
Snoring Remediation with Oral Appliance Therapy Potentially Reverses Cognitive Impairment: An Intervention Controlled Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Neurocognitive Testing
2.4. Dental Assessment and Oral Appliance Intervention
2.5. Sleep Data Collection
2.6. Statistical Analysis
3. Results
3.1. Intention-to-Treat Group
3.2. RR-Start of Stable Sleep Period and Response to Tx after 4 Weeks
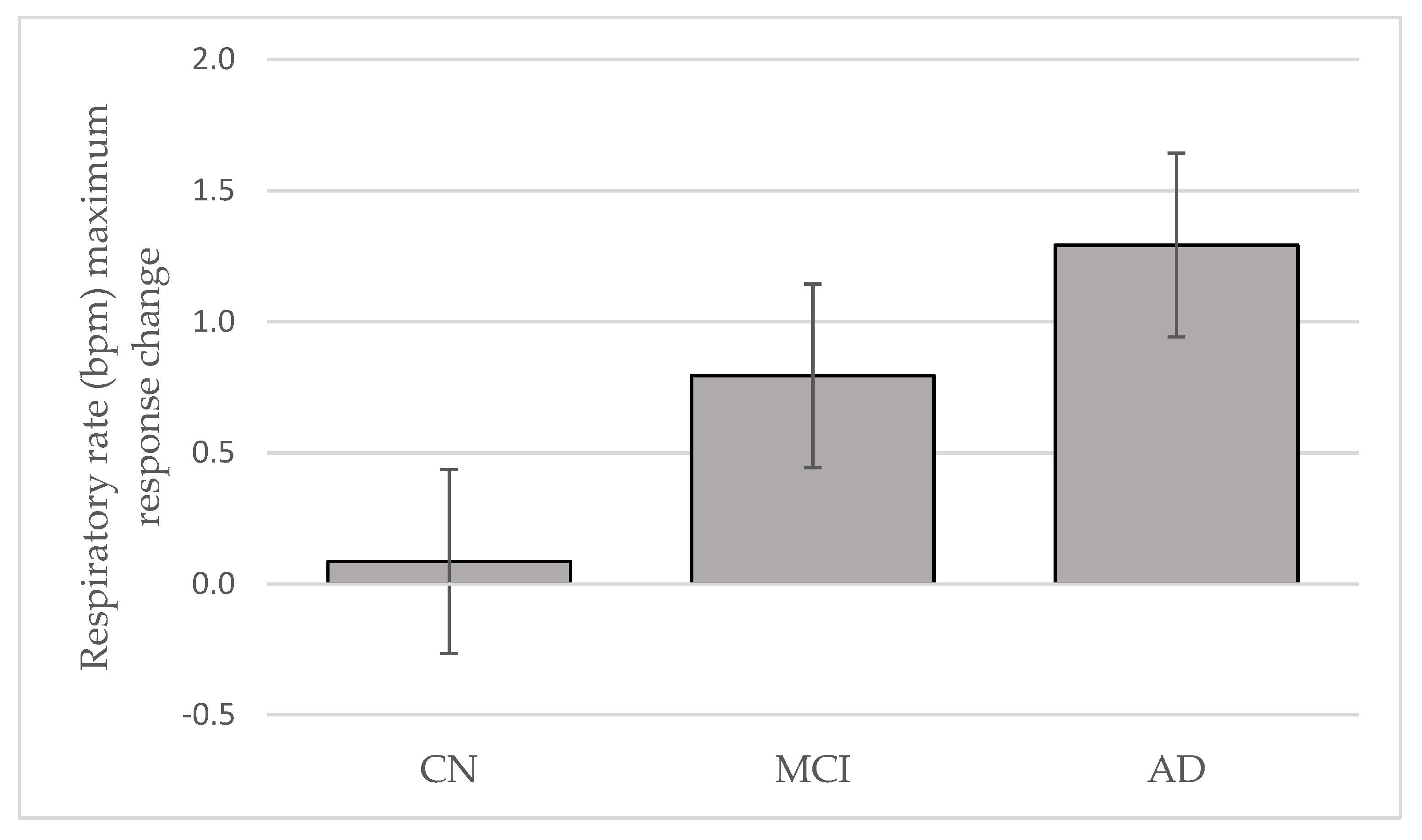
3.3. RR Max during Stable Sleep Period and Response to Tx after 4 Weeks
3.4. RR Fluctuation during Stable Sleep Period: Baseline and Tx after 4 Weeks
3.5. Snore Count Response to Tx after 4 Weeks
3.6. Compliance to Tx
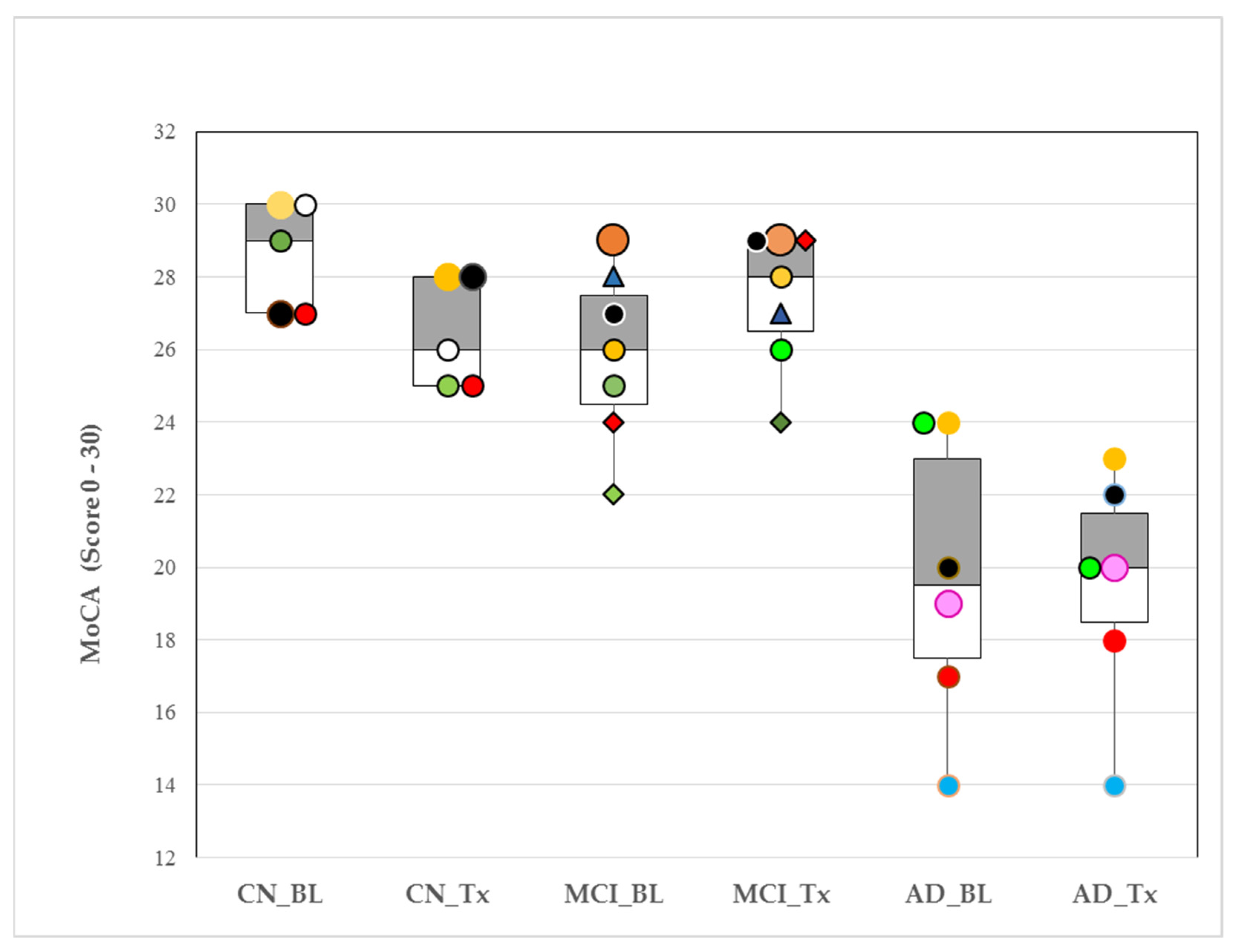
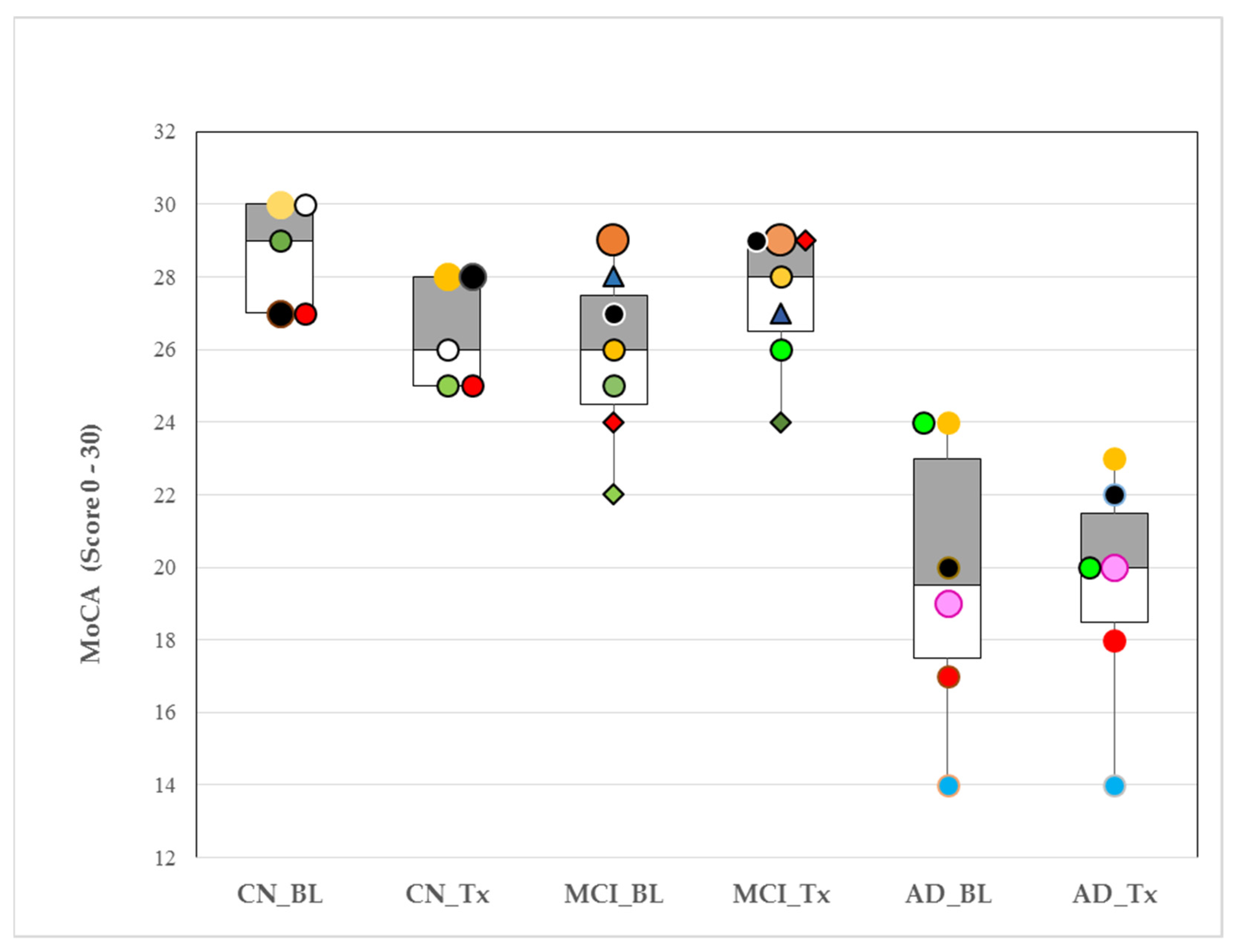
3.7. Montreal Cognitive Assessment (MoCA) Test Score—Response to Tx
3.8. Intervention Related Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Inclusion Criteria
Appendix A.2. Exclusion Criteria
References
- Wang, C.; Holtzman, D.M. Bidirectional relationship between sleep and Alzheimer’s disease: Role of amyloid, tau, and other factors. Neuropsychopharmacology 2020, 45, 104–120. [Google Scholar] [CrossRef] [PubMed]
- Ebel, D.L.; Torkilsen, C.G.; Ostrowski, T.D. Blunted Respiratory Responses in the Streptozotocin-Induced Alzheimer’s Disease Rat Model. J. Alzheimer’s Dis. 2017, 56, 1197–1211. [Google Scholar] [CrossRef] [PubMed]
- Fontanini, A.; Bower, J.M. Slow-waves in the olfactory system: An olfactory perspective on cortical rhythms. Trends Neurosci. 2006, 29, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Zelano, C.; Jiang, H.; Zhou, G.; Arora, N.; Schuele, S.; Rosenow, J.; Gottfried, J.A. Nasal Respiration Entrains Human Limbic Oscillations and Modulates Cognitive Function. J. Neurosci. 2016, 36, 12448–12467. [Google Scholar] [CrossRef] [Green Version]
- Heck, D.H.; McAfee, S.S.; Liu, Y.; Babajani-Feremi, A.; Rezaie, R.; Freeman, W.J.; Wheless, J.W.; Papanicolaou, A.C.; Ruszinkó, M.; Sokolov, Y.; et al. Breathing as a Fundamental Rhythm of Brain Function. Front. Neural. Circuits 2017, 10, 115. [Google Scholar] [CrossRef] [Green Version]
- Ito, J.; Roy, S.; Liu, Y.; Cao, Y.; Fletcher, M.L.; Lu, L.; Boughter, J.D.; Grün, S.; Heck, D.H. Whisker barrel cortex delta oscillations and gamma power in the awake mouse are linked to respiration. Nat. Commun. 2014, 5, 3572. [Google Scholar] [CrossRef] [Green Version]
- Johnson, D.A.; Lane, J.; Wang, R.; Reid, M.; Djonlagic, I.; Fitzpatrick, A.L.; Rapp, S.R.; Charles, L.E.; O’Hara, R.; Saxena, R.; et al. Greater Cognitive Deficits with Sleep-disordered Breathing among Individuals with Genetic Susceptibility to Alzheimer Disease. The Multi-Ethnic Study of Atherosclerosis. Ann. Am. Thorac. Soc. 2017, 14, 1697–1705. [Google Scholar] [CrossRef]
- Osorio, R.S.; Gumb, T.; Pirraglia, E.; Varga, A.W.; Lu, S.-E.; Lim, J.; Wohlleber, M.E.; Ducca, E.L.; Koushyk, V.; Glodzik, L.; et al. Sleep-disordered breathing advances cognitive decline in the elderly. Neurology 2015, 84, 1964–1971. [Google Scholar] [CrossRef] [Green Version]
- Liguori, C.; Maestri, M.; Spanetta, M.; Placidi, F.; Bonanni, E.; Mercuri, N.B.; Guarnieri, B. Sleep-disordered breathing and the risk of Alzheimer’s disease. Sleep Med. Rev. 2021, 55, 1–16. [Google Scholar] [CrossRef]
- Terpening, Z.; Lewis, S.J.; Yee, B.J.; Grunstein, R.R.; Hickie, I.B.; Naismith, S.L. Association between Sleep-Disordered Breathing and Neuropsychological Performance in Older Adults with Mild Cognitive Impairment. J. Alzheimers Dis. 2015, 46, 157–165. [Google Scholar] [CrossRef]
- Rimpilä, V.; Hosokawa, K.; Huhtala, H.; Saaresranta, T.; Salminen, A.V.; Polo, O. Transcutaneous carbon dioxide during sleep-disordered breathing. Resp. Physiol. Neurobi. 2015, 219, 95–102. [Google Scholar] [CrossRef]
- Wang, D.; Thomas, R.J.; Yee, B.J.; Grunstein, R.R. Hypercapnia is more important than hypoxia in the neuro-outcomes of sleep-disordered breathing. J. Appl. Physiol. 2016, 120, 1484. [Google Scholar] [CrossRef] [Green Version]
- Cooke, J.R.; Ancoli-Israel, S.; Liu, L.; Loredo, J.S.; Natarajan, L.; Palmer, B.S.; He, F.; Corey-Bloom, J. Continuous positive airway pressure deepens sleep in patients with Alzheimer’s disease and obstructive sleep apnea. Sleep Med. 2009, 10, 1101–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ancoli-Israel, S.; Palmer, B.W.; Cooke, J.R.; Corey-Bloom, J.; Fiorentino, L.; Natarajan, L.; Lui, L.; Ayalon, L.; He, F.; Loredo, J.S. Cognitive effects of treating obstructive sleep apnea in Alzheimer’s disease: A randomized controlled study. J. Am. Geriatr. Soc. 2008, 56, 2076–2081. [Google Scholar] [CrossRef] [Green Version]
- Cooke, J.R.; Ayalon, L.; Palmer, B.W.; Loredo, J.S.; Corey-Bloom, J.; Natarajan, L.; Liu, L.; Ancoli-Israel, S. Sustained use of CPAP slows deterioration of cognition, sleep, and mood in patients with Alzheimer’s disease and obstructive sleep apnea: A preliminary study. J. Clin. Sleep Med. 2009, 5, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Troussière, A.C.; Charley, C.M.; Salleron, J.; Richard, F.; Delbeuck, X.; Derambure, P.; Pasquier, F.; Bombios, S. Treatment of sleep apnoea syndrome decreases cognitive decline in patients with Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 2014, 85, 1405–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braak, H.; Del Tredici, K. The pathological process underlying Alzheimer’s disease in individuals under thirty. Acta Neuropathol. 2011, 121, 171–181. [Google Scholar] [CrossRef]
- Philby, M.F.; Macey, P.M.; Ma, R.A.; Kumar, R.; Gozal, D.; Gozal, L. Reduced Regional Grey Matter Volumes in Pediatric Obstructive Sleep Apnea. Sci. Rep. 2017, 7, 44566. [Google Scholar] [CrossRef]
- Berridge, C.W.; Schmeichel, B.E.; España, R.A. Noradrenergic modulation of wakefulness/arousal. Sleep Med. Rev. 2012, 16, 187–197. [Google Scholar] [CrossRef] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Das, N.; Ren, J.; Spence, J.S.; Rackley, A.; Chapman, S.B. Relationship of Parieto-Occipital Brain Energy Phosphate Metabolism and Cognition Using 31P MRS at 7-Tesla in Amnestic Mild Cognitive Impairment. Front. Aging Neurosci. 2020, 12, 222. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Wilkinson, G.S.; Robertson, G.J. Wide Range Achievement Test, 4th ed.; Professional manual; Psychological Assessment Resources: Lutz, FL, USA, 2006. [Google Scholar]
- Schneiderman, E.; Schramm, P.; Hui, J.; Wilson, P.D.; Moura, P.; German, Z.; McCann, A.; Newton, M. Randomized Trial of 2 Self-Titrated Oral Appliances for Airway Management. J. Dent. Res. 2021, 100, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.J.; Mietus, J.E.; Peng, C.K.; Goldberger, A.L. An electrocardiogram based technique to assess cardiopulmonary coupling during sleep. SLEEP 2005, 28, 1151–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: http://www.R-project.org/ (accessed on 1 April 2021).
- Nasreddine, Z.S.; Patel, B.B. Validation of Montreal Cognitive Assessment, MoCA, Alternate French Versions. Can. J. Neurol. Sci. 2016, 43, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Baril, A.A.; Gagnon, K.; Brayet, P.; Montplaisir, J.; De Beaumont, L.; Carrier, J.; Lafond, C.; L’Heureux, F.; Gagnon, J.; Gosselin, N. Gray Matter Hypertrophy and Thickening with Obstructive Sleep Apnea in Middle-aged and Older Adults. Am. J. Respir. Crit. Care Med. 2017, 195, 1509–1518. [Google Scholar] [CrossRef]
- Parvizi, J.; Van Hoesen, G.W.; Damasio, A. The selective vulnerability of brainstem nuclei to Alzheimer’s disease. Ann. Neurol. 2001, 49, 53–66. [Google Scholar] [CrossRef]
- O’Brien, L.M.; Mervis, C.B.; Holbrook, C.R.; Bruner, J.L.; Klaus, C.J.; Rutherford, J.; Raffield, T.J.; Gozal, D. Neurobehavioral Implications of Habitual Snoring in Children. Pediatrics 2004, 114, 44–49. [Google Scholar] [CrossRef] [Green Version]
- McCracken, J.T.; Poland, R.E.; Lutchmansingh, P.; Edwards, C. Sleep electroencephalographic abnormalities in adolescent depressives: Effects of scopolamine. Biol. Psychiatry 1997, 42, 577–584. [Google Scholar] [CrossRef]
- Rao, U.; Lin, K.M.; Schramm, P.; Poland, R.E. REM sleep and cortisol responses to scopolamine during depression and remission in women. Int. J. Neuropsychopharmacol. 2004, 7, 265–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleinfeld, D.; Deschênes, M.; Wang, F.; Moore, J.D. More than a rhythm of life: Breathing as a binder of orofacial sensation. Nat. Neurosci. 2014, 17, 647–651. [Google Scholar] [CrossRef] [Green Version]
- Başar, E.; Başar-Eroglu, C.; Karakaş, S.; Schürmann, M. Gamma, alpha, delta, and theta oscillations govern cognitive processes. Int. J. Psychophysiol. 2001, 39, 241–248. [Google Scholar] [CrossRef]
- Lucke, J.A.; de Gelder, J.; Blomaard, L.C.; Heringhaus, C.; Alsma, J.; Schuit, S.C.E.K.N.; Brink, A.; Anten, S.; Blauw, G.J.; De Groot, B.; et al. Vital signs and impaired cognition in older emergency department patients: The APOP study. PLoS ONE 2019, 14, e0218596. [Google Scholar] [CrossRef] [PubMed]
- Stoohs, R.A.; Blum, H.C.; Haselhorst, M.; Duchna, H.W.; Guilleminault, C.; Dement, W.C. Normative data on snoring: A comparison between younger and older adults. Eur. Respir. J. 1998, 11, 451–457. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Group (n = 18) | CN (n = 5) | MCI (n = 7) | AD (n = 6) | |
|---|---|---|---|---|
| Age (years) Mean ± SD (Range) | 67.67 ± 6.68 | 65.60 ± 7.30 (56–75) | 68.57 ± 7.55 (58–80) | 68.33 ± 6.12 (62–75) |
| Gender (M/F) | (9/9) | (2/3) | (2/5) | (5/1) |
| Education (years) Mean ± SD (Range) | 17.31 ± 2.83 | 18.0 ± 2.45 (16–22) | 16.93 ± 3.68 (12–24) | 17.17 ± 2.13 (14–19) |
| MMSE Mean ± SD (Range) | 27.39 ± 2.07 | 29.20 ± 1.30 (27–30) | 28.14 ± 1.35 (26–30) | 25.00 ± 2.82 (21–28) * |
| Geriatric depression scale Mean ± SD (Range) | 5.61 ± 4.74 | 3.20 ± 3.35 (0–8) | 8.71 ± 5.47 (2–17) | 4.00 ± 3.40 (0–9) |
| Mean ± SD | Contrasts (p Value) | ||||
|---|---|---|---|---|---|
| Variable | CN (n = 14) | MCI (n = 14) | AD (n = 9) | MCI-CN | AD-CN |
| RR start (bpm) | 13.56 ± 2.13 | 13.44 ± 2.17 | 13.87 ± 2.24 | 0.737 | 0.223 |
| RR max (bpm) | 20.95 ± 3.18 | 20.46 ± 3.95 | 20.32 ± 3.22 | 0.143 | 0.073 |
| RR fluctuation (pixels) | 46.89 ± 19.58 | 45.77 ± 17.65 | 38.81 ± 18.52 | 0.668 | <0.001 |
| Contrasts | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| BL | Tx | Within Group | p Value | Between Group | p Value | Change (∆) from Mean | p Value | ||
| RR start (bpm) Tx-BL (∆) | BL | Tx | Tx-BL (∆) | 0.763 | |||||
| CN | 14.30 ± 3.40 | 14.52 ± 3.51 | 0.22 ± 0.31 | 0.968 | |||||
| MCI | 14.06 ± 5.53 | 14.34 ± 3.47 | 0.28 ± 0.25 | 0.156 | MCI-CN | 0.820 | 0.948 | MCI(∆)-CN(∆) | 0.875 |
| AD | 13.96 ± 2.18 | 13.62 ± 3.19 | −0.34 ± 0.29 | 0.844 | AD-CN | 0.513 | <0.001 | AD(∆)-CN(∆) | 0.190 |
| RR max (bpm) | Tx-BL (∆) | 0.008 | |||||||
| CN | 20.77 ± 3.40 | 20.62 ± 3.51 | −0.15 ± 0.50 | 0.963 | |||||
| MCI | 21.88 ± 5.53 | 21.13 ± 3.47 | −0.75 ± 0.41 | 0.269 | MCI-CN | 0.533 | 0.738 | MCI(∆)-CN(∆) | 0.279 |
| AD | 20.37 ± 2.18 | 18.86 ± 3.19 | −1.51 ± 0.46 | 0.005 | AD-CN | 0.429 | <0.001 | AD(∆)-CN(∆) | 0.081 |
| RR fluctuation (pixels) | Tx-BL (∆) | 0.080 | |||||||
| CN | 37.31 ± 5.71 | 39.87 ± 5.80 | 2.56 ± 2.84 | 0.963 | |||||
| MCI | 50.62 ± 4.86 | 43.75 ± 4.87 | −6. 87 ± 2.36 | 0.003 | MCI-CN | 0.258 | 0.790 | MCI(∆)-CN(∆) | 0.012 |
| AD | 37.67 ± 5.22 | 33.94 ± 5.32 | −3.73 ± 0.46 | 0.593 | AD-CN | 0.718 | 0.692 | AD(∆)-CN(∆) | 0.109 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schramm, P.; Das, N.; Schneiderman, E.; German, Z.; Hui, J.; Wilson, D.; Spence, J.S.; Moura, P.; Chapman, S.B. Snoring Remediation with Oral Appliance Therapy Potentially Reverses Cognitive Impairment: An Intervention Controlled Pilot Study. Geriatrics 2021, 6, 107. https://doi.org/10.3390/geriatrics6040107
Schramm P, Das N, Schneiderman E, German Z, Hui J, Wilson D, Spence JS, Moura P, Chapman SB. Snoring Remediation with Oral Appliance Therapy Potentially Reverses Cognitive Impairment: An Intervention Controlled Pilot Study. Geriatrics. 2021; 6(4):107. https://doi.org/10.3390/geriatrics6040107
Chicago/Turabian StyleSchramm, Preetam, Namrata Das, Emet Schneiderman, Zohre German, Jason Hui, Duane Wilson, Jeffrey S. Spence, Pollyana Moura, and Sandra B. Chapman. 2021. "Snoring Remediation with Oral Appliance Therapy Potentially Reverses Cognitive Impairment: An Intervention Controlled Pilot Study" Geriatrics 6, no. 4: 107. https://doi.org/10.3390/geriatrics6040107
APA StyleSchramm, P., Das, N., Schneiderman, E., German, Z., Hui, J., Wilson, D., Spence, J. S., Moura, P., & Chapman, S. B. (2021). Snoring Remediation with Oral Appliance Therapy Potentially Reverses Cognitive Impairment: An Intervention Controlled Pilot Study. Geriatrics, 6(4), 107. https://doi.org/10.3390/geriatrics6040107