Effect of the Nurse-Led Sexual Health Discharge Program on the Sexual Function of Older Patients Undergoing Transurethral Resection of Prostate: A Randomized Controlled Trial

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
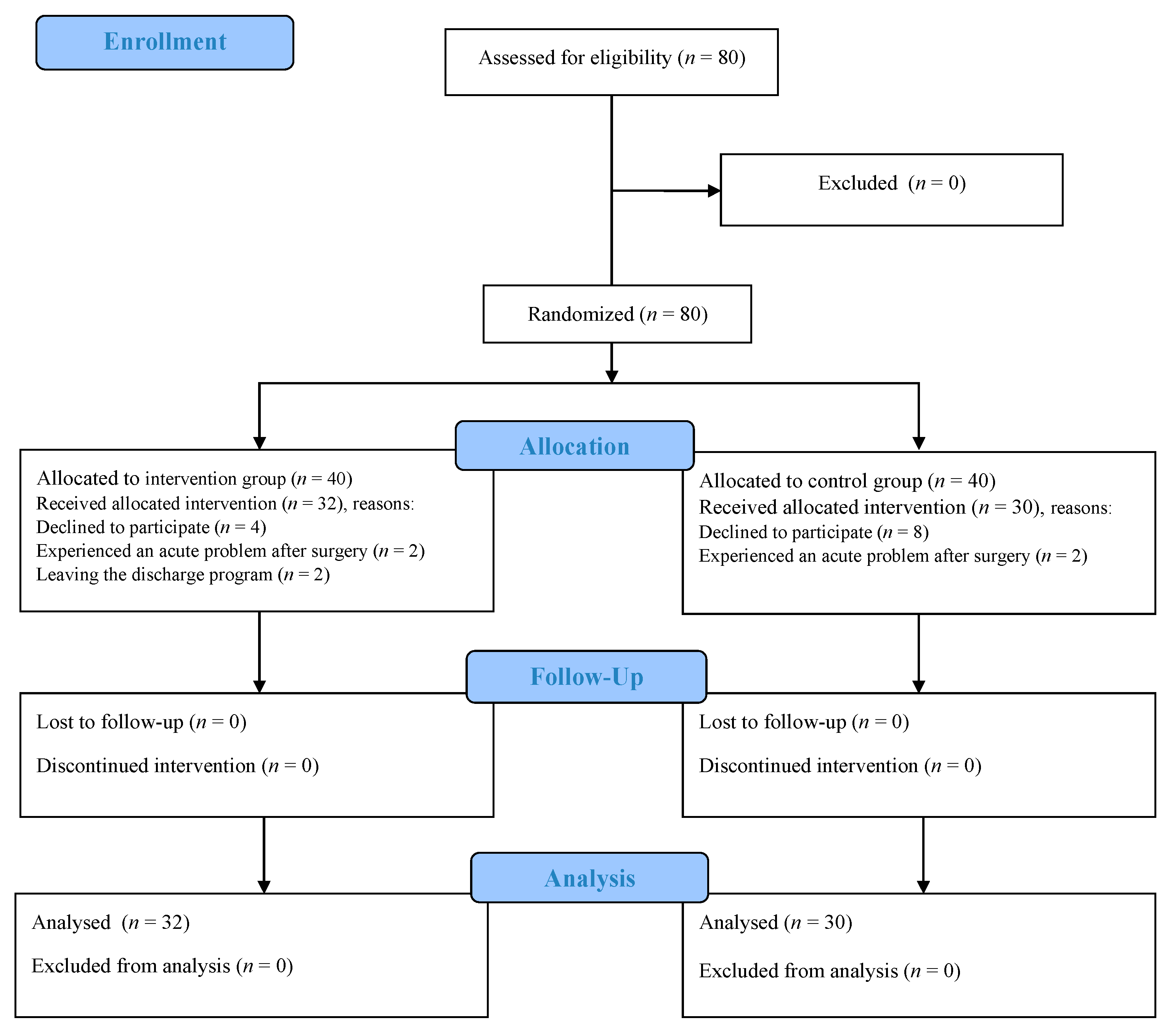
2.2. Setting and Participants
2.3. Measures
- ○
- The demographic data form for gathering data on the older patients’ age, body mass index, education level, health insurance status, employment status, economic status, independence in the activities of daily living, and past medical history.
- ○
- The IIEF Questionnaire was developed and validated by Rosen in 1997. It is a self-report questionnaire of the male sexual function and consists of 15 questions with a 5-point Likert scale. The minimum and maximum scores were 15 and 75, respectively and a higher score indicated a better sexual performance. Severity of erectile dysfunction was classified as follows: 6–10 (severe), 11–16 (moderate), 17–21 (mild-to-moderate), 22–25 (mild), 26–30 (no dysfunction) [15]. More details on the number of items and relating scores were presented in Table 1.
2.4. Validity and Reliability
2.5. Ethical Considerations
2.6. Intervention
- ○
- ○
- ○
- The third session: Effect of fatigue on sexual function, the importance of managing urinary incontinence for improving sexual satisfaction, role of physical activity and exercise in the recovery of sexual performance, role of pelvic floor muscle exercises in the improvement of sexual function and activity through controlling urinary incontinence [8,17,18].
2.7. Data analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hinkle, J.L.; Cheever, K.H. Brunner & Suddarth’s Textbook of Medical-Surgical Nursing; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Speakman, M.; Kirby, R.; Doyle, S.; Ioannou, C. Burden of male lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH)–focus on the UK. BJU Inter. 2015, 115, 508–519. [Google Scholar] [CrossRef] [PubMed]
- Bushman, W. Etiology, epidemiology, and natural history. Urol. Clin. 2009, 36, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Girman, C.J.; Jacobsen, S.J.; Guess, H.A.; Oesterling, J.E.; Chute, C.G.; Panser, L.A.; Lieber, M.M. Natural history of prostatism: Relationship among symptoms, prostate volume and peak urinary flow rate. J. Urol. 1995, 153, 1510–1515. [Google Scholar] [CrossRef]
- Milicevic, S. The impact of benign prostatic hyperplasia surgical treatment with turp method on the quality of life. Acta Inform. Med. 2011, 19, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Rassweiler, J.; Teber, D.; Kuntz, R.; Hofmann, R. Complications of transurethral resection of the prostate (TURP)—incidence, management, and prevention. Eur. Urol. 2006, 50, 969–980. [Google Scholar] [CrossRef] [PubMed]
- Salonia, A.; Burnett, A.L.; Graefen, M.; Hatzimouratidis, K.; Montorsi, F.; Mulhall, J.P.; Stief, C. Prevention and management of postprostatectomy sexual dysfunctions part 2: Recovery and preservation of erectile function, sexual desire, and orgasmic function. Eur. Urol. 2012, 62, 273–286. [Google Scholar] [CrossRef] [PubMed]
- Kozier, B.; Erb, G.L.; Berman, A.; Snyder, S.; Frandsen, G. Kozier and Erb’s Fundamentals of Nursing: Concepts, Process, and Practice, 10th ed.; Pearson Australia: Melbourne, Australia, 2016. [Google Scholar]
- Molton, I.R.; Siegel, S.D.; Penedo, F.J.; Dahn, J.R.; Kinsinger, D.; Traeger, L.N.; Antoni, M.H. Promoting recovery of sexual functioning after radical prostatectomy with group-based stress management: The role of interpersonal sensitivity. J. Psychosom. Res. 2008, 64, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Schover, L.R.; Canada, A.L.; Yuan, Y.; Sui, D.; Neese, L.; Jenkins, R.; Rhodes, M.M. A randomized trial of internet-based versus traditional sexual counseling for couples after localized prostate cancer treatment. Cancer 2012, 118, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Nurjannah, I.; Mills, J.; Usher, K.; Park, T. Discharge planning in mental health care: An integrative review of the literature. J. Clin. Nurs. 2014, 23, 1175–1185. [Google Scholar] [CrossRef] [PubMed]
- Sharif, F.; Moshkelgosha, F.; Molazem, Z.; Kalyani, M.N.; Vossughi, M. The effects of discharge plan on stress, anxiety and depression in patients undergoing percutaneous transluminal coronary angioplasty: A randomized controlled trial. Int. J. Community Based Nurs. Midwifery 2014, 2, 60–68. [Google Scholar] [PubMed]
- Andrietta, M.P.; Lopes Moreira, R.S.; Bottura Leite de Barros, A.L. Hospital discharge plan for patients with congestive heart failure. Revista Latino-Americana de Enfermagem 2011, 19, 1445–1452. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jack, B.W.; Chetty, V.K.; Anthony, D.; Greenwald, J.L.; Sanchez, G.M.; Johnson, A.E.; Martin, S. A reengineered hospital discharge program to decrease rehospitalization: A randomized trial. Ann. Int. Med. 2009, 150, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.C.; Cappelleri, J.C.; Gendrano, N., III. The International Index of Erectile Function (IIEF): A state-of-the-science review. Int. J. Impot. Res. 2002, 14, 226–244. [Google Scholar] [CrossRef] [PubMed]
- Tanagho, E.A.; McAninch, J.W. Smith’s Urology; McGraw Hill Professional: New York, NY, USA, 2008. [Google Scholar]
- Bridgeman, B.; Roberts, S.G. The 4-3-2 Method for Kegel Exercises. Am. J. Men’s Health 2010, 4, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Hodges, P.W.; Stafford, R.E.; Hall, L.; Neumann, P.; Morrison, S.; Frawley, H.; Cameron, A.P. Reconsideration of pelvic floor muscle training to prevent and treat incontinence after radical prostatectomy. Urol. Oncol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Simon, R.M.; Howard, L.; Zapata, D.; Frank, J.; Freedland, S.J.; Vidal, A.C. The association of exercise with both erectile and sexual function in black and white men. J. Sex. Med. 2015, 12, 1202–1210. [Google Scholar] [CrossRef] [PubMed]
- Geraerts, I.; Van Poppel, H.; Devoogdt, N.; De Groef, A.; Fieuws, S.; Van Kampen, M. Pelvic floor muscle training for erectile dysfunction and climacturia 1 year after nerve sparing radical prostatectomy: A randomized controlled trial. Int. J. Impot. Res. 2016, 28, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Brotto, L.A.; Heiman, J.R.; Goff, B.; Greer, B.; Lentz, G.M.; Swisher, E.; Van Blaricom, A. A psychoeducational intervention for sexual dysfunction in women with gynecologic cancer. Arch. Sex. Behav. 2008, 37, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Lassen, B.; Gattinger, H.; Saxer, S. A systematic review of physical impairments following radical prostatectomy: Effect of psychoeducational interventions. J. Adv. Nurs. 2013, 69, 2602–2612. [Google Scholar] [CrossRef] [PubMed]
- Assalian, P. Psychological and interpersonal dimensions of sexual function and dysfunction. Arab J. Urol. 2013, 11, 217–221. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Domain | Items | Score Range | Maximum Score |
|---|---|---|---|
| Erectile function | 1–5, 15 | 0–5 | 30 |
| Orgasmic function | 9–10 | 0–5 | 10 |
| Sexual desire | 11–12 | 1–5 | 10 |
| Intercourse satisfaction | 6–8 | 0–5 | 15 |
| Overall satisfaction | 13–14 | 1–5 | 10 |
| Variable | Mean ± Standard Deviation | Statistical Analysis/ p-Value | ||||
|---|---|---|---|---|---|---|
| Intervention Group | Control Group | |||||
| Age (year) | 6.23 ± 64.13 | 6.80 ± 67.27 | Df = 60 t = −1.897 p = 0.063 | |||
| Body mass index | 3.22 ± 24.5 | 2.71 ± 24.28 | p= 0.529 | |||
| Intervention group | Control group | |||||
| n | % | n | % | |||
| Education level | Illiterate | 5 | 15.6 | 5 | 16.7 | p = 0.018 |
| Primary | 7 | 21.9 | 17 | 56.6 | ||
| Under diploma | 7 | 21.9 | 5 | 16.7 | ||
| Diploma | 12 | 37.5 | 3 | 10 | ||
| Academic | 1 | 3.1 | 0 | 0 | ||
| Employment Status | Employee | 6 | 18.8 | 5 | 19.7 | p = 0.752 |
| Retired | 22 | 68.7 | 19 | 60.3 | ||
| Other | 4 | 12.5 | 6 | 20 | ||
| Insurance | Yes | 32 | 100 | 30 | 100 | p = 0.99 |
| No | 0 | 0 | 0 | 0 | ||
| Supplementary Insurance | Yes | 32 | 100 | 28 | 93.3 | p = 0.230 |
| No | 0 | 0 | 2 | 6.7 | ||
| Economic status | Good | 31 | 96.9 | 29 | 96.7 | p = 0.999 |
| Not good | 1 | 3.1 | 1 | 3.3 | ||
| Dependency in daily living | Yes | 31 | 96.9 | 30 | 100 | p = 0.999 |
| No | 1 | 3.1 | 0 | 0 | ||
| Hypertension | Yes | 9 | 28.1 | 6 | 20 | p = 0.558 |
| No | 23 | 71.9 | 24 | 80 | ||
| Diabetes | Yes | 5 | 15.6 | 2 | 6.7 | p = 0.427 |
| No | 27 | 84.4 | 28 | 93.3 | ||
| Heart failure | Yes | 3 | 9.4 | 2 | 6.7 | p = 0.999 |
| No | 29 | 90.6 | 28 | 93.3 | ||
| Smoking habit | Yes | 5 | 15.6 | 3 | 10 | p = 0.709 |
| No | 27 | 84.4 | 27 | 90 | ||
| Drug use for BPH | Yes | 20 | 62.5 | 14 | 46.7 | p = 0.307 |
| No | 12 | 37.5 | 16 | 53.3 | ||
| Drug use for COPD | Yes | 0 | 0 | 2 | 6.7 | p = 0.230 |
| No | 32 | 100 | 28 | 93.3 | ||
| Domains | Intervention Group | Control Group | p-Value |
|---|---|---|---|
| Before the intervention | |||
| Mean (standard deviation) | Mean (standard deviation) | ||
| Erectile function | 19.69 (10.38) | 18.59 (10.92) | Intervention: 0.68 control: 0. 61 |
| Orgasmic function | 7.12 (4.12) | 6.83 (4.46) | Intervention: 0.73 control: 0.71 |
| Sexual desire | 5.16 (2.05) | 5.63 (2.28) | Intervention: 0.31 control: 0.54 |
| Intercourse satisfaction | 7.03 (4.22) | 7.27 (5.07) | Intervention: 0.41 control: 0.59 |
| Overall satisfaction | 6.12 (2.62) | 5.73 (2.57) | Intervention: 0.98 control: 0.10 |
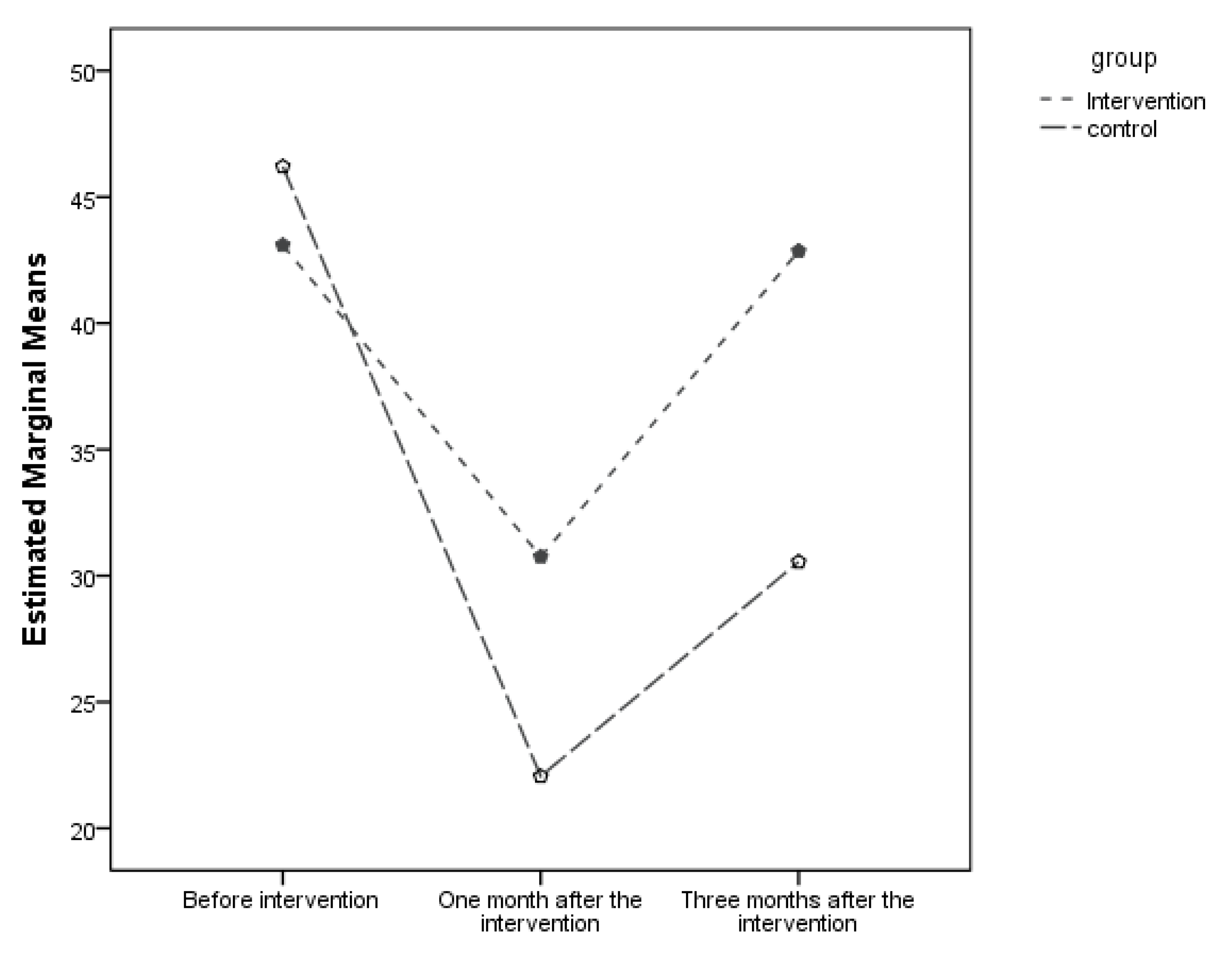
| Sexual function | 45.12 (22.21) | 44.03 (24.34) | Intervention: 0.61 control: 0.54 |
| One month after the intervention | |||
| Erectile function | 13.59 (11.03) | 8.70 (10.58) | Intervention: 0.195 control: 0.261 |
| Orgasmic function | 4 (4) | 2.60 (3.82) | Intervention: 0.273 control: 0.519 |
| Sexual desire | 5.16 (2.20) | 3.63 (2.10) | Intervention: 0.028 control: 0.256 |
| Intercourse satisfaction | 4.12 (3.96) | 2.67 (3.96) | Intervention: 0.268 control: 0.464 |
| Overall satisfaction | 4.84 (2.55) | 3.43 (2.22) | Intervention: 0.06 control: 0.35 |
| Sexual function | 31.72 (22.38) | 21.03 (21.93) | Intervention: 0.15 control: 0.315 |
| Three months after the intervention | |||
| Erectile function | 19.09 (10.41) | 12.67 (9.78) | Intervention: 0.044 control: 0.374 |
| Orgasmic function | 6.28 (3.97) | 4.90 (3.85) | Intervention: 0.331 control: 0.318 |
| Sexual desire | 5.69 (2.27) | 3.93 (2.05) | Intervention: 0.01 control: 0.29 |
| Intercourse satisfaction | 6.94 (4.17) | 4.27 (3.45) | Intervention: 0.03 control: 0.28 |
| Overall satisfaction | 5.57 (2.81) | 3.83 (2.16) | Intervention: 0.01 control: 0.61 |
| Sexual function | 43.75 (22.62) | 29.60 (20.18) | Intervention: 0.038 control: 0.33 |
| Interaction Effect | p-Value |
|---|---|
| Time | 0.92 |
| Time and intervention | 0.04 |
| Intervention | 0.24 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayat, R.; Shahsavari, H.; Faghihzadeh, S.; Amaniyan, S.; Vaismoradi, M. Effect of the Nurse-Led Sexual Health Discharge Program on the Sexual Function of Older Patients Undergoing Transurethral Resection of Prostate: A Randomized Controlled Trial. Geriatrics 2020, 5, 13. https://doi.org/10.3390/geriatrics5010013
Bayat R, Shahsavari H, Faghihzadeh S, Amaniyan S, Vaismoradi M. Effect of the Nurse-Led Sexual Health Discharge Program on the Sexual Function of Older Patients Undergoing Transurethral Resection of Prostate: A Randomized Controlled Trial. Geriatrics. 2020; 5(1):13. https://doi.org/10.3390/geriatrics5010013
Chicago/Turabian StyleBayat, Ramin, Hooman Shahsavari, Soghrat Faghihzadeh, Sara Amaniyan, and Mojtaba Vaismoradi. 2020. "Effect of the Nurse-Led Sexual Health Discharge Program on the Sexual Function of Older Patients Undergoing Transurethral Resection of Prostate: A Randomized Controlled Trial" Geriatrics 5, no. 1: 13. https://doi.org/10.3390/geriatrics5010013
APA StyleBayat, R., Shahsavari, H., Faghihzadeh, S., Amaniyan, S., & Vaismoradi, M. (2020). Effect of the Nurse-Led Sexual Health Discharge Program on the Sexual Function of Older Patients Undergoing Transurethral Resection of Prostate: A Randomized Controlled Trial. Geriatrics, 5(1), 13. https://doi.org/10.3390/geriatrics5010013