
Ex-Vivo Evaluation of “First Tip Closing” Radiofrequency Vessel Sealing Devices for Swine Small Intestinal Transection




Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Samples
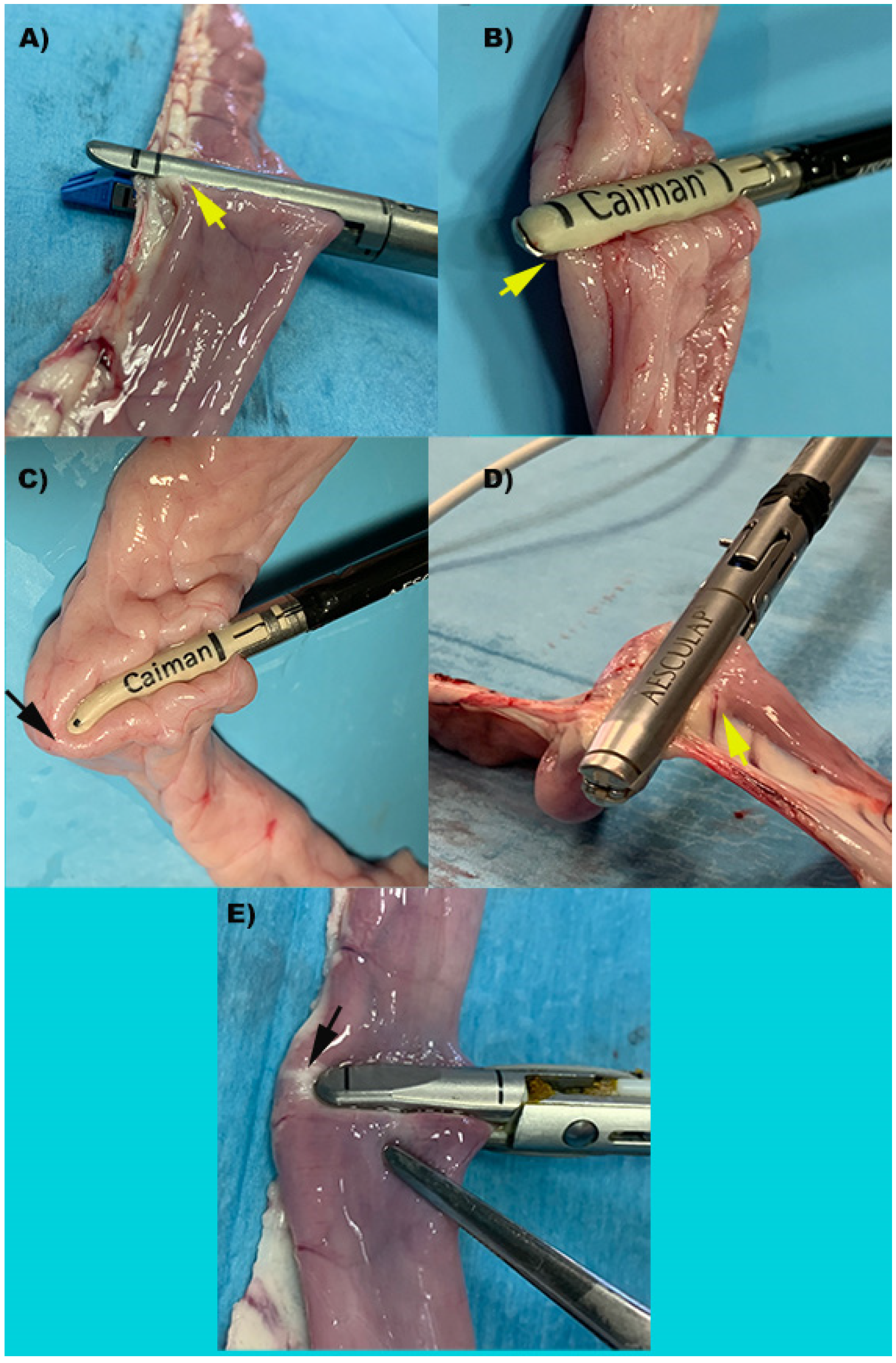
2.2. Experimental Groups
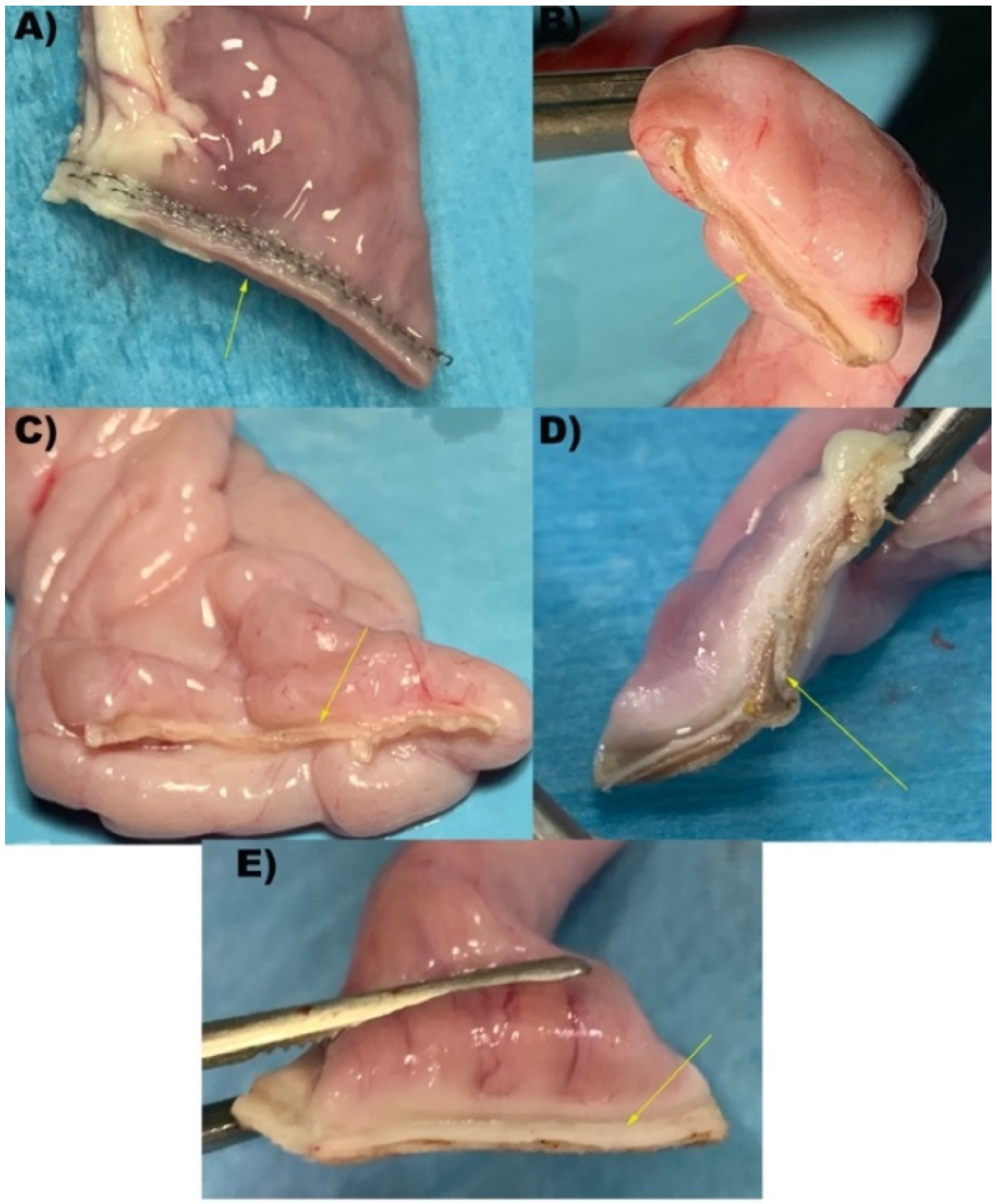
2.3. Sample Constructs & Burst Pressures
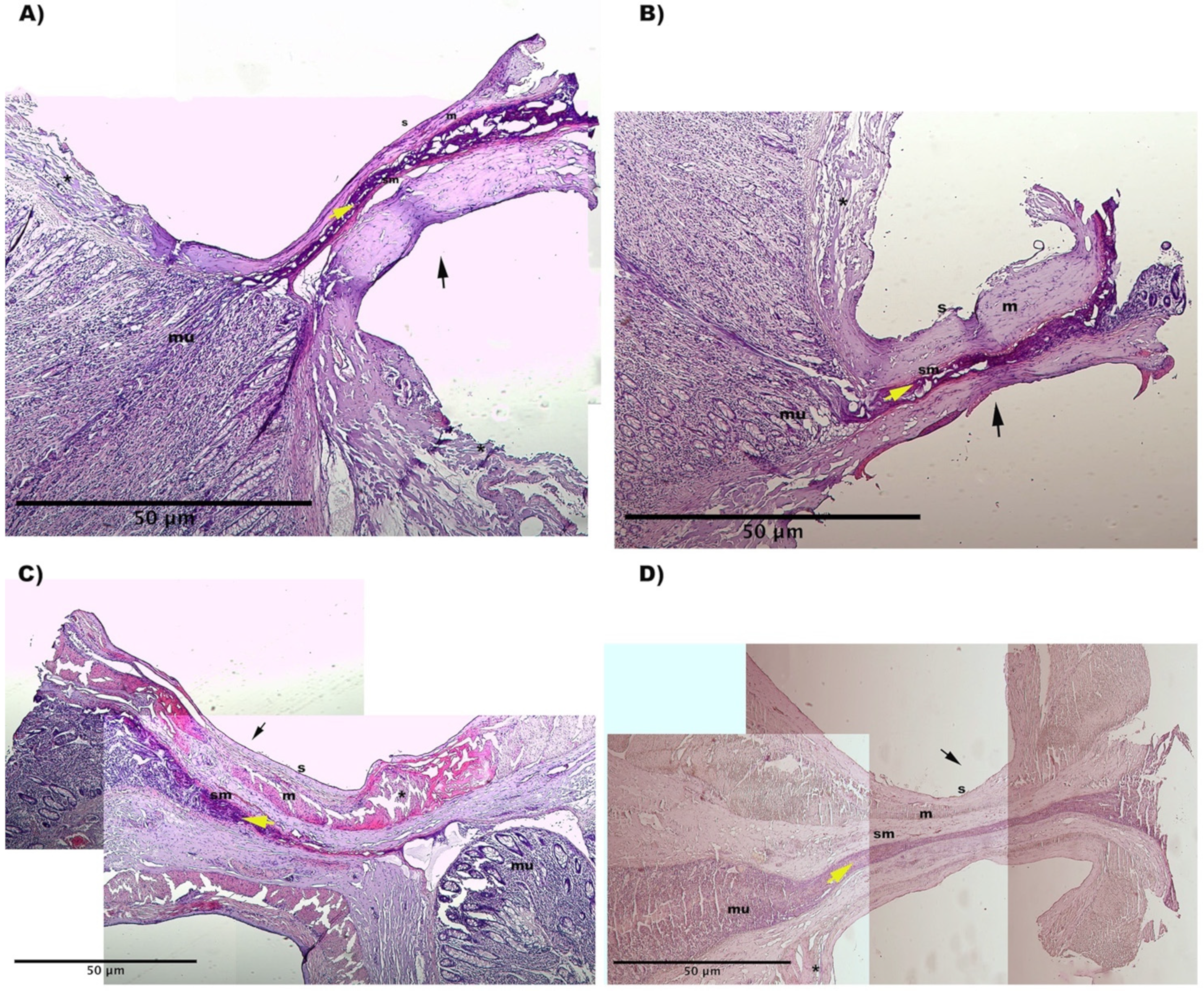
2.4. Histology
2.5. Statistical Analysis
3. Results
3.1. Number of Activations
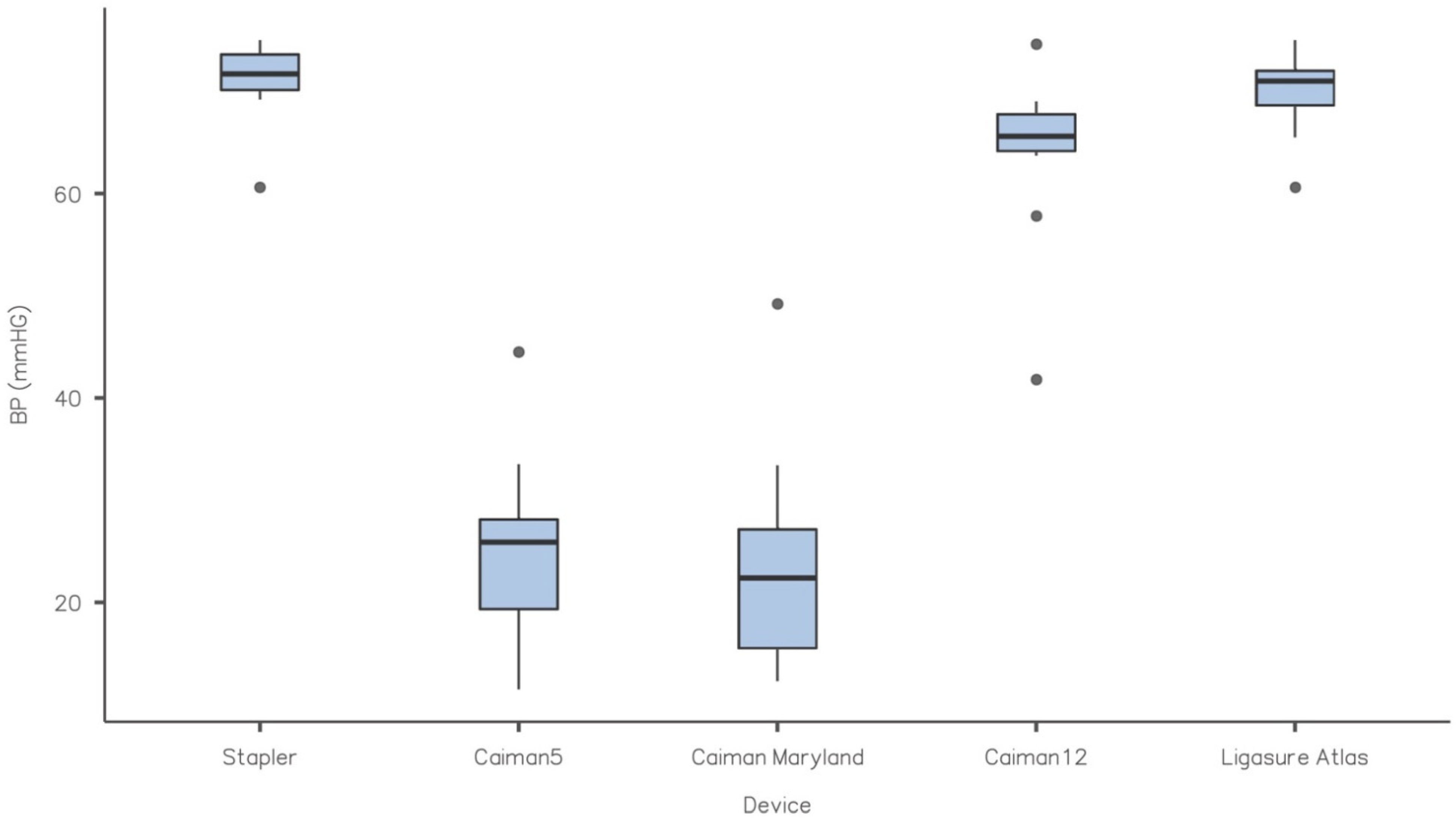
3.2. Burst Pressure
3.3. Hystology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arya, S.; Mackenzie, H.; Hanna, G.B. Non-vascular experimental and clinical applications of advanced bipolar radiofrequency thermofusion technology in the thorax and abdomen: A systematic review. Surg. Endosc. 2015, 29, 1659–1678. [Google Scholar] [CrossRef] [PubMed]
- Arya, S.; Hadjievangelou, N.; Lei, S.; Kudo, H.; Goldin, R.D.; Darzi, A.W.; Elson, D.S.; Hanna, G.B. Radiofrequency-induced small bowel thermofusion: An ex vivo study of intestinal seal adequacy using mechanical and imaging modalities. Surg. Endosc. 2013, 27, 3485–3496. [Google Scholar] [CrossRef] [PubMed]
- Santini, M.; Fiorelli, A.; Messina, G.; Laperuta, P.; Mazzella, A.; Accardo, M. Use of the LigaSure device and the Stapler for closure of the small bowel: A comparative ex vivo study. Surg. Today 2013, 43, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Smulders, J.F.; de Hingh, I.H.; Stavast, J.; Jackimowicz, J.J. Exploring new technologies to facilitate laparoscopic surgery: Creating intestinal anastomoses without sutures or staples, using a radio-frequency-energy-driven bipolar fusion device. Surg. Endosc. 2007, 21, 2105–2109. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tagkalos, E.; Heimann, A.; Gaiser, T.; Hirsch, D.; Gockel, I.; Lang, H.; Jansen-Winkeln, B. Cecal Resection with Bipolar Sealing Devices in a Rat Model. J. Investig. Surg. 2020, 33, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.T.; Yang, T.H.; Deng, X.B.; Meng, W.J.; Han, J.H.; Zhou, Z.G.; Wang, Z.Q. Laparoscopic colorectal anastomosis technique without ‘‘dog ear’’ formation using LigaSure for bowel transection. Tech. Coloproctol. 2019, 24, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, A.; Bulus, H.; Tas, A.; Aydin, A. Evaluation of Stump Pressure in Three Types of Appendectomy: Harmonic Scalpel, LigaSure, and Conventional Technique. J. Laparoendosc. Adv. Surg. Tech. A 2016, 26, 950–953. [Google Scholar] [CrossRef] [PubMed]
- Gehrig, T.; Billeter, A.T.; Wekerle, A.L.; Shevchenko, M.; Brand, K.; Muller-Stich, B.P. Evaluation of the LigaSure™ Vessel Sealing System for bowel transection and intestinal anastomosis-an experimental study in a porcine model. Langenbecks Arch. Surg. 2016, 401, 381–387. [Google Scholar] [CrossRef]
- Himpens, J.; Leman, G.; Sonneville, T. Laparoscopic Roux-en-Y gastric bypass performed without staples. Surg. Endosc. 2005, 19, 1003. [Google Scholar] [CrossRef]
- Kawahara, H.; Watanabe, K.; Tomoda, M.; Enomoto, H.; Akiba, T.; Yanaga, K. Single-incision clipless laparoscopic total colectomy. Hepatogastroenterology 2014, 61, 453–455. [Google Scholar]
- Moreno-Sanz, C.; Picazo-Yeste, J.; Seoane-Gonzales, J.; Manzanera-Diaz, M.; Tadeo-Ruiz, G. Division of the small bowel with the LigaSure Atlas device during the right laparoscopic colectomy. J. Laparoendosc. Adv. Surg. Tech. A 2008, 18, 99–101. [Google Scholar] [CrossRef]
- Rumbaugh, M.L.; Burba, D.J.; Natalini, C.; Hosgood, G.; Moore, R.M. Evaluation of a vessel-sealing device for small intestinal resection and anastomosis in normal horses. Veter Surg. 2003, 32, 574–579. [Google Scholar] [CrossRef]
- Sanchez Trejo, H.A.; Hakakian, D.; Rolandelli, R.H.; Nouri, A.M.; Antonioli, L.; Nemeth, Z.H. “Cecal Resection with Bipolar Sealing in a Rat Model”: A Promising Approach for Future Human Studies. J. Investig. Surg. 2020, 33, 67–68. [Google Scholar] [CrossRef]
- Sanchez-De Pedro, F.; Moreno-Sanz, C.; Morandeira-Rivas, A.; Tenias-Burillo, J.M.; Alhambra-Rodriguez De Guzman, C. Colorectal anastomosis facilitated by the use of the LigaSure® sealing device: Comparative study in an animal model. Surg. Endosc. 2014, 28, 508–514. [Google Scholar] [CrossRef]
- Santini, M.; Fiorelli, A.; Messina, G.; Mazzella, A.; Accardo, M. The Feasibility of LigaSure to Create Intestinal Anastomosis: Results of Ex Vivo Study. Surg. Innov. 2015, 22, 266–273. [Google Scholar] [CrossRef]
- Winter, H.; Holmer, C.; Buhr, H.J.; Lindner, G.; Lauster, R.; Kraft, M.; Ritz, J.P. Pilot study of bipolar radiofrequency-induced anastomotic thermofusion-exploration of therapy parameters ex vivo. Int. J. Color. Dis. 2010, 25, 129–133. [Google Scholar] [CrossRef]
- Lacitignola, L.; Imperante, A.; Trisciuzzi, R.; Zizzo, N.; Crovace, A.M.; Staffieri, F. Swine Small Intestine Sealing Performed by Different Vessel Sealing Devices: Ex-Vivo Test. Vet. Sci. 2021, 8, 34. [Google Scholar] [CrossRef]
- Chekan, E.G.; Davison, M.A.; Singleton, D.W.; Mennone, J.Z.; Hinoul, P. Consistency and sealing of advanced bipolar tissue sealers. Med. Devices 2015, 8, 193–199. [Google Scholar] [CrossRef]
- Chen, R.K.; Chastagner, M.W.; Geiger, J.D.; Shih, A.J. Bipolar electrosurgical vessel-sealing device with compressive force monitoring. J. Biomech. Eng. 2014, 136, 061001. [Google Scholar] [CrossRef]
- Eick, S.; Loudermilk, B.; Walberg, E.; Wente, M.N. Rationale, bench testing and in vivo evaluation of a novel 5 mm laparoscopic vessel sealing device with homogeneous pressure distribution in long instrument jaws. Ann. Surg. Innov. Res. 2013, 7, 15. [Google Scholar] [CrossRef]
- Holmer, C.; Winter, H.; Kroger, M.; Nagel, A.; Jaenicke, A.; Lauster, R.; Kraft, M.; Buhr, H.J.; Ritz, J.P. Bipolar radiofrequency-induced thermofusion of intestinal anastomoses--feasibility of a new anastomosis technique in porcine and rat colon. Langenbecks Arch. Surg. 2011, 396, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Okhunov, Z.; Yoon, R.; Lusch, A.; Spradling, K.; Suarez, M.; Kaler, K.S.; Patel, R.; Hwang, C.; Osann, K.; Huang, J.; et al. Evaluation and Comparison of Contemporary Energy-Based Surgical Vessel Sealing Devices. J. Endourol. 2018, 32, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Henze, L.J.; Koehl, N.J.; Bennett-Lenane, H.; Holm, R.; Grimm, M.; Schneider, F.; Weitschies, W.; Koziolek, M.; Griffin, B.T. Characterization of gastrointestinal transit and luminal conditions in pigs using a telemetric motility capsule. Eur. J. Pharm. Sci. 2021, 156, 105627. [Google Scholar] [CrossRef] [PubMed]
- Chaikomin, R.; Wu, K.L.; Doran, S.; Jones, K.L.; Smout, A.J.; Renooij, W.; Holloway, R.H.; Meyer, J.H.; Horowitz, M.; Rayner, C.K. Concurrent duodenal manometric and impedance recording to evaluate the effects of hyoscine on motility and flow events, glucose absorption, and incretin release. Am. J. Physiol. Gastrointest. Liver Physiol. 2007, 292, G1099–G1104. [Google Scholar] [CrossRef]
- Ellison, G.W. Intestinal obstruction. In Disease Mechanisms in Small Animal Surgery, 2nd ed.; Bojrab, M.J., Ed.; Lea & Febiger: Philadelphia, PA, USA, 1993; pp. 252–257. [Google Scholar]
- Elemen, L.; Yazir, Y.; Akay, A.; Boyacioglu, Z.; Ceyran, B.; Ceylan, S. Comparison of bipolar electrosurgical devices with ligatures and endoclips in the rat appendicitis model. J. Pediatr. Surg. 2011, 46, 1923–1929. [Google Scholar] [CrossRef]
- Pan, H.; Leung, K.K.C.; Ng, E.K.W. Tissue fusion technology versus suture and staple in porcine bowel anastomosis: An in vivo study. Braz. J. Med. Biol. Res. 2020, 53, e9305. [Google Scholar] [CrossRef]
- Kramer, E.A.; Rentschler, M.E. Energy-Based Tissue Fusion for Sutureless Closure: Applications, Mechanisms, and Potential for Functional Recovery. Annu. Rev. Biomed. Eng. 2018, 20, 1–20. [Google Scholar] [CrossRef]
- Gadiyaram, S.; Nachiappan, M. LigaSure Vessel Sealing System for Small Bowel Transection During Roux Limb Construction. Cureus 2022, 14, e21287. [Google Scholar] [CrossRef]
- Gehrig, T.; Knebel, P.; Scheel, V.; Hinz, U.; Seiler, C.M.; Muller-Stich, B.P.; Buchler, M.W.; Gutt, C.N. LigaSure Impact versus conventional dissection technique in pylorus-preserving pancreatoduodenectomy in clinical suspicion of cancerous tumours on the head of the pancreas: Study protocol for a randomised controlled trial. Trials 2011, 12, 162. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BP (mmHg) | |||||
|---|---|---|---|---|---|
| Device | Mean | Median | SD | Minimum | Maximum |
| Stapler | 71.0 | 71.7 | 4.15 | 60.6 | 75.0 |
| Caiman5 | 25.5 | 25.9 | 9.25 | 11.5 | 44.5 |
| Caiman Maryland | 24.0 | 22.4 | 11.25 | 12.3 | 49.2 |
| Caiman12 | 63.9 | 65.6 | 8.82 | 41.8 | 74.6 |
| Ligasure Atlas | 70.0 | 71.0 | 4.27 | 60.6 | 75.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lacitignola, L.; Crovace, A.; Passantino, G.; Staffieri, F. Ex-Vivo Evaluation of “First Tip Closing” Radiofrequency Vessel Sealing Devices for Swine Small Intestinal Transection. Vet. Sci. 2022, 9, 445. https://doi.org/10.3390/vetsci9080445
Lacitignola L, Crovace A, Passantino G, Staffieri F. Ex-Vivo Evaluation of “First Tip Closing” Radiofrequency Vessel Sealing Devices for Swine Small Intestinal Transection. Veterinary Sciences. 2022; 9(8):445. https://doi.org/10.3390/vetsci9080445
Chicago/Turabian StyleLacitignola, Luca, Alberto Crovace, Giuseppe Passantino, and Francesco Staffieri. 2022. "Ex-Vivo Evaluation of “First Tip Closing” Radiofrequency Vessel Sealing Devices for Swine Small Intestinal Transection" Veterinary Sciences 9, no. 8: 445. https://doi.org/10.3390/vetsci9080445
APA StyleLacitignola, L., Crovace, A., Passantino, G., & Staffieri, F. (2022). Ex-Vivo Evaluation of “First Tip Closing” Radiofrequency Vessel Sealing Devices for Swine Small Intestinal Transection. Veterinary Sciences, 9(8), 445. https://doi.org/10.3390/vetsci9080445