Abstract
Physical activity is vital for the prevention of sarcopenia and frailty. The training effects of recreational golf on muscle function in older people are unknown. The present study examined quadriceps muscle and subcutaneous fat thickness in 66 older females. Thirty-one golfers (mean age 69.1 years, standard deviation ±3.4) were compared with 35 less active non-golfers (73.4 ± 4.2 years). Images of the dominant anterior thigh were obtained using real-time B-mode ultrasound imaging. Thickness of muscle (rectus femoris, vastus intermedius, and intermuscular fascia) and subcutaneous tissue (fat and perimuscular fascia) was measured, and percentage contributions calculated. Muscle thickness was significantly greater (p < 0.001) in golfers (mean 2.78 cm ± 0.73 cm) than non-golfers (2.18 cm ± 0.55 cm). Mean percentage contribution of muscle and non-contractile tissue was 64% ± 9% and 36% ± 9%, respectively, in golfers, compared to 58% ± 8% and 42% ± 8% in non-golfers (p = 0.013). Multiple linear regression analysis, controlling for age and BMI, showed that golfers still had higher total anterior thigh thickness (regression parameter for non-golfers B = −0.984, p = 0.004) and higher muscle thickness (B = −0.619, p = 0.002). This study indicates an association between recreational golf and greater relative thigh muscle thickness and lower subcutaneous fat than in less active controls. Training effects need to be examined in prospective controlled trials in males and females in different age groups.
1. Introduction
Loss of muscle mass and strength, and the resulting loss of function that occur in sarcopenia begins at about the age of 40 years, and accelerates beyond 65–70 years [1]. Rates of decline can be slowed with regular strenuous training in masters athletes [2,3]. However, little is known about the effects of recreational activity on muscle in older people in the general population.
Quadriceps is an important muscle for mobility, and its relative thickness to subcutaneous fat has been quantified in healthy young and older adults who are not very active [4]. Studying thigh tissue thickness in groups with different activity levels may provide an indication of musculoskeletal health using the simple, rapid measurement of relative muscle thickness on ultrasound scans.
Recreational golf is associated with better cardiovascular health and musculoskeletal function [5] and balance [6] than sedentary controls, and greater life expectancy [7]. The specific effects of playing golf on aspects of musculoskeletal health warrant investigation.
Females have greater loss of muscle thickness (12%–23%) and strength (58%–68%) than males [8]. Agyapong-Badu et al. [4] reported that older females (aged 65–90) have a mean anterior thigh percentage muscle thickness of almost 20% (18%) less than males in the same age category. Sarcopenia can be partially reduced by physical activity; resistance exercise being the most effective type of training [2].
Ultrasound is suitable for routine imaging, as it is safe (contains no ionising radiation), rapid, portable, and cost-effective [9]. B-mode ultrasound imaging (USI) is a reliable (within and between investigators) method of measuring various skeletal muscles and sub-cutaneous tissue, when used by an experienced operator following strict protocol guidelines [9,10,11]. Ultrasound imaging of quadriceps has been shown to be valid when compared to magnetic resonance imaging (MRI) [9,12,13,14]. Muscle mass (cross-sectional area, CSA or thickness) and strength are highly correlated [8,15]. Therefore, measuring the thickness of a muscle will provide an estimate of its strength.
The World Health Organisation recommends that those over 65 years should carry out muscle strengthening activities on two or more days per week [16]. It is unknown whether playing golf would have sufficient strength training effects, and this knowledge gap has been highlighted as an urgent research need, particularly in older people [17].
The present study aimed to use B-mode USI to compare the relative proportions of quadriceps muscle and non-contractile (subcutaneous fat, SF, and perimuscular fascia) tissues to total anterior thigh thickness between moderately active and less active older females. The study addressed the question: is moderate activity in recreational golfers associated with greater relative muscle thickness and less subcutaneous fat than in less active older females? A positive outcome would warrant a prospective study to examine the strengthening effects of playing golf, as muscle size is an indicator of strength [8,15].
2. Materials and Methods
This was a cross-sectional, quantitative, observational comparative study.
2.1. Participants
A convenience sample of 31 female golfers (aged 65–77 years, mean 69.1 ± 3.4) were recruited from golf clubs in Hampshire. Inclusion criteria were: female golfer aged 65–80 years who played a minimum of one round of golf (18 holes) per week, walking between holes. Three questions from the Physical Activity Scale for the Elderly (PASE) were used for screening purposes to ensure that participants were moderately active. Questions included: “In a typical week, how many days would you participate in light sport/recreational activities (e.g., light cycling, lawn bowls, golf with buggy)?; In a typical week, how many days would you participate in moderate sport/recreational activities (e.g., doubles tennis, golf without a buggy, ballroom dancing)?; In a typical week, how many days would you participate in strenuous sport/recreational activities (e.g., singles tennis, swimming, jogging)?” An additional question for the golfers was: “Do you play a full round of golf (18 holes), by walking, every week? If so, how many times per week?” Participants were not requested to specify their activities other than golf, as the purpose was to ensure that they were moderately active and not considered sedentary, for inclusion in the study.
Participants were cognitively able and capable of travelling to the testing location. Those with common conditions (e.g., diabetes/blood pressure) were included providing that their condition was controlled and had not deteriorated recently. Exclusion criteria were: musculoskeletal injury in the last five years which led to immobility for more than one week; uncontrolled diabetes or blood pressure; a known neurological disorder; arthritis which restricted the ability to perform every-day activities; receiving treatment for cancer; taking medication which affects muscle function. These criteria aimed to include those whose thigh tissue thickness would represent a moderately active older population, unaffected by pathology. Ethical approval was gained from the Faculty of Health Sciences, University of Southampton Ethics Committee (Ethics approval number 9650). Participants provided written, informed consent prior to data collection.
The present participants were compared with a subset of non-golfing older females from a larger study of sedentary young and older males and females [4] whose scans were re-analysed using a modified measurement protocol (see below). The above inclusion (except regular moderate activity) and exclusion criteria applied to this group. The characteristics of both groups of participants are shown in Table 1.

Table 1.
Descriptive characteristics of golfers and non-golfers (from Agyapong-Badu et al. 2014 [4]).
2.2. Ultrasound Imaging
Participants rested while seated for a minimum of 10 minutes before the ultrasound images were taken. Images of the anterior thigh were produced using a real-time B-mode ultrasound scanner (Imagic Agile, Pie Data, Ltd., Kontron Medical, St Germaine en Laye, France) with a 5–6.6 MHz curvilinear (abdominal) transducer. The transducer was placed transversely at a point two-thirds of the distance between the anterior-superior iliac spine and the superior pole of the patella, which was marked on the skin with a non-toxic pen [18]. Participants lay relaxed in supine lying, with the knee extended and leg supported by sand bags on either side of the ankle to maintain the hip in neutral (Figure 1). The probe was placed on the skin, with minimal pressure, to produce an image showing rectus femoris (RF), vastus intermedius (VI), SF, and perimuscular fascia. Two images were taken from the dominant side by the same experienced operator (SB). Leg dominance was determined by the preferred leg for kicking a ball.
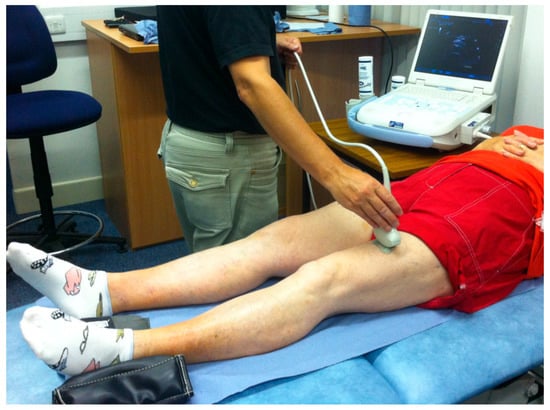
Figure 1.
Ultrasound imaging set up with the participant in supine.
Images were measured later off-line by IH, using a Matlab algorithm (written by MW). The thickness of two tissue layers was measured: (1) the superficial non-contractile layer comprised subcutaneous fat and superficial fascia measured from the skin to the inferior border of the superficial fascial layer; (2) the contractile layer consisted of RF and VI muscles, including the deep fascia between them, measured from the inside edge of the superior border of RF to the inside edge of the inferior border of VI (Figure 2). These two measurements were a simplified version of the measurement protocol used by [4], which involved making separate measurements of subcutaneous fat, superficial, and deep fascia and muscle thickness; hence, scans from the earlier study were re-analysed using the modified protocol. Each image was measured twice, and the mean values were used in the analysis.
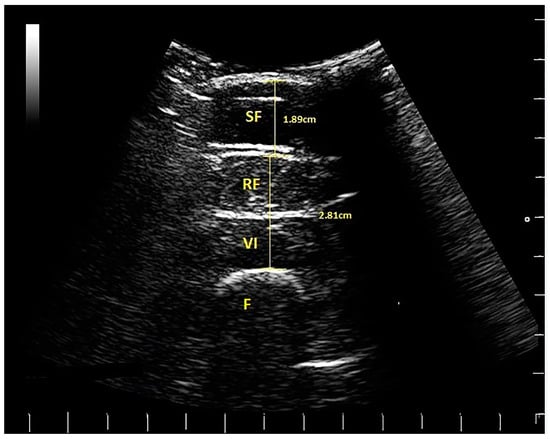
Figure 2.
Ultrasound scan from a female golfer, indicating subcutaneous fat (SF), rectus femoris (RF), vastus intermedius (VI) and the femur (F). The scale on the right and bottom of the scan is in cm (white lines). The thickness of the tissues is indicated (SF = 1.89 cm) and muscle (RF plus VI = 2.81 cm).
2.3. Statistical Analysis
Data collected on the dominant leg in the current study were compared with re-analysed scans from a subset of participants studied by [4], who were predominantly sedentary females aged 66 to 80 years. In the previous study, SAB—an experienced USI operator—had established the intra-rater between-day reliability of the USI technique (i.e., obtaining images and making measurements) [4].
During training prior to the present study, IH examined intra-rater reliability of measuring the same scans (n = 20) on two different days, and examined inter-rater reliability against the experienced investigator (SAB) who measured the same 20 scans. Intra-rater reliability of quadriceps muscle and SF thickness measured by IH was excellent, with an intraclass correlation coefficient (ICC 1,1) of 0.99 (95% confidence intervals (CI) of 0.987 to 0.996) for muscle and 0.99 (95% CI (0.990 to 0.997) for SF. Inter-rater reliability was also excellent: ICC (2,2) of 0.99 (95% CI (0.947 to 0.997) for muscle and 0.99 (95% CI (0.988 to 0.998) for SF.
Data were imported from Microsoft Excel and analysed using SPSS 21 (SPSS Inc., Chicago, IL, USA). Baseline characteristics of the golfers and non-golfers were analysed. Histograms revealed a non-Gaussian distribution for age and BMI for golfers and non-golfers. Therefore, the non-parametric Mann–Whitney U test was used to compare participant characteristics between groups.
Mean values for each soft tissue layer from the two images taken were used in the analysis. Percentage proportions of superficial non-contractile and deep muscle layers to total anterior thigh thickness were calculated. Distribution of ultrasound data was found to be normal using histograms. Independent samples t-tests were used to compare data between the golfers and sedentary older females. Multiple linear regression analyses compared thigh tissue thickness between golfers and non-golfers, whilst controlling for age and BMI.
3. Results
3.1. Participant Characteristics
Mann–Whitney U analysis revealed that the golfers were younger (median = 68 years) than the non-golfers (median = 74), and had lower BMI (golfers median = 24.8 kg/m2; non-golfers median = 27.7), and that these differences were significant (p < 0.0005). The weight of golfers (median = 64) was significantly less (p = 0.002) than that in non-golfers (median = 72.7).
The distribution of age and BMI in the two groups is displayed in Table 2, which shows more golfers in the lower age groups and BMI categories than non-golfers.
Table 2.
Age group and BMI categories of golfers and non-golfers.
All golfers participated in moderate activity at least once a week (n = 31), compared to only 28% (n = 9 of the 32) of non-golfers. Three non-golfers did not complete the PASE. Golfers were moderately active for a median of 3.5 days per week (some doing activities in addition to golf), which was significantly greater (p < 0.0005) than non-golfers (median = 0 days per week), and was intended to compare groups with differing levels of habitual physical activity.
3.2. Ultrasound Parameter Measurements
Independent t-tests revealed that golfers had significantly greater total anterior thigh thickness, higher actual and percentage muscle thickness, higher muscle thickness per kg of body mass, and lower percentage subcutaneous non-contractile tissue compared to non-golfers (Table 3).
Table 3.
Ultrasound measurements of non-contractile and contractile layers of the dominant anterior thigh in golfers and non-golfers.
Difference in percentage contributions between golfers and non-golfers is shown in Figure 3.
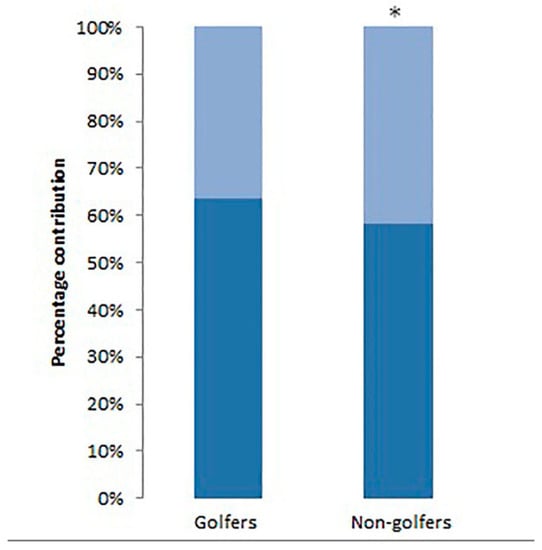
Figure 3.
Percentage contribution of muscle thickness plus deep fascia (dark blue) and subcutaneous fat plus superficial fascia (light blue) in golfers and non-golfers. * Difference between groups was statistically significant (p < 0.05).
Since there were significant differences in characteristics between golfers and non-golfers, multiple linear regression analysis examined the influence of age and BMI on the ultrasound findings. Total anterior thickness was higher in golfers (B = −0.984, p = 0.004), controlling for BMI and age (Table 4). Muscle thickness was also higher in golfers (B = −0.619, p =0.002), so age and BMI did not influence these soft tissue measurements on ultrasound scans.
Table 4.
Multiple regression analysis of ultrasound parameters, controlling for age and body mass index, in golfers and non-golfers.
4. Discussion
The relative contributions of quadriceps muscles and non-contractile tissue (subcutaneous fat and perimuscular fascia) to total anterior thigh thickness were quantified using USI in a group of moderately active older female golfers and were compared with non-golfers. Simple rapid ultrasound measurements showed that the golfers had greater proportions of muscle thickness and leaner thighs than the non-golfers, indicating an association with the moderate activity of recreational golf; however, controlled studies are needed to determine if there is a training effect on the thigh muscles from playing golf. These findings suggest that golf may be sufficient to enable older females to achieve the strengthening effects of moderate activity recommended by the World Health Organisation [16], but the possibility of other factors contributing to the muscle size differences between the groups needs to be studied.
Relative thigh tissue thickness of muscle and SF, measured using ultrasound imaging, may be a useful indicator of musculoskeletal health status. Golfers had a higher percentage of muscle thickness and actual muscle thickness, and a lower percentage of subcutaneous fat and fascia compared to non-golfers (Table 3). This may indicate that moderate activity in older females is associated with leaner thighs (less SF in relation to muscle thickness), which has implications for health and physical function. Muscle thickness (cm) per kg of body mass was higher (p < 0.0005) in golfers (0.44) than non-golfers (0.30). This indicates that in the groups studied, when a golfer and non-golfer of the same weight were compared, the golfer was likely to have (0.14 cm) more muscle per kg in the anterior thigh. The greater muscle thickness in golfers was expected, as golf is known to improve musculoskeletal function [5], but the present findings were the first to provide quantitative evidence of greater muscle size associated with playing golf.
The fact that there were differences in age and BMI between the groups did not explain the differences in tissue thickness measurements. Multiple regression analyses that controlled for the difference in age and BMI between the golfers and non-golfers showed that total anterior thigh thickness was almost 1 cm thicker in golfers compared to non-golfers, and muscle thickness was 0.6 cm thicker in golfers compared to non-golfers. As 28% of the non-golfers participated in moderate activity at least once a week and all volunteers were self-selected, even those who did not participate in moderate activity may be more active than those who would not volunteer for such a study. The difference in relative thigh tissue thickness between active and sedentary females may therefore be even larger when compared to a truly sedentary population.
The reliability and validity of ultrasound measures of thigh tissues have been established. The intra- and inter-rater reliability of muscle and non-contractile tissue thickness measurements made by IH and SAB on the same scans in a preparatory study were excellent (>0.99). Therefore, the thickness measurements in golfers (measured by IH) and non-golfers (measured by SAB) can be compared confidently. Evidence indicates that USI is valid when compared to MRI in the anterior thigh [13], rectus femoris [9], vastus medialis [14], whole quadriceps volume [12], and when measuring subcutaneous fat [11].
There are potential uses of measuring thigh tissue thickness with ultrasound imaging in a number of environments, as the technique is rapid, safe, and cost-effective [9]. Ultrasound is feasible for use in a clinical setting; e.g., to monitor thigh tissue thickness in the aging population to try to identify those losing muscle mass rapidly, who are at risk of functional decline and loss of independence. When monitoring weight loss, USI could ensure fat and not muscle was being lost and conversely during weight gain, that muscle was increasing and not subcutaneous fat. This scenario is also relevant to patients in intensive care to monitor muscle wasting and recovery, as demonstrated by [19].
The previous study of sedentary groups by [4] measured muscle thickness by excluding the inter-muscular fascia between RF and VI, but for ease and efficiency of measuring images in a clinical or field setting, the protocol used in the present study is advised for clinical use. The modified protocol includes the superficial fascia in the subcutaneous fat measurement, and includes the deep fascia in the muscle thickness measurement. This simple method of measuring means that images are easier and quicker to measure, as well as avoiding fascial measurements, which are less reliable than muscle measurements [4].
A limitation of including fascial measurements is that the amount of muscle and subcutaneous tissue will be over-estimated. However, this limitation is outweighed by the benefits of the simpler measuring method, as it may allow clinicians to use ultrasound imaging more regularly. Another limitation of using USI is that it is not possible to measure and subtract intramuscular fat from muscle tissue, so muscle thickness will be overestimated. MRI is considered to be the gold standard for identifying intramuscular fat, and provides a more accurate measure of total fat content [20], but is not feasible in field environments.
The thigh was only measured at one site, so this may not represent the whole thigh. One site was measured in the current study, as this is the protocol that clinicians are likely to follow, due to time constraints. Further research into the number of sites required to reflect whole body composition is warranted.
The present cross-sectional study comparing golfers—who were self-selected—with sedentary controls cannot be used to determine the training effects of golf, which needs to be examined in a randomised controlled prospective trial. Future studies should document levels and different types of physical activity undertaken by participants formally (which was a limitation of the present study), so that the true contribution of golf on training effects can be determined.
Golfers in the present study were compared retrospectively with sedentary controls from a prior related study; therefore, matching controls with golfers was not possible. This resulted in the non-golfers being an average of four years older than the golfers, although the multiple regression analysis did not demonstrate an effect of age on the difference in thigh tissue thickness. In the golfing group, the other moderate activities that some participants undertook could have contributed to the differences in muscle size found. There were also nine participants in the sedentary group who participated in moderate activity at least once a week, which did not represent a truly sedentary population. Other potential differences between the groups that were not examined in the present study include diet, socio-economic status, etc. Such confounding variables will need to be considered in future studies.
Further research is warranted to study relative thigh tissue thickness of other populations, such as females over 80, older male golfers, and active young people of both genders. A comprehensive database could then be used as a guide in clinical practice. It would also be interesting to compare relative thigh tissue thickness of participants in different sports. It would be useful to establish the relationship between tissue thickness of the anterior thigh—assessed at one site—with the rest of the body to determine whether the thigh reflects relative tissue thickness of the whole body. Regarding the training effect of recreational golf on thigh muscle size (an indirect measure of muscle strength), longitudinal studies are needed.
5. Conclusions
Relative thickness of quadriceps muscle was higher and subcutaneous non-contractile tissue thickness lower in moderately active older golfers, compared to less active older females. These findings provide the first objective indication that recreational golf is associated with larger quadriceps muscles (an indicator of strength), so a prospective study is warranted to see if there is a specific strengthening effect of golf, separate from other activities. Relative tissue thickness in the anterior thigh can be assessed simply using ultrasound imaging, which could be useful in clinical and field environments to assess those at risk of frailty and the effects of interventions.
Acknowledgments
The authors thank the participants, the Hampshire golf clubs that helped with recruitment (Corhampton, Chris Cheesman; Cams Hall, Sarah Moore (physiotherapist); Hayling Island, Moira Hoath), and Arthritis Research UK for funding MW as Senior Research Fellow in Biomechanics in the Arthritis Research UK Centre for Sport, Exercise and Osteoarthritis (Grant Reference 20194). The authors also thank fellow MSc students to I.H., Keira Rowsome and Charlotte Buckley, for their assistance with recruitment and screening in relation to their own projects, and Andrew Murray, University of Edinburgh, for his helpful comments on the manuscript.
Author Contributions
All authors conceived and designed the experiments; I.H., S.B. and S.A.-B. performed the experiments, under the supervision of M.S. and D.S.; I.H., S.B. and S.A.B. analysed the data and S.E. provided statistical support; M.W. wrote the Matlab algorithm; I.H. drafted the paper and all other authors contributed to writing the paper; S.B. imported the references into EndNote and M.S. prepared the final manuscript for submission.
Conflicts of Interest
The authors declare no conflict of interest. The funding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Janssen, I. Evolution of sarcopenia research. Appl. Physiol. Nutr. Metab. 2010, 35, 707–712. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine; Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Wroblewski, A.P.; Amati, F.; Smiley, M.A.; Goodpaster, B.; Wright, V. Chronic exercise preserves lean muscle mass in masters athletes. Phys. Sportsmed. 2011, 39, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Agyapong-Badu, S.; Warner, M.; Samuel, D.; Narici, M.; Cooper, C.; Stokes, M. Anterior thigh composition measured using ultrasound imaging to quantify relative thickness of muscle and non-contractile tissue: a potential biomarker for musculoskeletal health. Physiol. Meas. 2014, 35, 2165–2176. [Google Scholar] [CrossRef] [PubMed]
- Parkkari, J.; Natri, A.; Kannus, P.; Mänttäri, A.; Laukkanen, R.; Haapasalo, H.; Oja, P.; Vuori, I. A controlled trial of the health benefits of regular walking on a golf course. Am. J. Med. 2000, 109, 102–108. [Google Scholar] [CrossRef]
- Gao, K.L.; Hui-Chan, C.W.; Tsang, W.W. Golfers have better balance control and confidence than healthy controls. Eur. J. Appl. Physiol. 2011, 111, 2805–2812. [Google Scholar] [CrossRef] [PubMed]
- Farahmand, B.; Broman, G.; de Faire, U.; Vagero, D.; Ahlbom, A. Golf: A game of life and death—Reduced mortality in Swedish golf players. Scand. J. Med. Sci. Sports 2009, 19, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Strasser, E.M.; Draskovits, T.; Praschak, M.; Quittan, M.; Graf, A. Association between ultrasound measurements of muscle thickness, pennation angle, echogenicity and skeletal muscle strength in the elderly. Age 2013, 35, 2377–2388. [Google Scholar] [CrossRef] [PubMed]
- Bemben, M.G. Use of diagnostic ultrasound for assessing muscle size. J. Strength Cond. Res. 2002, 16, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, J.L.; Stokes, M. Ultrasound imaging and muscle function. J. Orthop. Sports Phys. Ther. 2011, 41, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Wagner, D.R. Ultrasound as a tool to assess body fat. J. Obes. 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Miyatani, M.; Kanehisa, H.; Kuno, S.; Nishijima, T.; Fukunaga, T. Validity of ultrasonograph muscle thickness measurements for estimating muscle volume of knee extensors in humans. Eur. J. Appl. Physiol. 2002, 86, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Sanada, K.; Kearns, C.F.; Midorikawa, T.; Abe, T. Prediction and validation of total and regional skeletal muscle mass by ultrasound in Japanese adults. Eur. J. Appl. Physiol. 2006, 96, 24–31. [Google Scholar] [CrossRef]
- Worsley, P.R.; Kitsell, F.; Samuel, D.; Stokes, M. Validity of measuring distal vastus medialis muscle using rehabilitative ultrasound imaging versus magnetic resonance imaging. Man. Ther. 2014, 19, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Kanehisa, H.; Ikegawa, S.; Fukunaga, T. Comparison of muscle cross-sectional area and strength between untrained women and men. Eur. J. Appl. Physiol. 1994, 68, 148–154. [Google Scholar] [CrossRef]
- World Health Organisation. Global Recommendations on Physical Activity for Health: 65 Years and Above; World Health Organisation: Geneva, Switzerland, 2011. [Google Scholar]
- Murray, A.; Daines, L.; Archibald, D.; Hawkes, R.; Schiphorst, C.; Kelly, P.; Grant, L.; Mutrie, N. The relationship and effects of golf on physical and mental health: A scoping review. Br. J. Sports Med. 2016. [Google Scholar] [CrossRef] [PubMed]
- Delaney, S.; Worsley, P.; Warner, M.; Taylor, M.; Stokes, M. Assessing contractile ability of the quadriceps muscle using ultrasound imaging. Muscle Nerve 2010, 42, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Gruther, W.; Benesch, T.; Zorn, C.; Paternostro-Sluga, T.; Quittan, M.; Fialka-Moser, V.; et al. Muscle wasting in intensive care patients: ultrasound observation of the M. quadriceps femoris muscle layer. J. Rehabil. Med. 2008, 40, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.M.; Galloway, G.J.; Jull, G.A.; Noteboom, J.T.; Centeno, C.J.; Gibbon, W.W. Magnetic resonance imaging analysis of the upper cervical spine extensor musculature in an asymptomatic cohort: An index of fat within muscle. Clin. Radiol. 2005, 60, 355–363. [Google Scholar] [CrossRef] [PubMed]
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).