
Program of All-Inclusive Care for the Elderly (PACE) versus Other Programs: A Scoping Review of Health Outcomes



Abstract
1. Introduction
2. Methods
2.1. Identifying the Initial Research Question
2.2. Identifying Relevant Studies
2.3. Study Selection
2.4. Data Charting and Collation
2.5. Summarizing and Reporting Findings
2.6. Risk of Bias Assessment
3. Results
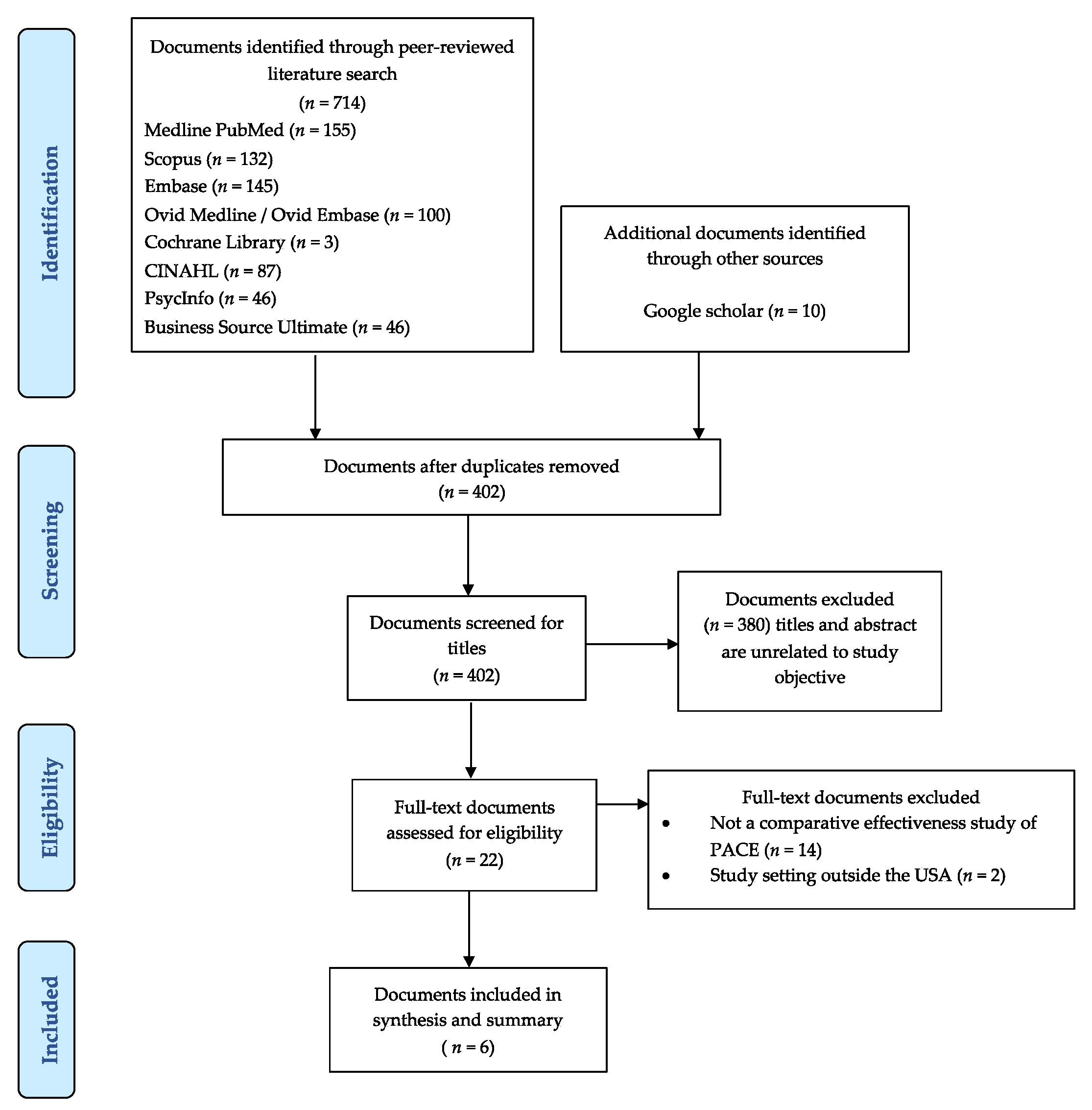
3.1. Identified Studies
3.2. Characteristics of Studies
3.3. Description of Programs Included in the Review
3.4. Study Outcomes
3.5. ADL, IADL, and Unmet Need Outcomes
3.6. Healthcare Resource Use Outcomes
3.7. Clinical and Survival Outcomes
3.8. Economic Outcomes
3.9. Risk of Bias in Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Older People Projected to Outnumber Children for First Time in U.S. History. Available online: https://www.census.gov/newsroom/press-releases/2018/cb18-41-population-projections.html (accessed on 19 January 2022).
- Let’s Work Together to Improve Care for Older Adults with Complex Needs. Available online: https://www.healthaffairs.org/do/10.1377/hblog20170214.058749/full/ (accessed on 19 January 2022).
- How High-Need Patients Experience Health Care in the United States. Available online: https://www.commonwealthfund.org/sites/default/files/documents/___media_files_publications_issue_brief_2016_dec_1919_ryan_high_need_patient_experience_hnhc_survey_ib_v2.pdf (accessed on 19 January 2022).
- A Summary of the 2021 Annual Reports. Available online: www.ssa.gov/oact/TRSUM/ (accessed on 19 January 2022).
- Medicaid.gov. Program of All-Inclusive Care for the Elderly. Available online: https://www.medicaid.gov/medicaid/long-term-services-supports/program-all-inclusive-care-elderly/index.html (accessed on 19 January 2022).
- Wieland, D.; Kinosian, B.; Stallard, E.; Boland, R. Does Medicaid pay more to a program of all-inclusive care for the elderly (PACE) than for fee-for-service long-term care? J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Kozma, C.M.; Reeder, C.E.; Schulz, R.M. Economic, clinical, and humanistic outcomes: A planning model for pharmacoeconomic research. Clin. Ther. 1993, 15, 1121–1132. [Google Scholar] [PubMed]
- Centers for Medicare & Medicaid Services. Program of All-Inclusive Care for the Elderly. Introduction to PACE. Available online: https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/pace111c01.pdf (accessed on 19 January 2022).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bas in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Nadash, P. Two models of managed long-term care: Comparing PACE with a Medicaid-only plan. Gerontologist 2004, 44, 644–654. [Google Scholar] [CrossRef][Green Version]
- Nadash, P. Comparing PACE with a Medicaid-only managed long-term care plan: Health outcomes over time. World Med. Health Policy 2013, 5, 201–216. [Google Scholar] [CrossRef]
- Kane, R.L.; Homyak, P.; Bershadsky, B. Consumer reactions to the Wisconsin Partnership Program and its parent, the Program for All-Inclusive Care of the Elderly (PACE). Gerontologist 2002, 42, 314–320. [Google Scholar] [CrossRef][Green Version]
- Weaver, F.M.; Hickey, E.C.; Hughes, S.L.; Parker, V.; Fortunato, D.; Rose, J.; Cohen, S.; Robbins, L.; Orr, W.; Priefer, B.; et al. Providing all-inclusive care for frail elderly veterans: Evaluation of three models of care. J. Am. Geriatr. Soc. 2008, 56, 345–353. [Google Scholar] [CrossRef]
- Wieland, D.; Boland, R.; Baskins, J.; Kinosian, B. Five-year survival in a program of all-inclusive care for elderly compared with alternative institutional and home-and community-based care. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 721–726. [Google Scholar] [CrossRef]
- Katz, S.; Akpom, C.A. A measure of primary sociobiological functions. Int. J. Health Serv. 1976, 6, 493–508. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Millán-Calenti, J.C.; Tubío, J.; Pita-Fernández, S.; Gonzalez-Abraldes, I.; Lorenzo, T.; Fernandez-Arruty, T.; Maseda, A. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch. Gerontol. Geriatr. 2010, 50, 306–310. [Google Scholar] [CrossRef]
- Norström, T.; Thorslund, M. The structure of IADL and ADL measures: Some findings from a Swedish study. Age Ageing 1991, 20, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Freedman, V.A.; Martin, L.G.; Schoeni, R.F. Recent trends in disability and functioning among older adults in the United States: A systematic review. JAMA 2002, 288, 3137–3146. [Google Scholar] [CrossRef] [PubMed]
- Depalma, G.; Xu, H.; Covinsky, K.E.; Craig, B.A.; Stallard, E.; Thomas, J.; Sands, L.P. Hospital readmission among older adults who return home with unmet need for ADL disability. Gerontologist 2013, 53, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Kelley, A.S.; Ettner, S.L.; Morrison, R.S.; Du, Q.; Sarkisian, C.A. Disability and decline in physical function associated with hospital use at end of life. J. Gen. Intern. Med. 2012, 27, 794–800. [Google Scholar] [CrossRef]
- The Impact of PACE on Participant Outcomes. Available online: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Reports/Downloads/Chatterji_1998_6.pdf (accessed on 19 January 2022).
- Segelman, M.; Szydlowski, J.; Kinosian, B.; McNabney, M.; Raziano, D.B.; Eng, C.; van Reenen, C.; Temkin-Greener, H. Hospitalizations in the Program of All-Inclusive Care for the Elderly. J. Am. Geriatr. Soc. 2014, 62, 320–324. [Google Scholar] [CrossRef]
- Friedman, S.M.; Steinwachs, D.M.; Rathouz, P.J.; Burton, L.C.; Mukamel, D.B. Characteristics predicting nursing home admission in the program of all-inclusive care for elderly people. Gerontologist 2005, 45, 157–166. [Google Scholar] [CrossRef]
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and fall injuries among adults aged ≥65 years—United States, 2014. MMWR Morb Mortal Wkly Rep. 2016, 65, 993–998. [Google Scholar] [CrossRef]
- Cheng, X.; Wu, Y.; Yao, J.; Schwebel, D.C.; Hu, G. Mortality from unspecified unintentional injury among individuals aged 65 years and older by US state, 1999-2013. Int. J. Environ. Res. Public Health 2016, 13, 763. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.J.; Lui, L.; Eng, C.; Jha, A.K.; Covinsky, K.E. Differences in mortality of black and white patients enrolled in the program of all-inclusive care for the elderly. J. Am. Geriatr. Soc. 2003, 51, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Beach, S.R.; Ives, D.G.; Martire, L.M.; Ariyo, A.A.; Kop, W.J. Association between depression and mortality in older adults: The cardiovascular health study. Arch. Intern. Med. 2000, 160, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- Effect of PACE on Costs, Nursing Home Admissions, and Mortality: 2006–2011. Available online: https://aspe.hhs.gov/reports/effect-pace-costs-nursing-home-admissions-mortality-2006-2011-0 (accessed on 19 January 2022).
- Petigara, T.; Anderson, G. Program of All-Inclusive Care for the Elderly. Health Policy Monitor. 2009. Available online: https://www.npaonline.org/sites/default/files/PDFs/Health%2520Policy%2520Monitor%2520-%25202009.pdf (accessed on 19 January 2022).
- Meret-Hanke, L.A. Effects of the Program of All-inclusive Care for the Elderly on hospital use. Gerontologist 2011, 51, 774–785. [Google Scholar] [CrossRef]
- The Effects of PACE on Medicare and Medicaid Expenditures. Available online: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Reports/downloads/Foster_PACE_2009.pdf (accessed on 19 January 2022).
- Evaluation of the Program of All-Inclusive Care for the Elderly: A Comparison of the PACE Capitation Rates to Projected Costs in the First Year of Enrollment. Available online: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Reports/Downloads/White_2000_6.pdf (accessed on 19 January 2022).
- PACE: An Evaluation. Available online: https://www.dshs.wa.gov/sites/default/files/rda/reports/research-8-26.pdf (accessed on 19 January 2022).
- White, A.J. The Effect of PACE on Costs to Medicare: A Comparison of Medicare Capitation Rates to Projected Costs in the Absence of PACE; Report Prepared for HCFA; Abt Associates Incorporated: London, UK, 1998. [Google Scholar]


{kind=link}
| Study Authors, Year | Study Design | Study Duration (Days) | PACE (N) | Comparison (N) | Comparison | PACE Patient Age Years, Mean ± SD or % | PACE Female (%) | Comparison Patient Age Years, Mean ± SD or % | Comparison Female (%) |
|---|---|---|---|---|---|---|---|---|---|
| Kane et al., 2002 | Cross sectional | 730 | 322 | 304 | Wisconsin Partnership Program (WPP) | 80 ± NR | 82.0 | 77 ± NR | 74.0 |
| Nadash, 2004 | Retrospective Cohort | 365 | 1382 | 1267 | Medicaid-only-managed long-term care | 79± NR | 71.5 | 79 ± NR | 72.5 |
| Nadash, 2013 | Retrospective Cohort | 540 | 1535 | 1540 | VNS CHOICE program (VCP) | ≥65 ± NR | 71.5 | ≥65 ± NR | 72.9 |
| Weaver et al., 2008 | Prospective Cohort | 1095 | 85 | 181 | VA as a sole provider | 76 (range; 56.1–93.2) | 1.0 | 75 (range; 55.6–101.3) | 4.0 |
| 102 | VA & PACE partnership with PACE | 77 (range; 55.2–94.6) | 6.0 | ||||||
| Wieland et al., 2010 | Prospective Cohort | 1825 | 554 | 468 | Nursing Home | 77.2 ± 0.42 | 65.9 | 74.8 ± 0.51 | 63.3 |
| 1018 | Aged and disabled waiver program | 74.5 ± 0.32 | 75.5 | ||||||
| Wieland et al., 2013 | Retrospective Cohort | 4015 | 948 | 1357 | Nursing Home | 55–64 (10.6%) 65–74 (27.0%) 75–84 (38.6%) ≥85 (23.8%) | 75.2 | 55–64 (18.7%) 65–74 (20.3%) 75–84 (38.3%) ≥85 (22.7%) | 63.1 |
| 1683 | Aged and disabled waiver program | 55–64 (18.8%) 65–74 (27.6%) 75–84 (34.6%) ≥85 (19.0%) | 76.4 |
| Study Authors, Year | Outcomes | PACE | Comparison 1 | p |
|---|---|---|---|---|
| Kane et al., 2002 | PACE (%) | WPP (%) | ||
| Needs a little help or more with ADLs | ||||
| Bathing | 64 | 44 | 0.000 | |
| Dressing | 47 | 29 | 0.000 | |
| Toileting | 32 | 15 | 0.000 | |
| Transferring | 28 | 17 | 0.002 | |
| Feeding | 15 | 5 | 0.000 | |
| Able to walk between rooms | 79 | 84 | ns | |
| Difficulty with IADLs | ||||
| Shopping | 74 | 63 | 0.003 | |
| Using phone | 38 | 28 | 0.014 | |
| Doing light housework | 67 | 53 | 0.000 | |
| Preparing meals | 75 | 59 | 0.000 | |
| Using transportation | 42 | 35 | ns | |
| Taking medications | 26 | 16 | 0.002 | |
| Managing finances | 75 | 53 | 0.000 | |
| Arranging services | 73 | 54 | 0.000 | |
| Unmet Needs, % (patients with unmet needs/patients with dependency | ||||
| Need help with bathing and did not receive | 8 | 9 | ns | |
| Not able to bathe | 15 | 15 | ns | |
| Need help with dressing and did not receive | 9 | 16 | ns | |
| Unable to put on clean clothes | 5 | 10 | ns | |
| Need help with toileting and did not receive | 27 | 10 | ns | |
| Wet or soiled because no help available | 54 | 30 | ns | |
| Had to wait 20 min or more wet/soiled | 18 | 19 | ns | |
| Need help transferring and did not receive | 11 | 17 | ns | |
| Fell because no help | 6 | 6 | ns | |
| Need help with eating and did not receive | 4 | 29 | ns | |
| Hungry because no help | 4 | 7 | ns | |
| Thirsty because no help | 6 | 14 | ns | |
| Nadash, 2004 | PACE | MMLTC Plan | ||
| Mean ADL i limitations | 2.9 | 3.6 | <0.0001 | |
| Mean IADL i limitations | 5.6 | 5.5 | <0.0001 | |
| Nadash, 2013 | PACE | VCP | ||
| Patients with decline in ADL ii, % | 27.05 | 23.69 | 0.0461 | |
| Patients with no change in ADL ii, % | 21.18 | 21.90 | 0.6500 | |
| Patients with improved ADL ii, % | 16.50 | 29.90 | <0.0001 | |
| Patients with decline in IADL ii, % | 11.03 | 13.68 | 0.0431 | |
| Patients with no change in IADL ii, % | 48.79 | 45.29 | 0.0734 | |
| Patients with improved IADL ii, % | 4.83 | 16.52 | <0.0001 |
| Study Authors, Year | Outcomes | PACE | Comparison 1 | Comparison 2 | p |
|---|---|---|---|---|---|
| Nadash, 2004 | PACE | MMLTC Plan | |||
| HCBS utilization per member per month i | |||||
| Nursing | 8.42 | 2.20 | <0.0001 | ||
| Nurse practitioner | 0.93 | 0.05 | <0.0001 | ||
| Social work | 2.79 | 0.37 | <0.0001 | ||
| Ancillary therapists | 6.43 | 0.73 | <0.0001 | ||
| Home-delivered services utilization per member per month i | |||||
| Nursing | 1.16 | 2.20 | <0.0001 | ||
| Nurse practitioner | 0.07 | 0.05 | 0.0054 | ||
| Social work | 0.35 | 0.37 | <0.0001 | ||
| Ancillary therapists | 0.24 | 0.73 | <0.0001 | ||
| Adult day center visits per member per month i | 11.38 | 0.23 | <0.0001 | ||
| Hospital users i, % | 33.7 | 35.2 | 0.0362 | ||
| Proportion of days in hospitals i | 1.0 | 2.0 | <0.0001 | ||
| Mean LOS in hospitals i (days) | 5.9 | 9.5 | <0.0001 | ||
| Nursing home users i, % | 21.0 | 5.7 | <0.0001 | ||
| Proportion of days in nursing homes i | 4.5 | 0.9 | <0.0001 | ||
| Mean LOS in nursing homes i (days) | 44.2 | 37.2 | ns | ||
| Nadash, 2013 | PACE | VCP | |||
| Hospital users i, % | 20.3 | 33.1 | <0.0001 | ||
| Proportion of days in hospitals i | 0.6 | 2.3 | <0.0001 | ||
| Mean LOS in hospitals i (days) | 5.8 | 9.7 | <0.0001 | ||
| Nursing home users i, % | 13.3 | 7.2 | <0.0001 | ||
| Proportion of days in nursing homes i | 2.3 | 1.3 | <0.0001 | ||
| Mean LOS in nursing homes i (days) | 36.4 | 42.8 | 0.2767 | ||
| Patients discharged ii, % | 13.26 | 13.98 | 0.5915 | ||
| Weaver et al., 2008 | PACE | VA-Sole | VA+PACE | ||
| Patients with inpatient admissions, % i | 35 | 49 | 41 | ||
| Inpatient admissions/patient, mean ± SD i | 0.56 ± 3.0 | 1.12 ± 5.3 | 0.68 ± 3.1 | NR | |
| Total inpatient days/patient, mean ± SD i | 2.07 ± 14.7 | 8.55 ± 57.9 | 2.59 ± 15.0 | NR | |
| Patients with nursing home admissions, % i | 38 | 26 | 40 | NR | |
| Total nursing home admissions, mean ± SD i | 0.59 ± 2.9 | 0.41 ± 2.8 | 0.87 ± 3.9 | NR | |
| Nursing home days/patient, mean ± SD i | 12.56 ± 127.9 | 10.96 ± 124.6 | 25.1 ± 09.3 | NR | |
| Patients with outpatient clinic visits, % i | 100 | 97 | 100 | NR | |
| Outpatient clinic visit/patient, mean ± SD i | 39.48 ± 74.8 | 23.45 ± 45.6 | 39.17 ± 5.4 | NR | |
| Patients with home care visits, % i | 93 | 42 | 91 | NR | |
| Number of home care visits/patient, mean ± SD i | 7.70 ± 21.9 | 16.46 ± 108.7 | 8.15 ± 25.9 | NR | |
| Patients with adult day healthcare use, % i | 100 | 54 | 100 | NR | |
| Adult day healthcare visits/patient, days, mean ± SD i | 165.87 ± 220.7 | 14.41 ± 95.4 | 120.5 ± 227.1 | NR |
| Study Authors, Year | Outcomes | PACE | Comparison 1 | Comparison 2 | p |
|---|---|---|---|---|---|
| Kane et al., 2002 | Dependency/Discomfort | PACE (%) | WPP (%) | ||
| Pain/discomfort moderate/severe i | 44 | 49 | ns | ||
| Pain interferes with normal activity some/most of time i | 50 | 59 | ns | ||
| Very satisfied with pain control | 91 | 91 | ns | ||
| Depression > 5 on GDS i | 15 | 18 | ns | ||
| Nadash, 2013 | PACE | VCP | |||
| Deaths ii, % | 22.05 | 10.01 | <0.0001 | ||
| Risk of death (for participants who were treated); HR | ref | 0.55 | 95% CI 0.26–1.22 | ||
| Weaver et al., 2008 | PACE | VA-Sole | VA + PACE | ||
| Deaths, n (%) iii | 29 (34) | 52 (28) | 28 (28) | NR | |
| Survived, n (%) iii | 37 (66) | 113 (62) | 51 (50) | NR | |
| Wieland et al., 2010 | PACE | Nursing Home | Waiver Program | ||
| Five-year median survival (years) iv | 4.2 | 2.3 | 3.5 | 0.015 |
| Study Authors, Year | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Results | Overall Risk of Bias Judgment |
|---|---|---|---|---|---|---|---|---|
| Kane et al., 2002 | No information | No information | Low | No information | No information | Moderate | No information | No information |
| Nadash, 2004 | Moderate | Low | Low | No information | Moderate | Moderate | No information | Moderate |
| Nadash, 2013 | Low | Low | Low | No information | No information | Moderate | No information | Moderate |
| Weaver et al., 2008 | Moderate | Moderate | Moderate | No information | No information | Moderate | No information | No information |
| Wieland et al., 2010 | High | Low | Low | Low | No information | Low | Low | Low |
| Wieland et al., 2013 | High | Low | Low | Low | No information | Low | No information | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arku, D.; Felix, M.; Warholak, T.; Axon, D.R. Program of All-Inclusive Care for the Elderly (PACE) versus Other Programs: A Scoping Review of Health Outcomes. Geriatrics 2022, 7, 31. https://doi.org/10.3390/geriatrics7020031
Arku D, Felix M, Warholak T, Axon DR. Program of All-Inclusive Care for the Elderly (PACE) versus Other Programs: A Scoping Review of Health Outcomes. Geriatrics. 2022; 7(2):31. https://doi.org/10.3390/geriatrics7020031
Chicago/Turabian StyleArku, Daniel, Mariana Felix, Terri Warholak, and David R. Axon. 2022. "Program of All-Inclusive Care for the Elderly (PACE) versus Other Programs: A Scoping Review of Health Outcomes" Geriatrics 7, no. 2: 31. https://doi.org/10.3390/geriatrics7020031
APA StyleArku, D., Felix, M., Warholak, T., & Axon, D. R. (2022). Program of All-Inclusive Care for the Elderly (PACE) versus Other Programs: A Scoping Review of Health Outcomes. Geriatrics, 7(2), 31. https://doi.org/10.3390/geriatrics7020031