
Smoothness Evaluation Indices during Sit-to-Stand-to-Sit Motions in Healthy Older Females and after Hip Fracture Using an Accelerometer: A Pilot Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Ethical Procedures
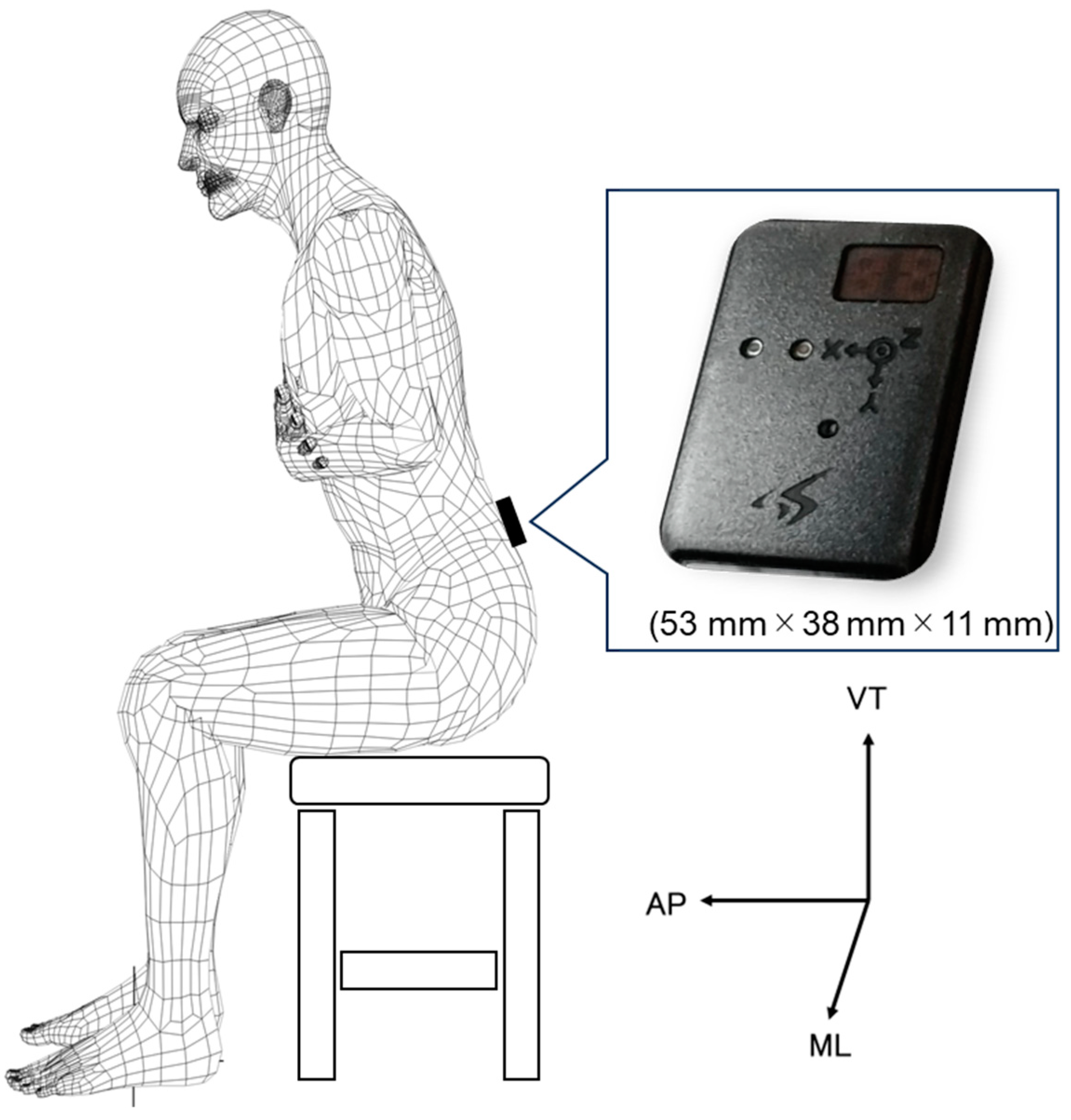
2.4. Measurements
2.5. Data Processing
2.5.1. Five Sit-to-Stand Test
2.5.2. Harmonic Ratio
2.5.3. Power Spectrum Entropy
2.6. Statistical Analyses
3. Results
3.1. Characterization of the Sample and Comparison of the Two Study Subgroups
3.2. Five Sit-to-Stand Test Compared with Maximum Gait Speed
3.3. Harmonic Ratio Comparison
3.4. Power Spectrum Entropy Comparison
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Treacy, D.; Hassett, L.; Schurr, K.; Fairhall, N.J.; Cameron, I.D.; Sherrington, C. Mobility training for increasing mobility and functioning in older people with frailty. Cochrane Database Syst. Rev. 2022, 2022, CD010494. [Google Scholar] [CrossRef]
- Dapp, U.; Vinyard, D.; Golgert, S.; Krumpoch, S.; Freiberger, E. Reference values of gait characteristics in community-dwelling older persons with different physical functional levels. BMC Geriatr. 2022, 22, 713. [Google Scholar] [CrossRef] [PubMed]
- Kobsar, D.; Charlton, J.M.; Tse, C.T.F.; Esculier, J.-F.; Graffos, A.; Krowchuk, N.M.; Thatcher, D.; Hunt, M.A. Validity and reliability of wearable inertial sensors in healthy adult walking: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2020, 17, 62. [Google Scholar] [CrossRef] [PubMed]
- Doi, T.; Hirata, S.; Ono, R.; Tsutsumimoto, K.; Misu, S.; Ando, H. The harmonic ratio of trunk acceleration predicts falling among older people: Results of a 1-year prospective study. J. Neuroeng. Rehabil. 2013, 10, 7. [Google Scholar] [CrossRef]
- Iosa, M.; Bini, F.; Marinozzi, F.; Fusco, A.; Morone, G.; Koch, G.; Cinnera, A.M.; Bonnì, S.; Paolucci, S. Stability and Harmony of Gait in Patients with Subacute Stroke. J. Med. Biol. Eng. 2016, 36, 635–643. [Google Scholar] [CrossRef]
- Bellanca, J.; Lowry, K.; VanSwearingen, J.; Brach, J.; Redfern, M. Harmonic ratios: A quantification of step to step symmetry. J. Biomech. 2013, 46, 828–831. [Google Scholar] [CrossRef]
- Kojima, M.; Obuchi, S.; Henmi, O.; Ikeda, N. Comparison of Smoothness during Gait between Community Dwelling Elderly Fallers and Non-Fallers Using Power Spectrum Entropy of Acceleration Time-Series. J. Phys. Ther. Sci. 2008, 20, 243–248. [Google Scholar] [CrossRef]
- Kojima, M.; Obuchi, S.; Mizuno, K.; Henmi, O.; Ikeda, N. Power spectrum entropy of acceleration time-series during movement as an indicator of smoothness of movement. J. Physiol. Anthropol. 2008, 27, 193–200. [Google Scholar] [CrossRef]
- Kojima, M.; Obuchi, S. Evaluating the usefulness of power spectrum entropy of acceleration time-series in setting the load for high-intensity strength training for the frail elderly. Rigakuryoho Kagaku. 2012, 27, 291–296. (In Japanese) [Google Scholar] [CrossRef][Green Version]
- Brach, J.S.; McGurl, D.; Wert, D.; VanSwearingen, J.M.; Perera, S.; Cham, R.; Studenski, S. Validation of a measure of smoothness of walking. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 136–141. [Google Scholar] [CrossRef]
- Wang, D.X.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachex Sarcopenia Muscle 2019, 11, 3–25. [Google Scholar] [CrossRef] [PubMed]
- Alcazar, J.; Kamper, R.S.; Aagaard, P.; Haddock, B.; Prescott, E.; Ara, I.; Suetta, C. Relation between leg extension power and 30-s sit-to-stand muscle power in older adults: Validation and translation to functional performance. Sci. Rep. 2020, 10, 16337. [Google Scholar] [CrossRef] [PubMed]
- Baltasar-Fernandez, I.; Alcazar, J.; Mañas, A.; Alegre, L.M.; Alfaro-Acha, A.; Rodriguez-Mañas, L.; Ara, I.; García-García, F.J.; Losa-Reyna, J. Relative sit-to-stand power cut-off points and their association with negatives outcomes in older adults. Sci. Rep. 2021, 11, 19460. [Google Scholar] [CrossRef] [PubMed]
- Bagalà, F.; Klenk, J.; Cappello, A.; Chiari, L.; Becker, C.; Lindemann, U. Quantitative Description of the Lie-to-Sit-to-Stand-to-Walk Transfer by a Single Body-Fixed Sensor. IEEE Trans. Neural. Syst. Rehabil. Eng. 2013, 21, 624–633. [Google Scholar] [CrossRef]
- Zablotny, C.; Hilton, T.; Riek, L.; Kneiss, J.; Tome, J.; Houck, J. Validity of Visual Assessment of Sit to Stand After Hip Fracture. J. Geriatr. Phys. Ther. 2020, 43, 12–19. [Google Scholar] [CrossRef]
- Marques, D.L.; Neiva, H.P.; Pires, I.M.; Marinho, D.A.; Marques, M.C. Accelerometer data from the performance of Sit-to-Stand test by elderly people. Data Brief 2020, 33, 106328. [Google Scholar] [CrossRef]
- Kampe, K.; Pfeiffer, K.; Lindemann, U.; Schoene, D.; Taraldsen, K.; Rapp, K.; Becker, C.; Klenk, J. Change of physical activity parameters of hip and pelvic fracture patients during inpatient rehabilitation and after discharge: Analysis of global and in-depth parameters. Eur. Rev. Aging Phys. Act 2021, 18, 9. [Google Scholar] [CrossRef]
- Jarchi, D.; Pope, J.; Lee, T.K.M.; Tamjidi, L.; Mirzaei, A.; Sanei, S. A Review on Accelerometry-Based Gait Analysis and Emerging Clinical Applications. IEEE Rev. Biomed. Eng. 2018, 11, 177–194. [Google Scholar] [CrossRef]
- Moe-Nilssen, R. Test-retest reliability of trunk accelerometry during standing and walking. Arch. Phys. Med. Rehabil. 1998, 79, 1377–1385. [Google Scholar] [CrossRef]
- Aylar, M.F.; Dionisio, V.C.; Jafarnezhadgero, A. Do the center of mass strategies change with restricted vision during the sit-to-stand task? Clin. Biomech. 2019, 62, 104–112. [Google Scholar] [CrossRef]
- Orakifar, N.; Shaterzadeh-Yazdi, M.J.; Salehi, R.; Mehravar, M.; Namnik, N. Muscle Activity Pattern Dysfunction During Sit to Stand and Stand to Sit in the Movement System Impairment Subgroups of Low Back Pain. Arch. Phys. Med. Rehabil. 2019, 100, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Orange, S.T.; Metcalfe, J.W.; Liefeith, A.; Jordan, A.R. Validity of various portable devices to measure sit-to-stand velocity and power in older adults. Gait Posture 2020, 76, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Shimamura, T.; Katoh, H. Validation of smoothness evaluation during standing and sitting motions using an accelerometer. J. Phys. Ther. Sci. 2021, 33, 246–249. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait Posture 2003, 18, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Bubela, D.J.; Magasi, S.R.; Wang, Y.-C.; Gershon, R.C. Sit-to-stand test: Performance and determinants across the age-span. Isokinet. Exerc. Sci. 2010, 18, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Baltasar-Fernandez, I.; Alcazar, J.; Losa-Reyna, J.; Soto-Paniagua, H.; Alegre, L.M.; Takai, Y.; Ruiz-Cárdenas, J.D.; Signorile, J.F.; Rodriguez-Mañas, L.; García-García, F.J.; et al. Comparison of available equations to estimate sit-to-stand muscle power and their association with gait speed and frailty in older people: Practical applications for the 5-rep sit-to-stand test. Exp. Gerontol. 2021, 156, 111619. [Google Scholar] [CrossRef]
- Narazaki, K.; Matsuo, E.; Honda, T.; Nofuji, Y.; Yonemoto, K.; Kumagai, S. Physical Fitness Measures as Potential Markers of Low Cognitive Function in Japanese Community-Dwelling Older Adults without Apparent Cognitive Problems. J. Sports Sci. Med. 2014, 13, 590–596. [Google Scholar]
- Tainaka, K.; Aoki, J. Fitness-related factors associated with changes in walking speed in elderly women. Jpn. J. Phys. Fit. Sports Med. 2002, 51, 245–251. (in Japanese). [Google Scholar] [CrossRef]
- Pai, Y.C.; Rogers, M.W. Control of body mass transfer as a function of speed of ascent in sit-to-stand. Med. Sci. Sports Exerc. 1990, 22, 378–384. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Healthy Group (n = 18) | Hip Fracture Group (n = 18) | p-Value |
|---|---|---|---|
| Height (cm) | 154.1 ± 4.8 | 150.7 ± 5.5 | 0.055 |
| Age (years) | 63.1 ± 3.2 | 76.2 ± 7.8 | <0.001 |
| Weight (kg) | 52.6 ± 9.0 | 45.3 ± 5.7 | 0.006 |
| BMI (kg/m2) | 22.1 ± 3.1 | 20.0 ± 2.4 | 0.029 |
| MMSE (points) | 27.3 ± 2.3 | ||
| Type of hip fracture | |||
| Trochanteric fracture after OLIF | 7 (39%) | ||
| Subtrochanteric fracture after OLIF | 2 (11%) | ||
| Neck fracture | 9 (50%) | ||
| Type of surgery | |||
| OLIF | 3 (33%) | ||
| BHA | 3 (33%) | ||
| THA | 3 (33%) | ||
| Laterality | |||
| Right | 7 (39%) | ||
| Left | 11 (61%) | ||
| Gait aid | |||
| None | 18 (100%) | 9 (50%) | |
| Cane | 0 (0%) | 9 (50%) | |
| Date of measurement (days after surgery) | 46.7 ± 10.7 | ||
| Seat height (cm) | 38.4 ± 0.8 | 38.9 ± 1.1 | 0.10 |
| Healthy Group | Hip Fracture Group | p-Value † | Effect Size, d | p-Value ‡ | |
|---|---|---|---|---|---|
| 5STS (s) | 8.75 ± 1.05 | 12.17 ± 3.20 | <0.001 | 1.43 | 0.754 |
| MGS (m/s) | 1.93 ± 0.21 | 1.09 ± 0.27 | <0.001 | 3.51 | 0.012 |
| HR | ||||
|---|---|---|---|---|
| Healthy Group | Hip Fracture Group | p-Value | Effect Size, d | |
| STSF | ||||
| ML | 1.88 ± 0.72 | 1.56 ± 0.26 | 0.092 | 0.59 |
| VT | 3.65 ± 1.74 | 2.67 ± 1.01 | 0.047 | 0.69 |
| AP | 3.26 ± 1.33 | 2.76 ± 0.88 | 0.443 | 0.44 |
| Triaxial | 2.53 ± 1.13 | 2.04 ± 0.63 | 0.406 | 0.53 |
| STS2s | ||||
| ML | 2.18 ± 0.89 | 1.75 ± 0.74 | 0.125 | 0.52 |
| VT | 3.42 ± 1.54 | 2.58 ± 0.83 | 0.049 | 0.69 |
| AP | 2.68 ± 0.67 | 2.34 ± 0.72 | 0.150 | 0.49 |
| Triaxial | 2.69 ± 1.19 | 2.18 ± 0.73 | 0.131 | 0.52 |
| PSE | ||||
|---|---|---|---|---|
| Healthy Group | Hip Fracture Group | p-Value | Effect Size, d | |
| STSF | ||||
| ML | 6.01 ± 0.22 | 5.94 ± 0.16 | 0.297 | 0.35 |
| VT | 5.78 ± 0.24 | 5.68 ± 0.16 | 0.148 | 0.49 |
| AP | 5.78 ± 0.16 | 5.61 ± 0.16 | 0.002 | 1.10 |
| Triaxial | 5.85 ± 0.21 | 5.68 ± 0.18 | 0.015 | 0.85 |
| STS2s | ||||
| ML | 7.63 ± 0.31 | 7.82 ± 0.16 | 0.035 | 0.74 |
| VT | 7.46 ± 0.22 | 7.63 ± 0.16 | 0.010 | 0.88 |
| AP | 7.47 ± 0.15 | 7.61 ± 0.17 | 0.014 | 0.86 |
| Triaxial | 7.45 ± 0.25 | 7.66 ± 0.17 | 0.003 | 0.97 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimamura, T.; Ishikawa, H.; Fujii, H.; Katoh, H. Smoothness Evaluation Indices during Sit-to-Stand-to-Sit Motions in Healthy Older Females and after Hip Fracture Using an Accelerometer: A Pilot Study. Geriatrics 2023, 8, 98. https://doi.org/10.3390/geriatrics8050098
Shimamura T, Ishikawa H, Fujii H, Katoh H. Smoothness Evaluation Indices during Sit-to-Stand-to-Sit Motions in Healthy Older Females and after Hip Fracture Using an Accelerometer: A Pilot Study. Geriatrics. 2023; 8(5):98. https://doi.org/10.3390/geriatrics8050098
Chicago/Turabian StyleShimamura, Takeshi, Hitoshi Ishikawa, Hiromi Fujii, and Hiroshi Katoh. 2023. "Smoothness Evaluation Indices during Sit-to-Stand-to-Sit Motions in Healthy Older Females and after Hip Fracture Using an Accelerometer: A Pilot Study" Geriatrics 8, no. 5: 98. https://doi.org/10.3390/geriatrics8050098
APA StyleShimamura, T., Ishikawa, H., Fujii, H., & Katoh, H. (2023). Smoothness Evaluation Indices during Sit-to-Stand-to-Sit Motions in Healthy Older Females and after Hip Fracture Using an Accelerometer: A Pilot Study. Geriatrics, 8(5), 98. https://doi.org/10.3390/geriatrics8050098