
The Challenge of Subjective Cognitive Complaints and Executive Functions in Middle-Aged Adults as a Preclinical Stage of Dementia: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Systematic Search (Databases, Descriptors, Search Formulas)
2.2. Inclusion Criteria
- 1.
- Empirical research on the relationship between subjective cognitive complaints and executive functions in preclinical stages of dementia;
- 2.
- Papers published from 2005 to the present and with a study population specificity of 60 years of age and older.
2.3. Exclusion Criteria
- 3.
- Papers addressing the topic of subjective cognitive complaints in a general or specific way in other clinical contexts;
- 4.
- Studies analyzing executive functions in stages where there is already a diagnosis of dementia in advanced stages.
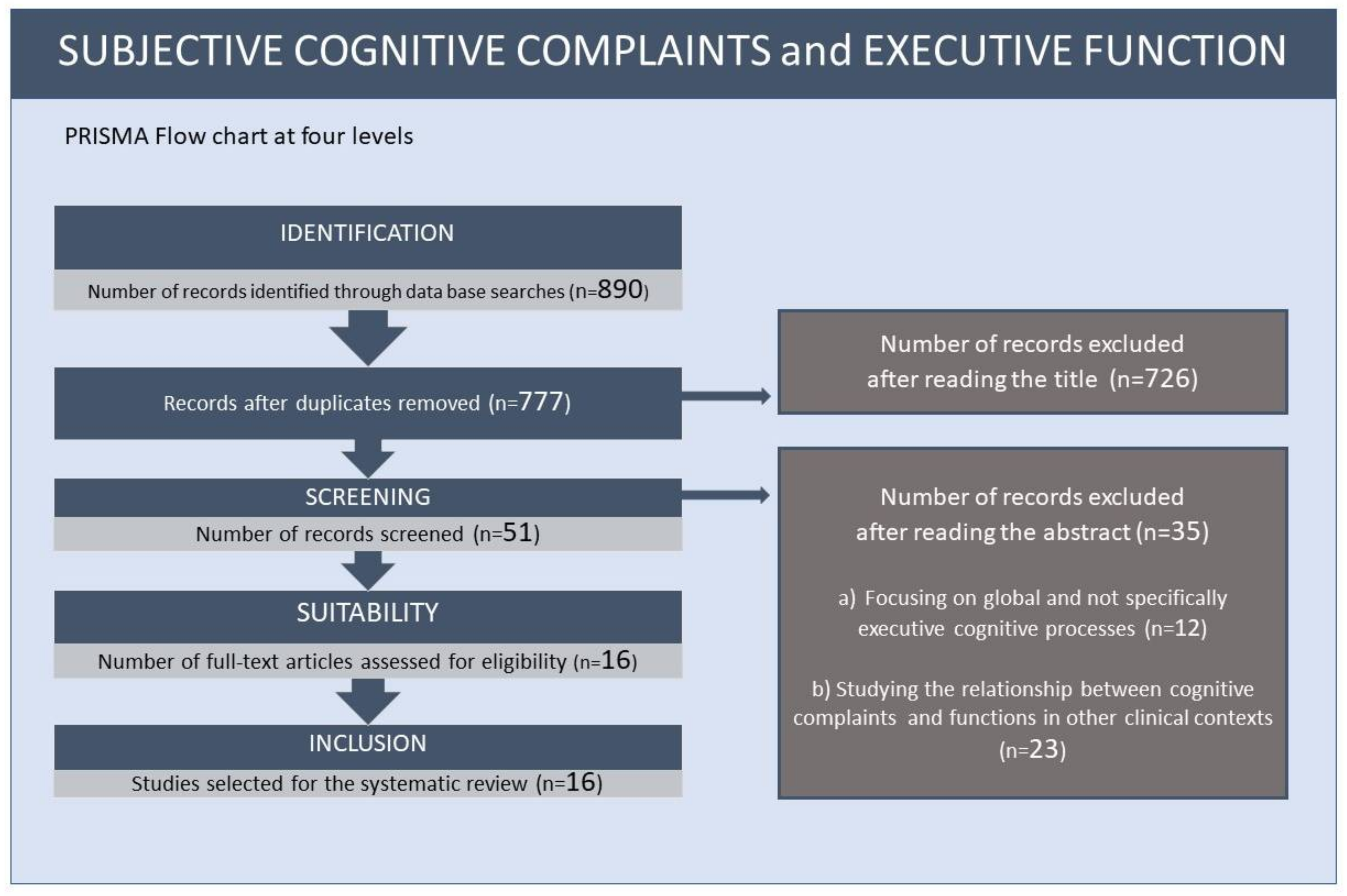
2.4. Flow Chart
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arai, H.; Ouchi, Y.; Yokode, M.; Ito, H.; Uematsu, H.; Eto, F.; Oshima, S.; Ota, K.; Saito, Y.; Sasaki, H.; et al. Members of Subcommittee for Aging. Toward the realization of a better aged society: Messages from gerontology and geriatrics. Geriatr. Gerontol. Int. 2012, 12, 16–22. [Google Scholar] [CrossRef]
- Marquet, M.; Missotten, P.; Adam, S. Ageism and overestimation of cognitive difficulties in older people: A review. Geriatr. Psychol. Neuropsychiatr. Vieil. 2016, 14, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Mazerolle, M.; Régner, I.; Morisset, P.; Rigalleau, F.; Huguet, P. Stereotype threat strengthens automatic recall and undermines controlled processes in older adults. Psychol. Sci. 2012, 23, 723–727. [Google Scholar] [CrossRef] [PubMed]
- Barber, S.J.; Lee, S.R. Stereotype Threat Lowers Older Adults’ Self-Reported Hearing Abilities. Gerontology 2015, 62, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Masse, M.; Meire, P. Is ageism a relevant concept for health care practice in the elderly? Geriatr. Psychol. Neuropsychiatr. Vieil. 2012, 10, 333–341. [Google Scholar] [CrossRef]
- Barber, S.J. An Examination of Age-Based Stereotype Threat about Cognitive Decline. Perspect. Psychol. Sci. 2017, 12, 62–90. [Google Scholar] [CrossRef]
- Marquet, M.; Missotten, P.; Dardenne, B.; Adam, S. Interactions between stereotype threat, subjective aging, and memory in older adults. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2019, 26, 121–143. [Google Scholar] [CrossRef]
- Smith, A.M.; Gallo, D.A.; Barber, S.J.; Maddox, K.B.; Thomas, A.K. Stereotypes, Warnings, and Identity-Related Variables Influence Older Adults’ Susceptibility to Associative False Memory Errors. Gerontologist 2017, 57 (Suppl. S2), S206–S215. [Google Scholar] [CrossRef]
- Armstrong, B.; Gallant, S.N.; Li, L.; Patel, K.; Wong, B.I. Stereotype Threat Effects on Older Adults’ Episodic and Working Memory: A Meta-Analysis. Gerontologist 2017, 57 (Suppl. S2), S193–S205. [Google Scholar] [CrossRef]
- Thomas, A.K.; Smith, A.M.; Mazerolle, M. The Unexpected Relationship between Retrieval Demands and Memory Performance When Older Adults Are Faced with Age-Related Stereotypes. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, 241–250. [Google Scholar] [CrossRef]
- Wurm, S.; Diehl, M.; Kornadt, A.E.; Westerhof, G.J.; Wahl, H.W. How do views on aging affect health outcomes in adulthood and late life? Explanations for an established connection. Dev. Rev. 2017, 46, 27–43. [Google Scholar] [CrossRef]
- Sindi, S.; Juster, R.P.; Wan, N.; Nair, N.P.; Ying Kin, N.; Lupien, S.J. Depressive symptoms, cortisol, and cognition during human aging: The role of negative aging perceptions. Stress 2012, 15, 130–137. [Google Scholar] [CrossRef]
- Weiss, D. On the Inevitability of Aging: Essentialist Beliefs Moderate the Impact of Negative Age Stereotypes on Older Adults’ Memory Performance and Physiological Reactivity. J. Gerontol. B Psychol. Sci. Soc. Sci. 2018, 73, 925–933. [Google Scholar] [CrossRef]
- Mazerolle, M.; Régner, I.; Barber, S.J.; Paccalin, M.; Miazola, A.C.; Huguet, P.; Rigalleau, F. Negative Aging Stereotypes Impair Performance on Brief Cognitive Tests Used to Screen for Predementia. J. Gerontol. B Psychol. Sci. Soc. Sci. 2017, 72, 932–936. [Google Scholar] [CrossRef]
- Jessen, F.; Amariglio, R.E.; van Boxtel, M.; Breteler, M.; Ceccaldi, M.; Chételat, G.; Wagner, M. A conceptual frame work for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimer’s Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef]
- Gallassi, R.; Oppi, F.; Poda, R.; Scortichini, S.; Stanzani Maserati, M.; Marano, G.; Sambati, L. Are subjective cognitive complaints a risk factor for dementia? Neurol. Sci. 2010, 31, 327–336. [Google Scholar] [CrossRef]
- Perrote, M.; Brochero, N.; Concari, I.; García, I.; Assante, M.; Lucero, C. Association between subjective memory loss, mild cognitive impairment and dementia. Neurol. Argent. 2017, 9, 156–162. [Google Scholar] [CrossRef]
- Brailean, A.; Steptoe, A.; Batty, G.D.; Zaninotto, P.; Llewellyn, D.J. Are subjective memory complaints indicative of objective cognitive decline or depressive symptoms? Findings from the English Longitudinal Study of Ageing. J. Psychiatr. Res. 2019, 110, 143–151. [Google Scholar] [CrossRef]
- Mias, C.; Causse, B. Subjective complaints of memory, objective performance and related neuropsychological functions. A systematic review. Perspect. Metodol. 2021, 21, 376–393. [Google Scholar]
- Ruiz-Sánchez de León, J.M.; Llanero-Luque, M.; Lozoya-Delgado, P.; Fernández-Blázquez, M.A.; Pedrero-Pérez, E.J. Neuropsychological study of young adults with subjective memory complaints: Involvement of executive functions and other associated symptoms. Rev. Neurol. 2010, 51, 650–660. [Google Scholar]
- Carrillo-Mora, P.; García-Juárez, B.; Lugo-Rodríguez, Y.; Moreno-Méndez, E.; Cruz-Alcalá, L. Subjective memory complaints in geriatric population and their associated factors: A pilot study in Mexican population. Rev. Mex. Neurocienc. 2017, 18, 20–31. Available online: https://www.medigraphic.com/pdfs/revmexneu/rmn-2017/rmn176b.pdf (accessed on 7 January 2022).
- Montejo-Carrasco, P.; Claver-Martín, M.; Montenegro-Peña, M.; Álvarez-Crespo, B.; Montejo-Rubio, B. Association of quality of life with episodic memory performance. Study in older people without cognitive impairment. Psicogeriatría 2016, 6, 69–80. [Google Scholar]
- Pellicer-Porcar, O.; Mirete-Fructuoso, M.; Molina-Rodríguez, S.; Soto-Amaya, J. Subjective memory complaints in young adults: Influence of emotional state. Rev. Neurol. 2014, 59, 543–550. [Google Scholar]
- Miskowiak, K.W.; Johnsen, S.; Sattler, S.M.; Nielsen, S.; Kunalan, K.; Rungby, J.; Lapperre, T.; Porsberg, C.M. Cognitive impairments four months after COVID-19 hospital discharge: Pattern, severity and association with illness variables. Eur. Neuropsychopharmacol. 2021, 46, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Torres, A.; Giménez-Llort, L. Confinement and the Hatred of Sound in Times of COVID-19: A Molotov Cocktail for People With Misophonia. Front. Psychiatry 2021, 12, 627044. [Google Scholar] [CrossRef] [PubMed]
- Slavin, M.; Sachdev, P.; Kochan, N.; Woolf, C.; Crawford, J.; Giskes, K.; Reppermund, S.; Trollor, J.; Draper, B.; Delbaere, K.; et al. Predicting Cognitive, Functional, and Diagnostic Change over 4 Years Using Baseline Subjective Cognitive Complaints in the Sydney Memory and Ageing Study. Am. J. Geriatr. Psychiatry 2015, 23, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Orueta, U.; Blanco-Campal, A.; Burke, T. Process-based neuropsychological evaluation: Review of the evidence and proposal for the improvement of dementia screening tools. Rev. Neurol. 2017, 64, 514–524. [Google Scholar]
- Barandiaran, M. Neuropsychology and early diagnosis. Rev. Esp. Geriatr. Gerontol. 2019, 46, 42–46. [Google Scholar] [CrossRef]
- Garcia-Ptacek, S.; Eriksdotter, M.; Jelic, V.; Porta-Etessam, V.; Kåreholt, I.; y Manzano, S. Subjective cognitive impairment: Towards early identification of Alzheimer disease. Neurology 2016, 31, 562–571. [Google Scholar] [CrossRef]
- Rolstad, S.; Berg, A.I.; Bjerke, M.; Blennow, K.; Johansson, B.; Zetterberg, H.; Wallin, H. Amyloid-beta42 is associated with cognitive impairment in healthy elderly and subjective cognitive impairment. J. Alzheimer’s Dis. 2011, 26, 135–142. [Google Scholar] [CrossRef]
- Saykin, A.J.; Wishart, H.A.; Rabin, L.A.; Santulli, R.B.; Flashman, L.A.; West, J.D.; McHugh, T.L.; Mamourian, A. Older adults with cognitive complaints show brain atrophy similar to that of amnestic mci. Neurology 2006, 67, 834–842. [Google Scholar] [CrossRef]
- Urrutia, G.; Bonfill, X. La declaración PRISMA: Un paso adelante en la mejora de las publicaciones de la Revista Española de Salud Pública. Rev. Esp. Salud. Publica 2013, 87, 99–102. [Google Scholar] [CrossRef]
- Rapp, M.A.; Reischies, F.M. Attention and executive control predict Alzheimer disease in late life: Results from the Berlin Aging Study (BASE). Am. J. Geriatr. Psychiatry 2005, 13, 134–141. [Google Scholar] [CrossRef]
- Rabin, L.; Roth, R.; Isquith, P.; Wishart, H.; Nutter-Upham, K.; Pare, N.; Flashman, L.; Saykin, A. Self- and informant reports of executive function on the BRIEF-A in MCI and older adults with cognitive complaints. Arch. Clin. Neuropsychol. 2006, 21, 721–732. [Google Scholar] [CrossRef]
- Grober, E.; Hall, C.B.; Lipton, R.B.; Zonderman, A.B.; Resnick, S.M.; Kawas, C. Memory impairment, executive dysfunction, and intellectual decline in preclinical Alzheimer’s disease. J. Int. Neuropsychol. Soc. 2008, 14, 266–278. [Google Scholar] [CrossRef]
- Saunders, N.L.; Summers, M.J. Attention and working memory deficits in mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2010, 32, 350–357. [Google Scholar] [CrossRef]
- Van Harten, A.C.; Smits, L.L.; Teunissen, C.E.; Visser, P.J.; Koene, T.; Blankenstein, M.A.; Scheltens, P.; van der Flier, W.M. Preclinical AD predicts decline in memory and executive functions in subjective complaints. Neurology 2013, 81, 1409–1416. [Google Scholar] [CrossRef]
- Toledo, J.B.; Bjerke, M.; Chen, K.; Rozycki, M.; Jack, C.R.; Weiner, M.W.; Arnold, S.E.; Reiman, E.M.; Davatzikos, C.; Shaw, L.M.; et al. Memory, executive, and multidomain subtle cognitive impairment. Neurology 2015, 85, 144–153. [Google Scholar] [CrossRef]
- Seo, E.H.; Kim, H.; Lee, K.H.; Choo, I.H. Altered Executive Function in Pre-Mild Cognitive Impairment. J. Alzheimer’s Dis. 2016, 54, 933–940. [Google Scholar] [CrossRef]
- Verfaillie, S.C.; Slot, R.E.; Tijms, B.; Bouwman, F.H.; Benedictus, M.; Overbeek, J.; Koene, T.; Vrenken, H.; Scheltens, P.; Barkhof, F.; et al. Thinner cortical thickness in patients with subjective cognitive decline is related to poor memory performance and faster decline of executive function. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2016, 12, 113–114. [Google Scholar] [CrossRef]
- Fogarty, J.; Almklov, E.; Borrie, M.; Wells, J.; Roth, R.M. Subjective rating of executive functions in mild Alzheimer’s disease. Aging Ment. Health 2017, 21, 1184–1191. [Google Scholar] [CrossRef]
- Bae, J.; Kim, W.; Kim, B.; Chang, S.; Lee, D.; Cho, M. Associations between subjective memory complaints and executive functions in a community sample of elderly without cognitive dysfunction. Alzheimer’s Dement. 2017, 13, 1183. [Google Scholar] [CrossRef]
- Viviano, R.P.; Hayes, J.M.; Pruitt, P.J.; Fernandez, Z.J.; van Rooden, S.; van der Grond, J.; Rombouts, S.; Damoiseaux, J.S. Aberrant memory system connectivity and working memory performance in subjective cognitive decline. Neuroimage 2019, 15, 556–564. [Google Scholar] [CrossRef]
- Valech, N.; Tort-Merino, A.; Coll-Padrós, N.; Olives, J.; León, M.; Rami, L.; Molinuevo, J.L. Executive and Language Subjective Cognitive Decline Complaints Discriminate Preclinical Alzheimer’s Disease from Normal Aging. J. Alzheimer’s Dis. 2018, 61, 689–703. [Google Scholar] [CrossRef]
- Pérez-Cordón, A.; Monté-Rubio, G.; Sanabria, A.; Rodriguez-Gomez, O.; Valero, S.; Abdelnour, C.; Marquié, M.; Espinosa, A.; Ortega, G.; Hernandez, I.; et al. Subtle executive deficits are associated with higher brain amyloid burden and lower cortical volume in subjective cognitive decline: The FACEHBI cohort. Sci. Rep. 2020, 10, 17721. [Google Scholar] [CrossRef]
- Kim, W.H.; Kim, B.S.; Chang, S.M.; Lee, D.W.; Bae, J.N. Relationship between subjective memory complaint and executive function in a community sample of South Korean elderly. Psychogeriatrics 2020, 20, 850–857. [Google Scholar] [CrossRef]
- Esmaeili, M.; Nejati, V.; Shati, M.; Vatan, R.F.; Chehrehnegar, N.; Foroughan, M. Attentional network changes in subjective cognitive decline. Aging Clin. Exp. Res. 2021, 1–9. [Google Scholar] [CrossRef]
- Garrido-Chaves, R.; Perez, V.; Perez-Alarcón, M.; Crespo-Sanmiguel, I.; Paiva, T.O.; Hidalgo, V.; Pulopulos, M.M.; Salvador, A. Subjective MemoryComplaints and Decision Making in Young and Older Adults: An Event-Related Potential Study. Front. Aging Neurosci. 2021, 13, 695275. [Google Scholar] [CrossRef]
- Wasef, S.; Laksono, I.; Kapoor, P.; Tang-Wei, D.; Gold, D.; Saripella, A.; Riazi, S.; Islam, S.; Englesakis, M.; Wong, J.; et al. Screening for subjective cognitive decline in the elderly via subjective cognitive complaints and informant-reported questionnaires: A systematic review. BMC Anesthesiol. 2021, 21, 277. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.H.; Park, S.; Jang, H.; Cho, S.H.; Kim, S.J.; Kim, J.P.; Kim, S.T.; Na, D.L.; Seo, S.W.; Kim, H.J. Frontal-executive dysfunction affects dementia conversion in patients with amnestic mild cognitive impairment. Sci. Rep. 2020, 10, 772. [Google Scholar] [CrossRef] [PubMed]
- Hoogenhout, E.M.; de Groot, R.H.; van der Elst, W.; Jolles, J. Effects of a comprehensive educational group intervention in older women with cognitive complaints: A randomized controlled trial. Aging Ment. Health 2012, 16, 135–144. [Google Scholar] [CrossRef][Green Version]
- Almkvist, O.; Bosnes, O.; Bosnes, I.; Stordal, E. Subjective working and declarative memory in dementia and normal aging. Acta Neurol. Scand. 2019, 140, 140–146. [Google Scholar] [CrossRef]
- Giovanello, K.S.; Verfaille, M. Memory systems of the brain: A cognitive neuropsychological analysis. Semin. Speech Lang. 2001, 22, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Grady, C. The cognitive neuroscience of aging. Nat. Rev. Neurosci. 2012, 13, 491–505. [Google Scholar] [CrossRef]
- Rabin, L.A.; Chi, S.Y.; Wang, C.; Fogel, J.; Kann, S.J.; Aronov, A. Prospective memory on a novel clinical task in older adults with mild cognitive impairment and subjective cognitive decline. Neuropsychol. Rehabil. Int. J. 2014, 24, 868–893. [Google Scholar] [CrossRef]
- Lee, S.D.; Ong, B.; Pike, K.E.; Kinsella, G.J. Prospective memory and subjective memory decline: A neuropsychological indicator of memory difficulties in community-dwelling older people. J. Clin. Exp. Neuropsychol. 2018, 40, 183–197. [Google Scholar] [CrossRef]
- Amanzio, M.; Bartoli, B.; Cipriani, G.E.; Palermo, S. Executive Dysfunction and Reduced Self-Awareness in Patients with Neurological Disorders. A Mini-Review. Front. Psychol. 2020, 11, 1697. [Google Scholar] [CrossRef]
- Vaskivuo, L.; Hokkanen, L.; Hänninen, T.; Antikainen, R.; Bäckman, L.; Laatikainen, T.; Paajanen, T.; Stigsdotter-Neely, A.; Strandberg, T.; Tuomilehto, J.; et al. Self and Informant Memory Reports in FINGER: Associations with Two-Year Cognitive Change. J. Alzheimer’s Dis. 2019, 71, 785–795. [Google Scholar] [CrossRef]
- De Almeida, M.L.; Dalpubel, D.; Ribeiro, E.B.; de Oliveira, E.S.B.; Ansai, J.H.; Vale, F.A.C. Subjective cognitive impairment, cognitive disorders and self-perceived health: The importance of the informant. Dement. Neuropsychol. 2019, 13, 335–342. [Google Scholar] [CrossRef]
- Baquero, M.; Martin, N. Depressive symptoms in neurodegenerative diseases. World J. Clin. Cases 2015, 3, 682–693. [Google Scholar] [CrossRef]
- Sánchez-Negrete, M.G.; Igol, P.; Mandich, V.C.; Lascar, M. Ansiedad, depresión y quejas cognitivas. In VIII Congreso Internacional de Investigación y Práctica Profesional en Psicología XXIII Jornadas de Investigación XII Encuentro de Investigadores en Psicología del MERCOSUR; Facultad de Psicología—Universidad de Buenos Aires: Buenos Aires, Argentina, 2016. [Google Scholar]
- Pedrero-Pérez, E.J.; Ruiz-Sánchez de León, J.M. Subjective complaints of memory, personality and prefrontal symptoms in young adults. Rev. Neurol. 2013, 57, 289–296. [Google Scholar] [PubMed]
- Lubitz, A.F.; Eid, M.; Niedeggen, M. Complainer Profile Identification (CPI): Properties of a new questionnaire on subjective cognitive complaints. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2018, 25, 99–121. [Google Scholar] [CrossRef] [PubMed]
- Baggio, G.; Corsini, A.; Floreani, A.; Giannini, S.; Zagonel, V. Gender medicine: A task for the third millennium. Clin. Chem. Lab. Med. 2013, 51, 713–727. [Google Scholar] [CrossRef]
- Giménez-Llort, L. The Moon Effect: Individual and Social Impact of Aging in Men and Women on the Third Millennium. In Proceedings of the 19th IPA International Congress, Santiago de Compostela, Spain, 31 August–3 September 2019. [Google Scholar] [CrossRef]
- Wang, L.; Tian, T. Gender Differences in Elderly with Subjective Cognitive Decline. Front. Aging Neurosci. 2018, 10, 166. [Google Scholar] [CrossRef]
- Oghagbon, E.K.; Giménez-Llort, L. Short height and poor education increase the risk of dementia in Nigerian type 2 diabetic women. Alzheimer’s Dement. 2019, 11, 493–499. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Sample | Methodology | Results |
|---|---|---|---|
| Rapp and Reischies (2005) [33] | 187 participants (83 W and 84 M): 15 cases who developed AD (7 W and 8 M) Mean age: 86.17 years Mean years of education: 11.43 172 cases who did not develop AD (76 W and 76 M) Mean age: 79.08 years Mean years of education: 11.30 Country: Germany | Longitudinal study (4 years) NEUROPSYCHOLOGY MMSE, TMT part B, Digit Symbol Substitution Test, Digit Letter test, Identical Pictures | In total, 15 participants developed Alzheimer’s disease at 4 years (scoring low on all follow-up assessments). |
| Rabin et al. (2006) [34] | 87 participants (54 W and 33 M): 30 HC subjects (21 W and 9 M) Mean age: 72 years Mean years of education: 17 28 SCC subjects (20 W and 8 M) Mean age: 74 years Mean years of education: 16 29 MCI subjects (13 W and 16 M) Mean age: 74 Mean years of education: 16 Country: United States | NEUROPSYCHOLOGY MMSE, CVLT-II, DRS-2, WCST, D-KEFS, WMS-III, BRIEF-A | The participants with MCI and SCCs reported significant difficulties with selective aspects of executive functioning (working memory). In addition, it was more likely that their informants reported the same difficulties. |
| Grober et al. (2008) [35] | 92 subjects with incident AD assessed for 15 years prior to diagnosis (48 W and 44 M) Mean age: 79.8 years Mean years of education: 16.5 Country: United States, Netherlands | NEUROPSYCHOLOGY Memory (Free Recall on the Free and Cued Selective Reminding Test), executive functions (categorical fluency, letter and path fluency), and verbal intelligence (AMNART) | The decline in the cognitive performance in episodic memory tests accelerated 7 years prior to diagnosis; this was 2–3 years for executive-function performance (associated with pathological signs in the frontal circuits), while verbal-intelligence performance declined in the vicinity of diagnosis. |
| Saunders and Summers (2010) [36] | 131 subjects (68 W and 63 M): 25 HC subjects Mean age: 69 years Mean years of education: 13.5 32 subjective MCI Mean age: 71 years Mean years of education: 13 60 amnestic MCI Mean age: 71 years Mean years of education: 13.1 14 mild AD Mean age: 76 years Mean years of education: 12 Country: Australia | NEUROPSYCHOLOGY Wechsler Test of Adult Reading (WTAR); estimated full-scale intelligence quotient (FSIQ); Boston Naming Test (BNT); Rey Auditory Verbal Learning Test (RAVLT); Paired AssociateLearning (PAL). | Both the amnestic-MCI and subjective-MCI groups displayed impaired attentional processing and working-memory capacity. |
| van Harten et al. (2013) [37] | 132 participants with SCCs (56 W and 76 M) Mean age: 61.4 years Mean years of education: 6 Country: Netherlands | NEUROPSYCHOLOGY Neuropsychological assessments with 1–2 years follow-up (MMSE) CSF BIOMARKERS CSF biomarker data on β-amyloid, total tau, hyperphosphorylated tau-181 | Patients meeting preclinical AD criteria showed deterioration of memory, executive functions and global cognition over time, associated with evidence of CSF. MMSE total scores, delayed recall and initiation/perseveration subscales were significantly lower than the control group. |
| Toledo et al. (2015) [38] | 522 subjects (253 W and 269 M): 307 CN subjects (138 W and 169 M) Mean age: 73.9 years 71 subjects with SCCs (25 W and 46 M) Mean age: 71.6 years 51 subjects with executive SCI (21 W and 30 M) Mean age: 77.3 years 66 subjects with memory SCI (49 W and 17 M) Mean age: 75 years 27 subjects with multi-domain SCI (20 W and 7 M) Mean age: 78 years Country: United States | CSF BIOMARKERS Analysis of CSF biomarker data NEUROIMAGING Hippocampal volume measurements and MRI-SPARE-AD values Hypometabolic convergence index Posterior cingulate metabolic rate for glucose | Conversion from executive SCI to MCI/dementia of 50% at 7 years. Participants with SCCs showed atrophy of orbital prefrontal regions and higher p-tau and RM-SPARE-EA values (indicative of pathological changes). |
| Seo et al. (2016) [39] | 265 participants (178 W and 79 M): 188 CN subjects (120 W and 60 M) Mean age: 71.94 years Mean years of education: 9.69 77 subjects with pre-DCL (58 W and 19 M) Mean age: 72.64 years Mean years of education: 9.64 Country: Korea | NEUROPSYCHOLOGY MMSE; categorical and phonemic fluency tests, Stroop test, path test and TMT A–B | Significantly lower pre-DCL-group scores in visual memory and executive functions, with poor performance in inhibition and goal-directed behavior. |
| Verfaillie et al. (2016) [40] | 238 participants with SCI (109 W and 129 M) Mean age: 62 years Country: Netherlands | NEUROPSYCHOLOGY Neuropsychological assessment (MMSE) NEUROIMAGING Measurement of cortical thickness by MRI | A total of 16% of participants showed progression to MCI and AD at the 2–3 year follow-up. Reduced fronto-temporo-parietal cortical thickness associated with reduced memory performance. Reduced temporal cortical thickness was associated with decreased executive performance. |
| Fogarty et al. (2017) [41] | 55 participants (35 W and 20 M): 23 subjects with mild AD (9 W and 14 M) Mean age: 73.95 years Mean years of education: 15.56 32 adult control subjects (26 W and 6 M) Mean age: 69.84 years Mean years of education: 13.96 Country: England | NEUROPSYCHOLOGY Application of the BRIEF-A to participants and informants (spouse/child) | Participants with mild AD and their informants reported greater difficulties in most of the clinical scales assessed. |
| Bae et al. (2017) [42] | 1442 participants 1088 HC subjects 354 with SCCs Country: South Korea | NEUROPSYCHOLOGY MMSE, initiation/perseveration (IP), Subscale of the Korean version of Mattis Dementia Rating Scale (K-DRS) | Participants with SCCs performed worse on all cognitive tests that evaluated memory and executive functions. |
| Viviano et al. (2018) [43] | 83 participants (51 W and 32 M): 35 adults with SCI (22 W and 13 M) Mean age: 68.5 years 48 adults without SCI (29 W and 19 M) Mean age: 67.08 years Country: United States, Netherlands | NEUROPSYCHOLOGY MMSE and Weschler Memory Scale, Geriatric Depression Scale, Beck Depression Inventory II and Big Five Inventory NEUROIMAGING Assessment of functional connectivity of brain regions using MRI and diffusion of regions | Patients and informants were more likely to report executive problems in working memory, planning/organising and monitoring. Subjective cognitive impairment was associated with lower functional connectivity in retrosplenial–precuneus regions and memory-system regions (poorer performance in visual working memory). |
| Valech et al. (2018) [44] | 68 normal subjects (46 W and 22 M): 52 HC (33 W and 19 M) Mean age: 63.87 years Mean years of education: 11.96 16 pre-AD (13 W and 3 M) Mean age: 66.5 years Mean years of education: 9.56 Country: Spain | Neuropsychological follow-up for 1 year NEUROPSYCHOLOGY Subjective Cognitive Complaints Questionnaire (SCI-Q) MMSE, Memory Alteration Test, Boston Naming Test, comprehension of commands (BDAE), incomplete letters and number location (VOSP), TMT-A, phonetic fluencies (FAS), Free and Cued Selective Reminding Test (FHCRT-IR), semantic fluency test (animals), Stroop test Hospital Anxiety and Depression Scale | Pre-AD subjects showed significantly higher scores with respect to language, attention and executive decline, confirmed by their informants. Significantly decreased cognitive performance in pre-AD on tests of inhibition and semantic fluency. |
| Pérez et al. (2020) [45] | 195 participants with SCD (121 W and 74 M) Mean age: 65.71 years Mean years of education: 14.94 Country: Spain | NEUROPSYCHOLOGY TMT A-B, rule shift card subtest (BADS), automatic inhibition subtest (AI-SKT), digits (WAIS-III), letter, semantic and verbal fluency tests NEUROIMAGING Functional neuroimaging studies (positron emission tomography with 18F-Florbetaben and MRI) Analysis of gray matter volume | Significant association between β-amyloid deposition and low executive performance in automatic inhibition (AI-SKT). Low executive performance was associated with lower volume in bilateral hippocampal and left frontal regions. |
| Kim et al. (2020) [46] | 1442 participants (886 W and 556 M) (age: ≥65 years): 1088 HC subjects (642 W and 446 M) Mean years of education: 5.66 354 SCC subjects (244 W and 110 M) Mean years of education: 3.33 Country: Korea | NEUROPSYCHOLOGY Mini-Mental State Examination, Korean version (MMSE-KC)—use of the recording and retrieval subscales for memory assessment and the initiation/perseveration subscales (Korean rating scale K-DRS) to assess executive functions | Significant relationship between depression and SCCs. Lower performance in global cognition, memory and executive functions (verbal fluency) in the study group. |
| Esmaeili et al. (2021) [47] | 62 subjects: 17 SCC subjects 30 amnestic-MCI subjects 15 HC subjects Country: Iran | NEUROPSYCHOLOGY Attention Network Test (ANT) | The older SCC subjects faced problems in maintaining alertness to external stimuli (attention-processing problems). |
| Garrido et al. (2021) [48] | 136 subjects (67 W and 59 M): 28 young adults with SCCs (17 W and 11 M) Mean age: 21 years 37 young adults without SCCs (16 W and 11 M) Mean age: 23 years 32 older adults with SCCs (18 W and 14 M) Mean age: 63 years 39 older adults without SCCs (16 W and 23 M) Mean age: 65 years Country: Spain | NEUROPSYCHOLOGY Iowa gambling task (IGT) NEUROLOGY Electroencephalogram (EEG) Feedback-related negativity (FRN) | The older adults with SCCs presented deficits in the decision-making process. These data were also observed in the neuronal mechanisms studied. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Webster-Cordero, F.; Giménez-Llort, L. The Challenge of Subjective Cognitive Complaints and Executive Functions in Middle-Aged Adults as a Preclinical Stage of Dementia: A Systematic Review. Geriatrics 2022, 7, 30. https://doi.org/10.3390/geriatrics7020030
Webster-Cordero F, Giménez-Llort L. The Challenge of Subjective Cognitive Complaints and Executive Functions in Middle-Aged Adults as a Preclinical Stage of Dementia: A Systematic Review. Geriatrics. 2022; 7(2):30. https://doi.org/10.3390/geriatrics7020030
Chicago/Turabian StyleWebster-Cordero, Felipe, and Lydia Giménez-Llort. 2022. "The Challenge of Subjective Cognitive Complaints and Executive Functions in Middle-Aged Adults as a Preclinical Stage of Dementia: A Systematic Review" Geriatrics 7, no. 2: 30. https://doi.org/10.3390/geriatrics7020030
APA StyleWebster-Cordero, F., & Giménez-Llort, L. (2022). The Challenge of Subjective Cognitive Complaints and Executive Functions in Middle-Aged Adults as a Preclinical Stage of Dementia: A Systematic Review. Geriatrics, 7(2), 30. https://doi.org/10.3390/geriatrics7020030