
Hemodynamic Effects of Protamine Infusion in Dogs with Myxomatous Mitral Valve Disease Undergoing Mitral Valvuloplasty

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
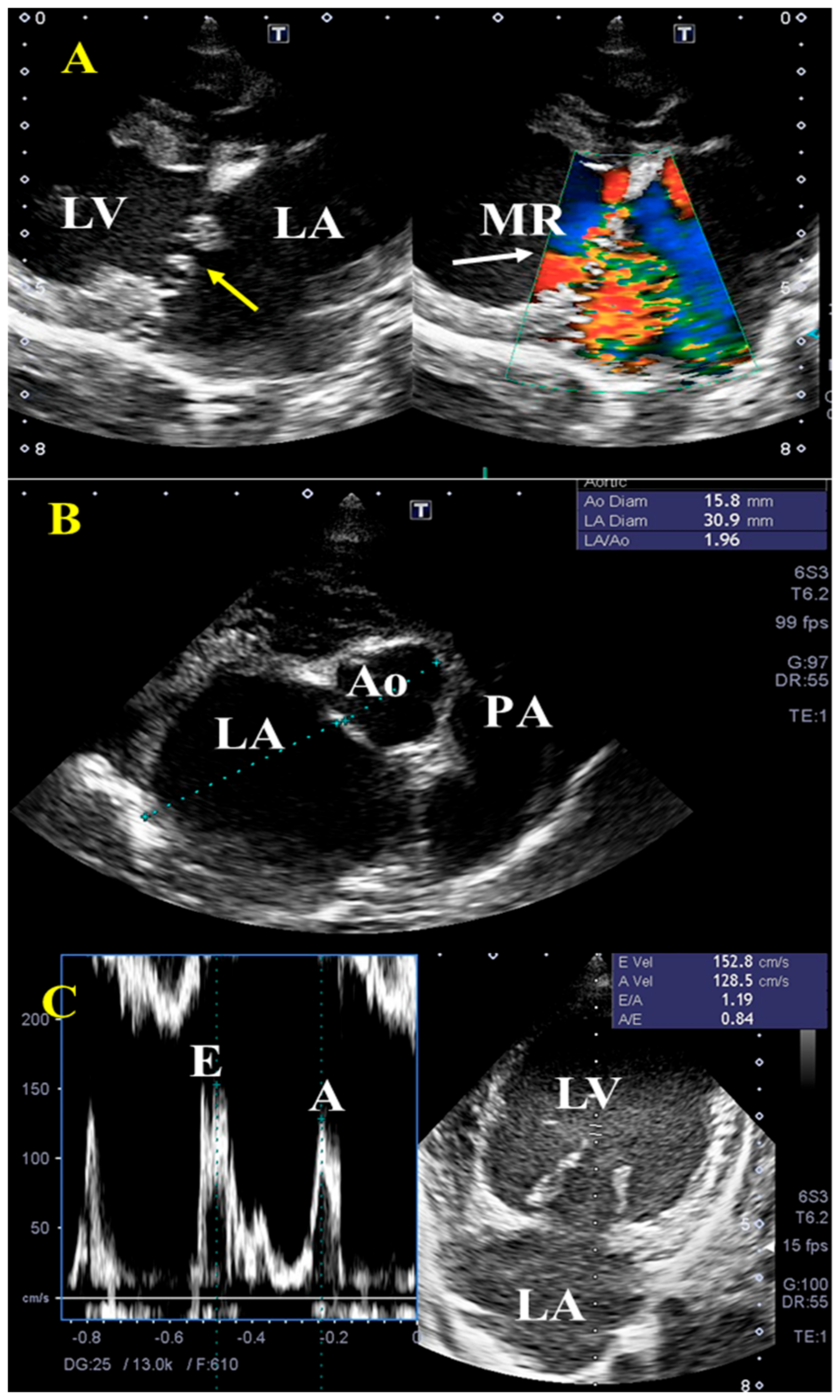
2.2. Echocardiography
2.3. Surgical Procedure
2.4. Definition of Hypotension after Protamine Infusion
2.5. Protocol of Protamine and Catecholamine Administration
2.6. Animal Classification
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Dogs and Preoperative Echocardiography Examination
3.2. Dose of Catecholamines during Protamine Infusion
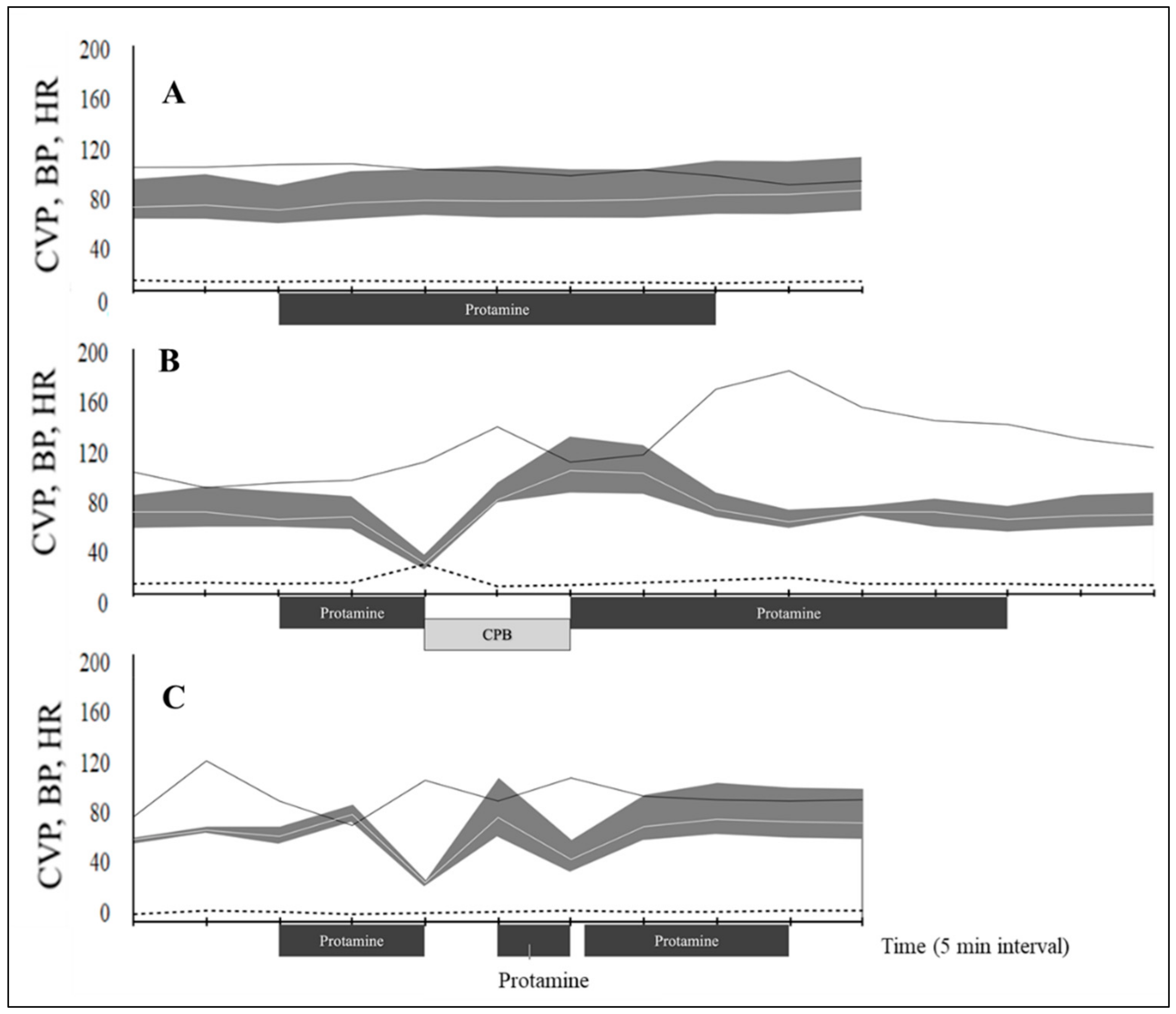
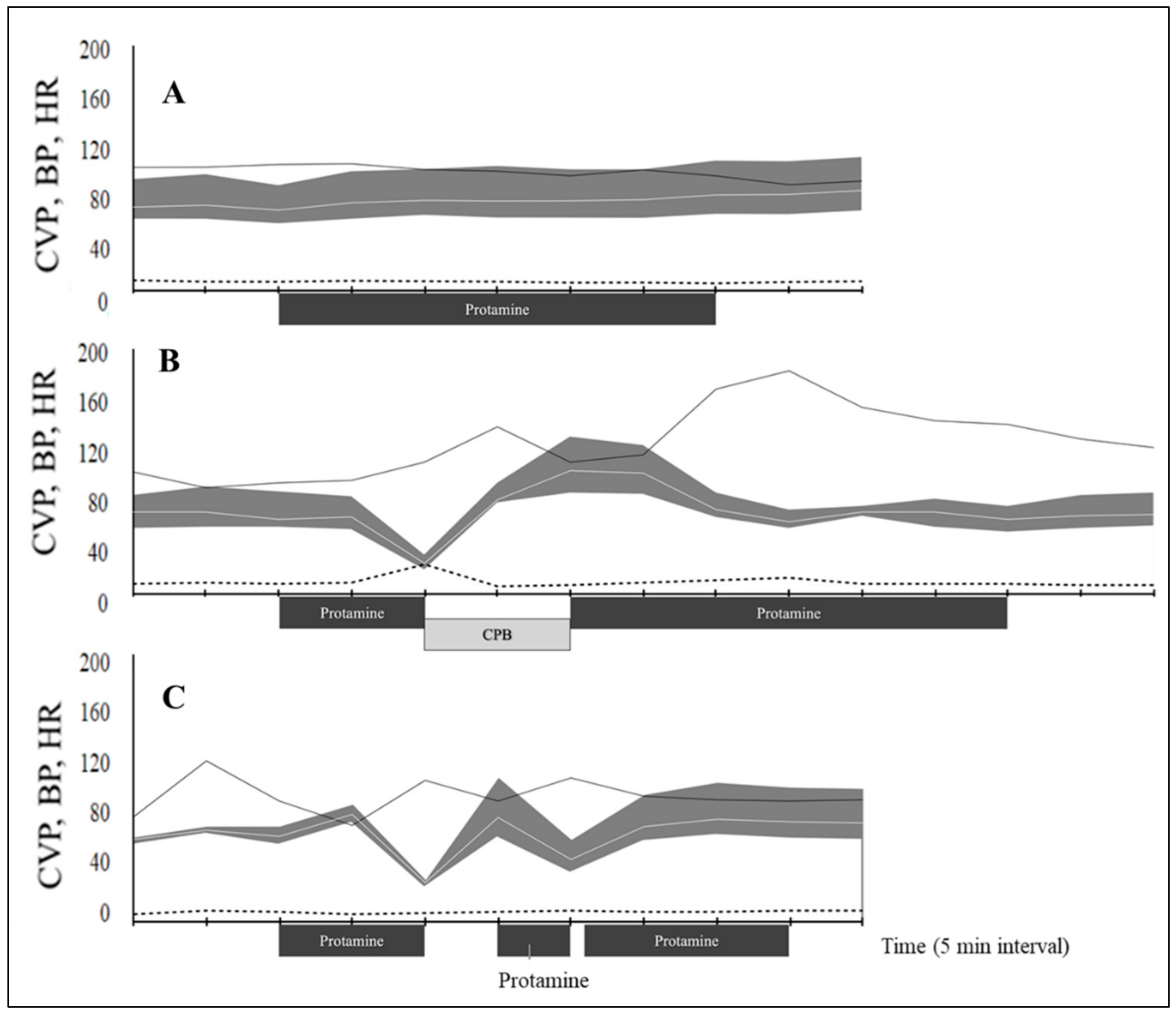
3.3. Arterial and Central Venous Pressure after Protamine Infusion
3.4. Protamine-Induced Hypotension
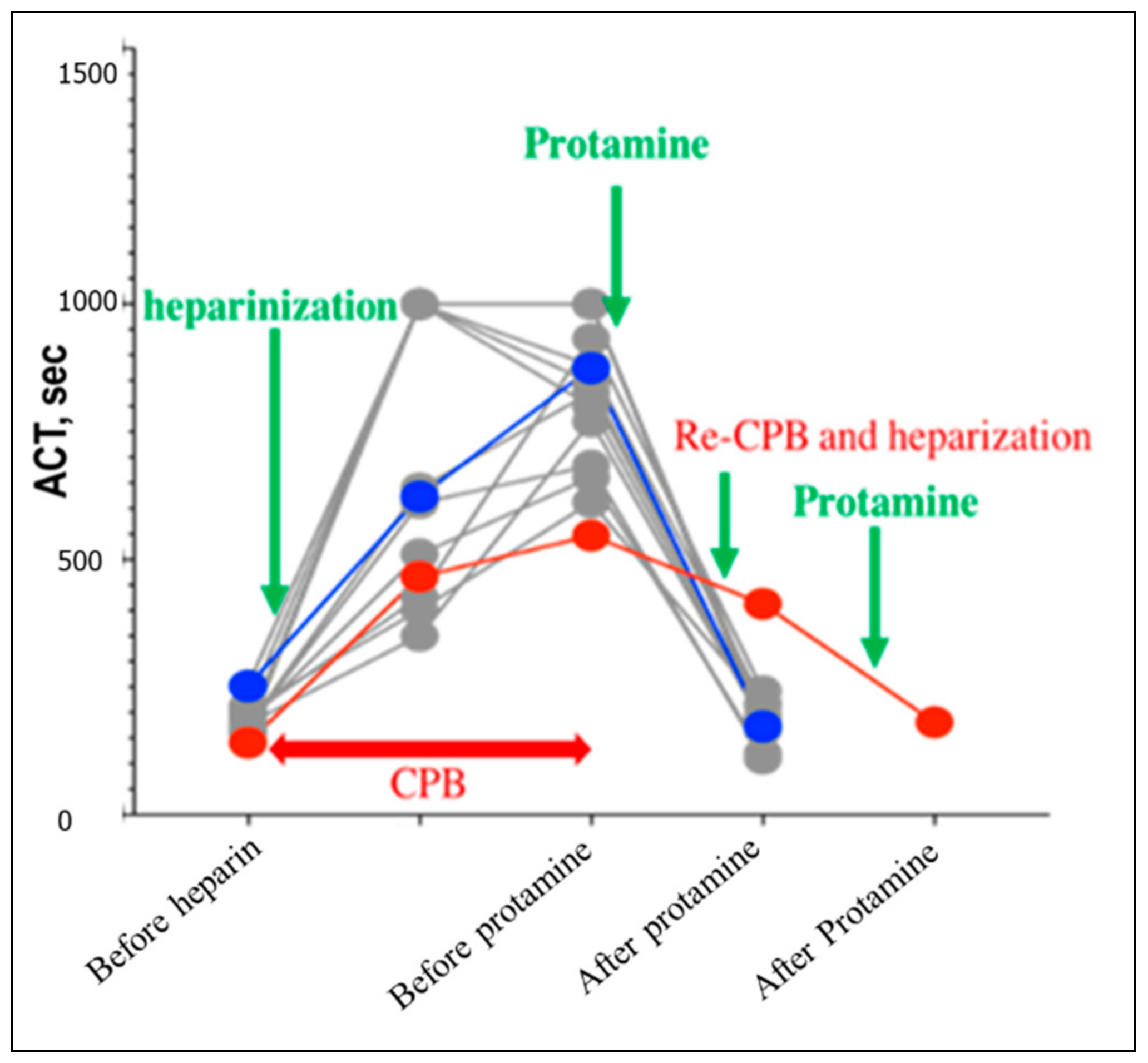
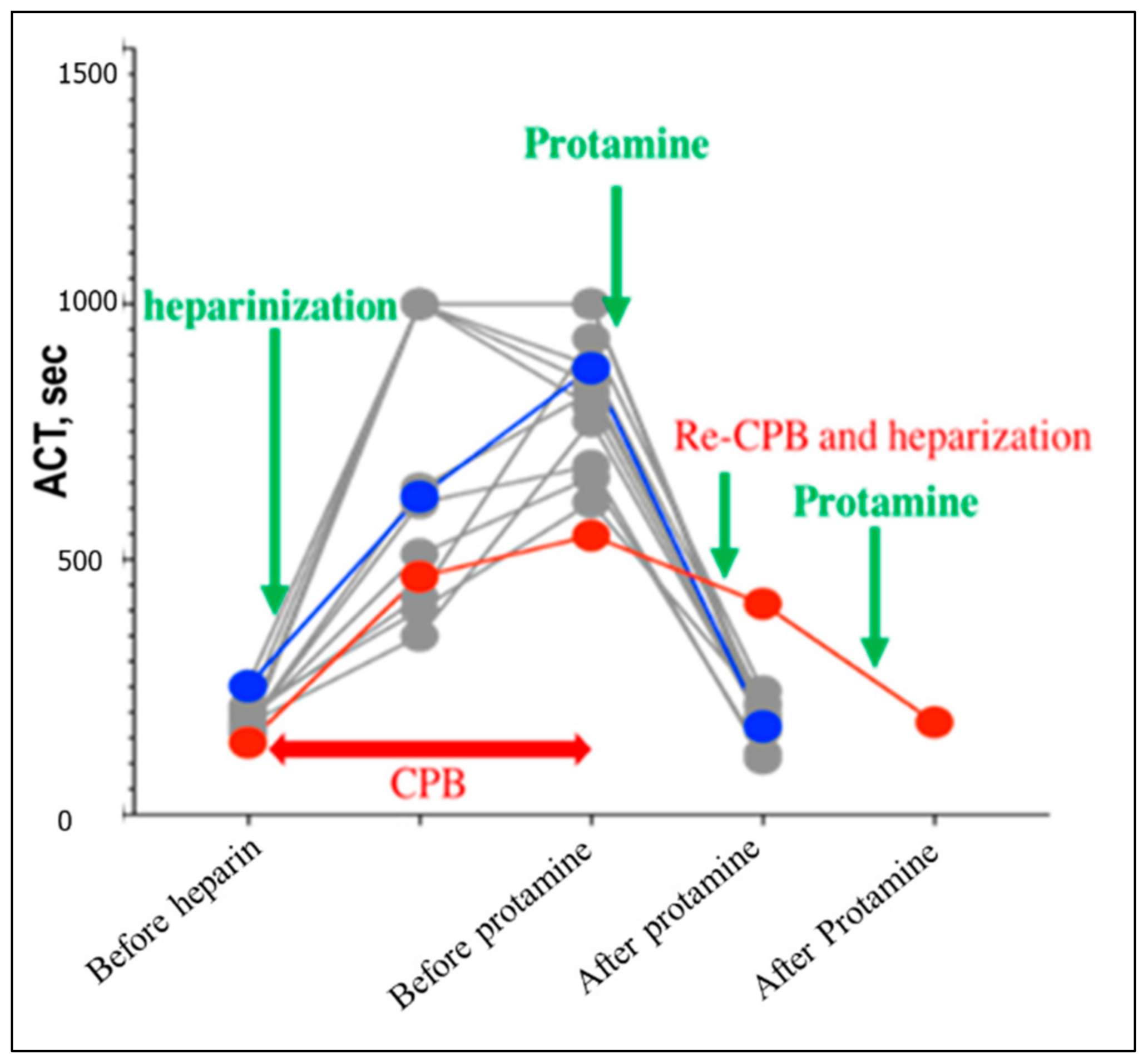
3.5. Activated Clotting Time (ACT)
3.6. Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Keene, B.W.; Atkins, C.E.; Bonagura, J.D.; Fox, P.R.; Häggström, J.; Fuentes, V.L.; Oyama, M.A.; Rush, J.E.; Stepien, R.; Uechi, M. ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. J. Vet. Intern. Med. 2019, 33, 1127–1140. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.-J.; Mandour, A.S.; Yoshida, T.; Watari, T.; Tanaka, R.; Matsuura, K. Changes in renin-angiotensin-aldosterone system during cardiac remodeling after mitral valvuloplasty in dogs. J. Vet. Intern. Med. 2022. [Google Scholar] [CrossRef]
- Kanemoto, I.; Taguchi, D.; Yokoyama, S.; Mizuno, M.; Suzuki, H.; Kanamoto, T. Open heart surgery with deep hypothermia and cardiopulmonary bypass in small and toy dogs. Vet. Surg. 2010, 39, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Shimada, K.; Hamabe, L.; Uchide, T.; Tanaka, R.; Matsuura, K. Measurement of Pulmonary Artery Wave Reflection Before and After Mitral Valvuloplasty in Canine Patients With Pulmonary Hypertension Caused by Myxomatous Mitral Valve Disease. Front. Vet. Sci. 2021, 8, 773035. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Ma, D.; Mandour, A.S.; Ozai, Y.; Yoshida, T.; Matsuura, K.; Takeuchi, A.; Cheng, C.-J.; El-Husseiny, H.M.; Hendawy, H.; et al. Evaluation of Changes in the Cardiac Function before and after Transcatheter Edge-to-Edge Mitral Valve Repair in Healthy Dogs: Conventional and Novel Echocardiography. Animals 2022, 12, 56. [Google Scholar] [CrossRef]
- Chu, Y.Q.; Cai, L.J.; Jiang, D.C.; Jia, D.; Yan, S.Y.; Wang, Y.Q. Allergic shock and death associated with protamine administration in a diabetic patient. Clin. Ther. 2010, 32, 1729–1732. [Google Scholar] [CrossRef] [PubMed]
- Leung, L.W.M.; Gallagher, M.M.; Evranos, B.; Bolten, J.; Madden, B.P.; Wright, S.; Kaba, R.A. Cardiac arrest following protamine administration: A case series. EP Eur. 2019, 21, 886–892. [Google Scholar] [CrossRef]
- Nybo, M.; Madsen, J.S. Serious anaphylactic reactions due to protamine sulfate: A systematic literature review. Basic Clin. Pharmacol. Toxicol. 2008, 103, 192–196. [Google Scholar] [CrossRef]
- Marin-Neto, J.A.; Sykes, M.K.; Marin, J.L.; Orchard, C.; Chakrabarti, M.K. Effects of heparin and protamine on left ventricular performance in the dog. Cardiovasc. Res. 1979, 13, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Morgan, M.R.; Monnet, E.; Gaynor, J.S. The effect of differing rates and injection sites on the amount of protamine delivered before detection of hemodynamic alterations in dogs. Vet. Surg. 2000, 29, 442–448. [Google Scholar] [CrossRef]
- Kien, N.D.; Quam, D.D.; Reitan, J.A.; White, D.A. Mechanism of hypotension following rapid infusion of protamine sulfate in anesthetized dogs. J. Cardiothorac. Vasc. Anesth. 1992, 6, 143–147. [Google Scholar] [CrossRef]
- Boswood, A.; Gordon, S.G.; Häggström, J.; Wess, G.; Stepien, R.L.; Oyama, M.A.; Keene, B.W.; Bonagura, J.; MacDonald, K.A.; Patteson, M.; et al. Longitudinal Analysis of Quality of Life, Clinical, Radiographic, Echocardiographic, and Laboratory Variables in Dogs with Preclinical Myxomatous Mitral Valve Disease Receiving Pimobendan or Placebo: The EPIC Study. J. Vet. Intern. Med. 2018, 32, 72–85. [Google Scholar] [CrossRef] [PubMed]
- Cornell, C.C.; Kittleson, M.D.; Della Torre, P.; Häggström, J.; Lombard, C.W.; Pedersen, H.D.; Vollmar, A.; Wey, A. Allometric scaling of M-mode cardiac measurements in normal adult dogs. J. Vet. Intern. Med. 2004, 18, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Oshima, N.; Watari, T. Effect of modified ultrafiltration on cytokines and hemoconcentration in dogs undergoing cardiopulmonary bypass. J. Vet. Med. Sci. 2020, 82, 1589–1593. [Google Scholar] [CrossRef]
- Mizutani, T.; Takahashi, S.; Kihara, S.; Toyooka, H. Repeated administration of protamine does not attenuate circulatory changes caused by protamine reversal of heparin in dogs. J. Cardiothorac Vasc. Anesth. 2001, 15, 346–351. [Google Scholar] [CrossRef]
- Viaro, F.; Dalio, M.B.; Evora Md, P.R.B. Catastrophic Cardiovascular Adverse Reactions to Protamine Are Nitric Oxide/Cyclic Guanosine Monophosphate Dependent and Endothelium Mediated: Should Methylene Blue Be the Treatment of Choice? Chest 2002, 122, 1061–1066. [Google Scholar] [CrossRef]
- Geurink, K.R.; Granger, C.B.; Liao, L.; Thomas, N.G.; Lindsey, B.C.; Babin, E.; Turgeon, N.; Alexander, J.; Pokorney, S.D. A reversal of fortune: A case of cardiovascular collapse following protamine sulfate infusion. HeartRhythm Case Rep. 2020, 6, 322–324. [Google Scholar] [CrossRef] [Green Version]
- Welsby, I.J.; Newman, M.F.; Phillips-Bute, B.; Messier, R.H.; Kakkis, E.D.; Stafford-Smith, M. Hemodynamic changes after protamine administration: Association with mortality after coronary artery bypass surgery. Anesthesiology 2005, 102, 308–314. [Google Scholar] [CrossRef]
- Lee, J.Z.; Boilson, B.A.; Killu, A.M. To the Editor-Hemodynamic collapse following protamine sulfate: The impact of acute pulmonary vasoconstriction. HeartRhythm Case Rep. 2020, 6, 547. [Google Scholar] [CrossRef]
- Wakefield, T.W.; Hantler, C.B.; Wrobleski, S.K.; Crider, B.A.; Stanley, J.C. Effects of differing rates of protamine reversal of heparin anticoagulation. Surgery 1996, 119, 123–128. [Google Scholar] [CrossRef]
- Levy, J.H.; Adkinson, N.F., Jr. Anaphylaxis during cardiac surgery: Implications for clinicians. Anesth. Analg. 2008, 106, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Valchanov, K.; Falter, F.; George, S.; Burt, C.; Roscoe, A.; Ng, C.; Besser, M.; Nasser, S. Three Cases of Anaphylaxis to Protamine: Management of Anticoagulation Reversal. J. Cardiothorac. Vasc. Anesth. 2019, 33, 482–486. [Google Scholar] [CrossRef]
- Nordström, L.; Fletcher, R.; Pavek, K. Shock of anaphylactoid type induced by protamine: A continuous cardiorespiratory record. Acta Anaesthesiol. Scand. 1978, 22, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Ford, S.A.; Kam, P.C.; Baldo, B.A.; Fisher, M.M. Anaphylactic or anaphylactoid reactions in patients undergoing cardiac surgery. J. Cardiothorac Vasc. Anesth. 2001, 15, 684–688. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, S.; Chan, S.P.; Tan, W.C.; Eng, J.; Li, B.; Luo, H.D.; Teoh, L.K. Cardiopulmonary bypass time: Every minute counts. J. Cardiovasc. Surg. 2018, 59, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Miles, L.F.; Burt, C.; Arrowsmith, J.; McKie, M.A.; Villar, S.S.; Govender, P.; Shaylor, R.; Tan, Z.; De Silva, R.; Falter, F. Optimal protamine dosing after cardiopulmonary bypass: The PRODOSE adaptive randomised controlled trial. PLoS Med. 2021, 18, e1003658. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variables | Non-Hypotensive (n = 12) | Hypotensive (n = 2) | |
|---|---|---|---|
| Dog 1 | Dog 2 | ||
| Mean of Age, y | 10.2 ± 1.5 (8.5–14) | 11 | 9 |
| Sex | cM (4), sF (4), M (3), F (1) | cM | cM |
| Breed | Chihuahua (5), Mongrel (2), Chin (1), CKCS (1), Maltese (1), Pomeranian (1), Shih Tzu (1) | CKCS | Chihuahua |
| Body weight, kg | 4.3 ± 3.7 (2.4–8.0) | 7 | 3.6 |
| ACVIM Stage | B2 (5), C (4), D (3) | C | C |
| Blood pressure | |||
| Before operation | |||
| Systolic, mmHg | 140 ± 23 | 156 | 146 |
| Mean, mmHg | 110 ± 30 | 110 | 109 |
| Diastolic, mmHg | 95 ± 30 | 87 | 91 |
| One day after the operation | |||
| Systolic BP, mmHg | 135 ± 11 | 122 | 143 |
| Mean BP, mmHg | 91 ± 12 | 106 | 122 |
| Diastolic BP, mmHg | 70 ± 25 | 99 | 112 |
| Heart rate, bpm | 150 ± 44 | 133 | 156 |
| Concurrent Disease | None (6), Renal Failure (1), Epilepsy (1), Hydrocephalus (1), Hypothyroidism (1), Idiopathic Thrombocytopenia (1) | none | None |
| Hospitalization, days | 6 (6–12) | 6 | 6 |
| Time between heparin and protamine, min | 125 ± 53 | 145 | 120 |
| Mortality | 1/12 (8.3%) | 0/2 (0%) | |
| Variables | Unit | Non-Hypotensive (n = 12) | Hypotensive (n = 2) | |
|---|---|---|---|---|
| Dog 1 | Dog 2 | |||
| BW | kg | 4.38 ± 1.5 | 8 | 3.55 |
| LVIDd | mm | 33.4 ± 2.3 | 43 | 26.3 |
| LVIDDN | 2.2 ± 0.12 | 2.32 | 2.02 | |
| LA/Ao | 2.55 ± 0.45 | 2.8 | 2.14 | |
| FS (%) | % | 52.6 ± 6.5 | 56 | 62.7 |
| E velocity | cm/s | 144.9 ± 23.2 | 175 | 131 |
| E/A | 2.2 ± 0.9 | 5.14 | 1.32 | |
| S’ sep | cm/s | 9.3 ± 1.5 | 9.1 | 10.9 |
| E’ sep | cm/s | 10.4 ± 2.6 | 7 | 10 |
| A’ sep | cm/s | 6.4 ± 1.5 | 7 | 7.3 |
| S’ lat | cm/s | 10.8 ± 3.0 | 6.1 | 10.3 |
| E’ lat | cm/s | 8.3 ± 2.0 | 7.2 | 9.1 |
| A’ lat | cm/s | 8.7 ± 3.6 | 5.3 | 8.9 |
| Variables | Non-Hypotensive (n = 12) | Hypotensive (n = 2) | ||
|---|---|---|---|---|
| Dog 1 | Dog 2 | |||
| Norepinephrine, μg–1 kg–1 min | 0.05 (0–0.1) | 0.1 | 0.2 | |
| Dobutamine, μg–1 kg–1 min | 4 (0–5) | 5 | 5 | |
| Variables | Time (min) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| −10 | −5 | 0 | 5 | 10 | 15 | 20 | 25 | 30 | 35 | 40 | ||
| HR | bpm | 102.6 (26.7) | 102.3 (31.6) | 104 (24) | 106.3 (31.7) | 98.4 (22.5) | 97.6 (21.2) | 93 (25.3) | 97.8 (28.9) | 94.7 (26.7) | 87.9 (20.4) | 90.5 (21.4) |
| SYS | mmHg | 90.5 (14.9) | 95.5 (17.8) | 86.6 (13.8) | 101.3 (24.3) | 100.2 (17.4) | 101.1 (20.5) | 100.3 (16.1) | 99.8 (19.8) | 106.8 (19.4) | 104.9 (17.3) | 109.2 (26.3) |
| DIA | mmHg | 59.9 (14.5) | 59.4 (11.5) | 55.7 (12.3) | 61.5 (15.4) | 62.7 (10.6) | 59.7 (11) | 60.4 (8.6) | 60.3 (8.2) | 63.6 (7.2) | 62.9 (5.6) | 65.9 (15.4) |
| MAP | mmHg | 69 (12.9) | 70.5 (11.5) | 66.3 (13) | 74.8 (17.7) | 74.6 (10.9) | 73.1 (12.7) | 74.1 (9.1) | 75.1 (10.4) | 78.8 (9.3) | 78.7 (8.5) | 81.6 (16.3) |
| CVP | mmHg | 8.3 (3.6) | 7.2 (4.1) | 7.1 (3.9) | 7.8 (4.9) | 7.5 (3.7) | 7.2 (3.5) | 6.4 (3.8) | 6.5 (4.2) | 5.9 (4.3) | 6.9 (4.1) | 7.4 (3.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshida, T.; Matsuura, K.; Mandour, A.S.; Aboshi, Y.; Yamada, S.; Yotsuida, H.; Hasegawa, M.; Cheng, C.-J.; Yaginuma, Y.; Watanabe, M.; et al. Hemodynamic Effects of Protamine Infusion in Dogs with Myxomatous Mitral Valve Disease Undergoing Mitral Valvuloplasty. Vet. Sci. 2022, 9, 178. https://doi.org/10.3390/vetsci9040178
Yoshida T, Matsuura K, Mandour AS, Aboshi Y, Yamada S, Yotsuida H, Hasegawa M, Cheng C-J, Yaginuma Y, Watanabe M, et al. Hemodynamic Effects of Protamine Infusion in Dogs with Myxomatous Mitral Valve Disease Undergoing Mitral Valvuloplasty. Veterinary Sciences. 2022; 9(4):178. https://doi.org/10.3390/vetsci9040178
Chicago/Turabian StyleYoshida, Tomohiko, Katsuhiro Matsuura, Ahmed S. Mandour, Yuki Aboshi, Shusaku Yamada, Hideki Yotsuida, Mizuki Hasegawa, Chieh-Jen Cheng, Youta Yaginuma, Momoko Watanabe, and et al. 2022. "Hemodynamic Effects of Protamine Infusion in Dogs with Myxomatous Mitral Valve Disease Undergoing Mitral Valvuloplasty" Veterinary Sciences 9, no. 4: 178. https://doi.org/10.3390/vetsci9040178
APA StyleYoshida, T., Matsuura, K., Mandour, A. S., Aboshi, Y., Yamada, S., Yotsuida, H., Hasegawa, M., Cheng, C.-J., Yaginuma, Y., Watanabe, M., & Fukuzumi, S. (2022). Hemodynamic Effects of Protamine Infusion in Dogs with Myxomatous Mitral Valve Disease Undergoing Mitral Valvuloplasty. Veterinary Sciences, 9(4), 178. https://doi.org/10.3390/vetsci9040178