1. Introduction
Otitis media is one of the most common infectious diseases in younger calves [
1,
2,
3]. The diagnosis of bovine otitis media is commonly obtained through specific clinical signal appearance and laboratory tests such as isolation of pathogenic microorganisms from deep nasal pharyngeal swabs and bronchial alveolar lavage [
3,
4]. Radiography is the traditional common imaging modality used to observe otitis media, although it provides inferior image quality where the structures of the ear and tympanic bulla are both difficult to distinguish [
2,
3,
4]. Additionally, the radiographic technique taken obliquely at 20° is required for visualizing each structure of the tympanic bulla, which prevents overlapping between targeted tympanic bulla and the peripheral osseous structures or opposite tympanic bulla [
2,
4,
5]. More recently, computed tomography (CT) has been touted as the gold standard ante mortem diagnostic imaging tool for bovine otitis media, providing a simultaneous evaluation of both the accumulation of exudates into the lumen of the tympanic bulla, and the osseous changes in tympanic bulla, such as extension, osteolysis, and osteoproliferation on the same section [
2,
4]. Thus, CT is superior to radiography in its diagnostic sensitivity and specificity [
4,
5]. However, few bovine reports have previously described the utility of CT in preoperative evaluation [
6,
7].
Continuous, long-term administration of antibiotics and anti-inflammatory drugs is the first choice of treatment for bovine otitis media [
1,
6,
7,
8,
9]. Irrigation into the affected tympanic cavity is chosen as an advanced conservative therapy [
1,
10]. The irrigation procedure—myringotomy—is commonly achieved via a perforation made in the tympanic membrane using a sharp metal needle inserted into the ear canal [
1]. As part of a modified myringotomy, an indwelling needle intravenous cannula has been previously utilized to perforate the tympanic membrane for subsequent irrigation, with pressure generated by a syringe [
11]. Some practitioners have performed high-pressure irrigation into the tympanic cavity using a continuous drench gun, with an oral jet irrigator modified from the human otologic therapy, obtaining the simultaneous effects of myringotomy and intra-ear irrigation [
11,
12,
13,
14]. High-pressure irrigation using a continuous drench gun could contribute to a higher healing rate (73.3%) than that of myringotomy (25.0%) [
12]. Conversely, high-pressure irrigation utilizing a modified myringotomy allowed for a higher healing rate than the drench gun technique, with rates of 87.5% vs. 53.3%, respectively [
11]. These two high-pressure irrigation techniques, when carried out two to three times during one procedure with 20 mL irrigation fluid, can result in unfavorable outcomes if irrigation fluids are not allowed to discharge from the nasal cavity, following passage through the Eustachian tube [
11,
12]. Additionally, though rare, high-pressure irrigation can lead to critical complications, as it may induce severe destruction of the tympanic bulla and cause traumatic inflammation within the inner ear [
11,
12]. In domestic ruminants, conservative therapy can commonly lead to therapeutic success for acute otitis media [
10]. However, surgical treatment is sometimes required in animals with chronic or end-stage otitis media, which is difficult to treat using these conservative treatments [
15].
In previous cases, affected calves have been treated with bulla osteotomy using lateral and ventral approaches [
6,
7,
8,
16,
17,
18]. Two types of lateral bulla osteotomy (LBO) have been reported. One LBO procedure was total ear canal ablation followed by curetting of the neighboring lateral surface of the tympanic bulla, this being the common method performed on sick ruminants such as llama, alpaca, camelid, buffalo, bison, and bongo [
10,
13,
19,
20,
21,
22]. The other previously documented LBO procedure was conducted by the following steps: (1) an incision was made in the lower area of the ear; (2) the surgical opening was extended deeply by blunt dissection, allowing the exposure of the lateral wall of the tympanic bulla in the deeper site of the stylohyoid bone; and (3) perforation of the lateral wall of the tympanic bulla was made via the surgical opening [
17,
18]. However, these methods are so invasive that they generate a high probability of postoperative complications such as neurological disturbances, e.g., issues with the facial nerve, hypoglossal nerve, and vestibular nerve [
10,
15,
20]. Thus, care should be taken to avoid injury of the facial arteries and nerves located on the surgical courses while performing both types of LBOs [
15,
16,
17]. Additionally, LBOs with total ear canal ablation are applicable to ruminants with concurrent involvements of otitis externa and otitis media/interna, allowing the removals of both lesions [
10,
15]. Total ear canal ablation has no therapeutic effect for the bovine cases commonly presenting with otitis media (without otitis externa), caused by the spread of the pathogen via the Eustachian tube from the area of the nasopharynx [
8,
10,
23].
Some previous reports have discussed ventral bulla osteotomy (VBO) as a minor surgical option in bovine otitis media, including detailed methodological explanations [
6,
7]. Regardless of whether LBO or VBO is chosen as a surgical intervention, surgical planning should be supported by preoperative evaluations of the affected tympanic bulla; such planning can determine whether there is unilateral or bilateral involvement, which side is affected in unilateral cases, and the degree of extension and destruction. These pathological changes in the affected tympanic bulla can be effectively detected using imaging examinations, supporting therapeutic decisions such as whether surgical intervention is required, the selection of suitable surgical techniques for each case, and diagnostic uses [
2,
3,
4,
5,
6,
10,
11,
15,
17,
19,
20,
21,
24]. In terms of the convenient imaging modalities used in bovine practice, many previous reports have described the clinical applicability of radiography, computed tomography (CT), or ultrasonography [
2,
3,
4,
5,
6,
10,
11,
15,
17,
19,
20,
21,
24]. This study aims to explain the role of CT evaluation prior to performing VBO in three calves with unilateral otitis media and discuss the applicability of CT. Additionally, this study includes the technical explanation of our VBO procedures, applied through a different surgical route to those carried out in previous bovine practice procedures [
6,
7] but one which is identical to the common VBO procedure in small-animal practice [
23,
25]. This technical explanation is followed by a discussion of CTs applicability and the problematic points of the present VBO procedure in comparison to the previous procedure, based on satisfactory or unsatisfactory outcomes.
4. Discussion
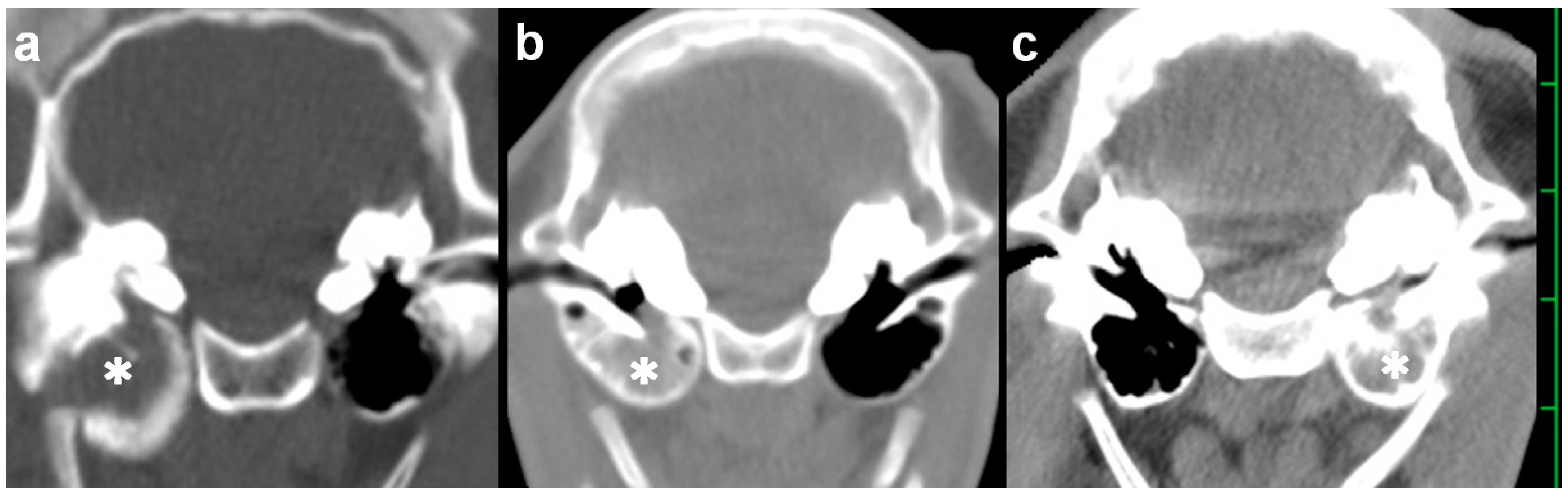
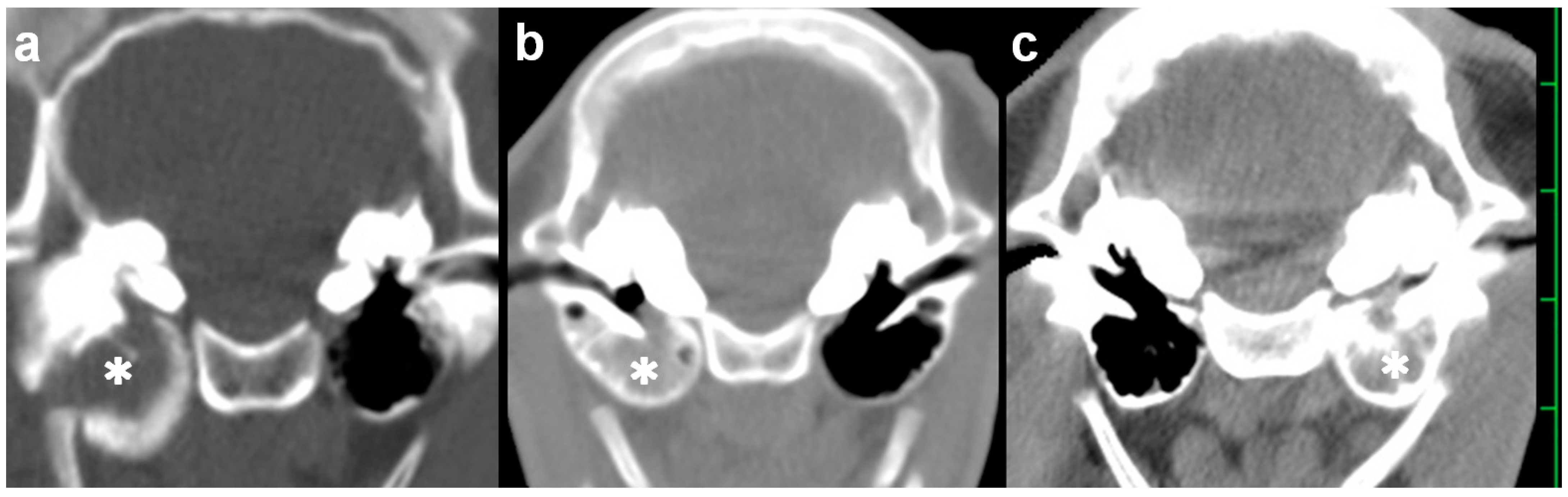
Radiography is a routinely used imaging modality, providing distinctive findings of bovine otitis media, as represented by osseous changes in the affected tympanic bulla. These include thickened walls or osteolysis and increased soft tissue opacity, which is clearly distinguishable from the radiolucent lumen of the normally air-filled tympanic bulla [
2,
5,
17,
20]. Contrast radiography has previously confirmed the presence of a rupture in the tympanic membrane [
19]. However, these radiographic characteristics can be difficult to demonstrate due to the visual obstacles of the peripheral skull’s structures and superimposition between both sides of the tympanic bulla [
2,
5]. The visual limitation can be resolved by observations of the lateral, ventrodorsal, and oblique radiographic views when taken from multiple directions of X-ray irradiation, despite the difficulty in proper positioning and requirement of sedation or anesthesia for the examined animals [
5]. Compared with radiography, CT is considered the gold standard in antemortem examinations, as it enables the visualization of both tympanic bullae without their superimposition on the transverse section when scanned once in the same position of the anesthetized animals [
5,
20,
24]. Ultrasonography also has a high diagnostic potential for bovine otitis media, with a sensitivity of 32–63% and specificity of 84–100% [
24]. The ultrasonographic findings concerning bovine otitis media could be characterized mostly by the accumulations of the echogenic, heterogeneous contents within the lumens deeper than the hyperechoic walls, and a little by the irregular, thickened contours, and deformation of the walls [
24]. However, ultrasonography may have less potential for surgical planning [
11].
Bovine cases of otitis media commonly involve bilateral lesions within the tympanic bulla, even if presenting unilateral clinical signs; the prevalence of bilateral affection in animals with otitis media accounted for 60–70% [
2,
3,
5]. In the three cases above, preoperative CT evaluations could provide positive evidence in judgments of surgical intervention using VBO, as the CT characteristics of otitis media were found unilaterally. The use of VBO led to a successful result in a previous calf with bilateral otitis media [
6]. However, different surgical openings should be made for approaching each affected tympanic bulla; two VBO procedures can be carried out for both ears using the same dorsal recumbent position. Simply, this means the surgical time is doubled when performing VBO for bilateral otitis media. The level of surgical invasion can increase depending on the openings made on both sides of the neck. If LBO is the choice of surgical option for bilateral otitis media, a positional change is required so that the treated ear faces upwards while positioned in lateral recumbency. Thus, to reduce surgical invasion, unilateral involvements of otitis media should be identified preoperatively, followed by the detection of the lesion’s side, regardless of whether the condition is treated with LBO or VBO. In this respect, CT would be superior to radiography.
Radiography has previously been applied slightly obliquely to the skull of the anesthetized, recumbent animal, while keeping a metal landmark placed on its surface ventrally than the ear, before treatment with LBO [
17]. Based on the relative location between the landmark and the affected tympanic bulla on the preoperative radiographic findings, accurately deciding whether to take the surgical route could contribute to minimizing operative invasion; a 5 cm skin incision could allow a pinpoint approach, compared with the common technique of LBO, in which a large, T-shaped skin incision is required for the wider surgical opening, as created by a >7 cm dorsoventral incision, followed by a >7 cm transverse incision made caudally from the dorsoventral cut line [
17,
18]. However, the LBO procedure has not been planned solely through using radiography, because of the difficulty in the evaluation of the degrees of extension and the changed shape of the affected tympanic bulla [
17].
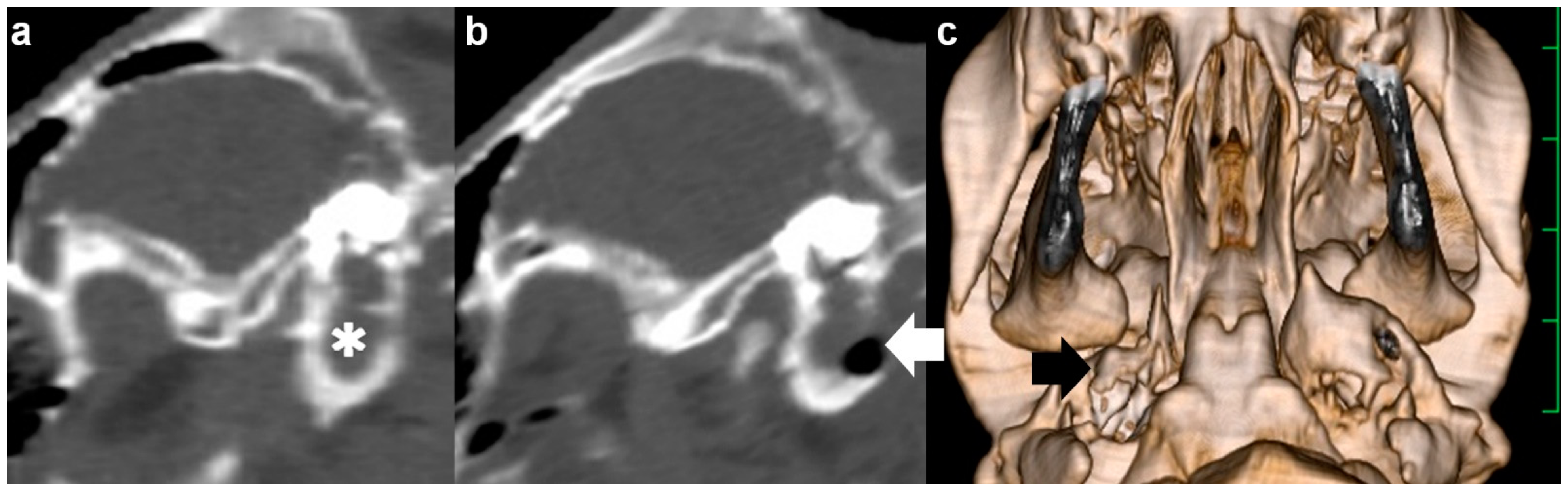
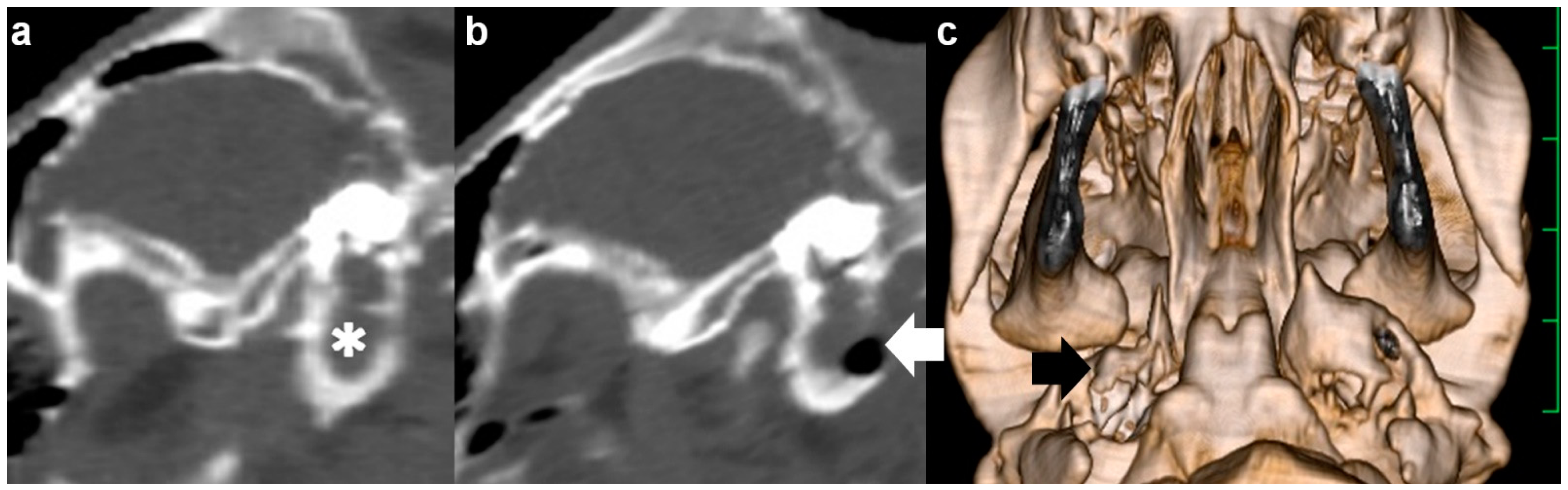
In bovines, chronic development of otitis media is a frequent cause of invasion of the peripheral structures [
3]. Extension of the affected tympanic bulla is a typical osseous change associated with this disease’s chronicity, allowing mechanical loosening of the mobile function of the mandible within the temporomandibular joint [
5]. Osteolytic changes that develop simultaneously within the extended tympanic bulla are the possible cause of infectious invasion to the meninges, together with elevated middle- and inner-ear pressure [
3,
5]. CT can provide sections from every direction and three-dimensional images can be built up through the reconstruction of consecutive scans, as well as the basic axial sections [
26,
27]. This function can allow the identification of the morphological relationship between the primary and secondary lesions, and the degree of the lesion’s extension, in diagnosis of various head diseases, inducing osseous abnormalities [
26,
27]. As demonstrated in this study, the measurements of the length and width in the middle-ear structures can confirm the severity of the extensive and destructive changes, providing useful evidence for surgical planning [
4,
5]. Additionally, in the evaluation of the CT values of osseous changes associated with otitis media with effusion, the reduced Hounsfield units display the increased severity of osteolytic changes, fragility, and the decreased degree of hardness of the walls of the tympanic bulla [
28]. Based on these parameters, the preoperative, quantitative evaluation of CT is very helpful for determining whether to choose surgical therapy, selecting the preferable equipment, i.e., an electric or manual drill, and making preoperative decisions concerning the size and location of perforation made on the surface of the tympanic bulla [
4,
5]. In this study, despite the preoperative CT evaluations, a successful result from surgical intervention was obtained for one of the three cases; Case 1 showed a satisfactory outcome but Cases 2 and 3 died on the 10th postoperative day and during surgery, respectively. However, the unsatisfactory results in Case 2 and 3 can provide positive feedback in terms of surgical improvements in cases of bovine otitis media. The unsatisfactory outcome in Case 2 indicated that VBO might have less therapeutic efficacy for more severe cases of bovine otitis media. Case 2 presented with horizontal nystagmus, one of the critical vestibular signs, and showed a high neurological severity (score 7) [
7,
8,
9,
10]. A neurological score ≤ 5 is usually related to satisfactory results after two weeks of medical treatments for otitis media [
9]. Severity of the clinical signs could also be related to the prognoses in the bovine cases treated with high-pressure irrigation, resulting in the different satisfactory outcomes in mild and severe cases (91.2% vs. 43.5%, respectively) [
14]. Thus, clinical severity criteria should be identified to determine whether VBO is indicated while being evaluated by CTs.
In Case 3, the present VBO procedure induced abnormal cardiac rhythms, characterized as an alternation between tachycardia and cardiac arrest, resulting in intraoperative death. Despite never being reported in bovine practice, this phenomenon may be explained by a previous human case study [
29]. The vagus nerve may be the efferent pathway responsible for bradycardia and cardiac arrest through the mechanical stimulation of the nerve and respiratory tract during endotracheal intubation and tracheal suction [
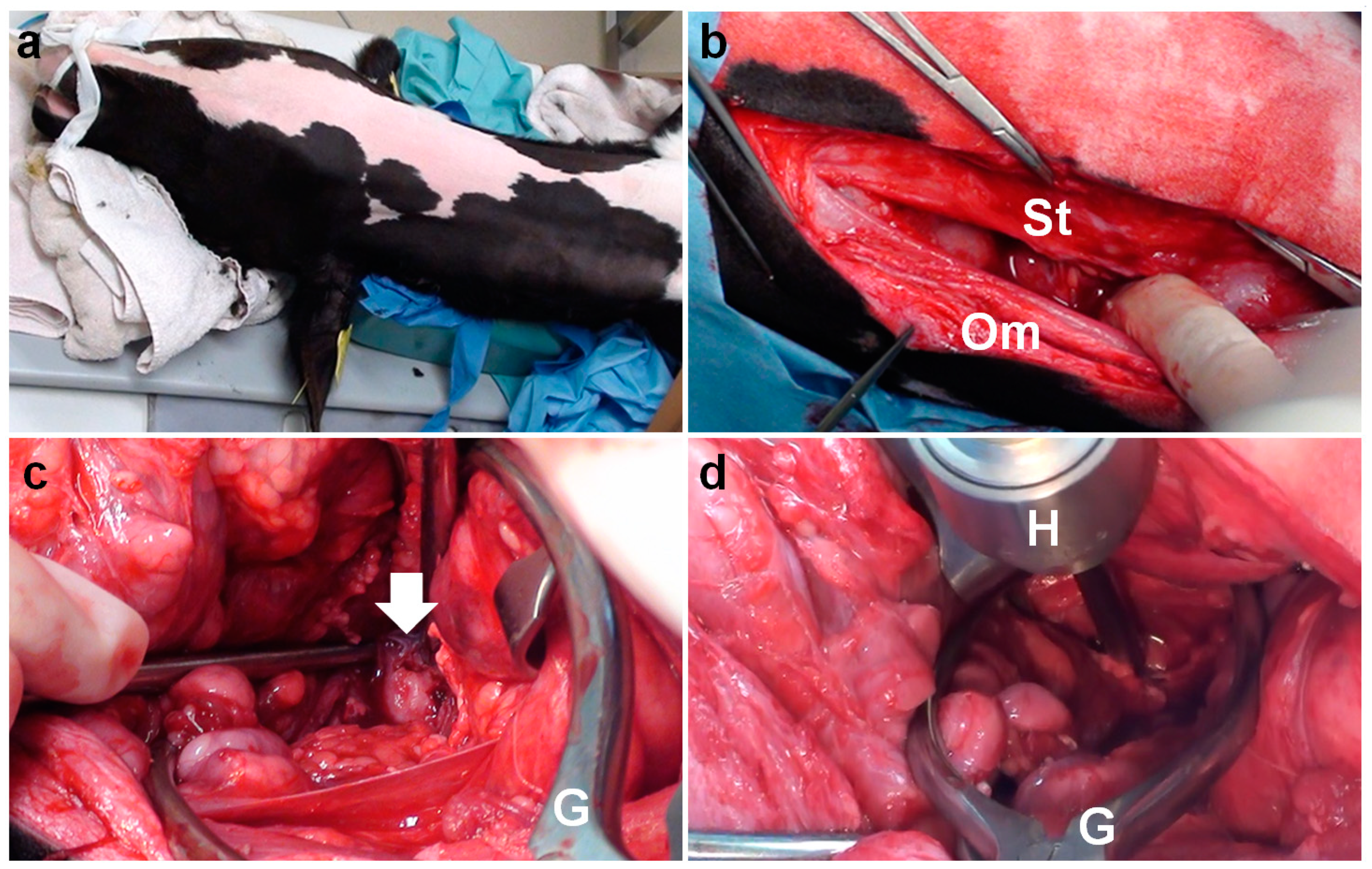
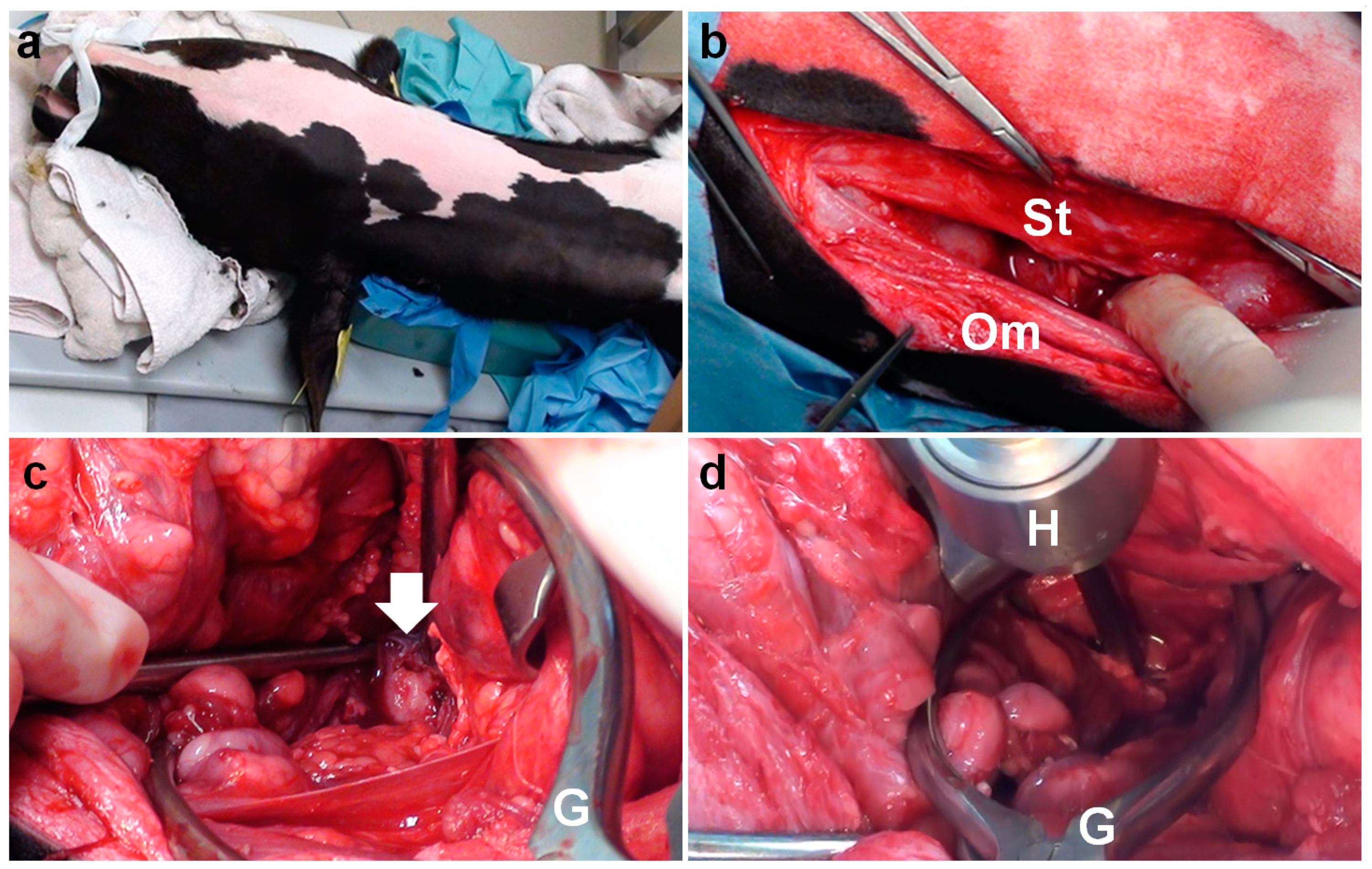
29]. In the present VBO procedure, incisions were made caudally to the area of the thyroid cartilage. This is distinct from the previous procedure of VBO, in which an incision is made cranially to the area of the thyroid cartilage, in the anatomical space between the vertical ramus of the mandible and the paracondylar process of the occipital bone [
6,
7]. Thus, the difference between the previous and present procedures is in the main muscular layers presented on the surgical routes between the incision and the tympanic bulla. In the previous VBO procedure, these layers included the digastricus muscle (grouped in the muscles of mastication), and the hyoglossal and styloglossal muscles (grouped in the extrinsic lingual muscles), while in the present VBO procedure, these layers consisted of the sternothyroid muscle (grouped in the extrinsic laryngeal muscles) and the omohyoid muscle (grouped in the hyoid muscles) [
6,
7,
30,
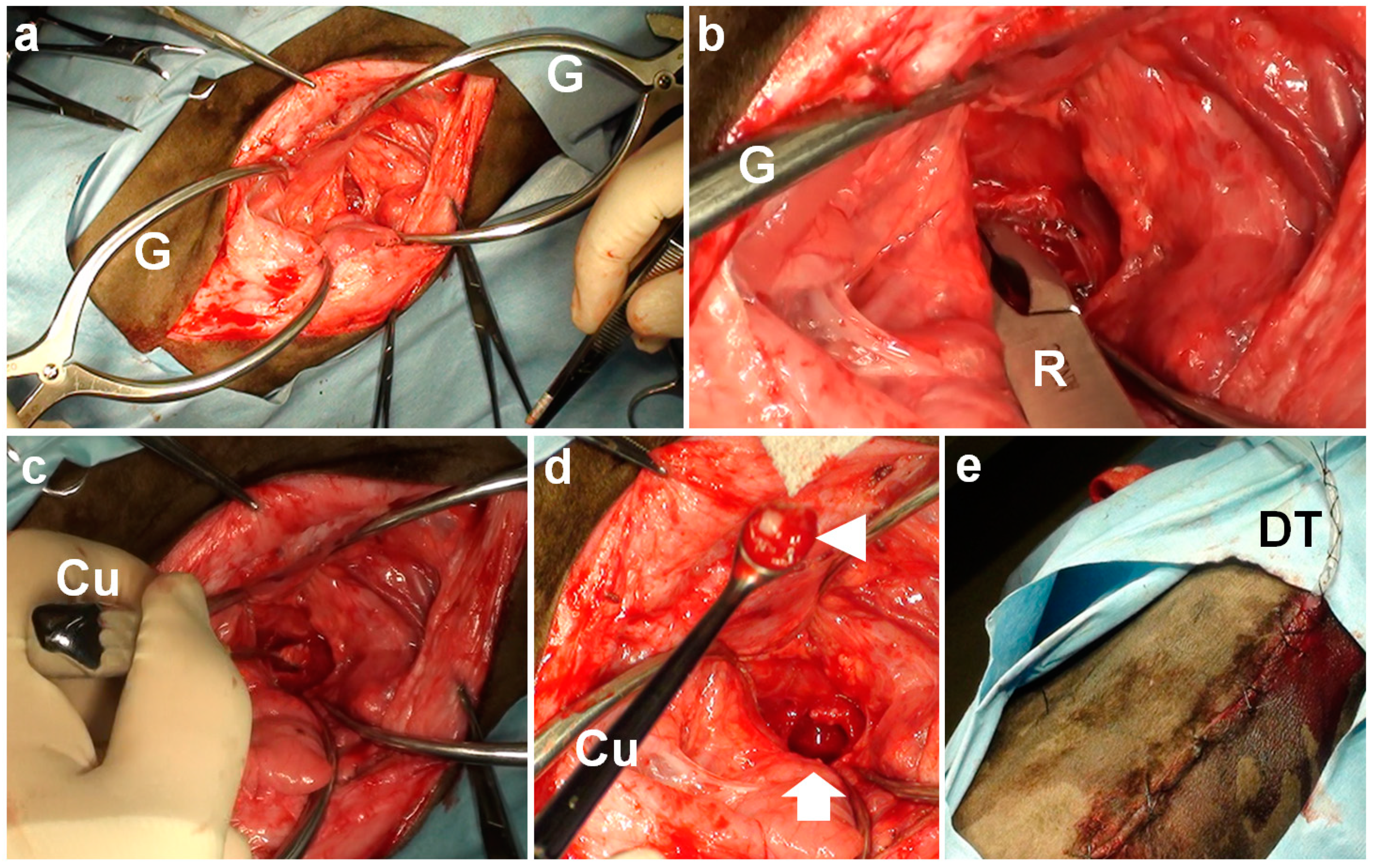
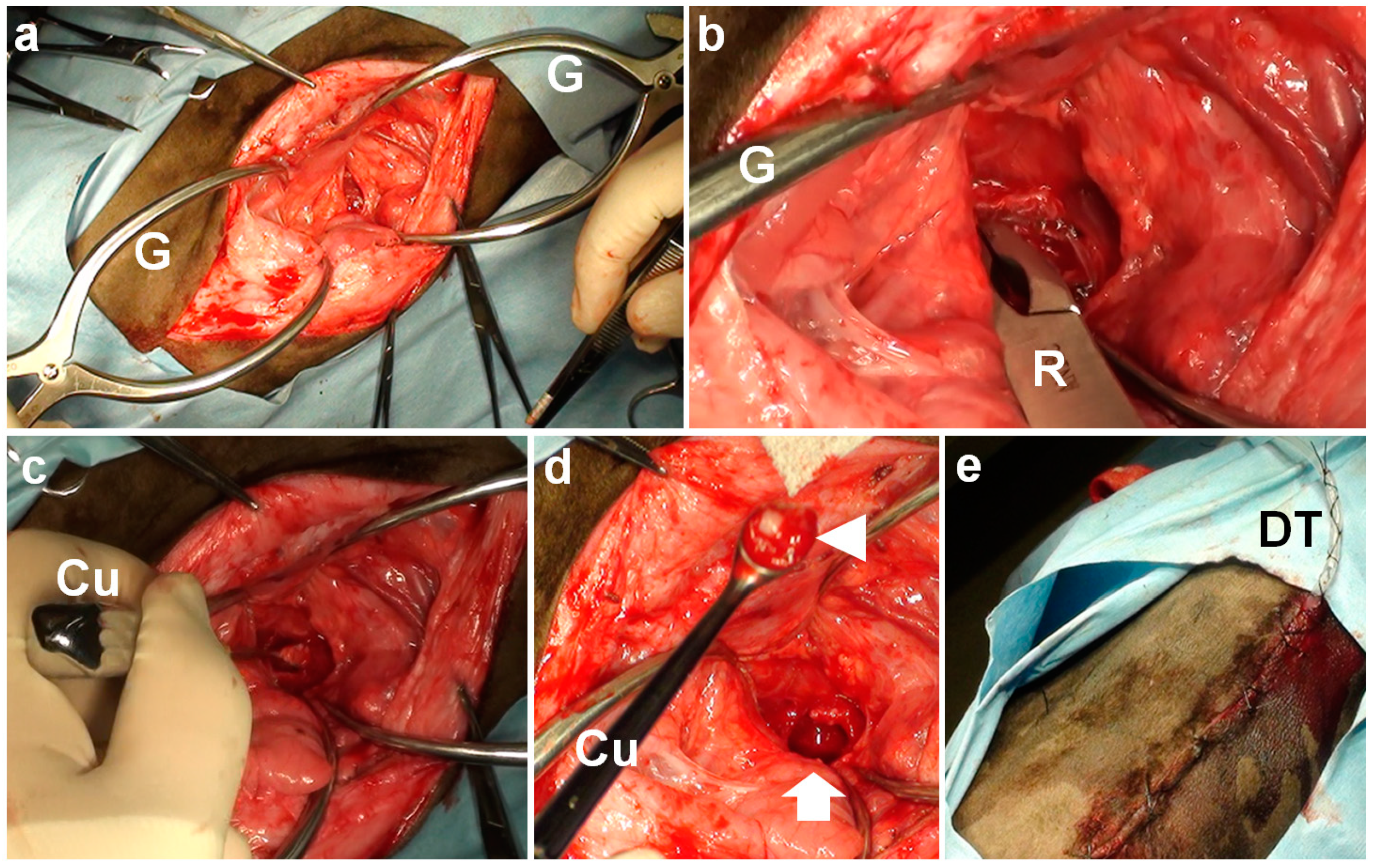
31]. Additionally, the vagus nerve is present on this surgical route. During the present procedure of VBO, the trachea and the vagus nerve may have been stressed by the mechanical pressure generated by the Gelpi retractors. During VBOs in canine and feline cases, the use of self-retaining retractors is also unavoidable to maintain a good surgical view, and care must be taken to prevent injury of the nerves and vessels [
23,
25]. In this study, the length of the extended skin incisions depended on the body size of the treated animals; a 15 cm skin incision in Case 1 vs. a 10 cm skin incision in Cases 2 and 3. The extension of the skin incision may contribute to a reduction in the mechanical stress generated by the Gelpi retractors, although this increases surgical invasiveness.
To enhance the therapeutic effects obtained from VBO, it is recommended that a drain tube be placed into the tympanic cavity via the perforation made at the ventral wall of the tympanic bulla, to allow postoperative irrigation in bovine cases [
7]. However, the drainage and irrigation effects rendered by the placing of a drainage tube have not been fully evaluated. Regardless of whether a drainage tube is used or not, the effusion and irrigation solution may naturally seep out via the perforation made ventrally, and retained within the surgical wounds. Based on the favorable result in Case 1, which was treated with VBO without the placing of a drainage tube, the applicability and necessity of using the drainage method should, therefore, be assessed, in terms of the technical development of VBO for the bovine cases.
In addition to preoperative and/or postoperative uses of CT in diagnosing, therapeutic planning, and evaluating the degree of surgical achievements, the intraoperative utilization of CT may represent an advanced technique to prevent intraoperative contingency and postoperative complications. Instead of the macroscopic operation via the surgical view obtained from the use of self-retaining retractors, the procedure of VBOs assisted by CT may contribute to a reduction in surgical time, >1 h in three present cases, because it is effective to perforate the tympanic bulla via a shortened skin incision. The imaging can provide therapeutic evidence to detect whether LBO or VBO is applicable for each case based on preoperative evaluations, such as the concurrent situation of otitis media/interna and otitis externa, degree of extension in the surrounding structures, and the osseous changes in the tympanic bulla, such as the degrees of expansion, thickening, and osteolysis. Based on the utility of CT in the three cases above, the severity of such osseous changes can be evaluated quantitatively by comparison with the normal ranges obtained from age-matched animals. Further utilization of CT for bovine otitis media is required to establish the age-based reference values of tympanic bulla sizes.



{kind=link}
{kind=link}
{kind=link}
{kind=link}