
Comparing Auditory and Visual Distractions for Reducing Pain Severity and Pain Anxiety in Older Outpatients with Burn: A Randomized Controlled Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Subjects
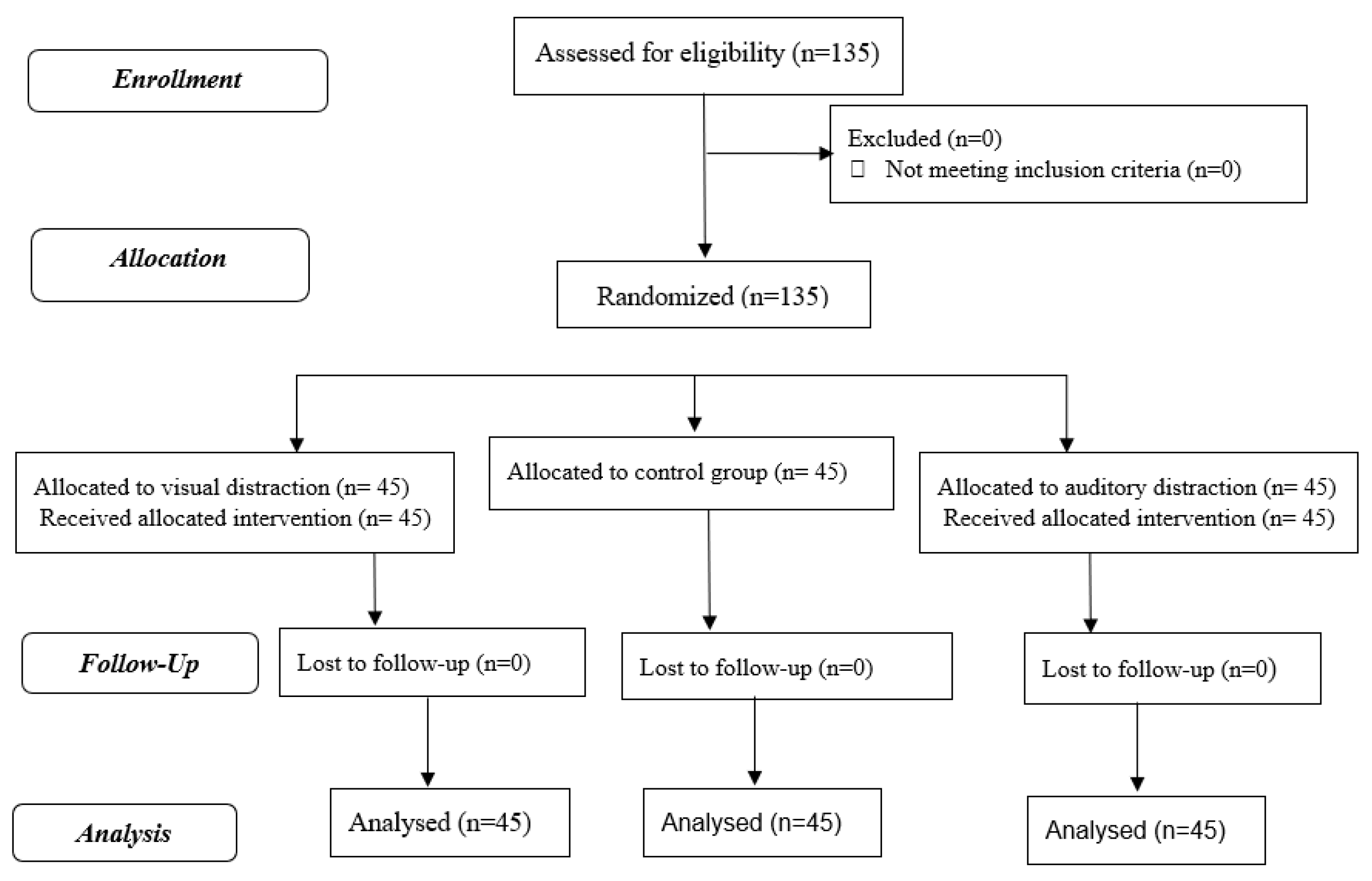
2.2. Sampling
2.3. Interventions
2.3.1. Auditory Distraction
2.3.2. Visual Distraction
2.3.3. Control Group
2.4. Outcomes
2.5. Data Collection
2.5.1. Demographic Data Form
2.5.2. Abbreviated Mental Test (AMT)
2.5.3. Pain Severity
2.5.4. Burn Specific Pain Anxiety Scale (BSPAS)
2.6. Statistical Data Analysis
2.7. Ethical Considerations
3. Results
3.1. Demographic Characteristics of the Participants
3.2. Pain Severity
3.3. Pain Anxiety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mengistu, N.D.; Obsa, M.S.; Gemeda, L.A. Burn Pain Management at Burn Unit of Yekatit 12 Hospitals, Addis Ababa. Pain Res. Treat. 2018, 2018, 1092650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, R.; Lozenski, J.; Wyatt, M.; Peña, M.; Northrop, K.; Bhavsar, D.; Kovac, A. Sedation and Analgesia for Dressing Change: A Survey of American Burn Association Burn Centers. J. Burn Care Res.: Off. Publ. Am. Burn Assoc. 2017, 38, e48–e54. [Google Scholar] [CrossRef] [PubMed]
- Spronk, I.; Legemate, C.; Oen, I.; van Loey, N.; Polinder, S.; van Baar, M. Health related quality of life in adults after burn injuries: A systematic review. PLoS ONE 2018, 13, e0197507. [Google Scholar] [CrossRef] [Green Version]
- Lundgren, R.S.; Kramer, C.B.; Rivara, F.P.; Wang, J.; Heimbach, D.M.; Gibran, N.S.; Klein, M.B. Influence of comorbidities and age on outcome following burn injury in older adults. J. Burn Care Res. 2009, 30, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowan, M.P.; Cancio, L.C.; Elster, E.A.; Burmeister, D.M.; Rose, L.F.; Natesan, S.; Chan, R.K.; Christy, R.J.; Chung, K.K. Burn wound healing and treatment: Review and advancements. Crit Care 2015, 19, 243. [Google Scholar] [CrossRef] [Green Version]
- Goei, H.; van Baar, M.E.; Dokter, J.; Vloemans, J.; Beerthuizen, G.I.J.M.; Middelkoop, E.; van der Vlies, K.H. Burns in the elderly: A nationwide study on management and clinical outcomes. Burn. Trauma 2020, 8, tkaa027. [Google Scholar] [CrossRef] [PubMed]
- Jeschke, M.G.; Peck, M.D. Burn Care of the Elderly. J. Burn Care Res.: Off. Publ. Am. Burn Assoc. 2017, 381. Jesch, e625–e628. [Google Scholar] [CrossRef]
- Bryant, C.; Jackson, H.; Ames, D. The prevalence of anxiety in older adults: Methodological issues and a review of the literature. J. Affect. Disord. 2008, 109, 233–250. [Google Scholar] [CrossRef]
- Magnon, V.; Dutheil, F.; Vallet, G.T. Benefits from one session of deep and slow breathing on vagal tone and anxiety in young and older adults. Sci. Rep. 2021, 11, 19267. [Google Scholar] [CrossRef]
- Kazeminia, M.; Salari, N.; Vaisi-Raygani, A.; Jalali, R.; Abdi, A.; Mohammadi, M.; Daneshkhah, A.; Hosseinian-Far, M.; Shohaimi, S. The effect of exercise on anxiety in the elderly worldwide: A systematic review and meta-analysis. Health Qual. Life Outcomes 2020, 18, 363. [Google Scholar] [CrossRef]
- Fallah, L.Y.; Ahmadi, A.; Ruche, A.B.; Taremiha, A.; Soltani, N.; Mafi, M. The effect of early change of skin graft dressing on pain and anxiety among burn patients: A two-group randomized controlled clinical trial. Int. J. Burn. Trauma 2019, 9, 13–18. [Google Scholar]
- Wang, Y.; Wu, B.; Ma, S.; Wang, D.; Gan, T.; Liu, H.; Yang, Z. Effect of mapping characteristic on audiovisual warning: Evidence from a simulated driving study. Appl. Ergon. 2022, 99, 103638. [Google Scholar] [CrossRef] [PubMed]
- Najafi Ghezeljeh, T.; Mohades Ardebili, F.; Rafii, F. The effects of massage and music on pain, anxiety and relaxation in burn patients: Randomized controlled clinical trial. Burn. J. Int. Soc. Burn Inj. 2017, 43, 1034–1043. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.N.; Kramer, C.B.; Wang, J.; Rivara, F.P.; Heimbach, D.M.; Gibran, N.S.; Klein, M.B. Epidemiology and outcomes of older adults with burn injury: An analysis of the National Burn Repository. J. Burn Care Res.: Off. Publ. Am. Burn Assoc. 2009, 30, 30–36. [Google Scholar] [CrossRef]
- James, D.L.; Jowza, M. Principles of Burn Pain Management. Clin. Plast. Surg. 2017, 44, 737–747. [Google Scholar] [CrossRef]
- Rohilla, L.; Agnihotri, M.; Trehan, S.K.; Sharma, R.K.; Ghai, S. Effect of Music Therapy on Pain Perception, Anxiety, and Opioid Use During Dressing Change Among Patients With Burns in India: A Quasi-experimental, Cross-over Pilot Study. Ostomy/Wound Manag. 2018, 64, 40–46. [Google Scholar] [CrossRef]
- Abdulla, A.; Adams, N.; Bone, M.; Elliott, A.M.; Gaffin, J.; Jones, D.; Knaggs, R.; Martin, D.; Sampson, L.; Schofield, P. Guidance on the management of pain in older people. Age Ageing 2013, 42 (Suppl. 1), i1-57. [Google Scholar] [CrossRef] [Green Version]
- De Silva, A.P.; Niriella, M.A.; Nandamuni, Y.; Nanayakkara, S.D.; Perera, K.R.P.; Kodisinghe, S.K.; Subasinghe, K.C.E.; Pathmeswaran, A.; de Silva, H.J. Effect of audio and visual distraction on patients undergoing colonoscopy: A randomized controlled study. Endosc. Int. Open 2016, 4, E1211–E1214. [Google Scholar] [CrossRef] [Green Version]
- Aghbolagh, M.G.; Bahrami, T.; Rejeh, N.; Heravi-Karimooi, M.; Tadrisi, S.D.; Vaismoradi, M. Comparison of the Effects of Visual and Auditory Distractions on Fistula Cannulation Pain among Older Patients Undergoing Hemodialysis: A Randomized Controlled Clinical Trial. Geriatrics 2020, 5, 53. [Google Scholar] [CrossRef]
- Azarmnejad, E.; Sarhangi, F.; Javadi, M.; Rejeh, N.; Amirsalari, S.; Tadrisi, S.D. The effectiveness of familiar auditory stimulus on hospitalized neonates’ physiologic responses to procedural pain. Int. J. Nurs. Pract. 2017, 23, e12527. [Google Scholar] [CrossRef]
- Xiaolian, J.; Xiaolin, L.; Lan, Z.H. Effects of visual and audiovisual distraction on pain and anxiety among patients undergoing colonoscopy. Gastroenterol. Nurs.: Off. J. Soc. Gastroenterol. Nurses Assoc. 2015, 38, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.H. How does distraction work in the management of pain? Curr. Pain Headache Rep. 2005, 9, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Yang, K.; Zhang, L.; Lu, X. Effect of media distraction (audio-visual and music) for pain and anxiety control in patients undergoing shock-wave lithotripsy: A systematic review and meta-analysis. Exp. Ther. Med. 2021, 21, 623. [Google Scholar] [CrossRef] [PubMed]
- Martins, B.; Sheppes, G.; Gross, J.J.; Mather, M. Age Differences in Emotion Regulation Choice: Older Adults Use Distraction Less Than Younger Adults in High-Intensity Positive Contexts. J. Gerontology. Ser. Bpsychological Sci. Soc. Sci. 2018, 73, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Clark, I.N.; Baker, F.A.; Taylor, N.F. Older Adults’ Music Listening Preferences to Support Physical Activity Following Cardiac Rehabilitation. J. Music Ther. 2016, 53, 364–397. [Google Scholar] [CrossRef]
- Gamble, K.R.; Howard, J.H.J.; Howard, D.V. Not just scenery: Viewing nature pictures improves executive attention in older adults. Exp. Aging Res. 2014, 40, 513–530. [Google Scholar] [CrossRef] [Green Version]
- Scapin, S.; Echevarría-Guanilo, M.E.; Boeira Fuculo Junior, P.R.; Gonçalves, N.; Rocha, P.K.; Coimbra, R. Virtual Reality in the treatment of burn patients: A systematic review. Burn.: J. Int. Soc. Burn Inj. 2018, 44, 1403–1416. [Google Scholar] [CrossRef]
- Furness, P.J.; Phelan, I.; Babiker, N.T.; Fehily, O.; Lindley, S.A.; Thompson, A.R. Reducing Pain During Wound Dressings in Burn Care Using Virtual Reality: A Study of Perceived Impact and Usability With Patients and Nurses. J. Burn Care Res.: Off. Publ. Am. Burn Assoc. 2019, 40, 878–885. [Google Scholar] [CrossRef]
- Hsu, K.-C.; Chen, L.F.; Hsiep, P.H. Effect of music intervention on burn patients’ pain and anxiety during dressing changes. Burn.: J. Int. Soc. Burn Inj. 2016, 42, 1789–1796. [Google Scholar] [CrossRef]
- Gezginci, E.; Iyigun, E.; Kibar, Y.; Bedir, S. Three Distraction Methods for Pain Reduction During Cystoscopy: A Randomized Controlled Trial Evaluating the Effects on Pain, Anxiety, and Satisfaction. J. Endourol. 2018, 32, 1078–1084. [Google Scholar] [CrossRef]
- Byers, J.F.; Bridges, S.; Kijek, J.; LaBorde, P. Burn patients’ pain and anxiety experiences. J. Burn Care Rehabil 2001, 22, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi Fakhar, F.; Rafii, F.; Jamshidi Orak, R. The effect of jaw relaxation on pain anxiety during burn dressings: Randomised clinical trial. Burn.: J. Int. Soc. Burn Inj. 2013, 39, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Faraji, J.; Khoshknab, M.F.; Khankeh, H. The effect of poetry therapy on the cognitive status in elderly residents of a nursing home. Complementary Med. J. Fac. Nurs. Midwifery 2013, 2, 33–44. [Google Scholar]
- Bakhtiyari, F.; Foroughan, M.; Fakhrzadeh, H.; Nazari, N.; Najafi, B.; Alizadeh, M.; Arzaghi, M.; Sharifi, F.; Shoaee, S.; Mostafa, Q. Validation of the persian version of Abbreviated Mental Test (AMT) in elderly residents of Kahrizak charity foundation. Iran. J. Diabetes Metab. 2014, 13, 487–494. [Google Scholar]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Taal, L.A.; Faber, A.W.; van Loey, N.E.; Reynders, C.L.; Hofland, H.W. The abbreviated burn specific pain anxiety scale: A multicenter study. Burn.: J. Int. Soc. Burn Inj. 1999, 25, 493–497. [Google Scholar] [CrossRef]
- Ghezeljeh, T.N.; Ardebili, F.M.; Rafii, F.; Hagani, H. Translation and psychometric evaluation of Persian versions of Burn Specific Pain Anxiety Scale and Impact of Event Scale. Burn.: J. Int. Soc. Burn Inj. 2013, 39, 1297–1303. [Google Scholar] [CrossRef]
- Chu, H.; Brailey, R.; Clarke, E.; Sen, S.K. Reducing pain through distraction therapy in small acute paediatric burns. Burns 2021, 47, 1635–1638. [Google Scholar] [CrossRef]
- Li, J.; Zhou, L.; Wang, Y. The effects of music intervention on burn patients during treatment procedures: A systematic review and meta-analysis of randomized controlled trials. Bmc Complementary Altern. Med. 2017, 17, 158. [Google Scholar] [CrossRef] [Green Version]
- Cheraghi, F.; Kalili, A.; Soltanian, A.; Eskandarlou, M.; Sharifian, P. A Comparison of the Effect of Visual and Auditory Distractions on Physiological Indicators and Pain of Burn Dressing Change Among 6-12-Year-Oldchildren: A Clinical Trial Study. J. Pediatric Nurs. 2021, 58, e81–e86. [Google Scholar] [CrossRef]
- Umezawa, S.; Higurashi, T.; Uchiyama, S.; Sakai, E.; Ohkubo, H.; Endo, H.; Nonaka, T.; Nakajima, A. Visual distraction alone for the improvement of colonoscopy-related pain and satisfaction. World J. Gastroenterol 2015, 21, 4707–4714. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, N.C.A.C.; Santos, J.L.F.; Linhares, M.B.M. Audiovisual distraction for pain relief in paediatric inpatients: A crossover study. Eur. J. Pain (Lond. Engl.) 2017, 21, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Cao, C.; Zhong, J.; Chen, J.; Cen, Y. Adjunctive virtual reality for procedural pain management of burn patients during dressing change or physical therapy: A systematic review and meta-analysis of randomized controlled trials. Wound Repair Regen. Off. Publ. Wound Heal. Soc. Eur. Tissue Repair Soc. 2019, 27, 90–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhlib, A.R.; Haffejee, M.; Nel, M.J. Pain modulation by audiovisual distraction during cystoscopy. Urol. Ann. 2021, 13, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Najafi Ghezeljeh, T.; Mohades Ardebili, F.; Rafii, F.; Manafi, F. The Effect of Massage on Anticipatory Anxiety and Procedural Pain in Patients with Burn Injury. World J. Plast. Surg. 2017, 6, 40–47. [Google Scholar] [PubMed]
- Tan, X.; Yowler, C.J.; Super, D.M.; Fratianne, R.B. The efficacy of music therapy protocols for decreasing pain, anxiety, and muscle tension levels during burn dressing changes: A prospective randomized crossover trial. J. Burn Care Res.: Off. Publ. Am. Burn Assoc. 2010, 31, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Fratianne, R.B.; Prensner, J.D.; Huston, M.J.; Super, D.M.; Yowler, C.J.; Standley, J.M. The effect of music-based imagery and musical alternate engagement on the burn debridement process. J. Burn Care Rehabil. 2001, 22, 47–53. [Google Scholar] [CrossRef]
- Ferguson, S.L.; Voll, K.V. Burn pain and anxiety: The use of music relaxation during rehabilitation. J. Burn Care Rehabil. 2004, 25, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Haythronthwaite, J.A.; Lawrence, J.W.; Fauerbach, J.A. Brief cognitive interventions for burn pain. Ann. Behav. Med.: A Publ. Soc. Behav. Med. 2001, 23, 42–49. [Google Scholar] [CrossRef]
- Schwan, J.; Sclafani, J.; Tawfik, V.L. Chronic Pain Management in the Elderly. Anesth. Clin 2019, 37, 547–560. [Google Scholar] [CrossRef]
- Fernie, B.A.; Wright, T.; Caselli, G.; Nikčević, A.V.; Spada, M.M. Metacognitions as Mediators of Gender Identity-related Anxiety. Clin. Psychol. Psychother. 2017, 24, 264–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieretti, S.; Di Giannuario, A.; Di Giovannandrea, R.; Marzoli, F.; Piccaro, G.; Minosi, P.; Aloisi, A.M. Gender differences in pain and its relief. Ann. Dell’istituto Super. Di Sanita 2016, 52, 184–189. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Groups | Test, p-Value | ||
|---|---|---|---|---|
| Auditory Distraction Mean ± SD | Visual Distraction Mean ± SD | Control Mean ± SD | ||
| Age, year | 66.07 ± 5.24 | 67.69 ± 4.22 | 67.56 ± 5.02 | H (2) = 3.36 |
| p * = 0.18 | ||||
| Percentage of the burn, % | 76.79 ± 8.4 | 49.34 ± 8.4 | 62.45 ± 8.3 | H (2) = 0.52 |
| p = 0.77 | ||||
| Characteristic | Auditory Distraction n(%) | Visual Distraction n(%) | Control n(%) | Test, p-value |
| Marital Status | ||||
| Married | 33 (24.4) | 32 (23.7) | 38 (28.1) | X2(2) = 2.53 p ** = 0.28 |
| Widower/divorced | 12 (8.9) | 13 (9.6) | 7 (5.2) | |
| Education Level | ||||
| Illiterate | 2 (1.5) | 11 (8.1) | 7 (5.2) | X2(6) = 11.21 p = 0.08 |
| Elementary | 25 (18.5) | 16 (11.9) | 17 (12.6) | |
| Diploma | 15 (11.1) | 11 (8.1) | 16 (11.9) | |
| Academic | 3 (2.2) | 7 (5.2) | 5 (3.7) | |
| Occupation | ||||
| Employee | 6 (4.4) | 13 (9.6) | 4 (3) | X2(4) = 9.29 p = 0.05 |
| Self-employment | 18 (13.3) | 9 (6.7) | 16 (11.9) | |
| Retired | 21 (15.6) | 23 (17) | 25 (18.5) | |
| Living Condition | ||||
| Alone | 13 (9.6) | 9 (6.7) | 16 (11.9) | X2(4) = 8.34 p = 0.08 |
| With spouse | 21 (15.6) | 23 (17) | 25 (18.5) | |
| With spouse and children | 11 (8.1) | 19 (14.1) | 16 (11.9) | |
| Smoking | ||||
| Yes | 26 (19.3) | 22 (16.3) | 32 (23.7) | X2(2) = 4.66 p = 0.09 |
| No | 19 (14.1) | 23 (17) | 13 (9.6) | |
| Reason for the Burn | ||||
| Hot object, chemical material, electricity | 16 (11.9) | 17 (12.6) | 16 (11.9) | X2(4) = 0.34 p = 0.98 |
| Hot liquid | 15 (11.1) | 15 (11.1) | 17 (12.6) | |
| Area of the Burn | ||||
| Having single burn (hand or foot) | 12 (8.9) | 20 (14.8) | 12(8.9) | X2(2) = 4.31 p = 0.11 |
| Having multiple burns (hand and foot) | 33 (24.4) | 25 (18.5) | 33(24.4) | |
| Painkiller Use | ||||
| Acetaminophen or Gelofen | 21 (15.6) | 23 (17) | 24 (17.8) | X2(2) = 0.41 p = 0.81 |
| No medication | 24 (17.8) | 22 (16.6) | 21 (15.6) | |
| Groups. | Before the Intervention Mean ± SD | After the Intervention Mean ± SD | After Wound Dressing Mean ± SD |
|---|---|---|---|
| Auditory Distraction | 7.77 ± 0.70 | 7.08 ± 1.12 | 7.17 ± 1.00 |
| Severe pain | Severe pain | Severe pain | |
| Visual Distraction | 7.75 ± 0.64 | 6.06 ± 0.91 | 6.62 ± 1.19 |
| Severe pain | Moderate pain | Moderate pain | |
| Control | 7.60 ± 0.86 | 7.73 ± 0.75 | 7.68 ± 0.87 |
| Severe pain | Severe pain | Severe pain | |
| p-value a | Group | Time | Group × time |
| W b (2) = 79.85 p = 0.001 | W (1) =2.96 p = 0.08 | W (2) =7.54 p = 0.02 |
| Study Group | Before the Intervention | After the Intervention | After Wound Dressing | Statistical Test | Effect Size |
|---|---|---|---|---|---|
| Auditory distraction | 70.22 ± 6.49 | 64.37 ± 9.59 | 66.91 ± 6.11 | M a (2) = 0.80 | ή2 c = 0.09 |
| p = 0.009 | |||||
| F b (1.6, 73.5) = 7.48 | d d = 0.6 | ||||
| p = 0.002 | |||||
| Visual distraction | 70.20 ± 5.64 | 62.55 ± 6.98 | 65.11 ± 6.46 | M (2) = 0.97 | ή2 = 0.20 |
| p = 0.62 | |||||
| F (2, 88) = 17.72 | d = 1 | ||||
| p = 0.001 | |||||
| Control | 70.86 ± 6.87 | 70.51 ± 7.65 | 70.33 ± 7.52 | M (2) = 0.98 | |
| p = 0.68 | |||||
| F (2, 88) = 0.08 | |||||
| p = 0.91 | |||||
| Group | Group × time | ||||
| F (2, 264) = 17.23, p = 0.001 | F (4, 264) = 3.88 | ή2 = 0.063, d = 0.51 | |||
| p = 0.001 | |||||
| M (2) = 0.97, p = 0.62 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moradipoor, Y.; Rejeh, N.; Heravi Karimooi, M.; Tadrisi, S.D.; Dahmardehei, M.; Bahrami, T.; Vaismoradi, M. Comparing Auditory and Visual Distractions for Reducing Pain Severity and Pain Anxiety in Older Outpatients with Burn: A Randomized Controlled Trial. Geriatrics 2022, 7, 54. https://doi.org/10.3390/geriatrics7030054
Moradipoor Y, Rejeh N, Heravi Karimooi M, Tadrisi SD, Dahmardehei M, Bahrami T, Vaismoradi M. Comparing Auditory and Visual Distractions for Reducing Pain Severity and Pain Anxiety in Older Outpatients with Burn: A Randomized Controlled Trial. Geriatrics. 2022; 7(3):54. https://doi.org/10.3390/geriatrics7030054
Chicago/Turabian StyleMoradipoor, Yaghob, Nahid Rejeh, Majideh Heravi Karimooi, Seyed Davood Tadrisi, Mostafa Dahmardehei, Tahereh Bahrami, and Mojtaba Vaismoradi. 2022. "Comparing Auditory and Visual Distractions for Reducing Pain Severity and Pain Anxiety in Older Outpatients with Burn: A Randomized Controlled Trial" Geriatrics 7, no. 3: 54. https://doi.org/10.3390/geriatrics7030054
APA StyleMoradipoor, Y., Rejeh, N., Heravi Karimooi, M., Tadrisi, S. D., Dahmardehei, M., Bahrami, T., & Vaismoradi, M. (2022). Comparing Auditory and Visual Distractions for Reducing Pain Severity and Pain Anxiety in Older Outpatients with Burn: A Randomized Controlled Trial. Geriatrics, 7(3), 54. https://doi.org/10.3390/geriatrics7030054