
Metallosis after Hip Arthroplasty Damages Skeletal Muscle: A Case Report

 , ,
, , 
Abstract
1. Introduction
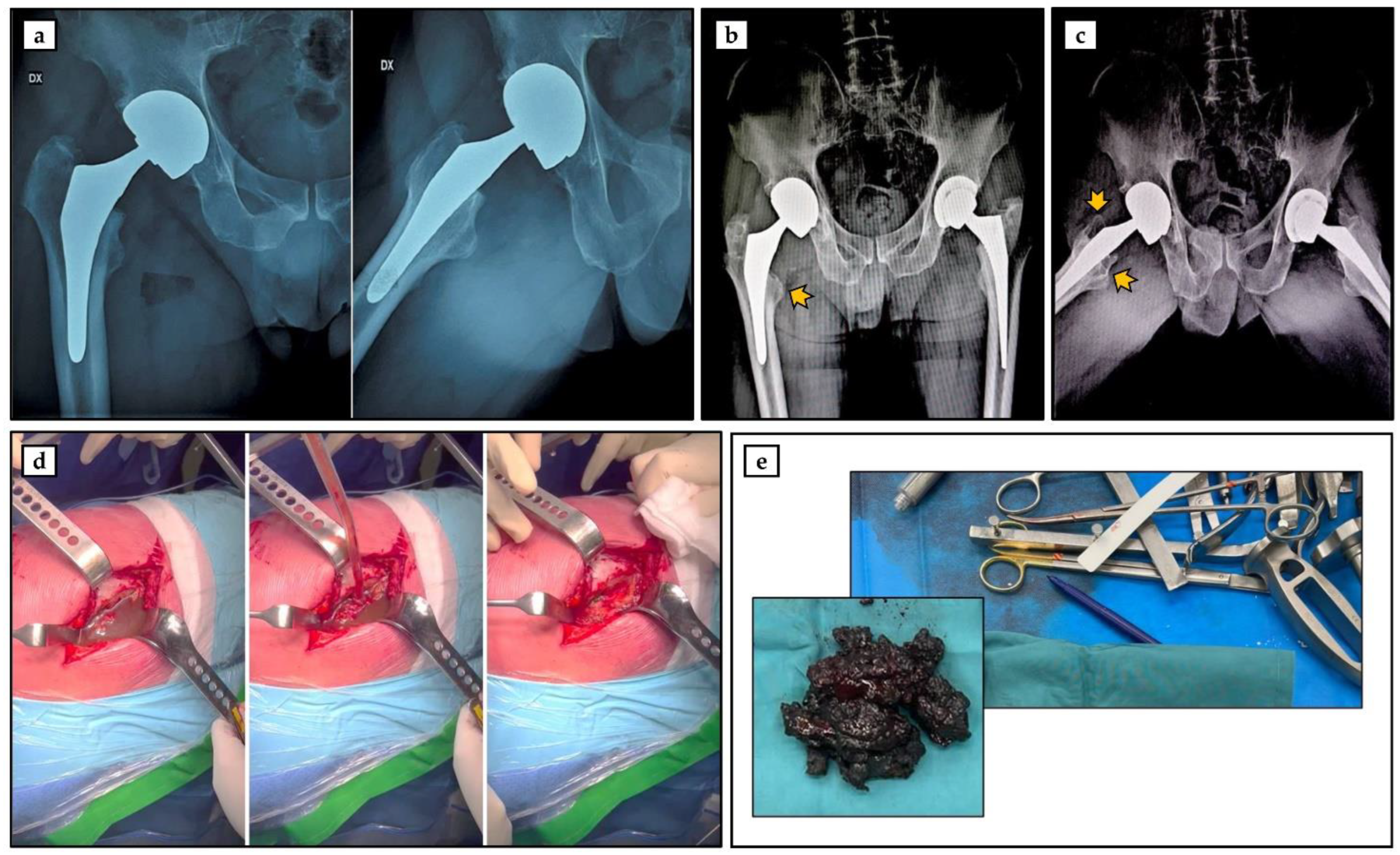
2. Case Report Description
3. Materials and Methods
3.1. Participants
3.2. Histological and Morphometric Analysis
3.3. Immunohistochemistry
3.4. Statistical Analysis
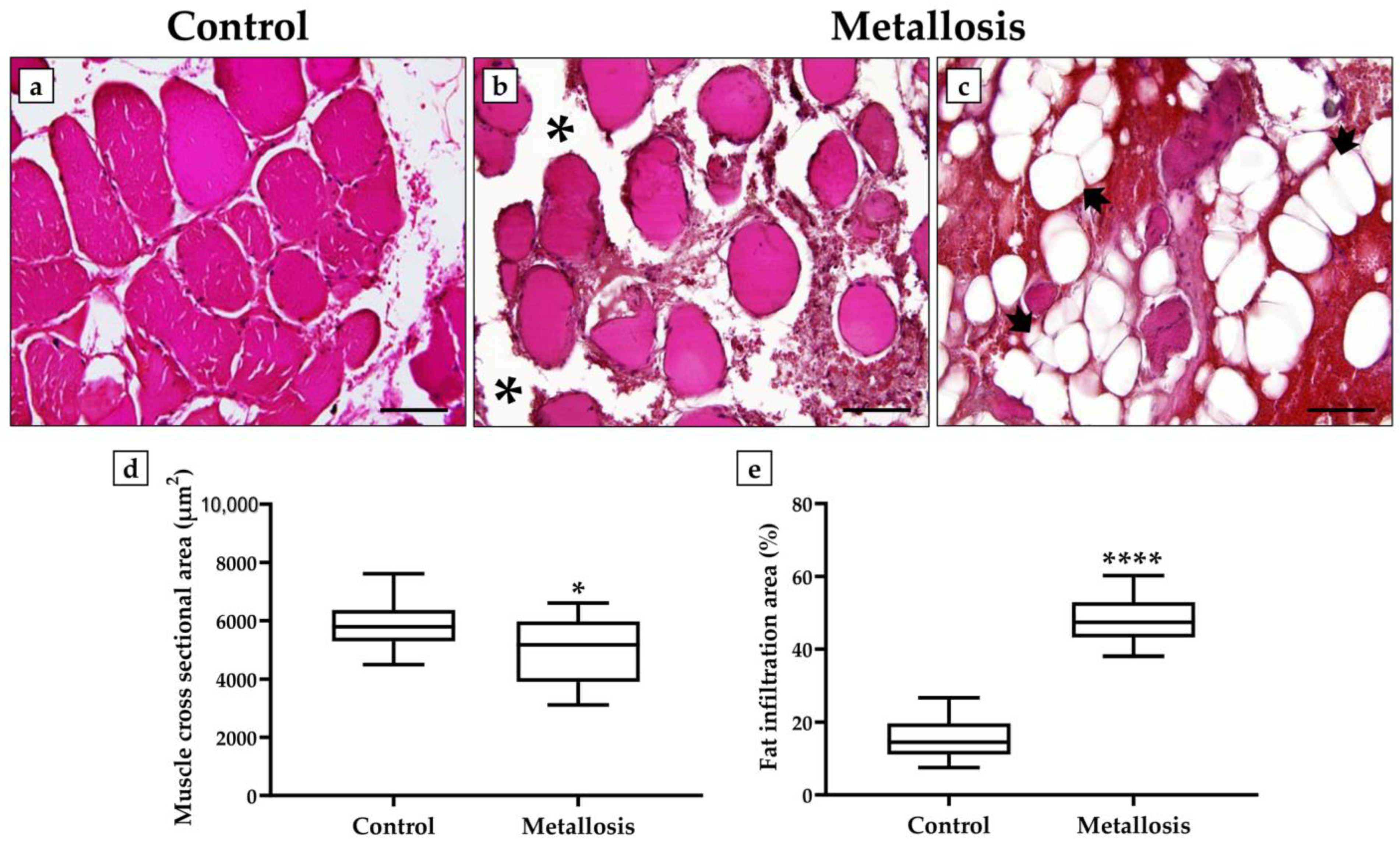
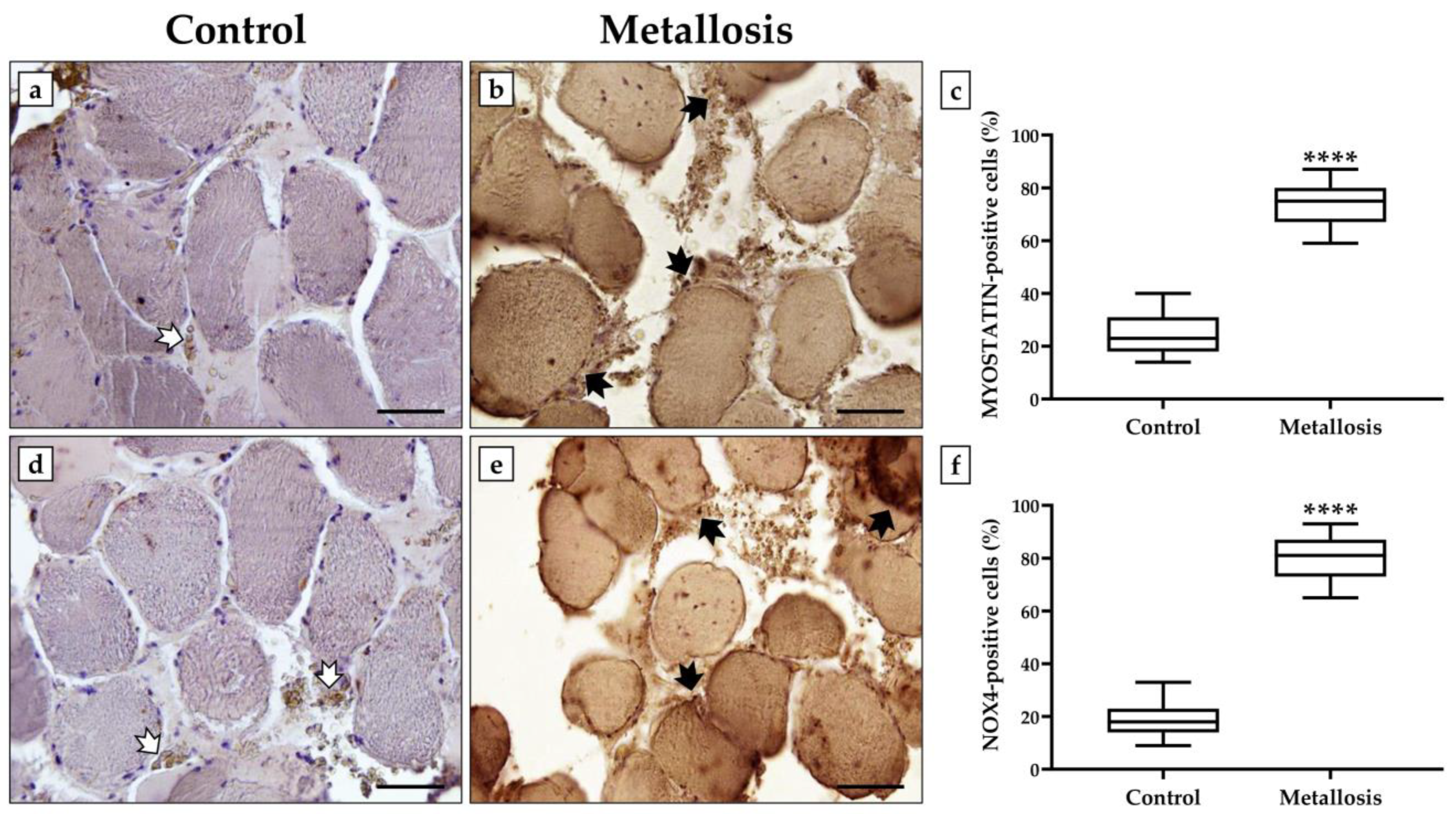
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Banjabi, A.A.; Kurunthachalam, K.; Kumosani, T.A.; Abulnaja, K.O.; Al-Malki, A.L.; Moselhy, S.S. Serum heavy metals of passive smoker females and its correlation to bone biomarkers and risk of osteoporosis. Environ. Sci. Pollut. Res. Int. 2022, 29, 6943–6948. [Google Scholar] [CrossRef]
- Ximenez, J.P.B.; Zamarioli, A.; Kacena, M.A.; Barbosa, R.M.; Barbosa, F.J. Association of Urinary and Blood Concentrations of Heavy Metals with Measures of Bone Mineral Density Loss: A Data Mining Approach with the Results from the National Health and Nutrition Examination Survey. Biol. Trace Elem. Res. 2021, 199, 92–101. [Google Scholar] [CrossRef]
- Scimeca, M.; Feola, M.; Romano, L.; Rao, C.; Gasbarra, E.; Bonanno, E.; Brandi, M.L.; Tarantino, U. Heavy metals accumulation affects bone microarchitecture in osteoporotic patients. Environ. Toxicol. 2017, 32, 1333–1342. [Google Scholar] [CrossRef]
- He, H.; Lin, X.; Tong, T.; Xu, Y.; Hong, H.; Zhang, J.; Xu, Y.; Huang, C.; Zhou, Z. Cadmium exposure impairs skeletal muscle function by altering lipid signature and inducing inflammation in C57BL/6J mice. Ecotoxicol. Environ. Saf. 2023, 258, 114986. [Google Scholar] [CrossRef]
- Rony, L.; Lancigu, R.; Hubert, L. Intraosseous metal implants in orthopedics: A review. Morphologie 2018, 102, 231–242. [Google Scholar] [CrossRef]
- Alm, J.J.; Moritz, N.; Aro, H.T. In vitro osteogenic capacity of bone marrow MSCs from postmenopausal women reflect the osseointegration of their cementless hip stems. Bone Rep. 2016, 5, 124–135. [Google Scholar] [CrossRef][Green Version]
- Gasbarra, E.; Perrone, F.L.; Celi, M.; Rao, C.; Feola, M.; Cuozzo, N.; Tarantino, U. Total hip arthroplasty revision in elderly patients. Aging Clin. Exp. Res. 2013, 25 (Suppl. 1), S61–S63. [Google Scholar] [CrossRef]
- Ikeda, T.; Takahashi, K.; Kabata, T.; Sakagoshi, D.; Tomita, K.; Yamada, M. Polyneuropathy caused by cobalt-chromium metallosis after total hip replacement. Muscle Nerve 2010, 42, 140–143. [Google Scholar] [CrossRef]
- Czekaj, J.; Ehlinger, M.; Rahme, M.; Bonnomet, F. Metallosis and cobalt-chrome intoxication after hip resurfacing arthroplasty. J. Orthop. Sci. Off. J. Jpn. Orthop. Assoc. 2016, 21, 389–394. [Google Scholar] [CrossRef]
- Marzetti, E. Musculoskeletal Aging and Sarcopenia in the Elderly. Int. J. Mol. Sci. 2022, 23, 2808. [Google Scholar] [CrossRef]
- Bonanni, R.; Gino Grillo, S.; Cariati, I.; Tranquillo, L.; Iundusi, R.; Gasbarra, E.; Tancredi, V.; Tarantino, U. Osteosarcopenia and Pain: Do We Have a Way Out? Biomedicines 2023, 11, 1285. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Jo, D.; Yoon, G.; Kim, O.Y.; Song, J. A new paradigm in sarcopenia: Cognitive impairment caused by imbalanced myokine secretion and vascular dysfunction. Biomed. Pharmacother. 2022, 147, 112636. [Google Scholar] [CrossRef]
- Dao, T.; Green, A.E.; Kim, Y.A.; Bae, S.-J.; Ha, K.-T.; Gariani, K.; Lee, M.-R.; Menzies, K.J.; Ryu, D. Sarcopenia and Muscle Aging: A Brief Overview. Endocrinol. Metab. 2020, 35, 716–732. [Google Scholar] [CrossRef]
- Bilski, J.; Pierzchalski, P.; Szczepanik, M.; Bonior, J.; Zoladz, J.A. Multifactorial Mechanism of Sarcopenia and Sarcopenic Obesity. Role of Physical Exercise, Microbiota and Myokines. Cells 2022, 11, 160. [Google Scholar] [CrossRef] [PubMed]
- Scimeca, M.; Piccirilli, E.; Mastrangeli, F.; Rao, C.; Feola, M.; Orlandi, A.; Gasbarra, E.; Bonanno, E.; Tarantino, U. Bone Morphogenetic Proteins and myostatin pathways: Key mediator of human sarcopenia. J. Transl. Med. 2017, 15, 34. [Google Scholar] [CrossRef]
- Deng, B.; Zhang, F.; Wen, J.; Ye, S.; Wang, L.; Yang, Y.; Gong, P.; Jiang, S. The function of myostatin in the regulation of fat mass in mammals. Nutr. Metab. 2017, 14, 29. [Google Scholar] [CrossRef]
- Guo, T.; Jou, W.; Chanturiya, T.; Portas, J.; Gavrilova, O.; McPherron, A.C. Myostatin inhibition in muscle, but not adipose tissue, decreases fat mass and improves insulin sensitivity. PLoS ONE 2009, 4, e4937. [Google Scholar] [CrossRef]
- Konopka, A.R.; Wolff, C.A.; Suer, M.K.; Harber, M.P. Relationship between intermuscular adipose tissue infiltration and myostatin before and after aerobic exercise training. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2018, 315, R461–R468. [Google Scholar] [CrossRef]
- Sullivan-Gunn, M.J.; Lewandowski, P.A. Elevated hydrogen peroxide and decreased catalase and glutathione peroxidase protection are associated with aging sarcopenia. BMC Geriatr. 2013, 13, 104. [Google Scholar] [CrossRef]
- Lian, D.; Chen, M.-M.; Wu, H.; Deng, S.; Hu, X. The Role of Oxidative Stress in Skeletal Muscle Myogenesis and Muscle Disease. Antioxidants 2022, 11, 755. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-E.; Hsu, J.-C.; Chang, Y.-L.; Chuang, H.-C.; Chiu, Y.-L.; Chen, W.-L. Benzo[a]pyrene exposure in muscle triggers sarcopenia through aryl hydrocarbon receptor-mediated reactive oxygen species production. Ecotoxicol. Environ. Saf. 2022, 239, 113599. [Google Scholar] [CrossRef] [PubMed]
- Marzetti, E.; Calvani, R.; Cesari, M.; Buford, T.W.; Lorenzi, M.; Behnke, B.J.; Leeuwenburgh, C. Mitochondrial dysfunction and sarcopenia of aging: From signaling pathways to clinical trials. Int. J. Biochem. Cell Biol. 2013, 45, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- Alway, S.E.; Siu, P.M. Nuclear apoptosis contributes to sarcopenia. Exerc. Sport. Sci. Rev. 2008, 36, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Huo, F.; Liu, Q.; Liu, H. Contribution of muscle satellite cells to sarcopenia. Front. Physiol. 2022, 13, 892749. [Google Scholar] [CrossRef]
- Antuña, E.; Cachán-Vega, C.; Bermejo-Millo, J.C.; Potes, Y.; Caballero, B.; Vega-Naredo, I.; Coto-Montes, A.; Garcia-Gonzalez, C. Inflammaging: Implications in Sarcopenia. Int. J. Mol. Sci. 2022, 23, 15039. [Google Scholar] [CrossRef]
- Tu, H.; Li, Y.-L. Inflammation balance in skeletal muscle damage and repair. Front. Immunol. 2023, 14, 1133355. [Google Scholar] [CrossRef]
- Oliveira, C.A.; Candelária, I.S.; Oliveira, P.B.; Figueiredo, A.; Caseiro-Alves, F. Metallosis: A diagnosis not only in patients with metal-on-metal prostheses. Eur. J. Radiol. Open 2015, 2, 3–6. [Google Scholar] [CrossRef]
- Wolfson, M.; Curtin, P.; Curry, E.J.; Cerda, S.; Li, X. Giant cell tumor formation due to metallosis after open latarjet and partial shoulder resurfacing. Orthop. Rev. 2020, 12, 8522. [Google Scholar] [CrossRef]
- Green, B.; Griffiths, E.; Almond, S. Neuropsychiatric symptoms following metal-on-metal implant failure with cobalt and chromium toxicity. BMC Psychiatry 2017, 17, 33. [Google Scholar] [CrossRef]
- Jayasekera, N.; Gouk, C.; Patel, A.; Eyres, K. Apparent Skin Discoloration about the Knee Joint: A Rare Sequela of Metallosis after Total Knee Replacement. Case Rep. Orthop. 2015, 2015, 891904. [Google Scholar] [CrossRef] [PubMed]
- Cariati, I.; Bonanni, R.; Onorato, F.; Mastrogregori, A.; Rossi, D.; Iundusi, R.; Gasbarra, E.; Tancredi, V.; Tarantino, U. Role of Physical Activity in Bone-Muscle Crosstalk: Biological Aspects and Clinical Implications. J. Funct. Morphol. Kinesiol. 2021, 6, 55. [Google Scholar] [CrossRef] [PubMed]
- Cariati, I.; Scimeca, M.; Bonanni, R.; Triolo, R.; Naldi, V.; Toro, G.; Marini, M.; Tancredi, V.; Iundusi, R.; Gasbarra, E.; et al. Role of Myostatin in Muscle Degeneration by Random Positioning Machine Exposure: An in vitro Study for the Treatment of Sarcopenia. Front. Physiol. 2022, 13, 782000. [Google Scholar] [CrossRef] [PubMed]
- Elkasrawy, M.N.; Hamrick, M.W. Myostatin (GDF-8) as a key factor linking muscle mass and bone structure. J. Musculoskelet. Neuronal Interact. 2010, 10, 56–63. [Google Scholar]
- Bonanni, R.; Cariati, I.; Marini, M.; Tarantino, U.; Tancredi, V. Microgravity and Musculoskeletal Health: What Strategies Should Be Used for a Great Challenge? Life 2023, 13, 1423. [Google Scholar] [CrossRef]
- Palmieri, M.; Cariati, I.; Scimeca, M.; Pallone, G.; Bonanno, E.; Tancredi, V.; D’Arcangelo, G.; Frank, C. Effects of short-term aerobic exercise in a mouse model of Niemann-Pick type C disease on synaptic and muscle plasticity. Ann. Ist. Super. Sanita 2019, 55, 330–337. [Google Scholar] [CrossRef]
- Qin, Y.; Peng, Y.; Zhao, W.; Pan, J.; Ksiezak-Reding, H.; Cardozo, C.; Wu, Y.; Divieti Pajevic, P.; Bonewald, L.F.; Bauman, W.A.; et al. Myostatin inhibits osteoblastic differentiation by suppressing osteocyte-derived exosomal microRNA-218: A novel mechanism in muscle-bone communication. J. Biol. Chem. 2017, 292, 11021–11033. [Google Scholar] [CrossRef]
- Tang, L.; Yang, X.; Gao, X.; Du, H.; Han, Y.; Zhang, D.; Wang, Z.; Sun, L. Inhibiting myostatin signaling prevents femoral trabecular bone loss and microarchitecture deterioration in diet-induced obese rats. Exp. Biol. Med. 2016, 241, 308–316. [Google Scholar] [CrossRef]
- Piccirilli, E.; Cariati, I.; Primavera, M.; Triolo, R.; Gasbarra, E.; Tarantino, U. Augmentation in fragility fractures, bone of contention: A systematic review. BMC Musculoskelet. Disord. 2022, 23, 1046. [Google Scholar] [CrossRef]
- Sahan, I.; Anagnostakos, K. Metallosis after knee replacement: A review. Arch. Orthop. Trauma. Surg. 2020, 140, 1791–1808. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Values |
|---|---|
| Age (years) | 75 |
| BMI (Kg/cm2) | 24.7 |
| T-score (L1–L4) | −0.9 |
| T-score (femoral neck) | −0.1 |
| T-score (total femur) | 1.3 |
| PTH (pg/mL) | 55.0 |
| 25-(OH)-VitD (ng/mL) | 15.4 |
| HHS | 100 |
| Cr (μg/L) | 2.7 |
| Co (μg/L) | 2.1 |
| Urinary Cr (mcg/g) | 4.7 |
| Urinary Co (mcg/L) | 14.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonanni, R.; Abbondante, L.; Cariati, I.; Gasbarra, E.; Tarantino, U. Metallosis after Hip Arthroplasty Damages Skeletal Muscle: A Case Report. Geriatrics 2023, 8, 92. https://doi.org/10.3390/geriatrics8050092
Bonanni R, Abbondante L, Cariati I, Gasbarra E, Tarantino U. Metallosis after Hip Arthroplasty Damages Skeletal Muscle: A Case Report. Geriatrics. 2023; 8(5):92. https://doi.org/10.3390/geriatrics8050092
Chicago/Turabian StyleBonanni, Roberto, Lorenzo Abbondante, Ida Cariati, Elena Gasbarra, and Umberto Tarantino. 2023. "Metallosis after Hip Arthroplasty Damages Skeletal Muscle: A Case Report" Geriatrics 8, no. 5: 92. https://doi.org/10.3390/geriatrics8050092
APA StyleBonanni, R., Abbondante, L., Cariati, I., Gasbarra, E., & Tarantino, U. (2023). Metallosis after Hip Arthroplasty Damages Skeletal Muscle: A Case Report. Geriatrics, 8(5), 92. https://doi.org/10.3390/geriatrics8050092