–1739. [Google Scholar] [CrossRef]
- Möckelind, S.; Axelsson, J.; Pilebro, B.; Lindqvist, P.; Suhr, O.B.; Sundström, T. Quantification of cardiac amyloid with [18F]Flutemetamol in patients with V30M hereditary transthyretin amyloidosis. Amyloid 2020, 27, 191–199. [Google Scholar] [CrossRef]
- Perugini, E.; Guidalotti, P.L.; Salvi, F.; Cooke, R.M.; Pettinato, C.; Riva, L.; Leone, O.; Farsad, M.; Ciliberti, P.; Bacchi-Reggiani, L.; et al. Noninvasive etiologic diagnosis of cardiac amyloidosis using 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy. J. Am. Coll. Cardiol. 2005, 46, 1076–1084. [Google Scholar] [CrossRef]
- Rapezzi, C.; Quarta, C.C.; Guidalotti, P.L.; Longhi, S.; Pettinato, C.; Leone, O.; Ferlini, A.; Salvi, F.; Gallo, P.; Gagliardi, C.; et al. Usefulness and limitations of 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy in the aetiological diagnosis of amyloidotic cardiomyopathy. Eur. J. Nucl. Med. 2010, 38, 470–478. [Google Scholar] [CrossRef]
- Chen, W.; Dilsizian, V. Molecular imaging of amyloidosis: Will the heart be the next target after the brain? Curr. Cardiol. Rep. 2012, 14, 226–233. [Google Scholar] [CrossRef]
- Salvalaggio, A.; Cipriani, A.; Righetto, S.; Artioli, P.; Sinigiani, G.; De Michieli, L.; Cason, M.; Pilichou, K.; Cecchin, D.; Briani, C. Incidental cardiac uptake of 99mTc-diphosphonates is predictive of poor outcome: Data from 9616 bone scintigraphies. J. Nucl. Cardiol. 2022, 29, 3419–3425. [Google Scholar] [CrossRef] [PubMed]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, F.; Gallini, C.; Di Mario, C.; Costanzo, E.N.; Vaggelli, L.; Tutino, F.; Ciaccio, A.; Bartolini, S.; Angelotti, P.; Frusconi, S.; et al. Accuracy of 99mTc-Hydroxymethylene diphosphonate scintigraphy for diagnosis of transthyretin cardiac amyloidosis. J. Nucl. Cardiol. 2019, 26, 497–504. [Google Scholar] [CrossRef]
- Gillmore, J.D.; Maurer, M.S.; Falk, R.H.; Merlini, G.; Damy, T.; Dispenzieri, A.; Wechalekar, A.D.; Berk, J.L.; Quarta, C.C.; Grogan, M.; et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation 2016, 133, 2404–2412. [Google Scholar] [CrossRef] [PubMed]
- Abulizi, M.; Cottereau, A.S.; Guellich, A.; Vandeventer, S.; Galat, A.; Van Der Gucht, A.; Plante-Bordeneuve, V.; Dubois-Randé, J.L.; Bodez, D.; Rosso, J.; et al. Early-phase myocardial uptake intensity of 99mTc-HMDP vs. 99mTc-DPD in patients with hereditary transthyretin-related cardiac amyloidosis. J. Nucl. Cardiol. 2018, 25, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, M.B.; Cappelli, F.; Russo, D.; Tini, G.; Canepa, M.; Milandri, A.; Bonfiglioli, R.; Di Bella, G.; My, F.; Luigetti, M.; et al. Low Sensitivity of Bone Scintigraphy in Detecting Phe64Leu Mutation-Related Transthyretin Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2019, 13, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Hutt, D.F.; Quigley, A.-M.; Page, J.; Hall, M.L.; Burniston, M.; Gopaul, D.; Lane, T.; Whelan, C.J.; Lachmann, H.; Gillmore, J.D.; et al. Utility and limitations of 3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy in systemic amyloidosis. Eur. Heart J.—Cardiovasc. Imaging 2014, 15, 1289–1298. [Google Scholar] [CrossRef]
- Umaid Rauf, M.; Hawkins, P.N.; Cappelli, F.; Perfetto, F.; Zampieri, M.; Argiro, A.; Petrie, A.; Law, S.; Porcari, A.; Razvi, Y.; et al. Tc-99m labelled bone scintigraphy in suspected cardiac amyloidosis. Eur. Heart J. 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Aimo, A.; Merlo, M.; Porcari, A.; Georgiopoulos, G.; Pagura, L.; Vergaro, G.; Sinagra, G.; Emdin, M.; Rapezzi, C. Redefining the epidemiology of cardiac amyloidosis. A systematic review and meta-analysis of screening studies. Eur. J. Heart Fail. 2022, 24, 2342–2351. [Google Scholar] [CrossRef]
- Oerlemans, M.I.F.J.; Rutten, K.H.G.; Minnema, M.C.; Raymakers, R.A.P.; Asselbergs, F.W.; de Jonge, N. Cardiac amyloidosis: The need for early diagnosis. Neth. Heart J. 2019, 27, 525–536. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| HC | D | P Score = 1 | P Score = 2 | P Score = 3 | P-Total | |
|---|---|---|---|---|---|---|
| FEMALES: | ||||||
| Number | 89 | 11 | 12 | 3 | 1 | 16 |
| Age (years) | 73 ± 6 | 71 ± 8 | 78 ± 7 | 81 ± 5 | 83 | 79 ± 6 |
| Age range (years) | 65–90 | 49–79 | 66–88 | 77–86 | 83 | 66–88 |
| RHT | 2.52 ± 0.75 | 3.30 ± 0.93 | 5.39 ± 1.92 | 10.79 ± 4.79 | 21.91 | 7.43 ± 5.03 |
| RLT | 2.58 ± 0.85 | 2.62 ± 0.71 | 3.83 ± 1.56 | 4.20 ± 0.83 | 5.73 | 4.02 ± 1.45 |
| RFT | 2.74 ± 1.17 | 2.13 ± 0.61 | 2.60 ± 1.12 | 1.70 ± 0.11 | 1.88 | 2.39 ± 1.03 |
| MALES: | ||||||
| Number | 183 | 16 | 31 | 15 | 6 | 52 |
| Age (years) | 68 ± 9 | 68 ± 11 | 78 ± 8 | 80 ± 6 | 82 ± 5 | 79 ± 7 |
| Age range (years) | 50–86 | 50–86 | 62–100 | 69–86 | 72–89 | 62–100 |
| RHT | 2.28 ± 0.57 | 2.80 ± 0.83 | 3.55 ± 1.39 | 8.39 ± 3.55 | 12.34 ± 6.14 | 5.96 ± 4.25 |
| RLT | 2.26 ± 0.60 | 2.35 ± 0.92 | 2.44 ± 0.68 | 3.53 ± 0.94 | 4.92 ± 2.20 | 3.04 ± 1.33 |
| RFT | 2.31 ± 1.77 | 1.72 ± 0.70 | 1.87 ± 0.73 | 1.91 ± 1.02 | 1.35 ± 1.12 | 1.82 ± 0.84 |
| Females (n = 105) | ||||
|---|---|---|---|---|
| HC (n = 89), P (n = 16) | ||||
| Sensitivity (95% CI) | Specificity (95% CI) | Cut-Off | AUC (95% CI) | |
| RHT | 0.94 (0.81; 1.00) | 0.87 (0.79; 0.93) | ≥3.260 | 0.96 (0.90; 1.00) |
| RLT | 0.88 (0.69; 1.00) | 0.66 (0.57; 0.76) | ≥2.825 | 0.81 (0.68; 0.95) |
| RFT | 0.50 (0.25; 0.75) | 0.76 (0.67; 0.76) | <1.890 | 0.59 (0.43; 0.76) |
| Males (n = 235) | ||||
|---|---|---|---|---|
| HC (n = 183), P (n = 52) | ||||
| Sensitivity (95% CI) | Specificity (95% CI) | Cut-Off | AUC (95% CI) | |
| RHT | 0.81 (0.69; 0.90) | 0.88 (0.83; 0.93) | >2.965 | 0.87 (0.80; 0.94) |
| RLT | 0.33 (0.19; 0.46) | 0.95 (0.92; 0.98) | >3.290 | 0.67 (0.59; 0.76) |
| RFT | 0.38 (0.25; 0.52) | 0.86 (0.81; 0.91) | <1.305 | 0.62 (0.53; 0.71) |
| Doubtful | Females (n = 11) |
|---|---|
| Cut-Off | |
| RHT | n = 6 (54.54%) ≥ 3.260 |
| RLT | n = 2 (18.18%) ≥ 2.825 |
| RFT | n = 2 (18.18%) < 1.890 |
| Doubtful | Males (n = 16) |
|---|---|
| Cut-Off | |
| RHT | n = 5 (31.25%) > 2.965 |
| RLT | n = 2 (12.5%) > 3.290 |
| RFT | n = 6 (37.5%) < 1.305 |
| Males (n = 235) | ||||
|---|---|---|---|---|
| HC + Score = 1 (n = 214) vs. Score >1 (n = 21) | ||||
| Sensitivity (95% CI) | Specificity (95% CI) | Cut-Off | AUC (95% CI) | |
| RHT | 0.95 (0.86; 1.00) | 0.97 (0.95; 0.99) | ≥4.69 | 0.99 (0.98; 1.00) |
| RLT | 0.66 (0.47; 0.86) | 0.94 (0.91; 0.97) | ≥3.29 | 0.86 (0.76; 0.96) |
| RFT | 0.57 (0.38; 0.76) | 0.75 (0.69; 0.81) | <1.515 | 0.63 (0.48; 0.78) |
| Doubtful | Males (n = 16) |
|---|---|
| Cut-Off | |
| RHT | n = 1 (6.25%) ≥ 4.69 |
| RLT | n = 2 (12.5%) ≥ 3.29 |
| RFT | n = 9 (56.25%) < 1.515 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campi, C.; Briani, C.; Salvalaggio, A.; Giraudo, C.; Cipriani, A.; Zorzi, A.; Zucchetta, P.; Vettor, R.; Cecchin, D. Semi-Quantification of Myocardial Uptake of Bone-Seeking Agents in Suspected Cardiac Amyloidosis. J. Cardiovasc. Dev. Dis. 2023, 10, 184. https://doi.org/10.3390/jcdd10050184
Campi C, Briani C, Salvalaggio A, Giraudo C, Cipriani A, Zorzi A, Zucchetta P, Vettor R, Cecchin D. Semi-Quantification of Myocardial Uptake of Bone-Seeking Agents in Suspected Cardiac Amyloidosis. Journal of Cardiovascular Development and Disease. 2023; 10(5):184. https://doi.org/10.3390/jcdd10050184
Chicago/Turabian StyleCampi, Cristina, Chiara Briani, Alessandro Salvalaggio, Chiara Giraudo, Alberto Cipriani, Alessandro Zorzi, Pietro Zucchetta, Roberto Vettor, and Diego Cecchin. 2023. "Semi-Quantification of Myocardial Uptake of Bone-Seeking Agents in Suspected Cardiac Amyloidosis" Journal of Cardiovascular Development and Disease 10, no. 5: 184. https://doi.org/10.3390/jcdd10050184
APA StyleCampi, C., Briani, C., Salvalaggio, A., Giraudo, C., Cipriani, A., Zorzi, A., Zucchetta, P., Vettor, R., & Cecchin, D. (2023). Semi-Quantification of Myocardial Uptake of Bone-Seeking Agents in Suspected Cardiac Amyloidosis. Journal of Cardiovascular Development and Disease, 10(5), 184. https://doi.org/10.3390/jcdd10050184