
An Update on Apathy in Alzheimer’s Disease

 ,
,
Abstract
1. Introduction
2. Defining Apathy in Alzheimer’s Disease
3. Rating Scales and Assessments for Apathy in Alzheimer’s Disease
4. Prevalence of Apathy in Alzheimer’s Disease from MCI to Dementia
5. Correlates of Apathy in AD
6. Risk Factors for Apathy in AD
7. Underlying Neurobiology of Apathy in AD
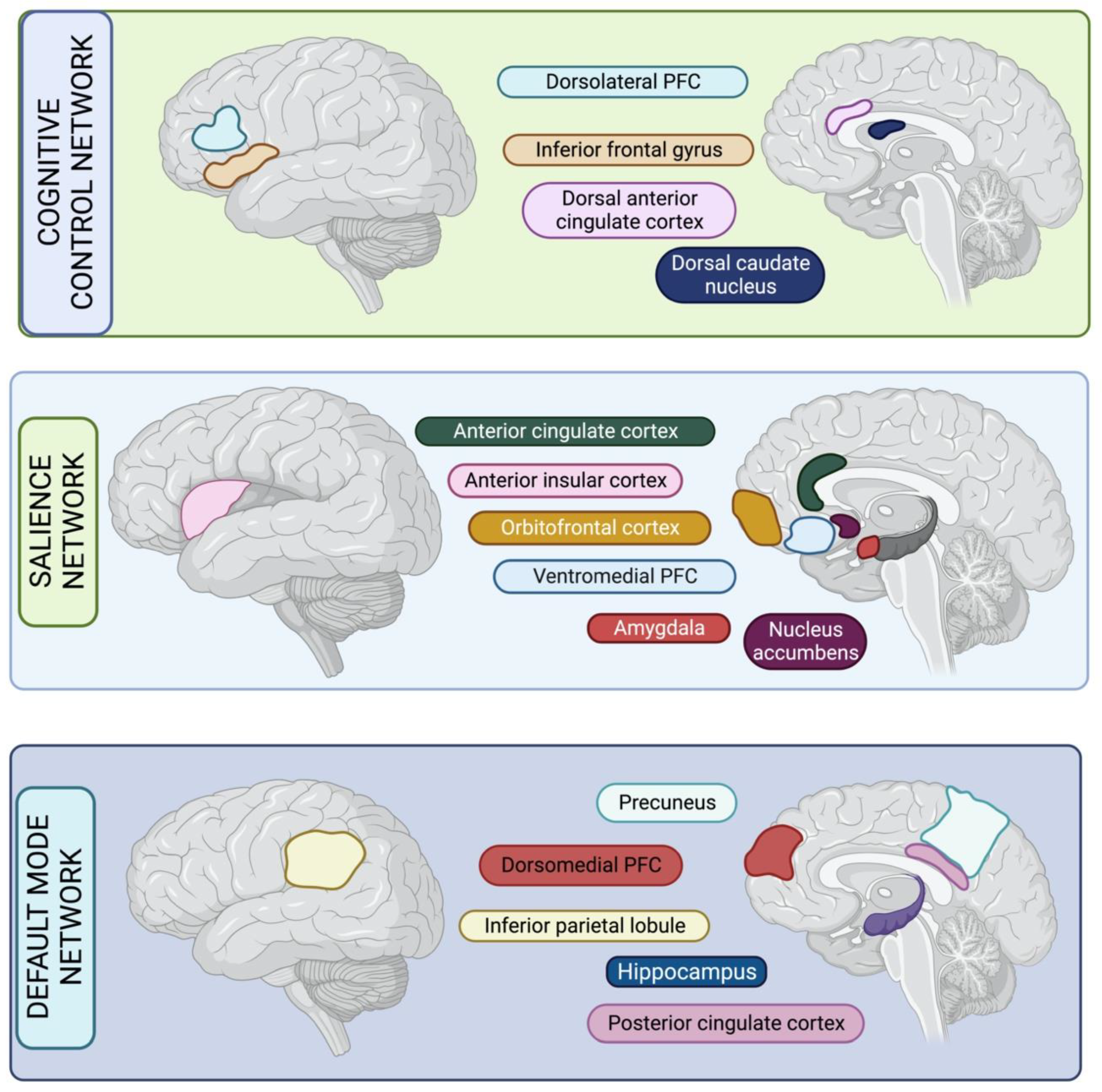
7.1. Networks Involved in Apathy Syndrome in AD
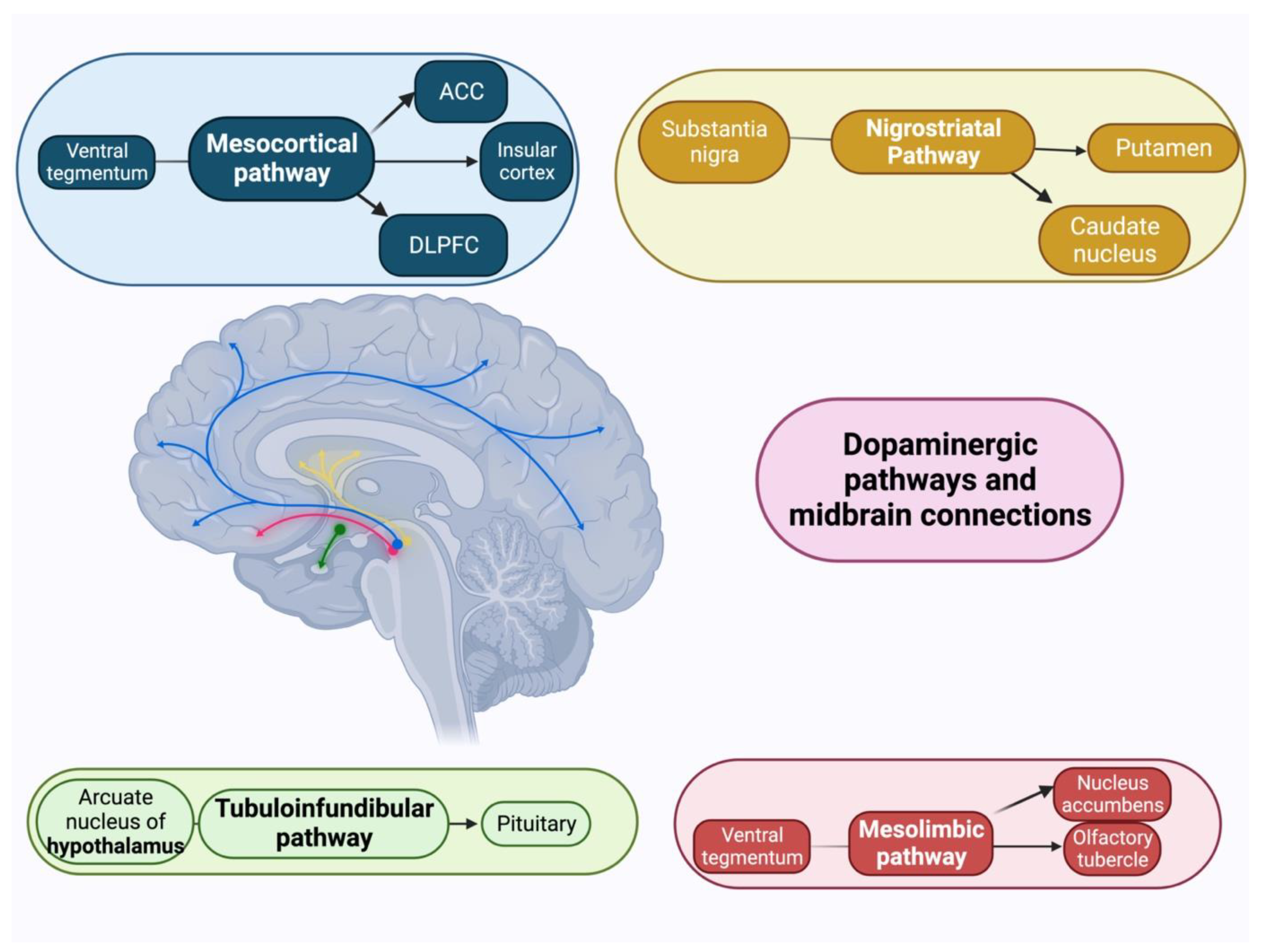
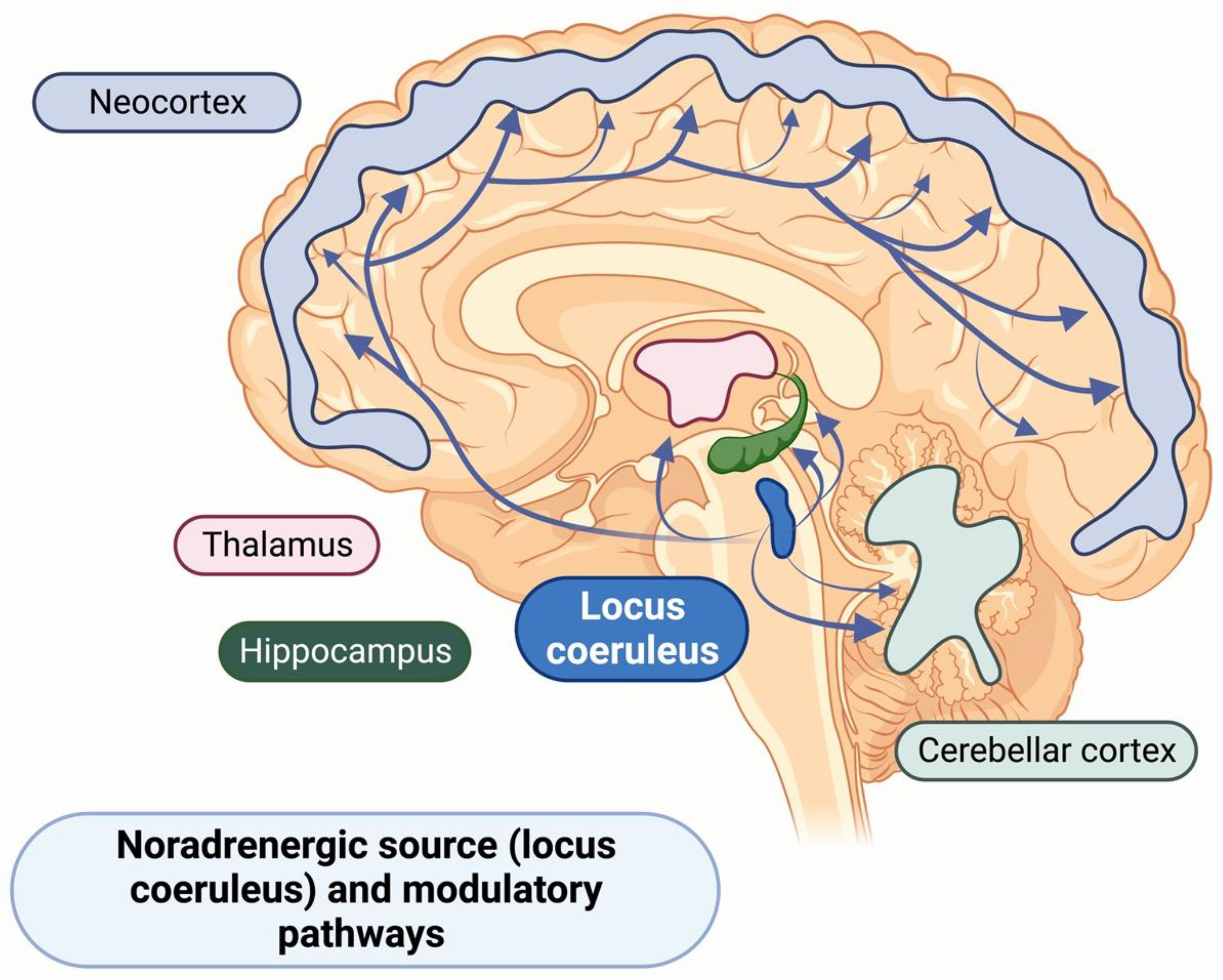
7.2. Neurochemistry of Apathy Syndrome in AD
8. Neuropsychology of Apathy in AD
9. Neuroimaging Studies of Apathy in AD
10. Treatment of Apathy in Alzheimer’s Disease
10.1. Non-Pharmacological Treatment of Apathy in AD
10.2. Pharmacological Management of Apathy in AD
10.3. Emerging Pharmacological Treatments for Apathy in AD
11. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [PubMed]
- Castro, D.M.; Dillon, C.; Machnicki, G.; Allegri, R.F. The economic cost of Alzheimer’s disease: Family or public health burden? Dement. Neuropsychol. 2010, 4, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Lyketsos, C.G.; Carrillo, M.C.; Ryan, J.M.; Khachaturian, A.S.; Trzepacz, P.; Amatniek, J.; Cedarbaum, J.; Brashear, R.; Miller, D.S. Neuropsychiatric symptoms in Alzheimer’s disease. Alzheimers Dement. 2011, 7, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.L.; Gonzales, M.M.; de Souza, L.C.; Weisenbach, S.L. Revisiting Apathy in Alzheimer’s Disease: From Conceptualization to Therapeutic Approaches. Behav. Neurol. 2021, 2021, 6319826. [Google Scholar] [CrossRef] [PubMed]
- Delfino, L.L.; Komatsu, R.S.; Komatsu, C.; Neri, A.L.; Cachioni, M. Neuropsychiatric symptoms associated with family caregiver burden and depression. Dement. Neuropsychol. 2021, 15, 128–135. [Google Scholar] [CrossRef]
- Khoo, S.A.; Chen, T.Y.; Ang, Y.H.; Yap, P. The impact of neuropsychiatric symptoms on caregiver distress and quality of life in persons with dementia in an Asian tertiary hospital memory clinic. Int. Psychogeriatr. 2013, 25, 1991–1999. [Google Scholar] [CrossRef]
- Truzzi, A.; Valente, L.; Engelhardt, E.; Laks, J. The association between caregiver distress and individual neuropsychiatric symptoms of dementia. Dement. Neuropsychol. 2013, 7, 286–291. [Google Scholar] [CrossRef]
- Shao, Y.; Xu, H.; Wang, J.; Dai, X.; Liang, W.; Ren, L.; Wang, Y. Agitation and apathy increase risk of dementia in psychiatric inpatients with late-onset psychiatric symptoms. BMC Psychiatry 2021, 21, 214. [Google Scholar] [CrossRef]
- Miller, D.S.; Robert, P.; Ereshefsky, L.; Adler, L.; Bateman, D.; Cummings, J.; DeKosky, S.T.; Fischer, C.E.; Husain, M.; Ismail, Z.; et al. Diagnostic criteria for apathy in neurocognitive disorders. Alzheimers Dement. 2021, 17, 1892–1904. [Google Scholar] [CrossRef]
- Ishii, S.; Weintraub, N.; Mervis, J.R. Apathy: A common psychiatric syndrome in the elderly. J. Am. Med. Dir. Assoc. 2009, 10, 381–393. [Google Scholar] [CrossRef]
- Aalten, P.; Verhey, F.R.; Boziki, M.; Bullock, R.; Byrne, E.J.; Camus, V.; Caputo, M.; Collins, D.; De Deyn, P.P.; Elina, K.; et al. Neuropsychiatric syndromes in dementia. Results from the European Alzheimer Disease Consortium: Part I. Dement. Geriatr. Cogn. Disord. 2007, 24, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Aalten, P.; Verhey, F.R.; Boziki, M.; Brugnolo, A.; Bullock, R.; Byrne, E.J.; Camus, V.; Caputo, M.; Collins, D.; De Deyn, P.P.; et al. Consistency of neuropsychiatric syndromes across dementias: Results from the European Alzheimer Disease Consortium. Part II. Dement. Geriatr. Cogn. Disord. 2008, 25, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, G.; Lucetti, C.; Danti, S.; Nuti, A. Apathy and dementia. Nosology, assessment and management. J. Nerv. Ment. Dis. 2014, 202, 718–724. [Google Scholar] [CrossRef]
- Nobis, L.; Husain, M. Apathy in Alzheimer’s disease. Curr. Opin. Behav. Sci. 2018, 22, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Marin, R.S. Differential diagnosis and classification of apathy. Am. J. Psychiatry 1990, 147, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Marin, R.S. Apathy: A neuropsychiatric syndrome. J. Neuropsychiatry Clin. Neurosci. 1991, 3, 243–254. [Google Scholar] [CrossRef]
- Robert, P.; Onyike, C.U.; Leentjens, A.F.; Dujardin, K.; Aalten, P.; Starkstein, S.; Verhey, F.R.; Yessavage, J.; Clement, J.P.; Drapier, D.; et al. Proposed diagnostic criteria for apathy in Alzheimer’s disease and other neuropsychiatric disorders. Eur. Psychiatry 2009, 24, 98–104. [Google Scholar] [CrossRef]
- Mulin, E.; Leone, E.; Dujardin, K.; Delliaux, M.; Leentjens, A.; Nobili, F.; Dessi, B.; Tible, O.; Agüera-Ortiz, L.; Osorio, R.S.; et al. Diagnostic criteria for apathy in clinical practice. Int. J. Geriatr. Psychiatry 2011, 26, 158–165. [Google Scholar] [CrossRef]
- Mortby, M.E.; Maercker, A.; Forstmeier, S. Midlife motivational abilities predict apathy and depression in Alzheimer disease: The aging, demographics, and memory study. J. Geriatr. Psychiatry Neurol. 2011, 24, 151–160. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Ingram, L.; Garau, M.L.; Mizrahi, R. On the overlap between apathy and depression in dementia. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1070–1074. [Google Scholar] [CrossRef]
- Benoit, M.; Berrut, G.; Doussaint, J.; Bakchine, S.; Bonin-Guillaume, S.; Frémont, P.; Gallarda, T.; Krolak-Salmon, P.; Marquet, T.; Mékiès, C.; et al. Apathy and depression in mild Alzheimer’s disease: A cross-sectional study using diagnostic criteria. J. Alzheimer’s Dis. 2012, 31, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Hongisto, K.; Hallikainen, I.; Selander, T.; Törmälehto, S.; Väätäinen, S.; Martikainen, J.; Välimäki, T.; Hartikainen, S.; Suhonen, J.; Koivisto, A.M. Quality of Life in relation to neuropsychiatric symptoms in Alzheimer’s disease: 5-year prospective ALSOVA cohort study. Int. J. Geriatr. Psychiatry 2018, 33, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Loewenstein, D.A.; Argüelles, S.; Bravo, M.; Freeman, R.Q.; Argüelles, T.; Acevedo, A.; Eisdorfer, C. Caregivers’ judgments of the functional abilities of the Alzheimer’s disease patient: A comparison of proxy reports and objective measures. J. Gerontol. B Psychol. Sci. Soc. Sci. 2001, 56, P78–P84. [Google Scholar] [CrossRef]
- Cummings, J.; Zhong, K. Trial design innovations: Clinical trials for treatment of neuropsychiatric symptoms in Alzheimer’s Disease. Clin. Pharmacol. Ther. 2015, 98, 483–485. [Google Scholar] [CrossRef]
- Murphy, C.; Dyer, A.H.; Lawlor, B.; Kennelly, S.P. Potentially inappropriate medication use in older adults with mild-moderate Alzheimer’s disease: Prevalence and associations with adverse events. Age Ageing 2020, 49, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Dyer, A.H.; Murphy, C.; Lawlor, B.; Kennelly, S.P.; For The Nilvad Study, G. Long-term antipsychotic use and cognitive decline in community-dwelling older adults with mild-moderate Alzheimer disease: Data from NILVAD. Int. J. Geriatr. Psychiatry 2021, 36, 1708–1721. [Google Scholar] [CrossRef]
- Dyer, A.H.; Murphy, C.; Briggs, R.; Lawlor, B.; Kennelly, S.P. Antidepressant use and orthostatic hypotension in older adults living with mild-to-moderate Alzheimer disease. Int. J. Geriatr. Psychiatry 2020, 35, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D.A.; Gornbein, J. The Neuropsychiatric Inventory: Comprehensive assessment of psychopathology in dementia. Neurology 1994, 44, 2308–2314. [Google Scholar] [CrossRef]
- Mohammad, D.; Ellis, C.; Rau, A.; Rosenberg, P.B.; Mintzer, J.; Ruthirakuhan, M.; Herrmann, N.; Lanctôt, K.L. Psychometric Properties of Apathy Scales in Dementia: A Systematic Review. J. Alzheimer’s Dis. 2018, 66, 1065–1082. [Google Scholar] [CrossRef]
- Cummings, J.L. The Neuropsychiatric Inventory: Assessing psychopathology in dementia patients. Neurology 1997, 48, S10–S16. [Google Scholar] [CrossRef]
- Marin, R.S.; Biedrzycki, R.C.; Firinciogullari, S. Reliability and validity of the Apathy Evaluation Scale. Psychiatry Res. 1991, 38, 143–162. [Google Scholar] [CrossRef] [PubMed]
- Guercio, B.J.; Donovan, N.J.; Munro, C.E.; Aghjayan, S.L.; Wigman, S.E.; Locascio, J.J.; Amariglio, R.E.; Rentz, D.M.; Johnson, K.A.; Sperling, R.A.; et al. The Apathy Evaluation Scale: A Comparison of Subject, Informant, and Clinician Report in Cognitively Normal Elderly and Mild Cognitive Impairment. J. Alzheimer’s Dis. 2015, 47, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.; Friedman, J.H.; Garibaldi, G.; Jones, M.; Macfadden, W.; Marsh, L.; Robert, P.H. Apathy in Neurodegenerative Diseases: Recommendations on the Design of Clinical Trials. J. Geriatr. Psychiatry Neurol. 2015, 28, 159–173. [Google Scholar] [CrossRef]
- Lee, B.; Gleason, C.; Umucu, E. Clinical utility and psychometric properties of the Apathy Evaluation Scale. Rehabil. Psychol. 2020, 65, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Furneri, G.; Platania, S.; Privitera, A.; Martelli, F.; Smeriglio, R.; Razza, G.; Maci, T.; Castellano, S.; Drago, F.; Santagati, M.; et al. The Apathy Evaluation Scale (AES-C): Psychometric Properties and Invariance of Italian Version in Mild Cognitive Impairment and Alzheimer’s Disease. Int. J. Environ. Res. Public Health 2021, 18, 9597. [Google Scholar] [CrossRef]
- Lueken, U.; Seidl, U.; Völker, L.; Schweiger, E.; Kruse, A.; Schröder, J. Development of a short version of the Apathy Evaluation Scale specifically adapted for demented nursing home residents. Am. J. Geriatr. Psychiatry 2007, 15, 376–385. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Mayberg, H.S.; Preziosi, T.J.; Andrezejewski, P.; Leiguarda, R.; Robinson, R.G. Reliability, validity, and clinical correlates of apathy in Parkinson’s disease. J. Neuropsychiatry Clin. Neurosci. 1992, 4, 134–139. [Google Scholar] [CrossRef]
- Robert, P.H.; Clairet, S.; Benoit, M.; Koutaich, J.; Bertogliati, C.; Tible, O.; Caci, H.; Borg, M.; Brocker, P.; Bedoucha, P. The apathy inventory: Assessment of apathy and awareness in Alzheimer’s disease, Parkinson’s disease and mild cognitive impairment. Int. J. Geriatr. Psychiatry 2002, 17, 1099–1105. [Google Scholar] [CrossRef]
- Strauss, M.E.; Sperry, S.D. An informant-based assessment of apathy in Alzheimer disease. Neuropsychiatry Neuropsychol. Behav. Neurol. 2002, 15, 176–183. [Google Scholar]
- Radakovic, R.; Starr, J.M.; Abrahams, S. A Novel Assessment and Profiling of Multidimensional Apathy in Alzheimer’s Disease. J. Alzheimer’s Dis. 2017, 60, 57–67. [Google Scholar] [CrossRef]
- Radakovic, R.; McGrory, S.; Chandran, S.; Swingler, R.; Pal, S.; Stephenson, L.; Colville, S.; Newton, J.; Starr, J.M.; Abrahams, S. The brief Dimensional Apathy Scale: A short clinical assessment of apathy. Clin. Neuropsychol. 2020, 34, 423–435. [Google Scholar] [CrossRef] [PubMed]
- Klar, V.S.; Ang, Y.S.; Lockwood, P.; Attaallah, B.; Dickson, S.; Drew, D.; Kienast, A.; Maio, M.R.; Plant, O.; Slavkova, E.; et al. Assessment of apathy in neurological patients using the Apathy Motivation Index caregiver version. J. Neuropsychol. 2022, 16, 236–258. [Google Scholar] [CrossRef] [PubMed]
- Sockeel, P.; Dujardin, K.; Devos, D.; Denève, C.; Destée, A.; Defebvre, L. The Lille apathy rating scale (LARS), a new instrument for detecting and quantifying apathy: Validation in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2006, 77, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Matarrubia, M.; Matías-Guiu, J.A.; Moreno-Ramos, T.; Valles-Salgado, M.; Marcos-Dolado, A.; García-Ramos, R.; Matías-Guiu, J. Validation of the Lille’s Apathy Rating Scale in Very Mild to Moderate Dementia. Am. J. Geriatr. Psychiatry 2016, 24, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Agüera-Ortiz, L.; Gil-Ruiz, N.; Cruz-Orduña, I.; Ramos-García, I.; Osorio, R.S.; Valentí-Soler, M.; Olazarán-Rodriguez, J.; Dobato-Ayuso, J.L.; Lanctôt, K.; Martínez-Martín, P. A novel rating scale for the measurement of apathy in institutionalized persons with dementia: The APADEM-NH. Am. J. Geriatr. Psychiatry 2015, 23, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Jao, Y.L.; Williams, K.; Mogle, J.; Behrens, L.; McDermott, C. Assessing apathy in long-term care residents with dementia: Who should be the rater? Dementia 2019, 18, 2220–2229. [Google Scholar] [CrossRef]
- Lanctôt, K.L.; Scherer, R.W.; Li, A.; Vieira, D.; Coulibaly, H.; Rosenberg, P.B.; Herrmann, N.; Lerner, A.J.; Padala, P.R.; Brawman-Mintzer, O.; et al. Measuring Apathy in Alzheimer’s Disease in the Apathy in Dementia Methylphenidate Trial 2 (ADMET 2): A Comparison of Instruments. Am. J. Geriatr. Psychiatry 2021, 29, 81–89. [Google Scholar] [CrossRef]
- Barnes, J.; Dickerson, B.C.; Frost, C.; Jiskoot, L.C.; Wolk, D.; van der Flier, W.M. Alzheimer’s disease first symptoms are age dependent: Evidence from the NACC dataset. Alzheimers Dement. 2015, 11, 1349–1357. [Google Scholar] [CrossRef]
- Kwon, C.Y.; Lee, B. Prevalence of Behavioral and Psychological Symptoms of Dementia in Community-Dwelling Dementia Patients: A Systematic Review. Front. Psychiatry 2021, 12, 741059. [Google Scholar] [CrossRef]
- Zhao, Q.F.; Tan, L.; Wang, H.F.; Jiang, T.; Tan, M.S.; Tan, L.; Xu, W.; Li, J.Q.; Wang, J.; Lai, T.J.; et al. The prevalence of neuropsychiatric symptoms in Alzheimer’s disease: Systematic review and meta-analysis. J. Affect. Disord. 2016, 190, 264–271. [Google Scholar] [CrossRef]
- Siafarikas, N.; Selbaek, G.; Fladby, T.; Šaltytė Benth, J.; Auning, E.; Aarsland, D. Frequency and subgroups of neuropsychiatric symptoms in mild cognitive impairment and different stages of dementia in Alzheimer’s disease. Int. Psychogeriatr. 2018, 30, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Forrester, S.N.; Gallo, J.J.; Smith, G.S.; Leoutsakos, J.M. Patterns of Neuropsychiatric Symptoms in Mild Cognitive Impairment and Risk of Dementia. Am. J. Geriatr. Psychiatry 2016, 24, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Palmer, K.; Di Iulio, F.; Varsi, A.E.; Gianni, W.; Sancesario, G.; Caltagirone, C.; Spalletta, G. Neuropsychiatric predictors of progression from amnestic-mild cognitive impairment to Alzheimer’s disease: The role of depression and apathy. J. Alzheimer’s Dis. 2010, 20, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Robert, P.H.; Berr, C.; Volteau, M.; Bertogliati-Fileau, C.; Benoit, M.; Guerin, O.; Sarazin, M.; Legrain, S.; Dubois, B. Importance of lack of interest in patients with mild cognitive impairment. Am. J. Geriatr. Psychiatry 2008, 16, 770–776. [Google Scholar] [CrossRef]
- Ruthirakuhan, M.; Herrmann, N.; Vieira, D.; Gallagher, D.; Lanctôt, K.L. The Roles of Apathy and Depression in Predicting Alzheimer Disease: A Longitudinal Analysis in Older Adults With Mild Cognitive Impairment. Am. J. Geriatr. Psychiatry 2019, 27, 873–882. [Google Scholar] [CrossRef]
- Fresnais, D.; Humble, M.B.; Bejerot, S.; Meehan, A.D.; Fure, B. Apathy as a Predictor for Conversion From Mild Cognitive Impairment to Dementia: A Systematic Review and Meta-Analysis of Longitudinal Studies. J. Geriatr. Psychiatry Neurol. 2023, 36, 3–17. [Google Scholar] [CrossRef]
- Goukasian, N.; Hwang, K.S.; Romero, T.; Grotts, J.; Do, T.M.; Groh, J.R.; Bateman, D.R.; Apostolova, L.G. Association of brain amyloidosis with the incidence and frequency of neuropsychiatric symptoms in ADNI: A multisite observational cohort study. BMJ Open 2019, 9, e031947. [Google Scholar] [CrossRef]
- Johansson, M.; Stomrud, E.; Johansson, P.M.; Svenningsson, A.; Palmqvist, S.; Janelidze, S.; van Westen, D.; Mattsson-Carlgren, N.; Hansson, O. Development of Apathy, Anxiety, and Depression in Cognitively Unimpaired Older Adults: Effects of Alzheimer’s Disease Pathology and Cognitive Decline. Biol. Psychiatry 2022, 92, 34–43. [Google Scholar] [CrossRef]
- Johansson, M.; Stomrud, E.; Lindberg, O.; Westman, E.; Johansson, P.M.; van Westen, D.; Mattsson, N.; Hansson, O. Apathy and anxiety are early markers of Alzheimer’s disease. Neurobiol. Aging 2020, 85, 74–82. [Google Scholar] [CrossRef]
- Banning, L.C.P.; Ramakers, I.; Rosenberg, P.B.; Lyketsos, C.G.; Leoutsakos, J.S. Alzheimer’s disease biomarkers as predictors of trajectories of depression and apathy in cognitively normal individuals, mild cognitive impairment, and Alzheimer’s disease dementia. Int. J. Geriatr. Psychiatry 2021, 36, 224–234. [Google Scholar] [CrossRef]
- Borges, L.G.; Rademaker, A.W.; Bigio, E.H.; Mesulam, M.M.; Weintraub, S. Apathy and Disinhibition Related to Neuropathology in Amnestic Versus Behavioral Dementias. Am. J. Alzheimer’s Dis. Dement. ® 2019, 34, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Quaranta, D.; Marra, C.; Rossi, C.; Gainotti, G.; Masullo, C. Different apathy profile in behavioral variant of frontotemporal dementia and Alzheimer’s disease: A preliminary investigation. Curr. Gerontol. Geriatr. Res. 2012, 2012, 719250. [Google Scholar] [CrossRef]
- Wei, G.; Irish, M.; Hodges, J.R.; Piguet, O.; Kumfor, F. Disease-specific profiles of apathy in Alzheimer’s disease and behavioural-variant frontotemporal dementia differ across the disease course. J. Neurol. 2020, 267, 1086–1096. [Google Scholar] [CrossRef] [PubMed]
- Kumfor, F.; Zhen, A.; Hodges, J.R.; Piguet, O.; Irish, M. Apathy in Alzheimer’s disease and frontotemporal dementia: Distinct clinical profiles and neural correlates. Cortex 2018, 103, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Gibson, L.L.; Grinberg, L.T.; Ffytche, D.; Leite, R.E.P.; Rodriguez, R.D.; Ferretti-Rebustini, R.E.L.; Pasqualucci, C.A.; Nitrini, R.; Jacob-Filho, W.; Aarsland, D.; et al. Neuropathological correlates of neuropsychiatric symptoms in dementia. Alzheimers Dement. 2022, 19, 1372–1382. [Google Scholar] [CrossRef]
- Gauthreaux, K.; Mock, C.; Teylan, M.A.; Culhane, J.E.; Chen, Y.C.; Chan, K.C.G.; Katsumata, Y.; Nelson, P.T.; Kukull, W.A. Symptomatic Profile and Cognitive Performance in Autopsy-Confirmed Limbic-Predominant Age-Related TDP-43 Encephalopathy With Comorbid Alzheimer Disease. J. Neuropathol. Exp. Neurol. 2022, 81, 975–987. [Google Scholar] [CrossRef]
- Castillo-García, I.M.; López-Álvarez, J.; Osorio, R.; Olazarán, J.; Ramos García, M.I.; Agüera-Ortiz, L. Clinical Trajectories of Neuropsychiatric Symptoms in Mild-Moderate to Advanced Dementia. J. Alzheimer’s Dis. 2022, 86, 861–875. [Google Scholar] [CrossRef]
- Brodaty, H.; Connors, M.H.; Xu, J.; Woodward, M.; Ames, D. The course of neuropsychiatric symptoms in dementia: A 3-year longitudinal study. J. Am. Med. Dir. Assoc. 2015, 16, 380–387. [Google Scholar] [CrossRef]
- Connors, M.H.; Teixeira-Pinto, A.; Ames, D.; Woodward, M.; Brodaty, H. Distinguishing apathy and depression in dementia: A longitudinal study. Aust. N. Z. J. Psychiatry 2022, 57, 884–894. [Google Scholar] [CrossRef]
- Grossman, H.T.; Sano, M.; Aloysi, A.; Elder, G.A.; Neugroschl, J.; Schimming, C.; Soleimani, L.; Zhu, C.W. Prevalent, persistent, and impairing: Longitudinal course and impact of apathy in Alzheimer’s disease. Alzheimers Dement. 2021, 13, e12169. [Google Scholar] [CrossRef]
- Vik-Mo, A.O.; Giil, L.M.; Ballard, C.; Aarsland, D. Course of neuropsychiatric symptoms in dementia: 5-year longitudinal study. Int. J. Geriatr. Psychiatry 2018, 33, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Wetzels, R.B.; Zuidema, S.U.; de Jonghe, J.F.; Verhey, F.R.; Koopmans, R.T. Course of neuropsychiatric symptoms in residents with dementia in nursing homes over 2-year period. Am. J. Geriatr. Psychiatry 2010, 18, 1054–1065. [Google Scholar] [CrossRef] [PubMed]
- Delgado, C.; Vergara, R.C.; Martínez, M.; Musa, G.; Henríquez, F.; Slachevsky, A. Neuropsychiatric Symptoms in Alzheimer’s Disease Are the Main Determinants of Functional Impairment in Advanced Everyday Activities. J. Alzheimer’s Dis. 2019, 67, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Lam, L.C.; Tam, C.W.; Chiu, H.F.; Lui, V.W. Depression and apathy affect functioning in community active subjects with questionable dementia and mild Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2007, 22, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Lechowski, L.; Benoit, M.; Chassagne, P.; Vedel, I.; Tortrat, D.; Teillet, L.; Vellas, B. Persistent apathy in Alzheimer’s disease as an independent factor of rapid functional decline: The REAL longitudinal cohort study. Int. J. Geriatr. Psychiatry 2009, 24, 341–346. [Google Scholar] [CrossRef]
- Liew, T.M. Neuropsychiatric symptoms in early stage of Alzheimer’s and non-Alzheimer’s dementia, and the risk of progression to severe dementia. Age Ageing 2021, 50, 1709–1718. [Google Scholar] [CrossRef]
- Saari, T.; Hallikainen, I.; Hintsa, T.; Koivisto, A.M. Neuropsychiatric symptoms and activities of daily living in Alzheimer’s disease: ALSOVA 5-year follow-up study. Int. Psychogeriatr. 2020, 32, 741–751. [Google Scholar] [CrossRef]
- Stella, F.; Laks, J.; Govone, J.S.; de Medeiros, K.; Forlenza, O.V. Association of neuropsychiatric syndromes with global clinical deterioration in Alzheimer’s disease patients. Int. Psychogeriatr. 2016, 28, 779–786. [Google Scholar] [CrossRef]
- Stella, F.; de Andrade, L.P.; Vital, T.M.; Coelho, F.G.M.; Nascimento, C.M.C.; Hernández, S.S.S. Apathy in Alzheimer’s disease: Contribution to a clinical view on progression of dementia. Dement. Neuropsychol. 2010, 4, 188–193. [Google Scholar] [CrossRef]
- Vilalta-Franch, J.; Calvó-Perxas, L.; Garre-Olmo, J.; Turró-Garriga, O.; López-Pousa, S. Apathy syndrome in Alzheimer’s disease epidemiology: Prevalence, incidence, persistence, and risk and mortality factors. J. Alzheimer’s Dis. 2013, 33, 535–543. [Google Scholar] [CrossRef]
- Zhu, C.W.; Grossman, H.T.; Sano, M. Why Do They Just Sit? Apathy as a Core Symptom of Alzheimer Disease. Am. J. Geriatr. Psychiatry 2019, 27, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Godinho, C.; Camozzato, A.; Kochhann, R.; Chaves, M.L.F. Association of caregiver demographic variables with neuropsychiatric symptoms in Alzheimer’s disease patients for distress on the Neuropsychiatric Inventory (NPI). Dement. Neuropsychol. 2008, 2, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Terum, T.M.; Testad, I.; Rongve, A.; Aarsland, D.; Svendsboe, E.; Andersen, J.R. The association between specific neuropsychiatric disturbances in people with Alzheimer’s disease and dementia with Lewy bodies and carer distress. Int. J. Geriatr. Psychiatry 2019, 34, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Camino, J.; Kishita, N.; Bregola, A.; Rubinsztein, J.; Khondoker, M.; Mioshi, E. How does carer management style influence the performance of activities of daily living in people with dementia? Int. J. Geriatr. Psychiatry 2021, 36, 1891–1898. [Google Scholar] [CrossRef] [PubMed]
- Wei, G.; Diehl-Schmid, J.; Matias-Guiu, J.A.; Pijnenburg, Y.; Landin-Romero, R.; Bogaardt, H.; Piguet, O.; Kumfor, F. The effects of the COVID-19 pandemic on neuropsychiatric symptoms in dementia and carer mental health: An international multicentre study. Sci. Rep. 2022, 12, 2418. [Google Scholar] [CrossRef]
- Simonetti, A.; Pais, C.; Jones, M.; Cipriani, M.C.; Janiri, D.; Monti, L.; Landi, F.; Bernabei, R.; Liperoti, R.; Sani, G. Neuropsychiatric Symptoms in Elderly With Dementia During COVID-19 Pandemic: Definition, Treatment, and Future Directions. Front. Psychiatry 2020, 11, 579842. [Google Scholar] [CrossRef]
- Eikelboom, W.S.; Pan, M.; Ossenkoppele, R.; Coesmans, M.; Gatchel, J.R.; Ismail, Z.; Lanctôt, K.L.; Fischer, C.E.; Mortby, M.E.; van den Berg, E.; et al. Sex differences in neuropsychiatric symptoms in Alzheimer’s disease dementia: A meta-analysis. Alzheimer’s Res. Ther. 2022, 14, 48. [Google Scholar] [CrossRef]
- Akyol, M.A.; Küçükgüçlü, Ö.; Yener, G. Investigation of Factors Affecting Apathy in Three Major Types of Dementia. Noro Psikiyatr. Ars. 2020, 57, 120–125. [Google Scholar] [CrossRef]
- Tanaka, H.; Hashimoto, M.; Fukuhara, R.; Ishikawa, T.; Yatabe, Y.; Kaneda, K.; Yuuki, S.; Honda, K.; Matsuzaki, S.; Tsuyuguchi, A.; et al. Relationship between dementia severity and behavioural and psychological symptoms in early-onset Alzheimer’s disease. Psychogeriatrics 2015, 15, 242–247. [Google Scholar] [CrossRef]
- Banning, L.C.P.; Ramakers, I.; Köhler, S.; Bron, E.E.; Verhey, F.R.J.; de Deyn, P.P.; Claassen, J.; Koek, H.L.; Middelkoop, H.A.M.; van der Flier, W.M.; et al. The Association Between Biomarkers and Neuropsychiatric Symptoms Across the Alzheimer’s Disease Spectrum. Am. J. Geriatr. Psychiatry 2020, 28, 735–744. [Google Scholar] [CrossRef]
- Skogseth, R.; Mulugeta, E.; Jones, E.; Ballard, C.; Rongve, A.; Nore, S.; Alves, G.; Aarsland, D. Neuropsychiatric correlates of cerebrospinal fluid biomarkers in Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2008, 25, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Banning, L.C.P.; Ramakers, I.; Deckers, K.; Verhey, F.R.J.; Aalten, P. Apolipoprotein E and affective symptoms in mild cognitive impairment and Alzheimer’s disease dementia: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2019, 96, 302–315. [Google Scholar] [CrossRef]
- Guimarães, H.C.; Caramelli, P.; Fialho, P.P.A.; França, E.P.; Afonso, M.P.D.; Teixeira, A.L. Serum levels of soluble TNF-α receptors but not BDNF are associated with apathy symptoms in mild Alzheimer’s disease and amnestic mild cognitive impairment. Dement. Neuropsychol. 2013, 7, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.L.; Salem, H.; Martins, L.B.; Gonzales, M.M.; Seshadri, S.; Suchting, R. Factors Associated with Apathy in Alzheimer’s Disease: A Cross-Sectional Analysis of the Texas Alzheimer’s Research and Care Consortium (TARCC) Study. J. Alzheimer’s Dis. 2022, 86, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Holmgren, S.; Hjorth, E.; Schultzberg, M.; Lärksäter, M.; Frenkel, D.; Tysen-Bäckström, A.C.; Aarsland, D.; Freund-Levi, Y. Neuropsychiatric symptoms in dementia-a role for neuroinflammation? Brain Res. Bull. 2014, 108, 88–93. [Google Scholar] [CrossRef]
- Ouanes, S.; Rabl, M.; Clark, C.; Kirschbaum, C.; Popp, J. Persisting neuropsychiatric symptoms, Alzheimer’s disease, and cerebrospinal fluid cortisol and dehydroepiandrosterone sulfate. Alzheimer’s Res. Ther. 2022, 14, 190. [Google Scholar] [CrossRef]
- Azocar, I.; Rapaport, P.; Burton, A.; Meisel, G.; Orgeta, V. Risk factors for apathy in Alzheimer’s disease: A systematic review of longitudinal evidence. Ageing Res. Rev. 2022, 79, 101672. [Google Scholar] [CrossRef]
- Yu, S.Y.; Lian, T.H.; Guo, P.; Li, L.X.; Ding, D.Y.; Li, D.N.; Liu, L.; Zhao, H.; Hu, Y.; Zuo, L.J.; et al. Correlations of apathy with clinical symptoms of Alzheimer’s disease and olfactory dysfunctions: A cross-sectional study. BMC Neurol. 2020, 20, 416. [Google Scholar] [CrossRef]
- Seligman, S.C.; Kamath, V.; Giovannetti, T.; Arnold, S.E.; Moberg, P.J. Olfaction and apathy in Alzheimer’s disease, mild cognitive impairment, and healthy older adults. Aging Ment. Health 2013, 17, 564–570. [Google Scholar] [CrossRef]
- Moretti, R.; Signori, R. Neural Correlates for Apathy: Frontal-Prefrontal and Parietal Cortical- Subcortical Circuits. Front. Aging Neurosci. 2016, 8, 289. [Google Scholar] [CrossRef]
- Bressler, S.L.; Menon, V. Large-scale brain networks in cognition: Emerging methods and principles. Trends Cogn. Sci. 2010, 14, 277–290. [Google Scholar] [CrossRef]
- Hamada, C.; Kawagoe, T.; Takamura, M.; Nagai, A.; Yamaguchi, S.; Onoda, K. Altered resting-state functional connectivity of the frontal-striatal circuit in elderly with apathy. PLoS ONE 2021, 16, e0261334. [Google Scholar] [CrossRef] [PubMed]
- Powers, J.P.; Massimo, L.; McMillan, C.T.; Yushkevich, P.A.; Zhang, H.; Gee, J.C.; Grossman, M. White matter disease contributes to apathy and disinhibition in behavioral variant frontotemporal dementia. Cogn. Behav. Neurol. 2014, 27, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.; Dubois, B. Apathy and the functional anatomy of the prefrontal cortex-basal ganglia circuits. Cereb. Cortex 2006, 16, 916–928. [Google Scholar] [CrossRef] [PubMed]
- Massimo, L.; Powers, J.P.; Evans, L.K.; McMillan, C.T.; Rascovsky, K.; Eslinger, P.; Ersek, M.; Irwin, D.J.; Grossman, M. Apathy in Frontotemporal Degeneration: Neuroanatomical Evidence of Impaired Goal-directed Behavior. Front. Hum. Neurosci. 2015, 9, 611. [Google Scholar] [CrossRef]
- Ducharme, S.; Price, B.H.; Dickerson, B.C. Apathy: A neurocircuitry model based on frontotemporal dementia. J. Neurol. Neurosurg. Psychiatry 2018, 89, 389–396. [Google Scholar] [CrossRef]
- Jenkins, L.M.; Wang, L.; Rosen, H.; Weintraub, S. A transdiagnostic review of neuroimaging studies of apathy and disinhibition in dementia. Brain 2022, 145, 1886–1905. [Google Scholar] [CrossRef]
- Lanctôt, K.L.; Agüera-Ortiz, L.; Brodaty, H.; Francis, P.T.; Geda, Y.E.; Ismail, Z.; Marshall, G.A.; Mortby, M.E.; Onyike, C.U.; Padala, P.R.; et al. Apathy associated with neurocognitive disorders: Recent progress and future directions. Alzheimers Dement. 2017, 13, 84–100. [Google Scholar] [CrossRef]
- Stuss, D.T.; Van Reekum, R.; Murphy, K.J. Differentiation of states and causes of apathy. In the Neuropsychology of Emotion; Borod, J.C., Ed.; Oxford University Press: Oxford, UK, 2000; pp. 340–363. [Google Scholar]
- Breukelaar, I.A.; Antees, C.; Grieve, S.M.; Foster, S.L.; Gomes, L.; Williams, L.M.; Korgaonkar, M.S. Cognitive control network anatomy correlates with neurocognitive behavior: A longitudinal study. Hum. Brain Mapp. 2017, 38, 631–643. [Google Scholar] [CrossRef]
- Badre, D.; Hoffman, J.; Cooney, J.W.; D’Esposito, M. Hierarchical cognitive control deficits following damage to the human frontal lobe. Nat. Neurosci. 2009, 12, 515–522. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: A latent variable analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed]
- Seeley, W.W. The Salience Network: A Neural System for Perceiving and Responding to Homeostatic Demands. J. Neurosci. 2019, 39, 9878–9882. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.C.; Knutson, B. Valence and salience contribute to nucleus accumbens activation. Neuroimage 2008, 39, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Menon, V. Large-scale brain networks and psychopathology: A unifying triple network model. Trends Cogn. Sci. 2011, 15, 483–506. [Google Scholar] [CrossRef] [PubMed]
- Bouret, S.; Richmond, B.J. Ventromedial and orbital prefrontal neurons differentially encode internally and externally driven motivational values in monkeys. J. Neurosci. 2010, 30, 8591–8601. [Google Scholar] [CrossRef] [PubMed]
- Rosen, H.J.; Hartikainen, K.M.; Jagust, W.; Kramer, J.H.; Reed, B.R.; Cummings, J.L.; Boone, K.; Ellis, W.; Miller, C.; Miller, B.L. Utility of clinical criteria in differentiating frontotemporal lobar degeneration (FTLD) from AD. Neurology 2002, 58, 1608–1615. [Google Scholar] [CrossRef]
- Boone, K.B.; Miller, B.L.; Swartz, R.; Lu, P.; Lee, A. Relationship between positive and negative symptoms and neuropsychological scores in frontotemporal dementia and Alzheimer’s disease. J. Int. Neuropsychol. Soc. 2003, 9, 698–709. [Google Scholar] [CrossRef]
- Craig, A.D. How do you feel—Now? The anterior insula and human awareness. Nat. Rev. Neurosci. 2009, 10, 59–70. [Google Scholar] [CrossRef]
- Allman, J.M.; Tetreault, N.A.; Hakeem, A.Y.; Manaye, K.F.; Semendeferi, K.; Erwin, J.M.; Park, S.; Goubert, V.; Hof, P.R. The von Economo neurons in the frontoinsular and anterior cingulate cortex. Ann. N. Y. Acad. Sci. 2011, 1225, 59–71. [Google Scholar] [CrossRef]
- Cavanna, A.E.; Trimble, M.R. The precuneus: A review of its functional anatomy and behavioural correlates. Brain 2006, 129, 564–583. [Google Scholar] [CrossRef]
- Amodio, D.M.; Frith, C.D. Meeting of minds: The medial frontal cortex and social cognition. Nat. Rev. Neurosci. 2006, 7, 268–277. [Google Scholar] [CrossRef]
- Berridge, K.C.; Robinson, T.E. What is the role of dopamine in reward: Hedonic impact, reward learning, or incentive salience? Brain Res. Brain Res. Rev. 1998, 28, 309–369. [Google Scholar] [CrossRef] [PubMed]
- Chong, T.T.; Husain, M. The role of dopamine in the pathophysiology and treatment of apathy. Prog. Brain Res. 2016, 229, 389–426. [Google Scholar] [CrossRef]
- Le Heron, C.; Apps, M.A.J.; Husain, M. The anatomy of apathy: A neurocognitive framework for amotivated behaviour. Neuropsychologia 2018, 118, 54–67. [Google Scholar] [CrossRef] [PubMed]
- David, R.; Mulin, E.; Friedman, L.; Le Duff, F.; Cygankiewicz, E.; Deschaux, O.; Garcia, R.; Yesavage, J.A.; Robert, P.H.; Zeitzer, J.M. Decreased daytime motor activity associated with apathy in Alzheimer disease: An actigraphic study. Am. J. Geriatr. Psychiatry 2012, 20, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Lanctôt, K.L.; Herrmann, N.; Black, S.E.; Ryan, M.; Rothenburg, L.S.; Liu, B.A.; Busto, U.E. Apathy associated with Alzheimer disease: Use of dextroamphetamine challenge. Am. J. Geriatr. Psychiatry 2008, 16, 551–557. [Google Scholar] [CrossRef]
- Betts, M.J.; Kirilina, E.; Otaduy, M.C.G.; Ivanov, D.; Acosta-Cabronero, J.; Callaghan, M.F.; Lambert, C.; Cardenas-Blanco, A.; Pine, K.; Passamonti, L.; et al. Locus coeruleus imaging as a biomarker for noradrenergic dysfunction in neurodegenerative diseases. Brain 2019, 142, 2558–2571. [Google Scholar] [CrossRef]
- Aston-Jones, G.; Cohen, J.D. An integrative theory of locus coeruleus-norepinephrine function: Adaptive gain and optimal performance. Annu. Rev. Neurosci. 2005, 28, 403–450. [Google Scholar] [CrossRef]
- Aston-Jones, G.; Waterhouse, B. Locus coeruleus: From global projection system to adaptive regulation of behavior. Brain Res. 2016, 1645, 75–78. [Google Scholar] [CrossRef]
- Szot, P.; Franklin, A.; Sikkema, C.; Wilkinson, C.W.; Raskind, M.A. Sequential Loss of LC Noradrenergic and Dopaminergic Neurons Results in a Correlation of Dopaminergic Neuronal Number to Striatal Dopamine Concentration. Front. Pharmacol. 2012, 3, 184. [Google Scholar] [CrossRef]
- Szot, P.; Knight, L.; Franklin, A.; Sikkema, C.; Foster, S.; Wilkinson, C.W.; White, S.S.; Raskind, M.A. Lesioning noradrenergic neurons of the locus coeruleus in C57Bl/6 mice with unilateral 6-hydroxydopamine injection, to assess molecular, electrophysiological and biochemical changes in noradrenergic signaling. Neuroscience 2012, 216, 143–157. [Google Scholar] [CrossRef] [PubMed]
- Zarow, C.; Lyness, S.A.; Mortimer, J.A.; Chui, H.C. Neuronal loss is greater in the locus coeruleus than nucleus basalis and substantia nigra in Alzheimer and Parkinson diseases. Arch. Neurol. 2003, 60, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Rommelfanger, K.S.; Weinshenker, D. Norepinephrine: The redheaded stepchild of Parkinson’s disease. Biochem. Pharmacol. 2007, 74, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Vazey, E.M.; Aston-Jones, G. The emerging role of norepinephrine in cognitive dysfunctions of Parkinson’s disease. Front. Behav. Neurosci. 2012, 6, 48. [Google Scholar] [CrossRef]
- Grossi, D.; Santangelo, G.; Barbarulo, A.M.; Vitale, C.; Castaldo, G.; Proto, M.G.; Siano, P.; Barone, P.; Trojano, L. Apathy and related executive syndromes in dementia associated with Parkinson’s disease and in Alzheimer’s disease. Behav. Neurol. 2013, 27, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Eggins, P.; Wong, S.; Wei, G.; Hodges, J.R.; Husain, M.; Piguet, O.; Irish, M.; Kumfor, F. A shared cognitive and neural basis underpinning cognitive apathy and planning in behavioural-variant frontotemporal dementia and Alzheimer’s disease. Cortex 2022, 154, 241–253. [Google Scholar] [CrossRef]
- Esposito, F.; Rochat, L.; Van der Linden, A.C.; Lekeu, F.; Quittre, A.; Charnallet, A.; Van der Linden, M. Apathy and executive dysfunction in Alzheimer disease. Alzheimer Dis. Assoc. Disord. 2010, 24, 131–137. [Google Scholar] [CrossRef]
- Nakaaki, S.; Murata, Y.; Sato, J.; Shinagawa, Y.; Hongo, J.; Tatsumi, H.; Hirono, N.; Mimura, M.; Furukawa, T.A. Association between apathy/depression and executive function in patients with Alzheimer’s disease. Int. Psychogeriatr. 2008, 20, 964–975. [Google Scholar] [CrossRef]
- Guimaraes, H.C.; Fialho, P.P.; Carvalho, V.A.; Machado, T.H.; Santos, E.L.; Caramelli, P. Apathy is not associated with performance in brief executive tests in patients with mild cognitive impairment and mild Alzheimer’s disease. Curr. Alzheimer Res. 2014, 11, 792–798. [Google Scholar] [CrossRef]
- Drijgers, R.L.; Verhey, F.R.; Leentjens, A.F.; Köhler, S.; Aalten, P. Neuropsychological correlates of apathy in mild cognitive impairment and Alzheimer’s disease: The role of executive functioning. Int. Psychogeriatr. 2011, 23, 1327–1333. [Google Scholar] [CrossRef]
- Bayard, S.; Jacus, J.P.; Raffard, S.; Gely-Nargeot, M.C. Apathy and emotion-based decision-making in amnesic mild cognitive impairment and Alzheimer’s disease. Behav. Neurol. 2014, 2014, 231469. [Google Scholar] [CrossRef]
- Wong, S.; Wei, G.; Husain, M.; Hodges, J.R.; Piguet, O.; Irish, M.; Kumfor, F. Altered reward processing underpins emotional apathy in dementia. Cogn. Affect. Behav. Neurosci. 2022, 23, 354–370. [Google Scholar] [CrossRef] [PubMed]
- Chau, S.A.; Chung, J.; Herrmann, N.; Eizenman, M.; Lanctôt, K.L. Apathy and Attentional Biases in Alzheimer’s Disease. J. Alzheimer’s Dis. 2016, 51, 837–846. [Google Scholar] [CrossRef]
- Jacus, J.P.; Voltzenlogel, V.; Mayelle, A.; Antoine, P.; Cuervo-Lombard, C.V. Awareness dimensions and associated factors in Alzheimer’s disease. Rev. Neurol. 2022, 178, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Jacus, J.P.; Voltzenlogel, V.; Antoine, P.; Cuervo-Lombard, C.V. Apathy Is the Best Dimension to Consider for Awareness Assessment in Alzheimer’s Disease. J. Alzheimer’s Dis. 2022, 87, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Perri, R.; Turchetta, C.S.; Caruso, G.; Fadda, L.; Caltagirone, C.; Carlesimo, G.A. Neuropsychological correlates of cognitive, emotional-affective and auto-activation apathy in Alzheimer’s disease. Neuropsychologia 2018, 118, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Theleritis, C.; Politis, A.; Siarkos, K.; Lyketsos, C.G. A review of neuroimaging findings of apathy in Alzheimer’s disease. Int. Psychogeriatr. 2014, 26, 195–207. [Google Scholar] [CrossRef]
- Alves, G.S.; Carvalho, A.F.; de Amorim de Carvalho, L.; Sudo, F.K.; Siqueira-Neto, J.I.; Oertel-Knochel, V.; Jurcoane, A.; Knochel, C.; Boecker, H.; Laks, J.; et al. Neuroimaging Findings Related to Behavioral Disturbances in Alzheimer’s Disease: A Systematic Review. Curr. Alzheimer Res. 2017, 14, 61–75. [Google Scholar] [CrossRef]
- Donovan, N.J.; Wadsworth, L.P.; Lorius, N.; Locascio, J.J.; Rentz, D.M.; Johnson, K.A.; Sperling, R.A.; Marshall, G.A. Regional cortical thinning predicts worsening apathy and hallucinations across the Alzheimer disease spectrum. Am. J. Geriatr. Psychiatry 2014, 22, 1168–1179. [Google Scholar] [CrossRef]
- Huey, E.D.; Lee, S.; Cheran, G.; Grafman, J.; Devanand, D.P. Brain Regions Involved in Arousal and Reward Processing are Associated with Apathy in Alzheimer’s Disease and Frontotemporal Dementia. J. Alzheimer’s Dis. 2017, 55, 551–558. [Google Scholar] [CrossRef]
- Marshall, G.A.; Monserratt, L.; Harwood, D.; Mandelkern, M.; Cummings, J.L.; Sultzer, D.L. Positron emission tomography metabolic correlates of apathy in Alzheimer disease. Arch. Neurol. 2007, 64, 1015–1020. [Google Scholar] [CrossRef] [PubMed]
- Moon, Y.; Moon, W.J.; Kim, H.; Han, S.H. Regional atrophy of the insular cortex is associated with neuropsychiatric symptoms in Alzheimer’s disease patients. Eur. Neurol. 2014, 71, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, P.B.; Nowrangi, M.A.; Lyketsos, C.G. Neuropsychiatric symptoms in Alzheimer’s disease: What might be associated brain circuits? Mol. Asp. Med. 2015, 43–44, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Tunnard, C.; Whitehead, D.; Hurt, C.; Wahlund, L.O.; Mecocci, P.; Tsolaki, M.; Vellas, B.; Spenger, C.; Kłoszewska, I.; Soininen, H.; et al. Apathy and cortical atrophy in Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2011, 26, 741–748. [Google Scholar] [CrossRef]
- Chaudhary, S.; Zhornitsky, S.; Chao, H.H.; van Dyck, C.H.; Li, C.R. Cerebral Volumetric Correlates of Apathy in Alzheimer’s Disease and Cognitively Normal Older Adults: Meta-Analysis, Label-Based Review, and Study of an Independent Cohort. J. Alzheimer’s Dis. 2022, 85, 1251–1265. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Brockman, S. The neuroimaging basis of apathy: Empirical findings and conceptual challenges. Neuropsychologia 2018, 118, 48–53. [Google Scholar] [CrossRef]
- Yeh, Y.C.; Li, C.W.; Kuo, Y.T.; Huang, M.F.; Liu, T.L.; Jaw, T.S.; Yang, Y.H.; Kuo, K.C.; Chen, C.S. Association between altered neurochemical metabolites and apathy in patients with Alzheimer’s disease. Int. Psychogeriatr. 2018, 30, 761–768. [Google Scholar] [CrossRef]
- Apostolova, L.G.; Akopyan, G.G.; Partiali, N.; Steiner, C.A.; Dutton, R.A.; Hayashi, K.M.; Dinov, I.D.; Toga, A.W.; Cummings, J.L.; Thompson, P.M. Structural correlates of apathy in Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2007, 24, 91–97. [Google Scholar] [CrossRef]
- Büyükgök, D.; Bayraktaroğlu, Z.; Buker, H.S.; Kulaksızoğlu, M.I.B.; Gurvit, İ.H. Resting-state fMRI analysis in apathetic Alzheimer’s disease. Diagn. Interv. Radiol. 2020, 26, 363–369. [Google Scholar] [CrossRef]
- Chan, N.K.; Gerretsen, P.; Chakravarty, M.M.; Blumberger, D.M.; Caravaggio, F.; Brown, E.; Graff-Guerrero, A. Structural Brain Differences Between Cognitively Impaired Patients With and Without Apathy. Am. J. Geriatr. Psychiatry 2021, 29, 319–332. [Google Scholar] [CrossRef]
- Chaudhary, S.; Zhornitsky, S.; Chao, H.H.; van Dyck, C.H.; Li, C.R. Hypothalamic Functional Connectivity and Apathy in People with Alzheimer’s Disease and Cognitively Normal Healthy Controls. J. Alzheimer’s Dis. 2022, 90, 1615–1628. [Google Scholar] [CrossRef]
- Guercio, B.J.; Donovan, N.J.; Ward, A.; Schultz, A.; Lorius, N.; Amariglio, R.E.; Rentz, D.M.; Johnson, K.A.; Sperling, R.A.; Marshall, G.A. Apathy is associated with lower inferior temporal cortical thickness in mild cognitive impairment and normal elderly individuals. J. Neuropsychiatry Clin. Neurosci. 2015, 27, e22–e27. [Google Scholar] [CrossRef]
- Kazui, H.; Takahashi, R.; Yamamoto, Y.; Yoshiyama, K.; Kanemoto, H.; Suzuki, Y.; Sato, S.; Azuma, S.; Suehiro, T.; Shimosegawa, E.; et al. Neural Basis of Apathy in Patients with Amnestic Mild Cognitive Impairment. J. Alzheimer’s Dis. 2017, 55, 1403–1416. [Google Scholar] [CrossRef]
- Desmarais, P.; Gao, A.F.; Lanctôt, K.; Rogaeva, E.; Ramirez, J.; Herrmann, N.; Stuss, D.T.; Black, S.E.; Keith, J.; Masellis, M. White matter hyperintensities in autopsy-confirmed frontotemporal lobar degeneration and Alzheimer’s disease. Alzheimer’s Res. Ther. 2021, 13, 129. [Google Scholar] [CrossRef] [PubMed]
- Torso, M.; Serra, L.; Giulietti, G.; Spanò, B.; Tuzzi, E.; Koch, G.; Caltagirone, C.; Cercignani, M.; Bozzali, M. Strategic lesions in the anterior thalamic radiation and apathy in early Alzheimer’s disease. PLoS ONE 2015, 10, e0124998. [Google Scholar] [CrossRef] [PubMed]
- Agüera-Ortiz, L.; Hernandez-Tamames, J.A.; Martinez-Martin, P.; Cruz-Orduña, I.; Pajares, G.; López-Alvarez, J.; Osorio, R.S.; Sanz, M.; Olazarán, J. Structural correlates of apathy in Alzheimer’s disease: A multimodal MRI study. Int. J. Geriatr. Psychiatry 2017, 32, 922–930. [Google Scholar] [CrossRef]
- Gatchel, J.R.; Donovan, N.J.; Locascio, J.J.; Becker, J.A.; Rentz, D.M.; Sperling, R.A.; Johnson, K.A.; Marshall, G.A. Regional 18F-Fluorodeoxyglucose Hypometabolism is Associated with Higher Apathy Scores Over Time in Early Alzheimer Disease. Am. J. Geriatr. Psychiatry 2017, 25, 683–693. [Google Scholar] [CrossRef] [PubMed]
- Hahn, C.; Lim, H.K.; Won, W.Y.; Ahn, K.J.; Jung, W.S.; Lee, C.U. Apathy and white matter integrity in Alzheimer’s disease: A whole brain analysis with tract-based spatial statistics. PLoS ONE 2013, 8, e53493. [Google Scholar] [CrossRef]
- Setiadi, T.M.; Martens, S.; Opmeer, E.M.; Marsman, J.C.; Tumati, S.; Reesink, F.E.; De Deyn, P.P.; Aleman, A.; Ćurčić-Blake, B. Widespread white matter aberration is associated with the severity of apathy in amnestic Mild Cognitive Impairment: Tract-based spatial statistics analysis. Neuroimage Clin. 2021, 29, 102567. [Google Scholar] [CrossRef]
- Jones, S.A.; De Marco, M.; Manca, R.; Bell, S.M.; Blackburn, D.J.; Wilkinson, I.D.; Soininen, H.; Venneri, A. Altered frontal and insular functional connectivity as pivotal mechanisms for apathy in Alzheimer’s disease. Cortex 2019, 119, 100–110. [Google Scholar] [CrossRef]
- Kim, J.W.; Lee, D.Y.; Choo, I.H.; Seo, E.H.; Kim, S.G.; Park, S.Y.; Woo, J.I. Microstructural alteration of the anterior cingulum is associated with apathy in Alzheimer disease. Am. J. Geriatr. Psychiatry 2011, 19, 644–653. [Google Scholar] [CrossRef]
- Ota, M.; Sato, N.; Nakata, Y.; Arima, K.; Uno, M. Relationship between apathy and diffusion tensor imaging metrics of the brain in Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2012, 27, 722–726. [Google Scholar] [CrossRef]
- Leung, D.K.Y.; Chan, W.C.; Spector, A.; Wong, G.H.Y. Prevalence of depression, anxiety, and apathy symptoms across dementia stages: A systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 2021, 36, 1330–1344. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.; Kang, I.; Park, J.S.; Na, S.H.; Kim, S.; Yoon, S.; Song, I.U.; Chung, Y.A. Regional Cerebral Blood Flow Correlates of Neuropsychiatric Symptom Domains in Early Alzheimer’s Disease. Diagnostics 2022, 12, 1246. [Google Scholar] [CrossRef]
- Jeong, H.; Kang, I.; Im, J.J.; Park, J.S.; Na, S.H.; Heo, Y.; Yang, Y.; Chung, Y.A.; Song, I.U. Brain Perfusion Correlates of Apathy in Alzheimer’s Disease. Dement. Neurocogn Disord. 2018, 17, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Lanctôt, K.L.; Moosa, S.; Herrmann, N.; Leibovitch, F.S.; Rothenburg, L.; Cotter, A.; Black, S.E. A SPECT study of apathy in Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2007, 24, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.Y.; Lee, J.S.; Kang, H.; Lee, H.W.; Kim, Y.K.; Jeon, H.J.; Chung, J.K.; Lee, M.C.; Cho, M.J.; Lee, D.S. Regional cerebral blood flow abnormalities associated with apathy and depression in Alzheimer disease. Alzheimer Dis. Assoc. Disord. 2012, 26, 217–224. [Google Scholar] [CrossRef]
- García-Alberca, J.M.; Florido, M.; Cáceres, M.; Sánchez-Toro, A.; Lara, J.P.; García-Casares, N. Medial temporal lobe atrophy is independently associated with behavioural and psychological symptoms in Alzheimer’s disease. Psychogeriatrics 2019, 19, 46–54. [Google Scholar] [CrossRef]
- Marshall, G.A.; Donovan, N.J.; Lorius, N.; Gidicsin, C.M.; Maye, J.; Pepin, L.C.; Becker, J.A.; Amariglio, R.E.; Rentz, D.M.; Sperling, R.A.; et al. Apathy is associated with increased amyloid burden in mild cognitive impairment. J. Neuropsychiatry Clin. Neurosci. 2013, 25, 302–307. [Google Scholar] [CrossRef]
- Marshall, G.A.; Gatchel, J.R.; Donovan, N.J.; Muniz, M.C.; Schultz, A.P.; Becker, J.A.; Chhatwal, J.P.; Hanseeuw, B.J.; Papp, K.V.; Amariglio, R.E.; et al. Regional Tau Correlates of Instrumental Activities of Daily Living and Apathy in Mild Cognitive Impairment and Alzheimer’s Disease Dementia. J. Alzheimer’s Dis. 2019, 67, 757–768. [Google Scholar] [CrossRef]
- Goris, E.D.; Ansel, K.N.; Schutte, D.L. Quantitative systematic review of the effects of non-pharmacological interventions on reducing apathy in persons with dementia. J. Adv. Nurs. 2016, 72, 2612–2628. [Google Scholar] [CrossRef] [PubMed]
- Oba, H.; Kobayashi, R.; Kawakatsu, S.; Suzuki, K.; Otani, K.; Ihara, K. Non-pharmacological Approaches to Apathy and Depression: A Scoping Review of Mild Cognitive Impairment and Dementia. Front. Psychol. 2022, 13, 815913. [Google Scholar] [CrossRef] [PubMed]
- Suarez Moreno, A.; Nguyen, J.P.; Calmelet, A.; Le Saout, E.; Damier, P.; de Decker, L.; Malineau, C.; Nizard, J.; Canoui-Poitrine, F.; Lefaucheur, J.P. Multi-site rTMS with cognitive training improves apathy in the long term in Alzheimer’s disease: A 4-year chart review. Clin. Neurophysiol. 2022, 137, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Padala, P.R.; Boozer, E.M.; Lensing, S.Y.; Parkes, C.M.; Hunter, C.R.; Dennis, R.A.; Caceda, R.; Padala, K.P. Neuromodulation for Apathy in Alzheimer’s Disease: A Double-Blind, Randomized, Sham-Controlled Pilot Study. J. Alzheimer’s Dis. 2020, 77, 1483–1493. [Google Scholar] [CrossRef] [PubMed]
- Padala, P.R.; Padala, K.P.; Lensing, S.Y.; Jackson, A.N.; Hunter, C.R.; Parkes, C.M.; Dennis, R.A.; Bopp, M.M.; Caceda, R.; Mennemeier, M.S.; et al. Repetitive transcranial magnetic stimulation for apathy in mild cognitive impairment: A double-blind, randomized, sham-controlled, cross-over pilot study. Psychiatry Res. 2018, 261, 312–318. [Google Scholar] [CrossRef]
- Fukushima, R.L.M.; do Carmo, E.G.; Pedroso, R.D.V.; Micali, P.N.; Donadelli, P.S.; Fuzaro, G.J.; Venancio, R.C.P.; Viola, J.; Costa, J.L.R. Effects of cognitive stimulation on neuropsychiatric symptoms in elderly with Alzheimer’s disease: A systematic review. Dement. Neuropsychol. 2016, 10, 178–184. [Google Scholar] [CrossRef]
- Niu, Y.X.; Tan, J.P.; Guan, J.Q.; Zhang, Z.Q.; Wang, L.N. Cognitive stimulation therapy in the treatment of neuropsychiatric symptoms in Alzheimer’s disease: A randomized controlled trial. Clin. Rehabil. 2010, 24, 1102–1111. [Google Scholar] [CrossRef]
- Hsieh, C.J.; Chang, C.; Su, S.F.; Shiao, Y.L. Reminiscence group therapy on depression and apathy in nursing home residents with mild-to-moderate dementia. J. Exp. Clin. Med. 2010, 2, 72–78. [Google Scholar] [CrossRef]
- Saredakis, D.; Keage, H.A.; Corlis, M.; Ghezzi, E.S.; Loffler, H.; Loetscher, T. The Effect of Reminiscence Therapy Using Virtual Reality on Apathy in Residential Aged Care: Multisite Nonrandomized Controlled Trial. J. Med. Internet Res. 2021, 23, e29210. [Google Scholar] [CrossRef]
- Raglio, A.; Bellelli, G.; Traficante, D.; Gianotti, M.; Ubezio, M.C.; Gentile, S.; Villani, D.; Trabucchi, M. Efficacy of music therapy treatment based on cycles of sessions: A randomised controlled trial. Aging Ment. Health 2010, 14, 900–904. [Google Scholar] [CrossRef]
- Raglio, A.; Bellelli, G.; Traficante, D.; Gianotti, M.; Ubezio, M.C.; Villani, D.; Trabucchi, M. Efficacy of music therapy in the treatment of behavioral and psychiatric symptoms of dementia. Alzheimer Dis. Assoc. Disord. 2008, 22, 158–162. [Google Scholar] [CrossRef]
- Kolanowski, A.; Litaker, M.; Buettner, L.; Moeller, J.; Costa, P.T., Jr. A randomized clinical trial of theory-based activities for the behavioral symptoms of dementia in nursing home residents. J. Am. Geriatr. Soc. 2011, 59, 1032–1041. [Google Scholar] [CrossRef] [PubMed]
- Lam, L.C.; Lui, V.W.; Luk, D.N.; Chau, R.; So, C.; Poon, V.; Tam, P.; Ching, R.; Lo, H.; Chiu, J.; et al. Effectiveness of an individualized functional training program on affective disturbances and functional skills in mild and moderate dementia—A randomized control trial. Int. J. Geriatr. Psychiatry 2010, 25, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Tappen, R.M.; Williams, C.L. Therapeutic conversation to improve mood in nursing home residents with Alzheimer’s disease. Res. Gerontol. Nurs. 2009, 2, 267–275. [Google Scholar] [CrossRef]
- Staal, J.A.; Sacks, A.; Matheis, R.; Collier, L.; Calia, T.; Hanif, H.; Kofman, E.S. The effects of Snoezelen (multi-sensory behavior therapy) and psychiatric care on agitation, apathy, and activities of daily living in dementia patients on a short term geriatric psychiatric inpatient unit. Int. J. Psychiatry Med. 2007, 37, 357–370. [Google Scholar] [CrossRef]
- Hattori, H.; Hattori, C.; Hokao, C.; Mizushima, K.; Mase, T. Controlled study on the cognitive and psychological effect of coloring and drawing in mild Alzheimer’s disease patients. Geriatr. Gerontol. Int. 2011, 11, 431–437. [Google Scholar] [CrossRef] [PubMed]
- van Weert, J.C.; van Dulmen, A.M.; Spreeuwenberg, P.M.; Ribbe, M.W.; Bensing, J.M. Behavioral and mood effects of snoezelen integrated into 24-hour dementia care. J. Am. Geriatr. Soc. 2005, 53, 24–33. [Google Scholar] [CrossRef]
- Ferrero-Arias, J.; Goñi-Imízcoz, M.; González-Bernal, J.; Lara-Ortega, F.; da Silva-González, A.; Díez-Lopez, M. The efficacy of nonpharmacological treatment for dementia-related apathy. Alzheimer Dis. Assoc. Disord. 2011, 25, 213–219. [Google Scholar] [CrossRef]
- Ruthirakuhan, M.T.; Herrmann, N.; Abraham, E.H.; Chan, S.; Lanctôt, K.L. Pharmacological interventions for apathy in Alzheimer’s disease. Cochrane Database Syst. Rev. 2018, 5, Cd012197. [Google Scholar] [CrossRef]
- Lee, C.W.; Chen, J.Y.; Ko, C.C.; Chuang, M.H.; Tsai, W.W.; Sun, C.K.; Hung, K.C. Efficacy of methylphenidate for the treatment of apathy in patients with Alzheimer’s disease: A systematic review and meta-analysis of randomized controlled studies. Psychopharmacology 2022, 239, 3743–3753. [Google Scholar] [CrossRef]
- Kishi, T.; Sakuma, K.; Iwata, N. Efficacy and Safety of Psychostimulants for Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Pharmacopsychiatry 2020, 53, 109–114. [Google Scholar] [CrossRef]
- Herrmann, N.; Rothenburg, L.S.; Black, S.E.; Ryan, M.; Liu, B.A.; Busto, U.E.; Lanctôt, K.L. Methylphenidate for the treatment of apathy in Alzheimer disease: Prediction of response using dextroamphetamine challenge. J. Clin. Psychopharmacol. 2008, 28, 296–301. [Google Scholar] [CrossRef]
- Rosenberg, P.B.; Lanctôt, K.L.; Drye, L.T.; Herrmann, N.; Scherer, R.W.; Bachman, D.L.; Mintzer, J.E.; Investigators, A. Safety and efficacy of methylphenidate for apathy in Alzheimer’s disease: A randomized, placebo-controlled trial. J. Clin. Psychiatry 2013, 74, 810–816. [Google Scholar] [CrossRef]
- Padala, P.R.; Padala, K.P.; Lensing, S.Y.; Ramirez, D.; Monga, V.; Bopp, M.M.; Roberson, P.K.; Dennis, R.A.; Petty, F.; Sullivan, D.H.; et al. Methylphenidate for Apathy in Community-Dwelling Older Veterans With Mild Alzheimer’s Disease: A Double-Blind, Randomized, Placebo-Controlled Trial. Am. J. Psychiatry 2018, 175, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Scherer, R.W.; Drye, L.; Mintzer, J.; Lanctôt, K.; Rosenberg, P.; Herrmann, N.; Padala, P.; Brawman-Mintzer, O.; Burke, W.; Craft, S.; et al. The Apathy in Dementia Methylphenidate Trial 2 (ADMET 2): Study protocol for a randomized controlled trial. Trials 2018, 19, 46. [Google Scholar] [CrossRef] [PubMed]
- Mintzer, J.; Lanctôt, K.L.; Scherer, R.W.; Rosenberg, P.B.; Herrmann, N.; van Dyck, C.H.; Padala, P.R.; Brawman-Mintzer, O.; Porsteinsson, A.P.; Lerner, A.J.; et al. Effect of Methylphenidate on Apathy in Patients With Alzheimer Disease: The ADMET 2 Randomized Clinical Trial. JAMA Neurol. 2021, 78, 1324–1332. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C. Methylphenidate and Other Pharmacologic Treatments for Apathy in Alzheimer’s Disease. J. Clin. Psychiatry 2022, 83, 39455. [Google Scholar] [CrossRef]
- Frakey, L.L.; Salloway, S.; Buelow, M.; Malloy, P. A randomized, double-blind, placebo-controlled trial of modafinil for the treatment of apathy in individuals with mild-to-moderate Alzheimer’s disease. J. Clin. Psychiatry 2012, 73, 796–801. [Google Scholar] [CrossRef]
- Maier, F.; Spottke, A.; Bach, J.P.; Bartels, C.; Buerger, K.; Dodel, R.; Fellgiebel, A.; Fliessbach, K.; Frölich, L.; Hausner, L.; et al. Bupropion for the Treatment of Apathy in Alzheimer Disease: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e206027. [Google Scholar] [CrossRef]
- Rodda, J.; Morgan, S.; Walker, Z. Are cholinesterase inhibitors effective in the management of the behavioral and psychological symptoms of dementia in Alzheimer’s disease? A systematic review of randomized, placebo-controlled trials of donepezil, rivastigmine and galantamine. Int. Psychogeriatr. 2009, 21, 813–824. [Google Scholar] [CrossRef]
- Waldemar, G.; Gauthier, S.; Jones, R.; Wilkinson, D.; Cummings, J.; Lopez, O.; Zhang, R.; Xu, Y.; Sun, Y.; Knox, S.; et al. Effect of donepezil on emergence of apathy in mild to moderate Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2011, 26, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Sepehry, A.A.; Sarai, M.; Hsiung, G.R. Pharmacological Therapy for Apathy in Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Can. J. Neurol. Sci. 2017, 44, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, N.; O’Regan, J.; Ruthirakuhan, M.; Kiss, A.; Eryavec, G.; Williams, E.; Lanctôt, K.L. A Randomized Placebo-Controlled Discontinuation Study of Cholinesterase Inhibitors in Institutionalized Patients With Moderate to Severe Alzheimer Disease. J. Am. Med. Dir. Assoc. 2016, 17, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Lanctôt, K.L.; Herrmann, N.; van Reekum, R.; Eryavec, G.; Naranjo, C.A. Gender, aggression and serotonergic function are associated with response to sertraline for behavioral disturbances in Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2002, 17, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Leonpacher, A.K.; Peters, M.E.; Drye, L.T.; Makino, K.M.; Newell, J.A.; Devanand, D.P.; Frangakis, C.; Munro, C.A.; Mintzer, J.E.; Pollock, B.G.; et al. Effects of Citalopram on Neuropsychiatric Symptoms in Alzheimer’s Dementia: Evidence From the CitAD Study. Am. J. Psychiatry 2016, 173, 473–480. [Google Scholar] [CrossRef]
- Trzepacz, P.T.; Cummings, J.; Konechnik, T.; Forrester, T.D.; Chang, C.; Dennehy, E.B.; Willis, B.A.; Shuler, C.; Tabas, L.B.; Lyketsos, C. Mibampator (LY451395) randomized clinical trial for agitation/aggression in Alzheimer’s disease. Int. Psychogeriatr. 2013, 25, 707–719. [Google Scholar] [CrossRef]
- Rosenberg, P.B.; Lanctôt, K.L.; Herrmann, N.; Mintzer, J.E.; Porsteinsson, A.P.; Sun, X.; Raman, R. Changes in Neuropsychiatric Inventory Associated with Semagacestat Treatment of Alzheimer’s Disease. J. Alzheimer’s Dis. 2016, 54, 373–381. [Google Scholar] [CrossRef]
- Cummings, J.; Lee, G.; Nahed, P.; Kambar, M.; Zhong, K.; Fonseca, J.; Taghva, K. Alzheimer’s disease drug development pipeline: 2022. Alzheimers Dement. 2022, 8, e12295. [Google Scholar] [CrossRef]
- Azhar, L.; Kusumo, R.W.; Marotta, G.; Lanctôt, K.L.; Herrmann, N. Pharmacological Management of Apathy in Dementia. CNS Drugs 2022, 36, 143–165. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Definition of Apathy in Neuro-Cognitive Disorders | |
|---|---|
| Definition | Components |
| European Psychiatric Association Diagnostic Criteria for Apathy in Alzheimer’s Disease and other Neuropsychiatric Disorders (2008) [17] | Apathy may be diagnosed if all four criteria are met: Loss of or diminished motivation compared to previous level of function (subjective or objective) The presence of at least one symptom in at least two of three domains of apathy for at least four weeks to include: reduced goal-directed behaviour reduced goal-directed cognitive activity loss of or diminished emotions Symptoms must result in clinically significant impairment Symptoms must not be explained by other possible causes, such as physical disabilities, change in level of consciousness, or the effect of a substance |
| The International Society for CNS Clinical Trials Methodology (ISCTM) Apathy Work Group Diagnostic Guidelines for Apathy in Neuro-Cognitive Disorders (2021) [9] | Apathy may be diagnosed if all four domains are fulfilled: Primary diagnosis: patient has diagnosis of cognitive impairment or dementia by established criteria Symptoms and duration: must be present for at least four weeks and represents a change from baseline and include two of the following: Reduced initiative (less spontaneity) Reduced interest (less curios or enthusiastic, reduced participation) Diminished emotional expression or responsiveness Symptoms must not be due to other illnesses, disability, related to substances or change in consciousness Symptoms must cause clinically significant impairment in functioning |
| Treatment Approaches for Apathy in AD | |
|---|---|
| Non-Pharmacological | Psychological: Cognitive stimulation therapy [187,188] Reminiscence therapy [189] Music-based therapy [190,191] One-to-one person-focused patient contact [192,193] Therapeutic conversation [194] Controlled multi-sensory environment [198] Neuromodulation: Repetitive transcranial magnetic stimulation (rTMS) [184,185,186] |
| Pharmacological | Apathy as primary outcome: Methylphenidate [203,204,205,207] Apathy as secondary outcome: Acetylcholinesterase inhibitors [200] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dolphin, H.; Dyer, A.H.; McHale, C.; O’Dowd, S.; Kennelly, S.P. An Update on Apathy in Alzheimer’s Disease. Geriatrics 2023, 8, 75. https://doi.org/10.3390/geriatrics8040075
Dolphin H, Dyer AH, McHale C, O’Dowd S, Kennelly SP. An Update on Apathy in Alzheimer’s Disease. Geriatrics. 2023; 8(4):75. https://doi.org/10.3390/geriatrics8040075
Chicago/Turabian StyleDolphin, Helena, Adam H. Dyer, Cathy McHale, Sean O’Dowd, and Sean P. Kennelly. 2023. "An Update on Apathy in Alzheimer’s Disease" Geriatrics 8, no. 4: 75. https://doi.org/10.3390/geriatrics8040075
APA StyleDolphin, H., Dyer, A. H., McHale, C., O’Dowd, S., & Kennelly, S. P. (2023). An Update on Apathy in Alzheimer’s Disease. Geriatrics, 8(4), 75. https://doi.org/10.3390/geriatrics8040075